")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
A Case of Vitiligo Combined with Systemic Lupus Erythematosus Treated with Tofacitinib
Received 6 November 2023
Accepted for publication 6 March 2024
Published 20 March 2024 Volume 2024:17 Pages 707—711
DOI https://doi.org/10.2147/CCID.S448535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Qingxia Lin,1 Jinrong Zhu,2 Xuelei Gao3
1Department of Dermatology, Affiliated Hospital of Weifang Medical University, Weifang, Shandong, People’s Republic of China; 2Department of Central Pharmacy, Zhucheng People’s Hospital, Weifang, Shandong, People’s Republic of China; 3Department of Hepatopancreatobiliary Surgery, Affiliated Hospital of Weifang Medical University, Weifang, Shandong, People’s Republic of China
Correspondence: Xuelei Gao, Department of Hepatopancreatobiliary Surgery, Affiliated Hospital of Weifang Medical University, Weifang, Shandong, People’s Republic of China, Email [email protected]
Abstract: Vitiligo is a skin depigmentation disease resulting from melanocyte destruction and often co-occurring with autoimmune disorders like hyperthyroidism, alopecia areata, pernicious anemia, and systemic lupus erythematosus (SLE). Although various traditional treatments exist for vitiligo, their effectiveness varies considerably. This report presents a unique case of a vitiligo patient with concomitant systemic lupus erythematosus. Remarkably, after a 30-day course of treatment with tofacitinib, complete repigmentation of the white macular rash was achieved, and there were no adverse drug reactions. These findings provide compelling evidence for the efficacy and safety of oral JAK inhibitors, such as tofacitinib, in vitiligo treatment. Additionally, JAK inhibitors can yet be regarded as a promising new treatment option for vitiligo patients with concurrent autoimmune diseases.
Keywords: vitiligo, systemic lupus erythematosus, tofacitinib, JAK inhibitors
Introduction
Vitiligo is a common skin depigmentation disorder that significantly impacts patients’ appearance and quality of life. With a prevalence rate of 0.5–2%,1 vitiligo is easy to diagnose and difficult to treat. Current understanding suggests that vitiligo is an autoimmune disease characterized by the dysregulation of the adaptive immune response.2 Increasing studies have shown that CD8+ T cells and the cytokines they secrete, notably interferon-γ (IFN-γ), by activating the JAK-STAT pathway, appear to play a pivotal role in the autoimmunity of vitiligo.3
Tofacitinib, an oral Janus kinase (JAK) inhibitor, demonstrates the ability to inhibit lymphocyte-mediated damage to melanocytes by blocking the JAK-STAT signaling pathway.3 Based on this mechanism of action, we hypothesize that JAK inhibitors hold promise as targeted therapeutic agents for vitiligo. We report a case of vitiligo combined with SLE, who quickly re-pigmented after treatment with tofacitinib and experienced no adverse reactions. It is reported as follows.
Case Presentation
A 56-year-old female with stably controlled SLE was diagnosed 10 years prior and currently taking 5 mg/d oral prednisone. She followed up at the rheumatology clinic every six months. One month prior, a white macular rash appeared on the patient’s forehead with a rapidly expanding area. Dermatological examination revealed a white patch on the forehead measuring approximately 2.5cm×1.5 cm with clear borders (Figure 1). Reflectance confocal microscopy (RCM) revealed complete depigmentation of the basal layer of the epidermis (Figure 2). The final diagnosis was vitiligo. Relevant imaging and laboratory tests were performed, including frontal and lateral chest radiographs, electrocardiography, complete blood count, liver function tests, kidney function tests, plasma lipid levels, D-dimer, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibodies, anti-dsDNA antibodies, complements, thyroid antibody, immunoglobulins, antibodies to various infectious diseases such as syphilis, hepatitis B, hepatitis C, HIV, tumor markers such as CEA, CA199, AFP, and PPD test; no significant abnormalities were observed. Considering that the patient is currently using glucocorticoids to treat SLE, and she refused to add the dose of glucocorticoid to treat vitiligo. After obtaining the patient’s written informed consent, the patient was given 10 mg/d oral tofacitinib, without the combination of phototherapy and topical medication. After 30 days, the white macular rash was completely re-pigmented (Figure 3), the pigment granules in the basal layer of the epidermis returned to normal on RCM (Figure 4), and no significant abnormalities were found on imaging and laboratory examination, including frontal and lateral chest radiographs, complete blood count, liver function tests, kidney function tests, plasma lipid levels, D-dimer, hepatitis B, and PPD test. No recurrence was observed at the 6-month follow-up, and the condition of SLE is stable.
