")
Back to Journals » Clinical Interventions in Aging » Volume 17
A Home-Based Dyadic Music-with-Movement Intervention for People with Dementia and Caregivers: A Hybrid Type 2 Cluster-Randomized Effectiveness-Implementation Design
Authors Cheung DSK , Ho LYW, Chan LCK, Kwok RKH, Lai CKY
Received 13 April 2022
Accepted for publication 28 July 2022
Published 11 August 2022 Volume 2022:17 Pages 1199—1216
DOI https://doi.org/10.2147/CIA.S370661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Daphne Sze Ki Cheung,1 Lily Yuen Wah Ho,1 Liliane Chui King Chan,2 Robin Ka Ho Kwok,1 Claudia Kam Yuk Lai1
1School of Nursing, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong Special Administrative Region, People’s Republic of China; 2Ho Cheung Shuk Yuen Charitable Foundation, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Daphne Sze Ki Cheung, School of Nursing, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong Special Administrative Region, People’s Republic of China, Tel +852 2766 4534, Email [email protected]; [email protected]
Background: Integrating evidence-based music-with-movement into routine practices for people with dementia requires effective implementation strategies. The objectives of this study were to evaluate the clinical efficacy of the intervention and to examine the effectiveness of the implementation strategies in promoting home-based adoption.
Methods: This was a cluster randomized controlled trial adopting a clinical effectiveness-implementation hybrid design. The 12-week music-with-movement intervention aims to promote the well-being of people with dementia and their caregivers. Clinical outcomes were assessed to evaluate the efficacy of the intervention. These included the symptoms of anxiety and depression of people with dementia; caregivers’ perception of their stress and the positive aspects of caregiving; and the quality of the dyadic relationship. Caregivers, staff, and volunteers were interviewed and objective figures on reach and adoption were collected to reflect the outcomes of the implementation.
Results: Compared to the waitlist control, there was a significant reduction in the anxiety and the symptoms of depression of those in the intervention group. There was also a significant reduction in the perceived stress level of the caregivers. Six focus group interviews were conducted. The intervention and the appropriateness of the implementation strategies were perceived positively by the dyad participants, the staff of the centres, and volunteers. Of the collaborating centres, 57% continued to use the intervention and, after six months, served six times more people than were recruited in this study. Over half of the participating families continued to use the intervention for at least six more months.
Conclusion: Music-with-movement interventions showed promise for improving the well-being of people with dementia and their caregivers. Effective strategies facilitated the implementation process, such as integrating communication technology to provide instant support and involving volunteers in engaging the collaborating centres and families. This study sheds light on perceptions of the intervention, and on its scalability for a broader population.
Trial Registration: NCT03575026, Registered 2 July 2018.
Keywords: music, dementia, implementation, acceptability, well-being
A Letter to the Editor has been published for this article.
A Response to Letter by Mrs Hefner has been published for this article.
Introduction
Dementia is a neurodegenerative disorder characterized by a progressive and continuous decline that can adversely affect a person’s cognitive, behavioural, social, and emotional functioning. Among the various types of non-pharmacological interventions that support older adults with dementia and their caregivers, music interventions have become popular.1 Elements of music, such as rhythm, melody, pitch, and harmony, have been shown to elicit a wide range of psychological and physiological responses that make physical activity more enjoyable, leading to improved health outcomes and quality of life.2 Meta-analyses showed that music interventions positively affected the behavioural, cognitive, physiological, and affective outcome measures of people with dementia.1,3 They also helped to improve communication and relationships between persons with dementia (PWD) and their family caregivers, reduce the caregivers’ burden, and improve psychological symptoms in family caregivers.4 With its promising effects, one music intervention programme, Music and Memory, has been successfully adopted in over 100 nursing facilities in the U.S.5 However, a number of barriers were faced in the implementation, such as the perception of the staff that the intervention was not effective and that it was too intensive in terms of time/labour; therefore, it was suggested that effective implementation strategies be designed to overcome the identified barriers.6
In Hong Kong, a music-with-movement intervention (MM) was developed for PWD, which later came to involve family caregivers as a dyadic intervention.7–10 The approach involves the movement of gross body muscles with preferred music, while little is required in terms of fine motor muscle coordination or verbal ability.7 It was found that this music intervention effectively reduced the anxiety levels of PWD, and the qualitative results indicated that it was helpful for family caregivers to have a better understanding of their relatives and to maintain a closer relationship with them.10 Similar approaches have been employed as an intervention for PWD in Taiwan,11 the United States,12 and Belgium.13 The development of the intervention protocol for PWD was based on theoretical principles of music therapy, experience in working with PWD, and ideas and principles collected from experts in dementia care.7,14 However, the major problem with regard to the uptake of evidence is that successful trials are often those conducted within a research context. It is crucial to disseminate an evidence-based intervention to benefit a broader population, which requires purposive and effective implementation strategies that fit the Asian context. More important, the experience and findings would inform practice and contribute to research on implementing and sustaining a potentially efficacious intervention.
