")
Back to Journals » Clinical Interventions in Aging » Volume 19
A Comparison Between Two Different Definitions of Contrast-Associated Acute Kidney Injury for Long-Term Mortality in Patients with Chronic Kidney Disease Undergoing Coronary Angiography
Authors Feng W, Zhou J, Lun Z, Zhou D, Li P , Ye J
Received 20 December 2023
Accepted for publication 14 February 2024
Published 19 February 2024 Volume 2024:19 Pages 303—311
DOI https://doi.org/10.2147/CIA.S452882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Wenwei Feng,* Jiancong Zhou,* Zhubin Lun, Dianhua Zhou, Peiwen Li, Jianfeng Ye
Department of Cardiology, Dongguan Hospital of Guangzhou University of Chinese Medicine, Dongguan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianfeng Ye, Department of Cardiology, Dongguan Hospital of Guangzhou University of Chinese Medicine, Dongguan, Guangdong, People’s Republic of China, Email [email protected]
Background: Contrast-associated acute kidney injury (CA-AKI) is a prevalent complication following coronary angiography (CAG). However, there is ongoing controversy surrounding its precise definition. Although previous studies have demonstrated the successful application of appropriate definitions in managing high-risk CA-AKI patients, there remains limited research on the association between different definitions and prognosis specifically in patients with chronic kidney disease (CKD).
Methods: A total of 4197 CKD patients undergoing coronary angiography (CAG) were included in this study. Two definitions of contrast-associated acute kidney injury (CA-AKI) were used: CA-AKIA, which was defined as an increase of ≥ 0.5 mg/dL or > 25% in serum creatinine (SCr) from baseline within 72 hours after CAG, and CA-AKIB, which was defined as an increase of ≥ 0.3 mg/dL or > 50% in SCr from baseline within 48 hours after CAG. Cox regression analysis was employed to assess the association between these two definitions and long-term mortality. Additionally, population attributable risks (PARs) were calculated to evaluate the impact of CA-AKI definitions on long-term prognosis.
Results: During the median follow-up period of 4.70 (2.50– 7.78) years, the overall long-term mortality was 23.6%, and the long-term mortality in patients with CA-AKI according to both CA-AKIA and CA-AKIB criteria were 33.5% and 33.8%, respectively. We found that CA-AKIA (HR: 1.45, 95% CI: 1.23– 1.70, p< 0.001) and CA-AKIB (HR: 1.44, 95% CI: 1.23– 1.69, p< 0.001) were associated with long-term mortality. The PARs were the highest for CA-AKIA (5.87%), followed by CA-AKIB (5.70%).
Conclusion: Contrast-associated acute kidney injury (CA-AKI) is a frequently observed complication in CKD patients undergoing coronary angiography (CAG), and both definitions of CA-AKI are significantly correlated with a poor long-term prognosis. Consequently, in the clinical management of CKD patients, it is crucial to prioritize CA-AKI, irrespective of the specific CA-AKI definition used.
Keywords: contrast-associated acute kidney injury, chronic kidney disease, definitions, long-term mortality, population attributable risks
Introduction
With the aging population, the incidence of coronary heart disease increases. Contrast-associated acute kidney injury (CA-AKI) is a common complication of coronary angiography (CAG) and is associated with a poor prognosis. Previous studies have shown that the incidence of CA-AKI is between 5–20%, with high rates of rehospitalization, dialysis, and mortality.1–4 However, the diversity in the definition of CA-AKI makes it challenging for clinicians to effectively recognize and address this issue in clinical practice. Different definitions of CA-AKI have varying incidence rates and prognoses.5 For instance, the Acute Kidney Injury Network (AKIN) criteria have demonstrated better efficacy in predicting long-term mortality in patients with ST-elevation myocardial infarction (STEMI).6 For diabetic patients, the definition of CA-AKIA (an increase in serum creatinine levels by 0.3 mg/dl or 50% within 72 hours after the procedure) is more suitable as it is associated with poorer clinical outcomes and higher population attributable risks (PARs).7 Furthermore, the European Society of Urogenital Radiology definition of CA-AKI can better identify high-risk patients with poor prognosis at an early stage in elderly and heart failure patients.8,9 It is well known that chronic kidney disease (CKD) is a risk factor for CA-AKI. CA-AKI patients with CKD have a 36% all-cause mortality rate and an increased risk of renal dialysis treatment as their estimated glomerular filtration rate (eGFR) decreases.10–12 However, few studies have explored the applicable definition of CA-AKI in patients with CKD. Therefore, this article aims to evaluate the association between different definitions of CA-AKI and long-term mortality in CKD patients after coronary angiography.
