")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Case of Paradoxical Reactions to Biologic Therapy for Psoriasis
Authors Zhou Q, Zhou S , Xiong H, Yang J, Yang Z, Zhou N, Mao J, Li M
Received 16 March 2023
Accepted for publication 16 May 2023
Published 12 June 2023 Volume 2023:16 Pages 1493—1497
DOI https://doi.org/10.2147/CCID.S412520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Qianqian Zhou,1 Shengru Zhou,1 Huizi Xiong,1 Jianqiu Yang,1 Ziliang Yang,2 Naihui Zhou,2 Jinzhu Mao,2 Min Li1,2
1Department of Dermatology, Dushu Lake Hospital Affiliated to Soochow University (Medical Center of Soochow University, Suzhou Dushu Lake Hospital), Suzhou, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China
Correspondence: Min Li, Department of Dermatology, Dushu Lake Hospital Affiliated to Soochow University (Medical Center of Soochow University, Suzhou Dushu Lake Hospital), No. 9, Chongwen Road, Suzhou, 215123, People’s Republic of China, Tel +86-18936140383, Email [email protected]
Introduction: Psoriasis is an immune-mediated chronic inflammatory skin disease. As our understanding of the pathogenesis of psoriasis has improved, biologic agents have become increasingly important in the treatment of psoriasis. However, the use of biologic agents is associated with cutaneous side effects. A new type of side effect called paradoxical reactions is an emerging threat arising from the increasing use of biologic agents.
Case: Here, we present a case of paradoxical skin reactions – pyoderma gangrenosum (PG) and eczema – induced by biologic therapy. The case was successfully and eventually treated with baricitinib.
Discussion: PG is a rare inflammatory disease characterised by painful and necrotic ulcerations containing neutrophils. It has been associated with autoimmune diseases such as inflammatory bowel disease (IBD). TNF (tumor necrosis factor) -α inhibitors can effectively treat refractory PG, while IL (interleukin) − 17A inhibitors may worsen IBD symptoms. The cause of PG in this case was believed to be secukinumab, not adalimumab. The patient was diagnosed with eczematous dermatitis due to TNF-α inhibitors, and baricitinib was added to treat eczematous dermatitis.
Conclusion: Paradoxical reactions are unpredictable events that may occur during treatment with biologics at anytime. They need further research in order to formulate personalised treatment.
Keywords: biology drugs, pyoderma gangrenosum, eczema, adalimumab, secukinumab, baricitinib
Introduction
Psoriasis is an immune-mediated chronic inflammatory skin disease, requiring long-term treatment.1 Currently, there are several treatments for psoriasis including topical therapy, phototherapy, oral systemic therapies and biologics.1 With the deepening of the understanding of the pathogenesis of psoriasis, biological agents occupy an increasingly important position in the treatment of psoriasis. However, the cutaneous side effects appear with the use of biological agents. A new type of side effect, known as paradoxical reactions, is an emerging threat arising from the increasing use of biological agents. These include paradoxical psoriasis, eczema, IBD, but also alopecia areata (AA), lichen planus (LP), hidradenitis suppurativa (HS), PG and bullous pemphigoid (BP).2 Here, we present a case of paradoxical skin reactions: PG and eczema, which are induced by biologic therapy.
Case Report
The PG Part of the Case
Previous History
A 38-year-old Chinese woman had a history of psoriasis for more than one year, accompanied by pain in the sacroiliac joints. In July 2020, she was treated with adalimumab, known under the trade name Anjianning, which is one of TNF-α inhibitors. However, there was no apparent improvement in the rash and joint symptoms after 6 weeks. The patient’s biologic drugs were changed to secukinumab, one of IL-17A inhibitors, from the end of August. The rash essentially resolved after the fifth injection, but the sacroiliac joint symptoms still persisted.
Dermatological Examination
One month later, the patient developed a painful mung bean-sized red papule with purulent discharge on the mons pubis without any obvious trigger. Subsequently, similar eruptions appeared in succession on the left thigh, right buttock, right breast, and eyebrows (Figure 1A–E), with ulcer surfaces containing red granulation tissue and yellow necrotic debris with raised oedematous borders.