The dissemination of evidence-based music interventions into routines is challenging.6 Therefore, implementing the MM intervention for PWD requires a comprehensive approach that addresses barriers and facilitators, which may lower the motivation of stakeholders to follow the recommended implementation protocol. This study follows the Consolidated Framework For Implementation Research (CFIR), which guides the identification of contextual determinants within the local context.15 The Expert Recommendations for Implementing Change (ERIC) were also considered when designing the implementation strategies targeting the identified barriers.16 The CRIF framework is composed of determinants that have been organized into five major domains: intervention characteristics, outer setting, inner setting, the characteristics of the individuals involved, and the process of implementation. The ERIC compilation provides a list by which to select discrete strategies that can be used to build a tailored multicomponent strategy for implementation.16–18
Based on experience accumulated from previous randomized controlled trials,8–10 the barriers to implementation were identified (see Table 1 for details) to be addressed by relevant ERIC implementation strategies (see Table 2 for details). The implementation strategies target the four categories of contextual barriers named by CFIR and are aimed at: (1) increasing the target population’s perception of their need for the intervention (ie, the outer-setting); (2) addressing the concerns of stakeholders (ie, the inner-setting and individual characteristics); and (3) facilitating the process. The effectiveness of these strategies had yet to be evaluated.
 |
Table 1 ERIC Implementation Strategies to Address Barriers Identified by CFIR |
 |
Table 2 Descriptions of the Strategies Used in the Study |
Objectives
This study was to evaluate the adoption of a music-with-movement (MM) intervention with a sustainable approach to improving the psychosocial well-being of PWD and their family caregivers. A multi-method approach using a combination of quantitative and qualitative research methods was used to evaluate the clinical efficacy of the intervention and examine the effectiveness of the implementation strategies. The objectives of the study were:
- To quantitatively evaluate the clinical efficacy of the intervention on the psychosocial well-being of PWD and their caregivers, and on the quality of the dyadic relationship, and.
- To qualitatively examine the effectiveness of the implementation strategies used to promote the adoption of the home-based, dyadic MM intervention.
Methods
Design
This is a cluster randomized controlled trial with an effectiveness-implementation hybrid design. This Type 2 hybrid design allows for a dual focus on assessing the clinical effectiveness of interventions and on addressing the methods and procedures necessary to deliver and sustain them in real-world settings.19 Unlike Type 1 and Type 3 hybrid design, which focuses on either testing the clinical effects or implementation strategies respectively.
To evaluate the efficacy of the intervention (Objective 1), the clinical outcomes were measured twice at baseline and at the Week 12 follow-up. To examine the effectiveness of the implementation strategies (Objective 2), semi-structured focus group interviews with the caregivers, volunteers, and staff were conducted after the completion of the programme. Objective figures showing the adoption and sustainability of the programme were also collected. The reporting of this study followed the Standards for Reporting Implementation Studies (STaRI)20 and the CONSORT guidelines.
Participants
The participants were PWD and their primary family caregiver who were referred to the researchers by the participating collaborators, which provided community services to the neighbourhood. PWD were: (1) aged 60 or above; (2) community-dwelling; (3) with cognitive impairment at stage 4 or 5 on the Global Deterioration Scale (early to moderate dementia);21 (4) in a stable medical or mental condition to participate in group activities; (5) able to communicate in Cantonese, the major Chinese dialect in Hong Kong; and (6) with a primary family caregiver who agreed to join the programme. Excluded were those who had suffered from any critical medical or psychiatric illnesses, had uncorrectable visual and auditory impairments; were unable to sit independently for around 30 minutes; or who had participated in any music intervention or clinical trial within the past six months. Caregiver participants had to be physically and mentally stable without critical illness or any impairment in mental health.
To address objective #2, to qualitatively examine the effectiveness of the implementation strategies adopted to promote the adoption of the home-based, dyadic MM intervention, the caregivers, staff members, and volunteers who were involved in this project were interviewed.
Sample Size
Although this study had two equally important objectives, the sample size was estimated through a power analysis based on the clinical efficacy of the intervention. A significant interaction effect was found for the anxiety level of people with early dementia, with an effect size of Cohen’s d = 0.361.7 A sample size of 86 families is needed to achieve a power of 0.80 and an alpha level of 0.05.22 Assuming an attrition rate of 20%, 103 families would need to be recruited.
Setting
The programme took place at seven collaborating centres and the participants’ home. To extend the reach of the service, collaborators were not limited to those who provide community services to older adults but also included a women’s services centre, and centres offering general community services. Five of the centres were collaborators of other projects led by the first author, and two of them approached the project team when they heard about the programme from their service users. These organizations needed to ensure that they would assign at least five staff members to undergo training on the MM intervention. This was to prevent a loss of knowledge in case of staff turnover, which would affect the sustainability of the programme. In addition, the centres were obligated to work with the project team to support at least 15 trained volunteers to aid the participating families.
Randomization and Blinding
Before randomization, all collaborating centres were informed about the design and aims of the study and the content of the intervention. Then, each centre was randomized to the intervention or the waitlist control using the simple randomization approach, with the random number generated by a computer. Participating dyads will follow the group allocation of their corresponding centres. Given that the collaborating centres implemented the project and given the nature of the intervention, both the staff and participants could not be blinded. Only the trained assessors were blinded to the group allocation.