Methods
Study Design and Population
This study is a single-center retrospective observational study conducted at Dongguan TCM Hospital. Between January 2015 and January 2023, a total of 4197 consecutive patients, aged 18 years or older, who were diagnosed with CKD, underwent coronary angiography and were included in the study. All patients underwent percutaneous coronary intervention (PCI) and coronary angiography (CAG) following standard guidelines. Exclusion criteria for the study included pregnancy, lactation, recent intravascular administration of contrast media within 7 days before or 3 days after the operation, non-use of low osmotic pressure contrast media, cardiovascular surgery or intravascular repair, end-stage renal disease or kidney replacement, creatinine deficiency before or after the operation, malignant tumor, and non-use of isotonic saline for hydration. The study protocol was designed following the principles outlined in the Declaration of Helsinki and received approval from the Ethics Committee of Dongguan TCM Hospital (approval number: PJ (2023) 31).
Endpoint and Definitions
The primary outcome in this article was long-term all-cause mortality. Our study calculated the estimated glomerular filtration rate (eGFR) by applying the Modification of Diet in Renal Disease (MDRD) formula. The definition of CKD was eGFR ≤60mL/min/1.73 m2.13,14 CA-AKIA was defined as an increase ≥0.5 mg/dL or >25% in SCr from baseline within 72 hours after CAG, and CA-AKIB was defined as an increase ≥0.3 mg/dL or >50% in serum creatinine (SCr) from baseline within 48 hours after CAG.15,16 Serum creatinine (SCr) concentrations were measured on days 1, 2, and 3 in all patients before and after surgery. Serum creatinine (SCr) from the day before surgery was used as baseline creatinine. Chronic heart failure (CHF) was defined as Killip classes II–IV or New York Heart Association (NYHA) classes III–IV.10 Anemia was confirmed by gender and hematocrit (male’s hematocrit below 39% and female’s hematocrit below 36%). Diabetes was defined as a previous diagnosis of diabetes or an HbAlc level≥6.5.
Statistical Analysis
Continuous variables were reported as mean ± standard deviation (SD) or median ± interquartile range (IQR). To compare differences between two independent samples (with and without CA-AKI) using different definitions, Wilcoxon rank-sum tests or Student’s t-tests were employed. Categorical variables, expressed as counts (percentages), were analyzed using the Chi-square test or Fisher’s exact test to assess differences. In the initial step, univariate logistic regression models were utilized to identify predictors of CA-AKIA and CA-AKIB. The results of this analysis are presented as hazard ratios with corresponding 95% confidence intervals (CIs). Additionally, multivariate logistic regression analysis was performed. Cumulative mortality rates based on various definitions were calculated using Kaplan-Meier analysis, and differences between survival curves were assessed using the Log rank test. A multivariate Cox regression model adjusting for other risk factors such as age, diabetes, CHF, and stroke was used to examine the relationship between CA-AKI and long-term mortality. The adjusted risk factors in the univariate Cox regression analysis were selected based on previous studies and clinical significance. Two separate multivariate Cox proportional hazard regression models were applied for each definition of CA-AKI. Population attributable risk (PAR) was computed using the equation: PAR = P(HR-1)/[1+P(HR-1)], where p represents the incidence of CA-AKI according to different definitions in our database. The standard error of the PAR was estimated using the delta method. A two-sided probability value less than 0.05 was considered statistically significant. All data analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC) and R software (version 4.0.0; R Core Team, Vienna, Austria).
Result
Patient Characteristics
A total of 4197 patients who received coronary angiography were ultimately included in the analysis. The baseline characteristics were shown in Table 1. The overall mean age was 67.56 ± 10.20 years, and 1141 (27.2%) patients were older than 75 years. There were 1009 (24.0%) patients with CHF, 2885 (68.7%) patients with hypertension, and 876 (20.9%) patients with AMI. A total of 2492 (59.4%) patients underwent PCI.