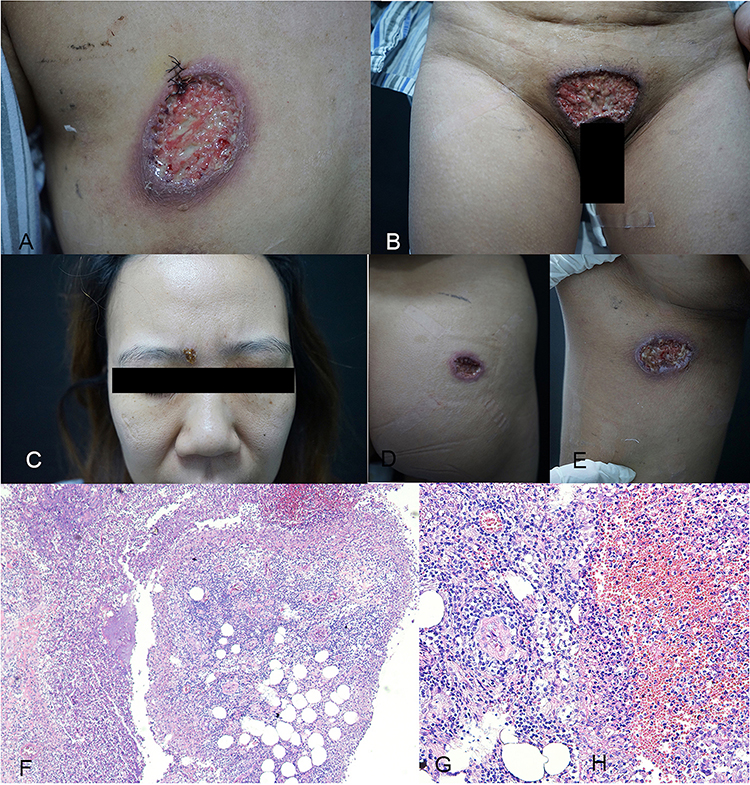 |
Figure 1 Clinical manifestations in a 38-year-old female with PG before treatment. Scattered ulcers were seen on the patient’s pubic area, left thigh, right buttock, right breast, and eyebrow, with red granulation tissue and yellow necrotic debris on the surface of the ulcers and edema at the elevated border. (A–E) Histopathology of a PG lesion from the right thorax (stained with haematoxylin and eosin; magnifications: (F) ×40, ((G and H) ×200). The epidermis is hypertrophic, spongy and oedematous, with neutrophil migration into the epidermis (F). The dermis is locally infiltrated with neutrophils forming areas of cerebral swelling and necrosis, with surrounding areas of granulomatous inflammation and infiltration of inflammatory cells such as lymphocytes, plasma cells and eosinophils (G), with necrosis of the vessel wall and spillage of large red blood cells (H). |
Laboratory, Ancillary and Histopathological Examination of Skin Lesions
All bacterial, mycobacterial and fungal cultures were negative and colonoscopy showed no obvious abnormalities. Pathology showed that acanthosis, sponge oedema and neutrophil infiltration into the epidermis. A large number of neutrophils formed a necrotic abscess in the dermal layer, surrounded by granulomatous inflammatory areas, and inflammatory cells such as lymphocytes, plasma cells, and eosinophils could infiltrated. It also shows necrosis of the vessel wall and overflow of large red blood cells (Figure 1F–H). PG should be considered combined with the patient’s clinical manifestations and examination after mycobacterial and fungal infections have been ruled out.
Treatment and Care
On the 15th day of admission, we had chosen another adalimumab, known by the trade name Humira, to treat the patient because that adalimumab had successfully treated PG.3,4 The patient was discharged at the end of December with gradual improvement in the skin lesions and joint symptoms.
