")
Back to Journals » Open Access Emergency Medicine » Volume 16
A Case Study on Unreported First Probable Human Rabies Following Honey Badger in Somalia
Authors Ali Osman UM, Turfan S, Farah Yusuf Mohamud M
Received 12 September 2023
Accepted for publication 24 January 2024
Published 30 January 2024 Volume 2024:16 Pages 15—18
DOI https://doi.org/10.2147/OAEM.S439996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Ubah Mumin Ali Osman,1 Selim Turfan,1 Mohamed Farah Yusuf Mohamud1– 3
1Emergency Department, Mogadishu Somali Turkey Training and Research Hospital, Mogadishu, Somalia; 2Faculty of Medicine, Mogadishu University, Mogadishu, Somalia; 3Tayo Institute for Health and Development, Mogadishu, Somalia
Correspondence: Mohamed Farah Yusuf Mohamud, Emergency Department, Mogadishu Somali Turkey Training and Research Hospital, Digfer Street, Hodan District, Mogadishu, Somalia, Tel +252615591689, Email [email protected]
Abstract: Rabies is a neglected zoonotic disease caused by a virus. It is an acute progressive neurological disease that affects people in many parts of the world, especially in low income countries including Somalia and it is always lethal once symptoms appear without immediate post-exposure prophylaxis (PEP). Nearly half of rabies cases occur in children. This case report presents a tragic and unique clinical scenario involving a 14-year-old boy from a rural area in Somalia who presented to our tertiary hospital after a bite from a honey badger. The patient’s younger sister, who was also bitten by the same honey badger, sadly succumbed to the disease two weeks prior. This report aims to contribute to the medical literature by highlighting the challenges faced in diagnosing and managing rabies in resource-constrained settings.
Keywords: rabies, honey badger, post-exposure prophylaxis, zoonotic disease, Somalia
Introduction
Rabies is a neglected, severe acute progressive neurological disease that is always lethal once symptoms appear without immediate post-exposure prophylaxis (PEP).1 In underdeveloped countries, where rabies is still a serious public health issue, the majority of human rabies deaths were associated with dog bites or scratches.2 In more than 150 nations and territories worldwide, rabies is one of the most significant viral zoonotic illnesses that can be prevented by vaccination and is responsible for 50,000 to 70,000 annual human fatalities.3 Twenty-one cases of rabies were seen at a tertiary facility in Ghana over a 25 month period, with more than half of cases aged >18 years.4 When rabies is widely distributed, it poses a public health risk to the local population through infected wildlife. For example, the Chinese ferret badger (Melogale moschata) has been associated with human rabies for several years.5 It was assumed that transmission happened either naturally within the population or as a result of spillover from other reservoirs like foxes, dogs, or jackals. Rabies has also been observed in other related subspecies, including honey badgers (Mellivora capensis) in Africa and European badgers (Meles meles) in Europe.6,7 Here, we parent reported a patient had experienced a rabies after of honey badger on her left leg four weeks prior to presentation, for which no antirabies prophylaxis was given. The patient died within two days of arrival in hospital. We hereby report a case involving a patient who suffered an encounter with a honey badger, resulting in a subsequent occurrence of rabies. This incident took place four weeks prior to the patient’s presentation at our hospital. Notably, no post exposure prophylaxis for rabies was administered following the incident. Regrettably, despite medical interventions, the patient’s condition deteriorated rapidly, and passed away within two days of being admitted to the hospital.
Case Report
On May 27, 2023, a 14-year-old boy from a rural area in Somalia came to the emergency room with complaining of agitation, high-grade fever, photophobia, and hydrophobia after a bite of a honey badger before four weeks. His younger sister, who is 4 years old, was attacked by the same honey-budger, and she died 2 weeks after the bite of the honey badger. The Young boy has no history of vaccination due to the lack of medical service in that area. No history of epilepsy or other chronic diseases. The boy and his sister slept in front of their room, and then a honey-budger attacked. First, the honey-budger bit the boy and then jumped on the little sister’s neck. Their mother screamed and killed the honey badger. The family does not seek any medical care. Two weeks later, his sister developed agitation and an altered level of consciousness. Twenty-four hours later, the little girl passed away. One week after the girl died, the young boy developed high-grade fever, photophobia, and hydrophobia. The family searched for medical care in a nearby regional hospital, where he was given tetanus toxoid, antibiotics, and rabies post-exposure prophylaxis (PEP). On May 27, 2023, 4 weeks after the bite, the young boy was transferred to our tertiary hospital located in the capital city of Somalia. The young baby presented to our hospital with agitation, a high-grade fever, photophobia, and hydrophobia. During the physical examination, an old healed superficial wound was observed on the anterior aspect of the left leg. The wound appeared jagged in nature, indicating irregular edges. It seemed to have previously healed without any complications (Figure 1). The neck was supple, and Kernig’s sign was negative. A presumptive diagnosis of rabies was made, and the boy was admitted to the intensive care unit. Eight hours later, the vital signs and consciousness levels of the boy declined. After 48 hours in the ICU, he passed away. No more testing was carried out.