Objective #1: Evaluating the Efficacy of the Intervention
Description of the Intervention
The 12-week dyadic MM intervention, which was held three times a week, with each session lasting 30–45 minutes, was designed to benefit the PWD and their family caregivers. The dyads moved body parts during the intervention while listening to their preferred music. As part of the intervention, the family caregivers also needed to engage the PWD in music activities at home, including dancing, playing with musical instruments, and so on. They were also asked to relax in the musical environment. The intervention protocol was published in our earlier publications.10,23 Empowering family caregivers at the early stage of the intervention is important to improve their confidence and competence in mastering the skills needed to participate/provide the music intervention, ensure the quality of the delivery of the intervention, and render the intervention sustainable. Therefore, of the 12 weeks of the intervention, trained centre staff members were asked to deliver one session of centre-based intervention at weeks 1, 3, 7, and 12. The home visits made by a team of trained volunteers to support families were scheduled at weeks 2, 5, and 9. The family caregivers were asked to deliver the intervention at home by themselves for the rest of the time to meet the prescribed dosage. Centre staff members and volunteers were available to offer continual support to the caregivers, if necessary, by phone or face-to-face in the centres. Details of the recruitment, training and monitoring of the volunteers were reported.24
After completing 12 weeks of the usual care, the participants in the waitlist control group received the identical MM intervention and implementation strategies to attract them to remain in the study.
Efficacy of the Intervention: Outcome Measures
Rating Anxiety in Dementia (RAID) is a clinical rating scale that assesses the severity of anxiety in PWD over the past two weeks, as reported by caregivers.25 Cheung et al26 translated and validated the scale into a Chinese version for use in this study. The RAID scale consists of 20 items, 18 of which can be divided into four domains: worry, apprehension and vigilance, motor tension, and autonomic hypersensitivity. Those items can be scored on a 4-point scale, ranging from 0 (absent) to 3 (severe), with higher scores indicating more severe anxiety. The total score ranges from 0 to 54. A cut-off score of 11 and above provides a sensitivity of 90% and a specificity of 78.5% for identifying clinically significant anxiety. Two additional items (phobias and panic attacks) are not included in the total score.25
The Cornell Scale for Depression in Dementia (CSDD) is an instrument that is used to rate symptoms of depression in PWD over the past week.27 Lin and Wang28 translated the scale into a Chinese version. The 19-item scale can be divided into five domains: signs of moodiness, behavioural disturbances, physical signs, biological functions, and ideational disturbances. Each item is rated on three levels of severity, from 0 (absent) to 2 (severe). The total score ranges from 0 to 38, with higher scores indicating a higher level of depression. A total score of > 10 indicates a probable or definite major depressive episode.
The Perceived Stress Scale (PSS) is a psychological instrument that is used to measure caregivers’ perception of stress over the last month.29 The items were developed to evaluate how respondents report on whether their lives have been unpredictable, uncontrollable, or overloaded. Leung et al30 translated the scale into a Chinese version. The 10-item scale consists of six negative and four positive items. Each item is rated on a 5-point Likert scale, from 0 (never) to 4 (very often). The total score is 40, with a higher score indicating a higher level of perceived stress.
Positive Aspects of Caregiving (PAC) is an instrument that is used to measure the psychosocial benefits to caregivers in the context of the caregiving experience.31 Lou et al32 translated the scale into a Chinese version. The 9-item scale can be divided into two subscales: self-affirmation and outlook on life. Each item is rated on a 5-point Likert scale, from 1 (disagree a lot) to 5 (agree a lot). The total score is 45, with a higher score indicating a more positive perception of the caregiving experience.
The Quality of the Caregiver-Care Recipient Relationship (QCCRR) is a scale that is used to measure the quality of the current relationship between caregivers and people with MCI/dementia.33 The 4-item scale covers general closeness, communication, similarity of views about life, and degree of getting along. Each item is rated on a 4-point Likert scale, from 1 (not at all close/well/similar) to 4 (very close/well/similar). The total score is 16, with a higher score indicating a better relationship between caregivers and people with MCI/dementia.
Objective #2: Examination of Implementation Strategies
Description of the Implementation Strategies
Eighteen implementation strategies were designed to address the four categories of contextual barriers according to the CFIR framework, namely outer setting, inner setting, characteristics of the individual, and process. These barriers were addressed by the careful mapping of ERIC implementation strategies following a discussion with the stakeholders as well as a literature review.34 For example, individual regular meetings were organized with each collaborating partner before, during, and after implementing the intervention to communicate the goals and answer queries; only organizations that agreed on the importance of music interventions for promoting the wellness of PWD and their caregivers were invited to be collaborating partners, and so on. In addition, we integrated technology to facilitate the implementation, such as forming a WhatsApp (instant chat) group for solving the problems of participants, staff members, or volunteers; using an E-manual; and using Google Form to collect feedback from volunteers. For details, please see Tables 1 and 2.
Implementation: Outcome Measures
The caregiver participants, trained volunteers, and staff of the centres were invited to comment on their perceptions and experiences of the implementation strategies in three focus groups. Prompting questions were designed according to the Proctor et al35 model. The focus was on the following areas: the acceptability of the intervention; the appropriateness of the implementation strategies and perceptions of the strategies; the feasibility of the centre adopting the intervention as a regular approach; the adoption of the intervention in the centres; the sustainability of the intervention in the centre and as practised at home by the families. We also asked for comments on the facilitators and barriers to the implementation of the intervention as delivered by the staff of the centres, the volunteers, and the families. The caregiver participants were also asked additional questions to evaluate the effects of the intervention on them and their relatives. The interviews were audio-recorded with the consent of all of the interviewees.