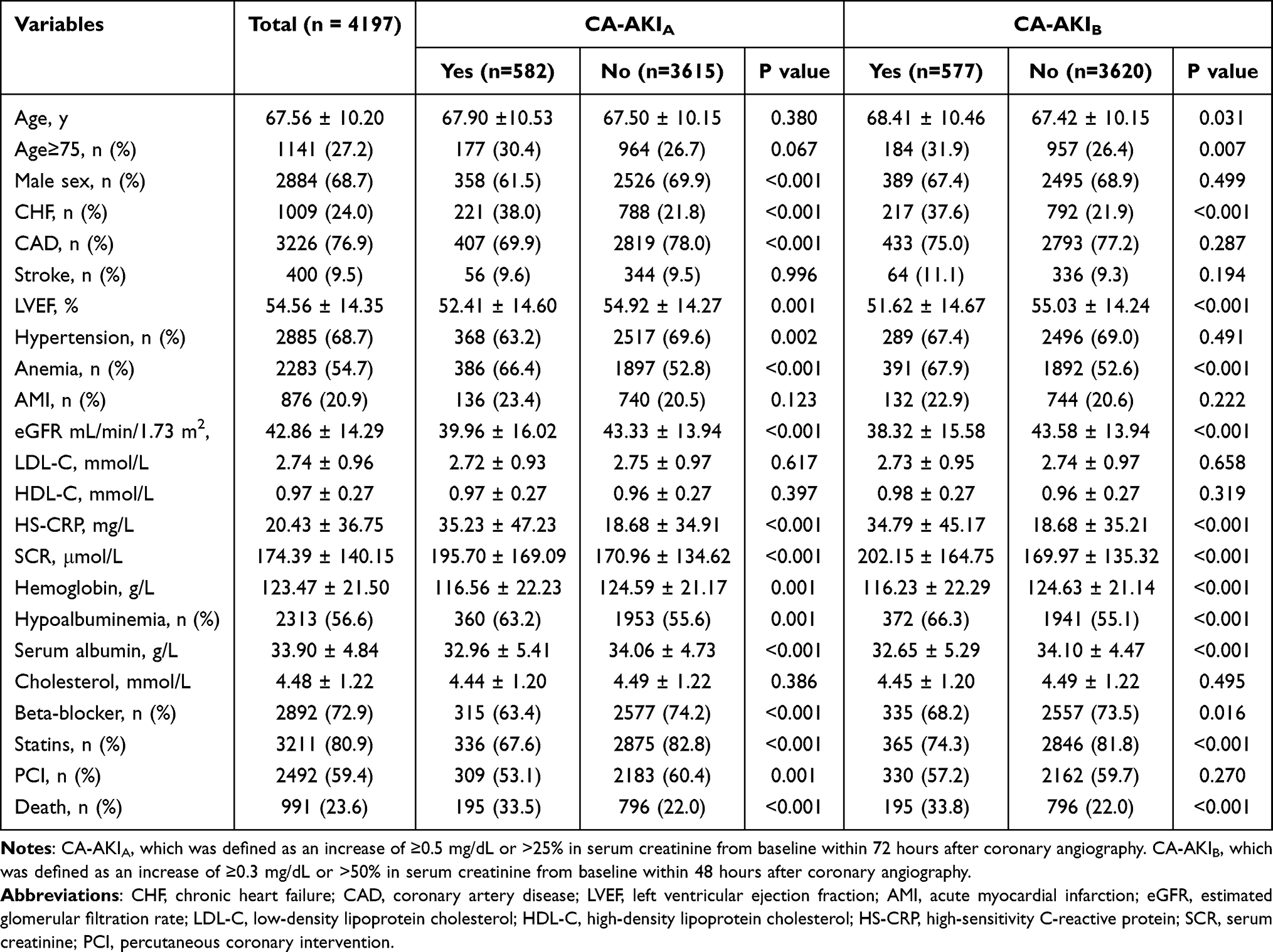 |
Table 1 Baseline Characteristics |
Incidence of CA-AKI by the CA-AKIA and CA-AKIB Criteria
According to the contrast-induced acute kidney injury (CA-AKIA) criteria, CA-AKI occurred in 582 patients (13.9%), while according to the CA-AKIB criteria, CA-AKI occurred in 577 patients (13.7%). However, regardless of the definition of contrast-induced acute kidney injury, patients with CA-AKI were older, had reduced left ventricular ejection fraction (LVEF), and had more underlying diseases. The usage of beta-blockers and statins was lower in patients with CA-AKIA or CA-AKIB. According to the CA-AKIB criteria, no significant association was found between hypertension and coronary artery disease (CAD) in patients with CA-AKI compared to non-CA-AKI patients.
Incidence and Predictors of Long‑term Mortality
During a median follow-up period of 4.70 (2.50–7.78) years, the overall long-term mortality rate was 23.6%. Specifically, among patients with CA-AKI according to both CA-AKIA and CA-AKIB criteria, the long-term mortality rates were 33.5% and 33.8%, respectively. Regardless of the definition of CA-AKI, Kaplan-Meier curves showed that the long-term prognosis of patients with CA-AKI was worse than that of those without CA-AKI according to both CA-AKI definitions (log-rank p<0.01; Figure 1).