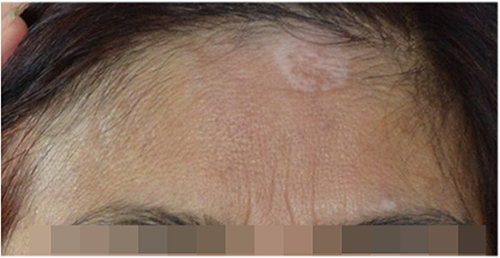 |
Figure 1 Before treatment, approximately 2.5cm × 1.5 cm white patches on the patient’s forehead. |
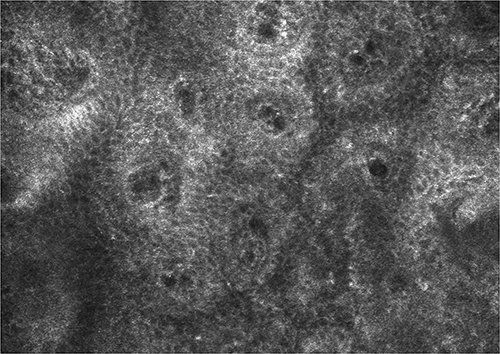 |
Figure 2 Before treatment, reflectance confocal microscopy (RCM) revealed complete depigmentation of the basal layer of the epidermis. |
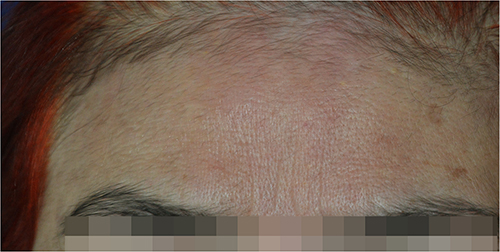 |
Figure 3 After 30 days after treatment, the white macular rash was completely re-pigmented. |
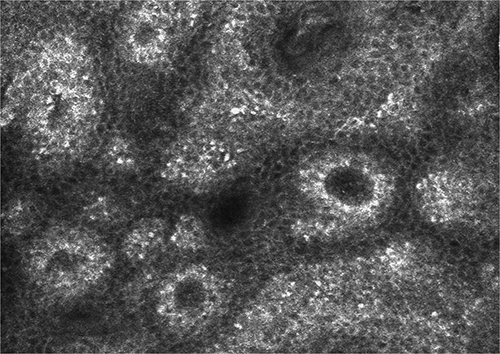 |
Figure 4 After 30 days after treatment, the pigment granules in the basal layer of the epidermis returned to normal on RCM. |
Discussion and Conclusion
Vitiligo is a prevalent skin disease characterized by the loss of pigment in the mucosa and epidermis of the affected area, leading to a significant impact on patients’ appearance and psychological well-being. The primary treatment goal for vitiligo is to control disease progression and achieve repigmentation of the white macular rash. Currently, the primary treatments for vitiligo include oral glucocorticoids, immunosuppressants, topical glucocorticoids, calcineurin inhibitors, vitamin D3 analogs, phototherapy, photosensitizers, and surgical interventions. However, treatment outcomes vary considerably among patients.4
The pathogenesis of vitiligo remains unclear, with several factors contributing to its development, including genetics, neuropsychiatric factors, melanocyte self-destruction, autoimmune factors, cytokine dysregulation, free radical damage, and trace element deficiencies. Among these factors, the autoimmune theory is widely accepted. Notably, about 23% of vitiligo patients also have one or more coexisting autoimmune diseases such as rheumatoid arthritis (RA), Sjögren’s syndrome, systemic lupus erythematosus (SLE), or inflammatory bowel disease (IBD),5 providing further support for the autoimmune nature of vitiligo. Autoimmune damage to melanocytes is considered the primary catalyst driving the progression of vitiligo. Extensive research has revealed the presence of a significant number of cytotoxic CD8+ T cells within the affected skin lesions of vitiligo patients. These cells secrete a range of inflammatory molecules, including interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α), granzyme B, and perforin, which specifically target and destroy melanocytes.6 IFN-γ plays a crucial role in activating the JAK-STAT pathway within keratinocytes, leading to the upregulation of the chemokine CXCL10.3 This, in turn, promotes the recruitment of CD8+ cytotoxic T lymphocytes, resulting in autoimmune dysregulation and subsequent melanocyte destruction, ultimately leading to the development of vitiligo. Remarkably, increased expression levels of JAK1 and JAK3 have been observed in vitiligo lesions.7 Moreover, the level of JAK1 was significantly higher in vitiligo patients, and there was a decline in the level of JAK1 after treatment,8 further supporting the important role of the JAK-STAT signaling pathway in the pathogenesis of vitiligo.
Capitalizing on the ability to block the JAK-STAT signaling pathway, JAK inhibitors have emerged as innovative therapeutic options for autoimmune diseases like rheumatoid arthritis, Crohn’s disease, inflammatory bowel disease, alopecia areata, psoriasis vulgaris, and atopic dermatitis.9 JAK inhibitors, such as tofacitinib and ruxolitinib, have shown promise in treating vitiligo by targeting key mechanisms involved in the disease.6 The possible mechanisms of JAK inhibitors in treating vitiligo include the following: Firstly, they inhibit the activity of cytokines, including interleukins, interferons, and growth factors, reduce the recruitment of CD8+ T cells, ameliorate melanocyte destruction, so promote repigmentation in vitiligo.10 Subsequently, they modulate the immune system by suppressing immune cell activation and proliferation, potentially reducing the autoimmune response against melanocytes.11 Moreover, they may promote the survival and function of existing melanocytes while stimulating the migration and differentiation of melanocyte precursor cells from hair follicles to repopulate depigmented areas.