The Eczema Part of the Case
The patient’s PG improved but pruritus and dark red macules appeared three months later (Figure 2A–C). We diagnose patients with eczema according to the lesions together with increasing of eosinophils and immunoglobulin E (lgE). Then, we changed the frequency of adalimumab in accordance with several cases of TNF-α inhibitors causing PG, including adalimumab, infliximab and etanercept.5–9 However, eczema was not well controlled and adalimumab was stopped on May 4. We selected baricitinib, one of janus kinase (JAK) inhibitors, to treat PG, eczema and psoriasis arthritis (PsA) based on European guideline on atopic eczema and Food and Drug Administration (FDA)-approved patient medication guide.10,11 PG, PsA and eczema improved, eosinophils and lgE decreased after one week of oral baricitinib treatment (Figure 2D).
 |
Figure 2 Clinical manifestations in a 38-year-old female with PG and eczema. Scattered ulcers with a small amount of pus on the surface were seen on the right chest and vulva. The ulcers were surrounded by erythema and hyperpigmentation. There were scattered erythema, claw marks, and crusts on the trunk. (A–C) and after 4 months of treatment with baricitinib. Pinkish scarring was seen on the right breast and vulva. There was scattered pigmentation on the trunk. (D). |
Discussion
PG is a rare neutrophilic dermatosis that presents with rapidly evolving, painful skin ulcers characterized by indurated margins and peripheral erythema.12 PG has been associated with autoimmune diseases, for example IBD and rheumatic arthritis.13 The levels of cytokines, including IL-17, TNF-α and IL-23, are high in PG skin lesions.14 Therefore, biologic drugs have been used to treat PG.15 These biologic agents are also used to treat psoriasis, but they could cause paradoxical reactions sometime, such as recrudescence and aggravation of the psoriasis. Our patient had two different types of paradoxical reactions. The first was the development of PG while on secukinumab and the second was the development of eczema while on adalimumab.
In our case, the patient had previously used TNF-α inhibitors and IL-17A inhibitors. The existing articles have clarified that TNF-α inhibitors can effectively treat refractory PG presently.16–18 Previous studies have found that the Th17-IL17 axis is upregulated in both psoriasis and IBD, and the axis plays an important role in the development of the disease.19 Therefore, people take it for granted that inhibiting IL-17 would be effective in IBD as the same as psoriasis.19 However, anti-IL-17A drugs have no significant effect in the treatment of IBD, and can even strengthen the activity of IBD.20,21 The reason may be that blocking IL-17 may increase intestinal inflammation, weaken the intestinal barrier and increase the risk of microbial infections.21 PG is closely related to IBD and is considered to be one of the skin manifestations of IBD.14 Skin manifestations include erythema nodosum, PG and Sweet syndrome. These skin symptoms are common in patients with IBD and it could be the first signs of IBD sometimes.22 At the same time, several cases have reported IL-17 inhibitors caused PG.23,24 The half-life of adalimumab is less than 20 days according to the instructions for use, and the last injection of adalimumab was more than a month after the appearance of PG lesions. In summary, we believe that the cause of PG is secukinumab.
We considered our case to be eczematous dermatitis due to adalimumab, one of the TNF-α inhibitors, a rare side effect that had already been reported in the cases and reviews.25–27 Cutaneous side effects caused by anti-TNF-α inhibitors have been reported in recent years including injection site reactions, multiple erythema, vasculitis, infection, cancerous and precancerous lesions, eczema-like purpura.26 Eczema dermatitis due to TNF-α inhibitors in patients may occur soon after the start of treatment, or it may occur several months later. In our case, it happened immediately. It is usually not necessary to stop anti-TNF-α treatment, because local treatment is sufficient to control eczema. In this case, itching and eczema are difficult to control, and we stopped adalimumab and added baricitinib to treat the eczematous dermatitis. According to literatures, baricitinib could treat PsA and PG as well as.28–31 TNF-α is the key mediators in the T-helper (Th)1 pathway. By inhibiting TNF-α to block the Th1 pathway, there is an imbalance that is conducive to increasing the activity of the reverse Th2 pathway associated with inflammatory diseases such as eczema asthma.32
Conclusion
Biological agents used in the treatment of psoriasis target-specific molecules such as TNF-α and IL-17. In predisposed individuals, a cytokine imbalance can occur, leading to an inflammatory process, when part of these immune pathways are blocked. Paradoxical reactions are unexpected and unpredictable events that can occur at anytime when treated with biologics. The understanding of their clinical presentation will have a profound impact on the identification of biologics that are predictive of the occurrence of paradoxical reactions. In our case, adalimumab successfully treated PG and baricitinib was successfully in the treatment of eczema with PG and PsA, providing a new therapeutic approach.