Reach represents the number who are willing to participate, while adoption is the proportion of settings and intervention staff who are willing to initiate an intervention or program.36 Therefore, to determine the reach and adoption of the intervention, information on the following aspects was collected: the integration of the intervention as a routine service; the number of families who continued the home-based practice; the number of downloads of the E-manual; and enrolment in a self-financed training programme beyond the funding period.
Ethical Considerations
Ethical approval was received from the University’s Research Committee (HSEARS20180319002) and the study was carried out following the Helsinki Declaration. An information sheet was given to the staff members, volunteers, family caregivers, and PWD. Their verbal and written informed consent to participate in the study was collected after they were given an explanation of the purpose and procedures of the research study. Continuous verbal consent was obtained from the participating PWD when the trained research assistant conducted data collection. When any PWD refused to continue participating during any intervention session, the staff of the centres, volunteers, and family caregivers were advised not to proceed. Social workers were available to offer support to the staff, volunteers, family caregivers, and PWD when any expressions of emotional distress were observed during the intervention.
Analysis
A comparison was made of the demographics and clinical outcomes of the intervention and control groups at baseline by using a chi-square test for categorical variables. An independent t-test was used for normally distributed continuous variables, while a Mann–Whitney U-test was used for non-parametric variables. To evaluate the clinical effectiveness of the MM intervention on PWD, family caregivers, and dyadic outcomes, the intention-to-treat analysis approach was employed to minimize the bias. Missing data were imputed by the last observation carried forward method. A generalized estimating equations (GEE) analysis was conducted to compare the differential changes in each outcome at baseline and at the follow-up between the two arms, with an adjustment for the baseline arm difference. Specifically, the interaction (Group*Time) was included in each GEE model to assess the differential changes. All statistical analyses were performed using IBM SPSS 26. All statistical tests were two-sided with the level of significance set at 0.05.
To examine the effectiveness of the implementation strategies, semi-structured focus group interviews were conducted with dyads, volunteers, and staff of the centres. The interviews were audio-recorded and transcribed. Coding were done by the first author and trained research assistants independently. Analysis was done by searching for themes that occurred across the interviews. The statistics on the reach and adoption of the intervention were reported descriptively.
Results
In this study, a total of 100 dyad participants, 50 centre staff members, and 125 volunteers were recruited. Seventy-seven of the dyad participants completed the intervention. A total of 40, 24, and 30 sessions of educational training were delivered to family caregivers, centre staff members, and volunteers, respectively. Only 59 family caregivers received support from volunteers to deliver the intervention at home because the rest turned down the offer to receive volunteer support at home. Figure 1 summarizes the number of dyad participants in each phase of the study.
 |
Figure 1 Trial flowchart. |
Clinical Efficacy
The characteristics of the dyad participants are summarized in Table 3. Among the PWD, there were no significant group differences in age, marital status, level of education, cognitive function, anxiety, and depressive symptoms at baseline. The proportion of females was higher in the intervention group than in the control group (61.82% vs 40.00%, p=0.030). Among the family caregivers, there were no significant group differences in age, gender, and perceived stress. The caregiver participants were either the spouse or the children of the participants with dementia in the control group, but some caregiver participants in the intervention group were the in-law, grandchild, sibling, or cousin of the PWD (p=0.042). The intervention group had more positive caregiving experiences (35.38 ± 7.43 vs 31.96 ± 7.75, p=0.017) and better-quality relationships (12.02 ± 2.35 vs 10.57 ± 2.05, p=0.002) than the control group at baseline.