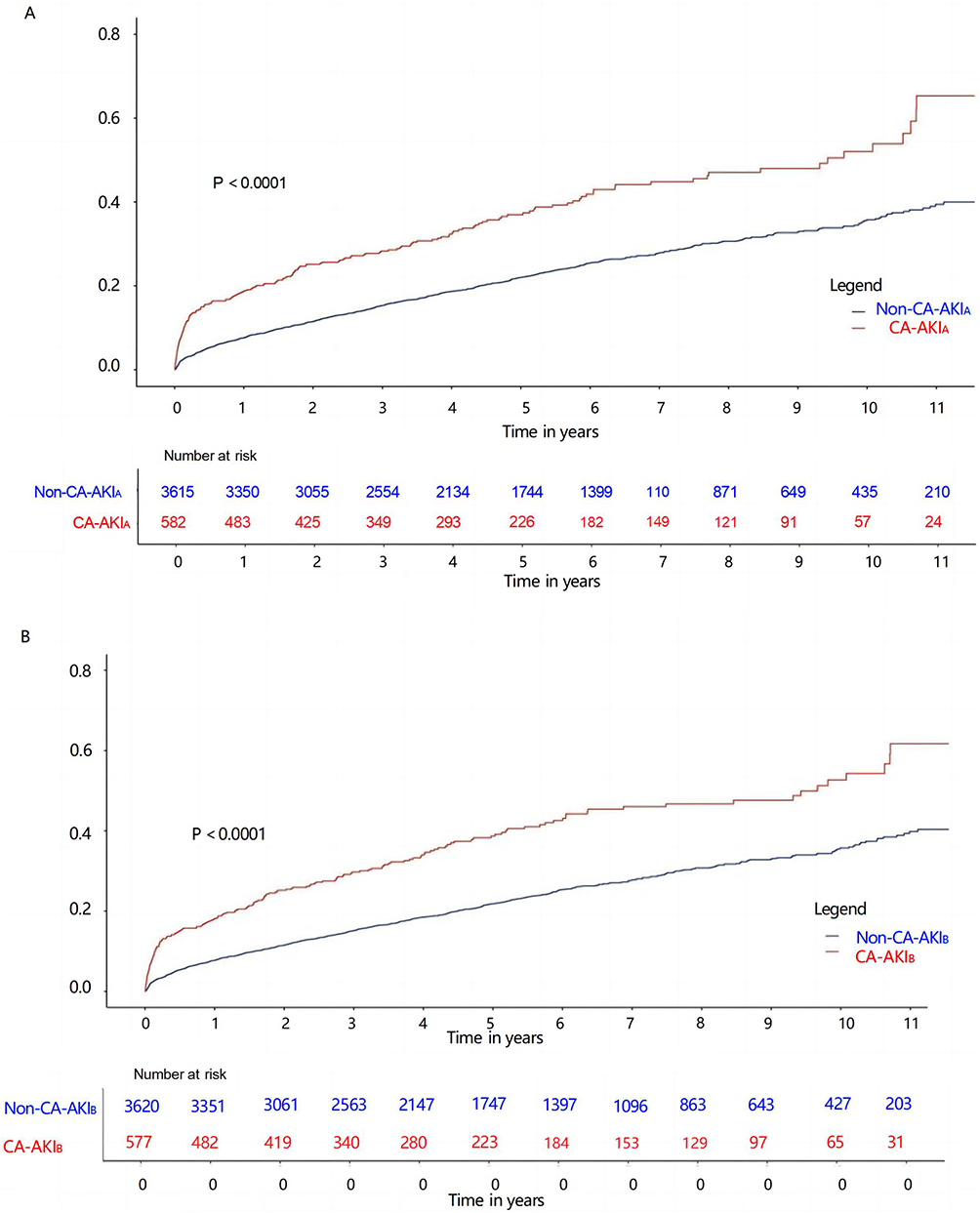 |
Figure 1 Kaplan-Meier curves for the long-term prognosis of patients with CA-AKI and without CA-AKI. (A) Kaplan-Meier for the long-term prognosis of patients with CA-AKIA and without CA-AKIA. (B) Kaplan-Meier for the long-term prognosis of patients with CA-AKIB and without CA-AKIB. Notes: CA-AKIA, which was defined as an increase of ≥0.5 mg/dL or >25% in serum creatinine from baseline within 72 hours after coronary angiography. CA-AKIB, which was defined as an increase of ≥0.3 mg/dL or >50% in serum creatinine from baseline within 48 hours after coronary angiography. |
Table 2 and Figure 2 present the results of univariate and multivariate analyses of risk factors for long-term mortality. The analyses revealed several independent predictive factors associated with long-term mortality, including age, PCI, DM, CHF, anemia, and CA-AKI. Notably, CA-AKI was associated with an increased risk of long-term mortality. Both CA-AKIA and CA-AKIB increased the risk of long-term mortality by approximately 1.45 times (95% CI 1.23–1.70 and 95% CI 1.23–1.69, respectively).