Ethics and Consent
Written informed consent for the publication of this case was provided by the patient for the publication of photographs and all test results. Institutional approval was not required as this is a case report and the patient had already given written informed consent for the publication of photographs and all test results.
Disclosure
The authors declare no conflict of interest.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Miyagawa F. Pathogenesis of paradoxical reactions associated with targeted biologic agents for inflammatory skin diseases. Biomedicines. 2022;10(7):1485. doi:10.3390/biomedicines10071485
3. McKenzie F, Cash D, Gupta A, Cummings LW, Ortega-Loayza AG. Biologic and small-molecule medications in the management of pyoderma gangrenosum. J Dermatolog Treat. 2019;30(3):264–276. doi:10.1080/09546634.2018.1506083
4. Yamamoto T. An update on Adalimumab for pyoderma gangrenos. Drugs Today. 2021;57(9):535–542. doi:10.1358/dot.2021.57.9.3293619
5. Hellstrom AE, Farkkila M, Kolho KL. Infliximab-induced skin manifestations in patients with inflammatory bowel disease. Scand J Gastroenterol. 2016;51(5):563–571. doi:10.3109/00365521.2015.1125524
6. Cleynen I, Van Moerkercke W, Billiet T, et al. Characteristics of skin lesions associated with anti-tumor necrosis factor therapy in patients with inflammatory bowel disease: a cohort study. Ann Intern Med. 2016;164(1):10–22. doi:10.7326/M15-0729
7. Wlodarczyk M, Sobolewska A, Wojcik B, Loga K, Fichna J, Wisniewska-Jarosinska M. Correlations between skin lesions induced by anti-tumor necrosis factor-alpha and selected cytokines in Crohn’s disease patients. World J Gastroenterol. 2014;20(22):7019–7026. doi:10.3748/wjg.v20.i22.7019
8. Esmailzadeh A, Yousefi P, Farhi D, et al. Predictive factors of eczema-like eruptions among patients without cutaneous psoriasis receiving infliximab: a cohort study of 92 patients. Dermatology. 2009;219(3):263–267. doi:10.1159/000235582
9. Davaine AC, Saraux A, Prigent S, et al. Cutaneous events during treatment of chronic inflammatory joint disorders with anti-tumour necrosis factor alpha: a cross-sectional study. J Eur Acad Dermatol Venereol. 2008;22(12):1471–1477. doi:10.1111/j.1468-3083.2008.02935.x
10. Roskoski R. Properties of FDA-approved small molecule protein kinase inhibitors: a 2023 update. Pharmacol Res. 2023;187:106552. doi:10.1016/j.phrs.2022.106552
11. Wollenberg A KM, Arents B, Aszodi N, et al. European guideline (EuroGuiDerm) on atopic eczema: part I – systemic therapy. J Eur Acad Dermatol Venereol. 2022;36(9):1409–1431. doi:10.1111/jdv.18345
12. Maverakis E, Marzano AV, Le ST, et al. Pyoderma gangrenosum. Nat Rev Dis Primers. 2020;6(1). doi:10.1038/s41572-020-0213-x
13. Puig L. Paradoxical reactions: anti-tumor necrosis factor alpha agents, ustekinumab, secukinumab, ixekizumab, and others. Curr Probl Dermatol. 2018;53:49–63.
14. Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal manifestations of inflammatory bowel disease: current concepts, treatment, and implications for disease management. Gastroenterology. 2021;161(4):1118–1132. doi:10.1053/j.gastro.2021.07.042
15. Patel F, Fitzmaurice S, Duong C, et al. Effective strategies for the management of pyoderma gangrenosum: a comprehensive review. Acta Derm Venereol. 2015;95(5):525–531. doi:10.2340/00015555-2008
16. Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14(3):225–233. doi:10.1080/1744666X.2018.1438269
17. Margaret A, Fonder B, Deborah L, et al. Adalimumab therapy for recalcitrant pyoderma gangrenosum. J Burns Wounds. 2006;5(8):66–71.