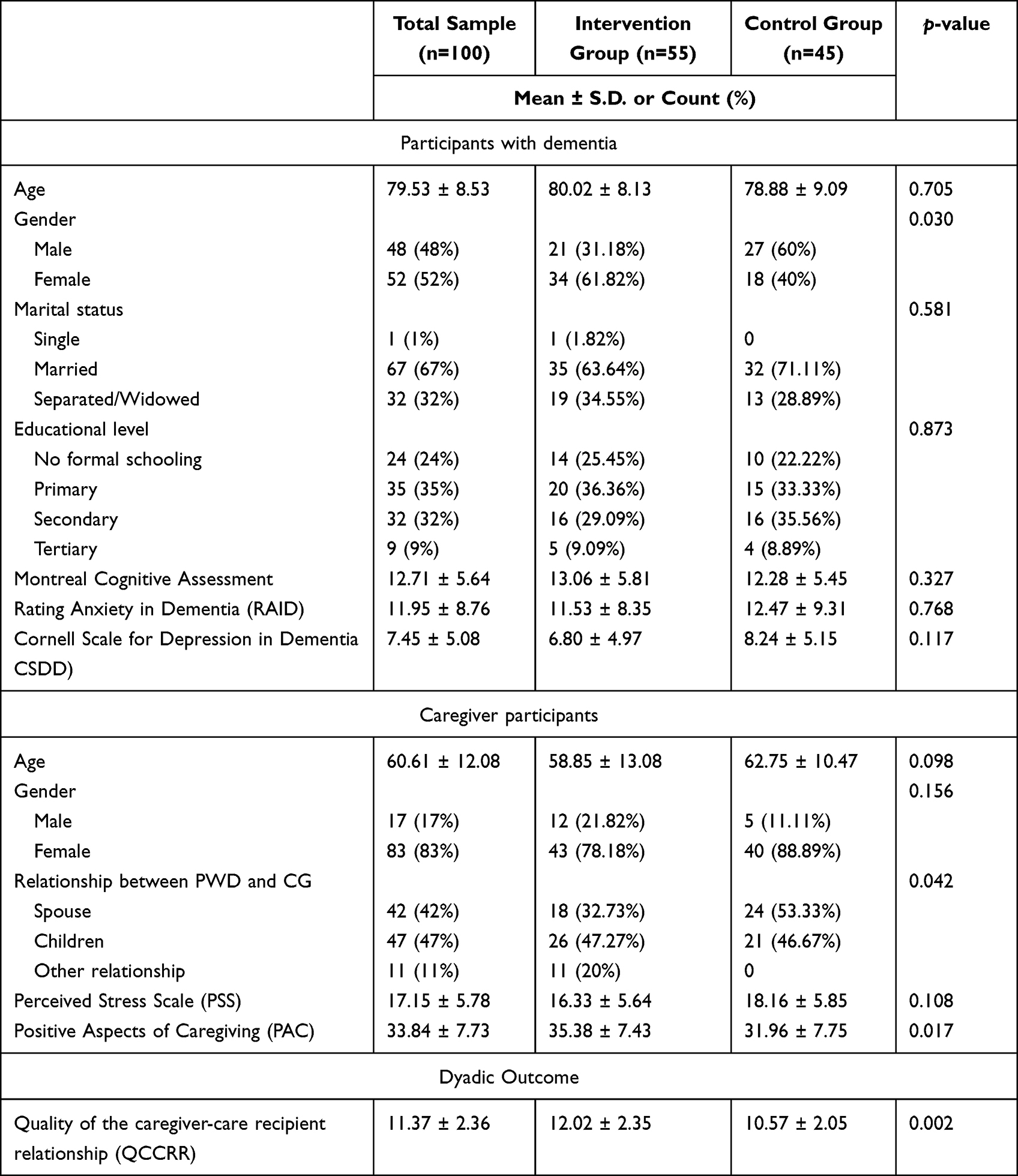 |
Table 3 Characteristics of the Participants at Baseline |
The changes in the clinical outcomes of the dyad participants are shown in Table 4. Among PWD, the GEE analyses revealed statistically significant differences between the groups in the proportion of those who experienced anxiety (β=−1.59, SE=0.48, p=0.001), indicating that the intervention improved anxiety. The analyses also showed statistically significant differences between the groups in the total score (β=−3.06, SE=1.02, p=0.003), mood domain score (β=−0.70, SE=0.34, p=0.036), and behaviour domain score of CSDD (β=−0.86, SE=0.36, p=0.017), indicating that the intervention reduced depressive symptoms, signs of moodiness, and behavioural disturbances. There were no significant differences between the groups in the RAID – Total score and other domain scores of CSDD. With regard to the caregiver participants, GEE analyses revealed statistically significant differences between the groups in the PSS score (β=−2.39, SE=1.21, p=0.047) but not in PAC, indicating that the intervention reduced perceived stress. There were no significant differences in the QCCRR – Total score between the groups.
 |
Table 4 Changes in Clinical Outcomes Between Baseline and Follow-Up, and the Results of the GEE Analysis |
Effectiveness of the Implementation Strategies
Focus Groups
Two focus groups were conducted separately with dyads, volunteers, and staff to qualitatively evaluate the implementation strategies developed for this study, for a total of six group interviews. Each interview lasted for 45–60 minutes and consisted of 4–6 interviewees; in total, 29 persons were interviewed. The interviewees were those who had completed the intervention within one month so that their memory of the intervention and the implementation strategies was fresh. Table 5 includes illustrative quotes from the focus groups in relation to each domain.
 |
Table 5 Selected Quotes from the Focus Groups Commenting on the Effectiveness of the Implementation Strategies |
Overall, the findings were consistent across staff, volunteers, and dyad participants. The intervention was acceptable to the dyad participants. The implementation strategies were perceived to be appropriate because the family caregivers received support when necessary. Staff members thought that the volunteers were a bridge between the staff and families. They also commented that it was feasible for the centres to adopt the intervention as a routine service because the materials were inexpensive and the home-based activity did not occupy space in the centre. The intervention was appraised as easy for non-professionals to adopt because the skills involved in delivering the intervention were not difficult to acquire. With a certain number of staff members trained, the intervention was sustainable. Family caregivers stated that they would continue the intervention upon the completion of this study.
Facilitators and barriers to the implementation of the intervention were identified from the interview data. A training package with other topics relating to the care of older people was a facilitator to retaining volunteers to support the intervention. Barriers to implementation included the steps and the movements that needed to be made during the intervention and the inertia of the participants with dementia. Overall, the qualitative data supported the view that the intervention exerted positive effects on both PWD and family caregivers.