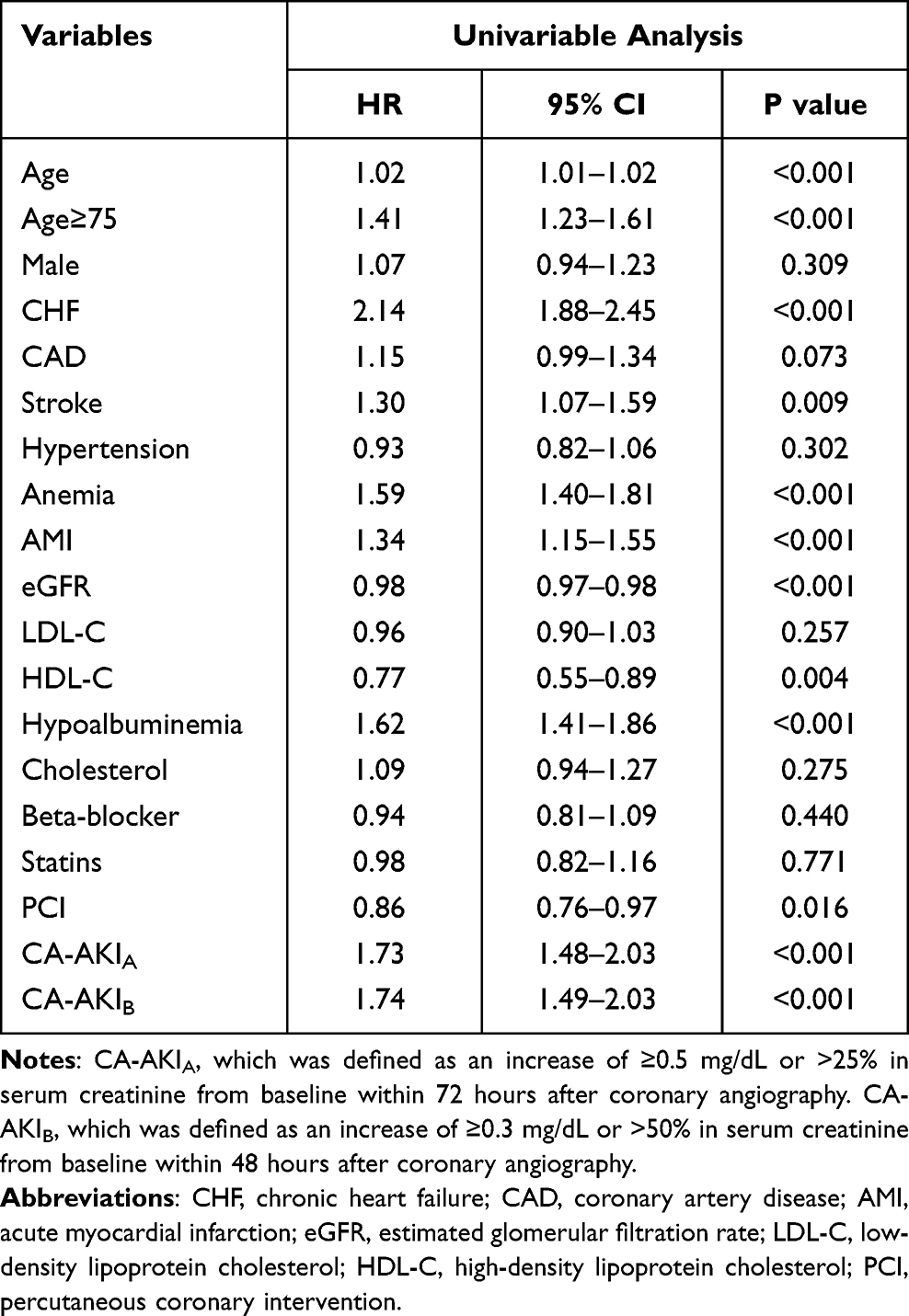 |
Table 2 Univariable Analysis of Risk Factors for Long-Term Mortality |
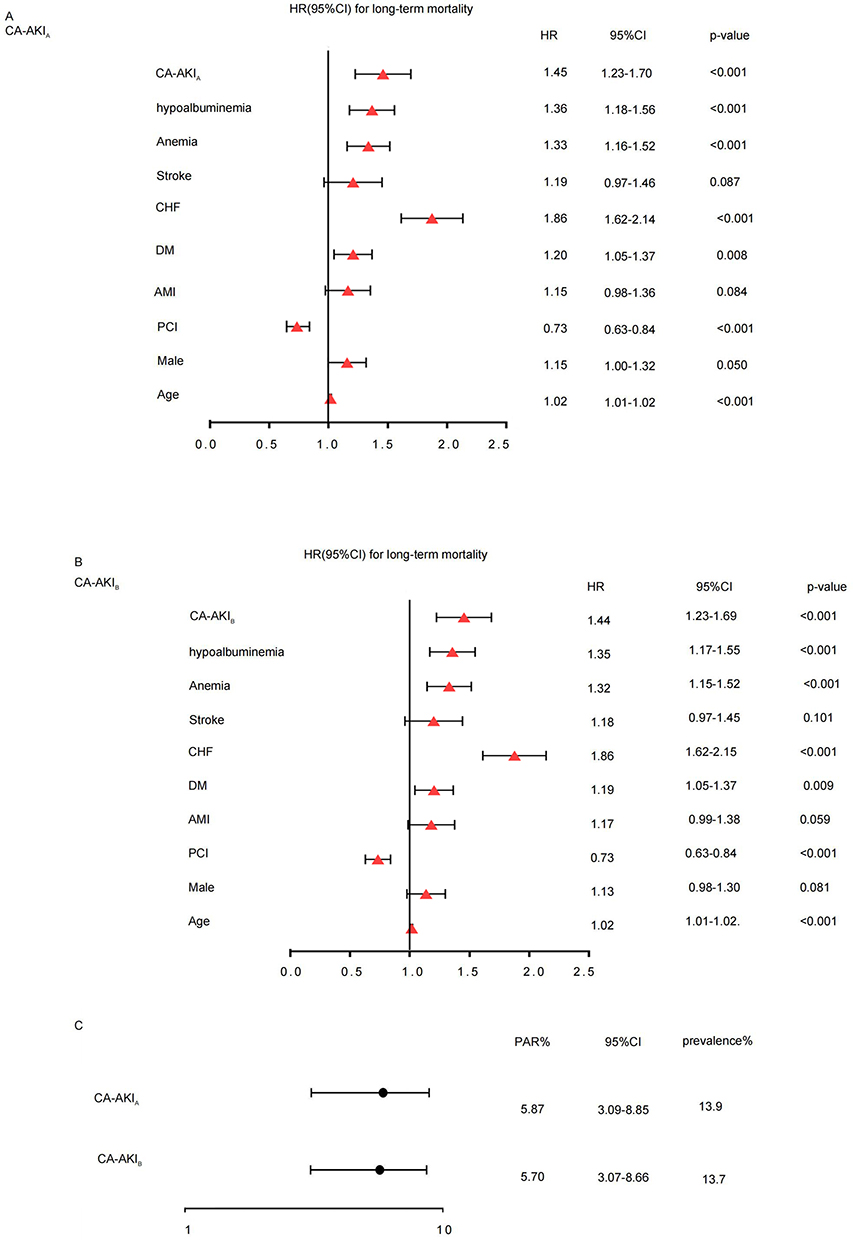 |
Figure 2 HR(95% CI) for long-term mortality. (A) HR(95% CI) for long-term mortality of CA-AKIA. (B) HR(95% CI) for long-term mortality of CA-AKIB. (C) The comparison of CA-AKIA and CA-AKIB. Abbreviation: PAR, the population attributable risk. Notes: CA-AKIA, which was defined as an increase of ≥0.5 mg/dL or >25% in serum creatinine from baseline within 72 hours after coronary angiography. CA-AKIB, which was defined as an increase of ≥0.3 mg/dL or >50% in serum creatinine from baseline within 48 hours after coronary angiography. |
PARs of CA‑AKI by CA‑AKIA and CA‑AKIB Criteria
Among the two definitions of CA-AKI, the prevalence of CA-AKIA was 13.9%, while the prevalence of CA-AKIB was 13.7%. The population attributable risk (PAR) for CA-AKIA was 5.87% (95% CI 3.09–8.85%), and for CA-AKIB it was 5.70% (95% CI 3.07–8.66%) (Figure 2).
Discussion
We are the first to investigate the relationship between the definition of CA-AKI and long-term mortality in CKD patients. Our findings demonstrate that regardless of the definition used, CA-AKI is associated with increased long-term mortality. Additionally, our study identifies age, PCI, DM, CHF, and anemia as independent risk factors for long-term mortality in CKD patients undergoing CAG.