18. Jaimes-Lopez N, Molina V, Arroyave JE, et al. Development of pyoderma gangrenosum during therapy with infliximab. J Dermatol Case Rep. 2009;3(2):20–23. doi:10.3315/jdcr.2009.1027
19. Hohenberger M, Cardwell LA, Oussedik E, Feldman SR. Interleukin-17 inhibition: role in psoriasis and inflammatory bowel disease. J Dermatolog Treat. 2018;29(1):13–18. doi:10.1080/09546634.2017.1329511
20. Lozano JF, Giménez RS, Fernández MC. Emergence of inflammatory bowel disease during treatment with secukinumab. J Crohns Colitis. 2018;12(9):1131–1133.
21. Fauny M, Moulin D, D’Amico F, et al. Paradoxical gastrointestinal effects of interleukin-17 blockers. Ann Rheum Dis. 2020;79(9):1132–1138. doi:10.1136/annrheumdis-2020-217927
22. Alavi A, French LE, Davis MD, Brassard A, Kirsner RS. Pyoderma gangrenosum: an update on pathophysiology, diagnosis and treatment. Am J Clin Dermatol. 2017;18(3):355–372. doi:10.1007/s40257-017-0251-7
23. Jin K, Matsuzaki Y, Akasaka E, Nakano H, Sawamura D. Pyoderma gangrenosum triggered by switching from adalimumab to secukinumab. J Dermatol. 2019;46(3):e108–e109. doi:10.1111/1346-8138.14611
24. Petty AJ, Whitley MJ, Balaban A, Ellington K, Marano AL. Pyoderma gangrenosum induced by secukinumab in a patient with psoriasis successfully treated with ustekinumab. JAAD Case Rep. 2020;6(8):731–733. doi:10.1016/j.jdcr.2020.06.011
25. Nakamura M, Lee K, Singh R, et al. Eczema as an adverse effect of anti-TNFalpha therapy in psoriasis and other Th1-mediated diseases: a review. J Dermatol Treat. 2017;28(3):237–241. doi:10.1080/09546634.2016.1230173
26. Lee HH, Song IH, Friedrich M, et al. Cutaneous side-effects in patients with rheumatic diseases during application of tumour necrosis factor-alpha antagonists. Br J Dermatol. 2007;156(3):486–491. doi:10.1111/j.1365-2133.2007.07682.x
27. Al‐Janabi A, Foulkes AC, Mason K, Smith CH, Griffiths CEM, Warren RB. Phenotypic switch to eczema in patients receiving biologics for plaque psoriasis: a systematic review. J Eur Acad Dermatol Venereol. 2020;34(7):1440–1448. doi:10.1111/jdv.16246
28. Papp KA, Menter MA, Raman M, et al. A randomized phase 2b trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br J Dermatol. 2016;174(6):1266–1276. doi:10.1111/bjd.14403
29. Scheinberg M, Machado LA, Ferreira SB, Michalany N, Michalany N. Successful treatment of ulcerated pyoderma gangrenosum with baricitinib, a novel JAK inhibitor. J Transl Autoimmun. 2021;4:100099. doi:10.1016/j.jtauto.2021.100099
30. Chovatiya R, Paller AS. JAK inhibitors in the treatment of atopic dermatitis. J Allergy Clin Immunol. 2021;148(4):927–940. doi:10.1016/j.jaci.2021.08.009
31. Fieke M, Rosenberg LL, Marie LA. Baricitinib treatment of severe chronic hand eczema: two case reports. Contact Dermatitis. 2022;86(5):419–421. doi:10.1111/cod.14039
32. Allam JP, Novak N. The pathophysiology of atopic eczema. Clin Exp Dermatol. 2006;31(1):89–93. doi:10.1111/j.1365-2230.2005.01980.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.