Objective Findings About the Reach and Adoption of the Intervention
Four out of seven partner organizations continued to use the music intervention in their centres to serve other older people and families. Other than the dyads who participated in this project, the number of people who were served within the first six months after the completion of the project was 651 (ie, six times the number that were targeted in the funded project). Forty-four families (58.4%) indicated they continued to use the MM interventions when they were asked six months after the completion of the intervention. The majority of them practised them once a week, which was lower than the recommended number of three times per week. Within the 18 months after the completion of the project, three rounds of self-financed training workshops were organized for health and social care personnel from 47 different organizations (approximately seven times the number of collaborating partners) or individual family caregivers. By six months after the completion of the project, the E-manual had been downloaded over 1300 times.
Discussion
This study is innovative because two major implementation sciences frameworks, CFIR and ERIC, were employed to systematically identify the contextual barriers to implementing an evidence-based MM intervention; and accordingly to comprehensively design the implementation strategies. This approach can be used as a template for researchers to use to translate their evidence-based non-pharmacological intervention into real practice. Our main findings were that the MM intervention was effective in alleviating the anxiety and depressive symptoms of PWD and the perceived stress of caregivers; while the implementation strategies were perceived positively by the staff, volunteers, and caregivers. This led to over half of the participating organizations and families continuing to use the intervention for at least more than 6 months. As word spread of the effectiveness of the intervention, staff from 47 other organizations were intrigued enough to be trained to use the same intervention at their own workplace within 18 months after the completion of the project.
Regarding the clinical efficacy of the intervention, the findings showed that the intervention was effective at improving the anxiety and depressive symptoms of PWD and reducing the stress level of family caregivers. Consistent with the findings of a previous study, a greater reduction in the behavioural and psychological symptoms of dementia was found in older people who participated in an interactive music intervention with individualized music and activities, such as clapping and dancing, than in older people who were in a no-music control group.37 The MM intervention was a means to provide support to family caregivers caring for PWD. At the same time, engaging in music activities may induce relaxation effects. It might thus reduce caregiver stress. The activities in the music intervention offered opportunities for social interaction between PWD and family caregivers, which encouraged active participation and engagement on the part of the dyads.
Partnering with stakeholders and good communication among the team set the basis for implementing the 18 designed strategies. The partnership between the stakeholders who were responsible for implementation and our research team increased the knowledge and skills of both parties and further improved the initiatives involved in the implementation.38 The strategies that were adopted were developed together with the stakeholders. The meaningful engagement with different stakeholders demonstrated that the adaptive strategies were effective in identifying the challenges to implementation. Those strategies involved seeking to generate information and knowledge that will lead to improvements in promoting and translating the evidence-based intervention as routine care practice. For example, staff identified that their busy schedule with limited manpower to assist the family caregivers in delivering the intervention at home was one of the contextual barriers (ie, CFIR – Inner setting contextual barrier: Available resources are insufficient to support the implementation of the innovation). Hence, a team of volunteers was trained to provide support, which was highly appreciated by staff and family caregivers. The staff regarded the volunteers as being able to bridge the gap between the limited provision of care and the families in need, while the family caregivers thought of the volunteers as a support network. In addition, unlike the staff, the volunteers had no affiliation, so they could be a mobile workforce implementing the intervention to others beyond the beneficiaries of the project. More importantly, from the implementation sciences perspective, the volunteers freed up valuable time for social and health professionals to devote to more complicated tasks; thus, their involvement was regarded as a very cost-effective measure.39 At the same time, these volunteers were taught valuable knowledge and skills about dementia care, making them valuable assets for public health.24
To facilitate communication between stakeholders and the project team, we attempted to integrate information and communication technology as implementation strategies to provide instant feedback to the participants, volunteers, and staff members; disseminate the intervention manual (E-manual); and collect feedback. Electronic messaging was found to improve efforts to exchange information in primary care.40 In this study, solving frontline practice problems or difficulties promptly favoured the delivery and, thus, the continuous adoption of the intervention by family caregivers. Information and communication technology has been identified as an important enabler to support the delivery of integrated and coordinated primary health care, but the technology is not without its limitations.41 For instance, it was believed that the E-manual would be able to facilitate the dissemination of the intervention manual, yet the caregivers stated that they still could not remember the steps. This feedback prompted us to consider further refining our implementation strategies, such as developing an MM system in which the music genres are stored in the system, which would make it easier for family caregivers to play the music; and showing the steps of the movement on screen as prompts; etc. The advancement of technology will further enhance the implementation of different psychosocial interventions.
It has been widely reported that evidence-based practices take an average of 17 years to be incorporated into routine general practice in health care.42 Those who fund biomedical research are increasingly concerned over the lack of public health impact of their research dollars.43 Taking Hong Kong as an example, in recent years one of the major biomedical research funding schemes (Health and Medical Research Fund by the Health & Food Bureau) opened up a new research priority – Implementation Science, in the hope of accelerating the integration of research innovations into real practice. Implementation strategies should be culturally appropriate, but regrettably, to the best of our knowledge, relatively few implementation studies are conducted in Asian regions. Therefore, our studies provide useful information on how to design strategies that fit the Asian context. For instance, our external stakeholders suggested that after completing the educational training, the volunteers should be given a certificate of accreditation issued by the project team and endorsed by our University. The majority of our volunteers were middle-aged or young-old retirees. Most had not received a tertiary education, and it made them feel honoured to receive such a certificate.