The incidence of CA-AKIA in our study was slightly lower than that of CA-AKIB, as well as their respective mortality rates. However, our study observed a higher incidence compared to previous reports, which can be attributed to the inclusion of CKD patients.17,18 CKD is a known significant risk factor for CA-AKI and is often incorporated into prediction models.19,20 Furthermore, different definitions of CA-AKI exhibit variations in incidence and mortality, a finding also supported by Wang et al’s study,8 affirming our results.
Additionally, our study shows that CA-AKIA and CA-AKIB increase the risk of long-term mortality by approximately 1.45 times and 1.44 times, respectively. This aligns with previous research indicating that different definitions of CA-AKI yield varying risks. Centola et al discovered that different definitions of CA-AKI lead to different long-term prognostic risks among 402 STEMI patients.6 They found that CA-AKI defined by the AKIN standard increased the risk of long-term mortality by 9.70 times, which is higher than our results, likely due to disparate follow-up durations. In our study, the median follow-up period was 4.7 years, while Centola’s study followed patients for only 12 months. Similarly, He et al identified different definitions of CA-AKI as having distinct long-term prognoses in PCI patients, with AKI defined by AKIN criteria increasing the risk of death by 2.2 times,9 closely resembling our findings. Wang et al conducted similar studies in patients with AMI, HF, and diabetes, further corroborating our results,7,8,21 adding credibility to our findings.