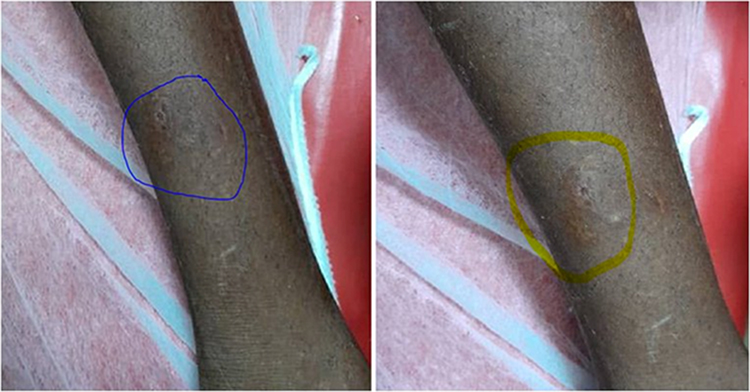 |
Figure 1 Shows a superficial, jagged wound on the anterior aspect of the left leg. both the blue and yellow areas indicates the healed area of honey badger bite. |
Discussion
Rabies is a neglected and zoonotic viral disease that affects the central nervous system and transmitted through the saliva of infected animals.1,2 Although effective human vaccines and immunoglobulins exist for rabies, these are often not readily available or accessible to those in need. The majority of human cases are due to dog bites. Analysis of 20 studies conducted in Africa, with a total of 48,092 animal bite victims, found that dog bites accounted for 91.9% of exposures, 2.9% of bites were from cats, 0.8% of bites were from jackals, and 4.4% of bites were from other animals such monkeys, donkeys, horses, rats, pigs, rabbits, honey badgers, kudus, goats, calves, elands, and hyaenas.8
Audu et al documented two instances of rabies in individuals who sought medical care but did not receive post-exposure prophylaxis (PEP).9 Both cases were bitten by a stray dog and presented with symptoms including fever, paresthesia of the right hand, difficulty swallowing, hypersalivation, photophobia, dyspnea, and hydrophobia. A presumptive diagnosis of rabies was made, and they passed away with in 48 hours of hospitalization. Our case initially presented with agitation, high-grade fever, photophobia, and hydrophobia after a bite of a honey badger before four weeks. After 48 hours of hospitalization in the ICU, he passed away. No further tests were conducted.
Since honey badgers are not normally known to contribute to the transmission of rabies, this incident emphasizes the significance of treating all wild animals as potential carriers of the disease. As early treatment is essential in preventing the development of clinical symptoms, the patient’s delayed presentation and absence of pre-exposure prophylaxis contributed to the disease’s progression. Additionally, it highlights the need for continuing education and awareness about the dangers of rabies, the value of vaccination, and the necessity of receiving quick medical assistance in the event of an animal bite or scratch.
This case report emphasizes the severe impact of rabies in both local and global contexts, primarily due to restricted healthcare accessibility and delayed administration of post-exposure prophylaxis. The delayed arrival of the patient, absence of preventive measures, and limited treatment alternatives significantly contributed to the unfortunate outcome. This situation underscores the immediate requirement for enhanced awareness, preventive measures, and increased availability of vaccinations to effectively combat rabies in resource-limited regions.
In conclusion, we believe that this case report provides valuable insights into the challenges faced in diagnosing and managing rabies in rural Somalia. By sharing information about this tragic case, we hope to raise awareness among healthcare professionals and policymakers regarding the importance of preventive measures, early recognition, and access to appropriate medical interventions for rabies.
Data Sharing Statement
We declared that we had full access to all of the data in this case report, and we take complete responsibility for the integrity of the data. All original data are available in the Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia. Data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
Based on the regulations of the review board of the Mogadishu Somali Turkish Training and Research Hospital, institutional review board approval is not required for case reports.
Consent for Publication
Written informed consent had obtained by the patient’s father to have the case details and any accompanying images published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, case presentation, or in all these areas; took part in drafting, revising or critically reviewing the case; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We declare that we have not received any financial support.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Rabies. Available from: https://www.who.int/news-room/fact-sheets/detail/rabies.
2. Hampson K, Coudeville L, Lembo T, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709. doi:10.1371/journal.pntd.0003709
3. World Health Organization. WHO Expert Consultation on Rabies: Second Report. World Health Organization; 2013.
4. Nyasulu PS, Weyer J, Tschopp R, et al. Rabies mortality and morbidity associated with animal bites in Africa: a case for integrated rabies disease surveillance, prevention and control: a scoping review. BMJ open. 2021;11(12):e048551. doi:10.1136/bmjopen-2020-048551
5. Zhenyu G, Zhen W, Enfu C, et al. Human rabies cluster following badger bites, People’s Republic of China. Emerg Infect Dis. 2007;13(12):1955. doi:10.3201/eid1312.070465
6. Pfukenyi DM, Pawandiwa D, Makaya PV, Ushewokunze-Obatolu U. A retrospective study of wildlife rabies in Zimbabwe, between 1992 and 2003. Trop Anim Health Prod. 2009;41:565–572. doi:10.1007/s11250-008-9224-4
7. Wandeler AI, Nadin-Davis SA, Tinline RR, Rupprecht CE. Rabies epidemiology: some ecological and evolutionary perspectives. Curr Top Microbiol Immunol. 1994;187:297–324. doi:10.1007/978-3-642-78490-3_16
8. Audu SW, Mshelbwala PP, Jahun BM, Bouaddi K, Weese JS. Two fatal cases of rabies in humans who did not receive rabies postexposure prophylaxis in Nigeria. Clin Case Rep. 2019;7(4):749. doi:10.1002/ccr3.1972
9. Amoako YA, El-Duah P, Sylverken AA, et al. Rabies is still a fatal but neglected disease: a case report. J Med Case Rep. 2021;15(1):1–6. doi:10.1186/s13256-021-03164-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.