As an implementation scientist, it is important to bridge the gap between knowledge and the adoption of research.38 There was some criticism that this hybrid study design might represent a compromise in methodological rigour and have a negative impact on the dissemination of scientific findings.44 However, we believe that this hybrid study design allows us to meaningfully target frontline practitioners, administrators, and researchers in a way that may aid in narrowing the current science-to-service gap.
Limitations
Most of the collaborating partners were long-term partners and were invited to take part in the study by the first author, who thought they were very cooperative. Whether the implementation strategies and intervention can be successfully applied to other settings has yet to be explored. Second, the cost of the intervention was largely covered by project or grant funding; whether the dyads would still be willing to adopt the intervention if they had to pay for the costs out of their own pocket is not known. However, the materials used in the intervention are not costly; what is costly is the training. If the training can be delivered on a large-scale (eg, through online webinars), we believe that the cost would be greatly reduced and should not be a hindering factor for most.
Conclusions
Through systematically identifying the contextual barriers to the implementation of the music-with-movement intervention using the CFIR framework and mapping them out with the strategies suggested by the ERIC frameworks, the findings of our study demonstrate that the intervention is both clinically efficient and can be implemented effectively. Working closely with external stakeholders with good communication skills and understanding cultural perspectives and human factors are the keys to success. The clinical effectiveness-implementation hybrid study design narrows the science-to-service gap through meaningful collaboration among frontline practitioners, administrators, and researchers.
Data Sharing Statement
The datasets that were generated and analysed in this study are not publicly available due to ethical restrictions prohibiting the sharing of personal data.
Ethics Approval and Informed Consent
The study was approved by the Human Subjects Ethics Sub-committee of the Hong Kong Polytechnic University (HSEARS20180319002). The verbal and written informed consent were obtained from all participants.
Consent for Publication
The manuscript does not contain information that can reveal the identities of the participants.
Funding
The project was funded by the Ho Cheung Shuk Yuen Charitable Foundation. The funding body was involved in the design of the implementation strategies and writing of the manuscript, but not in the collection, analysis, and interpretation of the data.
Disclosure
Dr Daphne Sze Ki Cheung reports grants from Ho Cheung Shuk Yuen Charitable Foundation, during the conduct of the study. The authors declare that they have no other competing interests.
References
1. Chang YS, Chu H, Yang CY., et al. The efficacy of music therapy for people with dementia: a meta‐analysis of randomised controlled trials. J Clin Nurs. 2015;24(23–24):3425–3440. doi:10.1111/jocn.12976
2. Murrock CJ, Higgins PA. The theory of music, mood and movement to improve health outcomes. J Adv Nurs. 2009;65(10):2249–2257. doi:10.1111/j.1365-2648.2009.05108.x
3. Vasionytė I, Madison G. Musical intervention for patients with dementia: a meta‐analysis. J Clin Nurs. 2013;22(9–10):1203–1216. doi:10.1111/jocn.12166
4. Raglio A, Fonte C, Reani P, Varalta V, Bellandi D, Smania N. Active music therapy for persons with dementia and their family caregivers. Int J Geriatr Psychiatry. 2016;31(9):1085–1087. doi:10.1002/gps.4421
5. Music & memory; 2022. Available from: https://musicandmemory.org/.
6. Kwak J, Ha J-H, O’Connell Valuch K. Lessons learned from the statewide implementation of the Music & Memory program in nursing homes in Wisconsin in the USA. Dementia. 2021;20(5):1617–1630. doi:10.1177/1471301220962234
7. Lai CK, Lai DL, Ho JS, Wong KK, Cheung DS. Interdisciplinary collaboration in the use of a music‐with‐movement intervention to promote the wellbeing of people with dementia and their families: development of an evidence‐based intervention protocol. Nurs Health Sci. 2016;18(1):79–84. doi:10.1111/nhs.12238
8. Cheung DSK, Lai CKY, Wong FKY, Leung MCP. The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: a randomized controlled trial. Aging Ment Health. 2018;22(3):306–315. doi:10.1080/13607863.2016.1251571
9. Cheung DSK, Lai CKY, Wong FKY, Leung MCP. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate dementia? A randomized controlled trial. Dementia. 2020;19(5):1413–1425. doi:10.1177/1471301218800195
10. Lai CKY. Music intervention for people with dementia and their family caregivers. A final report submitted to the Ho Cheung Shek Yuen Charitable Foundation; 2016.