Recent clinical studies have demonstrated the efficacy of topical ruxolitinib cream in the treatment of vitiligo,12,13 however, there remains a dearth of research regarding the use of oral JAK inhibitors for vitiligo treatment,14 and requires combined with phototherapy.10 Tofacitinib is an oral inhibitor of JAK1 and JAK3, the safety and tolerability of tofacitinib in systemic lupus erythematosus have been confirmed.15 In this particular case, we observed rapid onset of action, significant efficacy, and high safety with the use of tofacitinib, highlighting it as a promising treatment option for vitiligo patients with concurrent autoimmune diseases such as SLE. However, further clinical research is needed to support it.
Data Sharing Statement
Data would be available upon requests to corresponding author.
Consent Statement
The patients in this manuscript have given written informed consent to the publication of her clinical details and accompanying images. Institutional approval was not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kroger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206–1212. PMID: 22458952. doi:10.1111/j.1365-4632.2011.05377.x
2. Bergqvist C, Ezzedine K. Vitiligo: a focus on pathogenesis and its therapeutic implications. J Dermatol. 2021;48(3):252–270. PMID: 33404102. doi:10.1111/1346-8138.15743
3. Phan K, Phan S, Shumack S, Gupta M. Repigmentation in vitiligo using janus kinase (JAK) inhibitors with phototherapy: systematic review and Meta-analysis. J DermatolTreat. 2022;33(1):173–177. PMID: 32096671. doi:10.1080/09546634.2020.1735615
4. Daniel BS, Wittal R. Vitiligo treatment update. Australas J Dermatol. 2015;56(2):85–92. PMID: 25495880. doi:10.1111/ajd.12256
5. Lee JH, Ju HJ, Seo JM, et al. Comorbidities in patients with vitiligo: a systematic review and meta-analysis. J Invest Dermatol. 2023;143(5):777–789.e6. PMID: 36574529. doi:10.1016/j.jid.2022.10.021
6. Frisoli ML, Essien K, Harris JE. Vitiligo: mechanisms of pathogenesis and treatment. Annu Rev Immunol. 2020;38:621–648. PMID: 32017656. doi:10.1146/annurev-immunol-100919-023531
7. Abdel Motaleb AA, Tawfik YM, El-Mokhtar MA, et al. Cutaneous jak expression in vitiligo. J Cutan Med Surg. 2021;25(2):157–162. PMID: 33174479. doi:10.1177/1203475420972340
8. Nada HR, El Sharkawy DA, Elmasry MF, et al. Expression of Janus Kinase 1 in vitiligo & psoriasis before and after narrow band UVB: a case-control study. Arch Dermatol Res. 2018;310(1):39–46. PMID: 29127481. doi:10.1007/s00403-017-1792-6
9. Solimani F, Meier K, Ghoreschi K. Emerging topical and systemic JAK inhibitors in dermatology. Front Immunol. 2019;10:2847. PMID: 31849996; PMCID: PMC6901833. doi:10.3389/fimmu.2019.02847
10. Joshipura D, Plotnikova N, Goldminz A. Importance of light in the treatment of vitiligo with JAK-inhibitors. J DermatolTreat. 2018;29(1):98–99. PMID: 28581823. doi:10.1080/09546634.2017.1339013
11. Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nat Med. 2014;20(9):1043–1049. PMID: 25129481. doi:10.1038/nm.3645
12. Rothstein B, Joshipura D, Saraiya A, et al. Treatment of vitiligo with the topical janus kinase inhibitor ruxolitinib. J Am Acad Dermatol. 2017;76(6):1054–1060 e1051. PMID: 28390737. doi:10.1016/j.jaad.2017.02.049
13. Relke N, Gooderham M. The use of janus kinase inhibitors in vitiligo: a review of the literature. J Cutan Med Surg. 2019;23(3):298–306. PMID: 30902022. doi:10.1177/1203475419833609
14. Craiglow BG, King BA. Tofacitinib citrate for the treatment of vitiligo: a pathogenesis-directed therapy. JAMA Dermatol. 2015;151(10):1110–1112. PMID: 26107994. doi:10.1001/jamadermatol.2015.1520
15. Hasni SA, Gupta S, Davis M. Phase 1 double-blind randomized safety trial of the Janus kinase inhibitor tofacitinib in systemic lupus erythematosus. Nat Commun. 2021;12(1):3391. PMID: 34099646. doi:10.1038/s41467-021-23361-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.