Furthermore, our study reveals that the population attributable risks (PAR) of CA-AKIA and CA-AKIB are 5.87% and 5.70%, respectively. However, Wang et al’s study found that the PAR of CA-AKIA (an increase ≥0.5 mg/dl or >25% in SCr) was higher than that of CA-AKIB (an increase of ≥0.3 mg/dl or >50% in SCr),8 which differs from our results. The discrepancy can be attributed to the inclusion of CHF patients in Wang’s analysis, while our study focused on CKD patients. Moreover, previous studies have demonstrated that in patients with diabetes, CA-AKIA (an increase of ≥3 mg/dl or >50% in SCr) has a higher PAR. This indicates that the same definition of CA-AKI can yield varying PARs in different patient populations, underscoring the importance of tailoring the definition for each patient.7 In our study, different definitions of CA-AKI resulted in similar PARs, emphasizing the need to prevent and treat CA-AKI in CKD patients. CA-AKI may be a significant risk factor for long-term mortality rather than an intermediary factor, aligning with Mehran’s recently described viewpoint.22 Lassnigg et al’s research also supports this perspective, finding that even small fluctuations in serum creatinine are significantly associated with death.23
The pathogenesis of CA-AKI primarily involves hemodynamic changes in the kidney, the toxic effect of contrast agents on renal tubular cells, and oxidative stress. CKD reduces renal cell tolerance to toxins, increasing the risk of CA-AKI. Consequently, our findings highlight the need to prioritize attention and treatment for CA-AKI in CKD patients. While current guidelines recommend evaluating CA-AKI risk and administering hydration therapy to high-risk populations before CAG,24 there is no mention of CA-AKI prevention specifically for CKD patients. Recent studies have identified that preoperative simplified rapid hydration can effectively reduce the risk of CA-AKI in CKD patients.25
Limitations
Several limitations were identified in this study. Firstly, the study solely focused on patients with CKD, and therefore, caution should be exercised when extrapolating the findings to the general population. Secondly, the study utilized a single-center retrospective cohort design, potentially limiting its representativeness. However, the inclusion of over 4000 CKD patients enhanced the reliability of the results. Thirdly, the study’s sample size constraints restricted the number of variables available for adjustment in the multivariable analysis. It is important to note that long-term mortality is a complex outcome influenced by multiple factors. Fourthly, for acute patients, because the hospital stay is shorter, failure to complete the preoperative creatinine test may affect the applicability of the results.
Conclusion
Contrast-induced acute kidney injury (CA-AKI) is a frequently observed complication in CKD patients undergoing coronary angiography (CAG), and both CA-AKI definitions are linked to an unfavorable prognosis. Therefore, in the clinical practice of CKD patients, it is crucial to give heightened attention to CA-AKI, irrespective of the specific definition utilized.
Abbreviations
CA-AKI, Contrast-associated acute kidney injury; CAG, Complication following coronary angiography; CKD, Chronic kidney disease; AKIN, Acute Kidney Injury Network; PARs, Population attributable risks; eGFR, Estimated glomerular filtration rate; PCI, Percutaneous coronary intervention; MDRD, Modification of Diet in Renal Disease; CHF, Chronic heart failure; NYHA, New York Heart Association.
Data Sharing Statement
The dataset generated for this study is not publicly available, but is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The studies involving human participants were reviewed and approved by The Ethics Committee of Dongguan Traditional Chinese Medicine Hospital (approval number: PJ (2023) 31). Prior to the study, all participants had given informed consent and signed written informed consent.
Consent for Publication
All authors have given consent for publication.
Acknowledgments
We thank all subjects and colleagues for participating in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was sponsored by the Dongguan social development technology project (Grant Nos. 20231800935442).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Goldberg A, Hammerman H, Petcherski S, et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J. 2005;150(2):330–337. doi:10.1016/j.ahj.2004.09.055
2. Mitchell AM, Kline JA, Jones AE, Tumlin JA. Major Adverse Events One Year After Acute Kidney Injury After Contrast-Enhanced Computed Tomography. Ann Emergency Med. 2015;66(3):267–274. doi:10.1016/j.annemergmed.2015.04.028
3. Sato A, Aonuma K, Watanabe M, et al. Association of contrast-induced nephropathy with risk of adverse clinical outcomes in patients with cardiac catheterization: from the CINC-J study. Int J Cardiol. 2017;227:424–429. doi:10.1016/j.ijcard.2016.11.019
4. James MT, Samuel SM, Manning MA, et al. Contrast-Induced Acute Kidney Injury and Risk of Adverse Clinical Outcomes After Coronary Angiography A Systematic Review and Meta-Analysis. Circulation-Cardiovascular Interventions. 2013;6(1):37. doi:10.1161/circinterventions.112.974493
5. Chen S-Q, Liu Y, Smyth B, et al. Clinical Implications of Contrast-Induced Nephropathy in Patients Without Baseline Renal Dysfunction Undergoing Coronary Angiography. Heart Lung & Circulation. 2019;28(6):866–873. doi:10.1016/j.hlc.2018.04.291
6. Centola M, Lucreziotti S, Salerno-Uriarte D, et al. A comparison between two different definitions of contrast-induced acute kidney injury in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Int J Cardiol. 2016;210:4–9. doi:10.1016/j.ijcard.2016.02.086
7. Lun Z, Lei L, Zhou D, et al. A comparison between two different definitions of contrast-associated acute kidney injury for long-term mortality in patients with diabetes undergoing coronary angiography: a prospective cohort study. BMC Cardiovascular Disorders. 2020;20(1):485. doi:10.1186/s12872-020-01778-6
8. Wang B, Zheng Y, Li H, et al. Comparison Between Two Definitions of Contrast-Associated Acute Kidney Injury in Patients With Congestive Heart Failure. Front Cardiovascular Med. 2022:9763656. doi:10.3389/fcvm.2022.763656
9. He H, You Z, Lin X, et al. A Comparison Between Two Definitions of Contrast-Associated Acute Kidney Injury for Long-Term Mortality in Elderly and Non-elderly Patients After Elective Percutaneous Coronary Intervention. Front Cardiovascular Med. 2021:8720857. doi:10.3389/fcvm.2021.720857
10. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention - Development and initial validation. J Am Coll Cardiol. 2004;44(7):1393–1399. doi:10.1016/j.jacc.2004.06.068
11. Watabe H, Sato A, Hoshi T, et al. Association of contrast-induced acute kidney injury with long-term cardiovascular events in acute coronary syndrome patients with chronic kidney disease undergoing emergent percutaneous coronary intervention. Int J Cardiol. 2014;174(1):57–63. doi:10.1016/j.ijcard.2014.03.146
12. Tsai TT, Patel UD, Chang TI, et al. Contemporary Incidence, Predictors, and Outcomes of Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions. Jacc-Cardiovascular Interventions. 2014;7(1):1–9. doi:10.1016/j.jcin.2013.06.016
13. Eknoyan G, Levin NW. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification - Foreword. Am J Kidney Dis. 2002;39(2):S14–S266. doi:10.1053/ajkd.2002.30939
14. Manjunath G, Tighiouart H, Ibrahim H, et al. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J Am Coll Cardiol. 2003;41(1):47–55. doi:10.1016/s0735-1097(02)02663-3
15. Stacul F, van der Molen AJ, Reimer P, et al. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol. 2011;21(12):2527–2541. doi:10.1007/s00330-011-2225-0
16. Moriyama N, Ishihara M, Noguchi T, et al. Admission Hyperglycemia Is an Independent Predictor of Acute Kidney Injury in Patients With Acute Myocardial Infarction. Circ J. 2014;78(6):1475–1480. doi:10.1253/circj.CJ-14-0117
17. Cicek G, Yildirim E. CHA2DS2-VASc score predicts contrast-induced nephropathy in patients with ST-segment elevation myocardial infarction, who have undergone primary percutaneous coronary intervention. Kardiologia Polska. 2018;76(1):91–98. doi:10.5603/KP.a2017.0177
18. Jiang W, Yu J, Xu J, et al. Impact of cardiac catheterization timing and contrast media dose on acute kidney injury after cardiac surgery. BMC Cardiovascular Disorders. 2018:18191. doi:10.1186/s12872-018-0928-8
19. Fu N, Li X, Yang S, et al. Risk Score for the Prediction of Contrast-Induced Nephropathy in Elderly Patients Undergoing Percutaneous Coronary Intervention. Angiology. 2013;64(3):188–194. doi:10.1177/0003319712467224
20. Chong E, Poh KK, Liang S, Soon CY, Tan H-C. Comparison of Risks and Clinical Predictors of Contrast-Induced Nephropathy in Patients Undergoing Emergency versus Nonemergency Percutaneous Coronary Interventions. J Int Cardiol. 2010;23(5):451–459. doi:10.1111/j.1540-8183.2010.00581.x
21. Lei L, Xue Y, Guo Z, et al. A comparison between different definitions of contrast-induced acute kidney injury for long-term mortality in patients with acute myocardial infarction. Int J Cardiol Heart Vasculature. 2020;28:100522. doi:10.1016/j.ijcha.2020.100522
22. Mehran R, Dangas GD, Weisbord SD. Contrast-Associated Acute Kidney Injury. N Engl J Med. 2019;380(22):2146–2155. doi:10.1056/NEJMra1805256
23. Lassnigg A, Schmidlin D, Mouhieddine M, et al. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597–1605. doi:10.1097/01.Asn.0000130340.93930.Dd
24. Neumann F-J, Sousa-Uva M. ‘Ten commandments’ for the 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur Heart J. 2019;40(2):79–80. doi:10.1093/eurheartj/ehy855
25. Liu Y, Tan N, Huo Y, et al. Simplified Rapid Hydration Prevents Contrast-Associated Acute Kidney Injury Among CKD Patients Undergoing Coronary Angiography. Jacc-Cardiovascular Interventions. 2023;16(12):1503–1513. doi:10.1016/j.jcin.2023.03.025
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.