11. Sung H-C, Chang S-M, Lee W-L, Lee M-S. The effects of group music with movement intervention on agitated behaviours of institutionalized elders with dementia in Taiwan. Complement Ther Med. 2006;14(2):113–119. doi:10.1016/j.ctim.2006.03.002
12. Ray KD, Götell E. The use of music and music therapy in ameliorating depression symptoms and improving well-being in nursing home residents with dementia. Front Med. 2018;5:287. doi:10.3389/2Ffmed.2018.00287
13. Van de Winckel A, Feys H, De Weerdt W, Dom R. Cognitive and behavioural effects of music-based exercises in patients with dementia. Clin Rehabil. 2004;18(3):253–260. doi:10.1191/0269215504cr750oa
14. Cheung DS, Chien WT, Lai CK. Conceptual framework for cognitive function enhancement in people with dementia. J Clin Nurs. 2011;20(11‐12):1533–1541. doi:10.1111/j.1365-2702.2010.03584.x
15. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:1–15. doi:10.1186/1748-5908-4-50
16. Waltz TJ, Powell BJ, Fernández ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. 2019;14:1–15. doi:10.1186/s13012-019-0892-4
17. Powell BJ, McMillen JC, Proctor EK, et al. A compilation of strategies for implementing clinical innovations in health and mental health. Med Care Res Rev. 2012;69(2):123–157. doi:10.1177/1077558711430690
18. Powell BJ, Waltz TJ, Chinman MJ, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10:1–14. doi:10.1186/s13012-015-0209-1
19. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–226. doi:10.1097/mlr.0b013e3182408812
20. Pinnock H, Barwick M, Carpenter CR, et al. Standards for Reporting Implementation Studies (StaRI) statement. BMJ. 2017;356:1–9. doi:10.1136/bmj.i6795
21. Reisberg B, Ferris SH, de Leon MJ, Crook T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am J Psychiatry. 1982;139(9):1136–1139. doi:10.1176/ajp.139.9.1136
22. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
23. Wong KKY. 欣悅樂韻健身心 - 早期認知障礙人仕的音樂活動手册 [Music-with-Movement - Music activities handbook for early dementia]. The Centre for Gerontological Nursing (CGN) under the School of Nursing of The Hong Kong Polytechnic University; 2017. Chinese.
24. Cheung DSK, Ho LYW, Kwok RKH, Lai DLL, Lai CKY. The effects of involvement in training and volunteering with families of people with dementia on the knowledge and attitudes of volunteers towards dementia. BMC Public Health. 2022;22:1–12. doi:10.1186/s12889-022-12687-y
25. Shankar K, Walker M, Frost D, Orrell M. The development of a valid and reliable scale for rating anxiety in dementia (RAID). Aging Ment Health. 1999;3(1):39–49. doi:10.1080/13607869956424
26. Cheung DSK, Lai CKY, Leung MCP. The Chinese version rating anxiety in dementia scale: a validation study; 2018.
27. Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell scale for depression in dementia. Biol Psychiatry. 1988;23(3):271–284. doi:10.1016/0006-3223(88)90038-8
28. Lin J-N, Wang -J-J. Psychometric evaluation of the Chinese version of the Cornell scale for depression in dementia. J Nurs Res. 2008;16(3):202–210. doi:10.1097/01.jnr.0000387307.34741.39
29. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Beh. 1983;24:285. doi:10.2307/2136404
30. Leung DY, Lam T-H, Chan SS. Three versions of Perceived Stress Scale: validation in a sample of Chinese cardiac patients who smoke. BMC Public Health. 2010;10:1–7. doi:10.1186/1471-2458-10-513
31. Tarlow BJ, Wisniewski SR, Belle SH, Rubert M, Ory MG, Gallagher-Thompson D. Positive aspects of caregiving: contributions of the REACH project to the development of new measures for Alzheimer’s caregiving. Res Aging. 2004;26(4):429–453. doi:10.1177/2F0164027504264493
32. Lou VW, Lau BH-P, Cheung KS-L. Positive aspects of caregiving (PAC): scale validation among Chinese dementia caregivers (CG). Arch Gerontol Geriatr. 2015;60(2):299–306. doi:10.1016/j.archger.2014.10.019
33. Lawrence RH, Tennstedt SL, Assmann SF. Quality of the caregiver–care recipient relationship: does it offset negative consequences of caregiving for family caregivers? Psychol Aging. 1998;13(1):150–158. doi:10.1037//0882-7974.13.1.150
34. Cheung DSK, Tang SK, Ho KHM, et al. Strategies to engage people with dementia and their informal caregivers in dyadic intervention: a scoping review. Geriatr Nurs. 2021;42(2):412–420. doi:10.1016/j.gerinurse.2021.02.002
35. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
36. Gaglio B, Shoup JA, Glasgow RE. The RE-AIM framework: a systematic review of use over time. Am J Public Health. 2013;103(6):e38–46. doi:10.2105/AJPH.2013.301299
37. Sakamoto M, Ando H, Tsutou A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int Psychogeriatr. 2013;25(5):775–784. doi:10.1017/2FS1041610212002256
38. Rapport F, Smith J, Hutchinson K, et al. Too much theory and not enough practice? The challenge of implementation science application in healthcare practice. J Eval Clin Pract. 2021:1–12. doi:10.1111/jep.13600
39. Howson FFA, Robinson SM, Lin SX, et al. Can trained volunteers improve the mealtime care of older hospital patients? An implementation study in one English hospital. BMJ Open. 2018;8(8):1–10. doi:10.1136/bmjopen-2018-022285
40. Bergmo TS, Ersdal G, Rødseth E, Berntsen G. Electronic messaging to improve information exchange in primary care; 2013:172–177.
41. Steele Gray C, Barnsley J, Gagnon D, et al. Using information communication technology in models of integrated community-based primary health care: learning from the iCOACH case studies. Implement Sci. 2018;13:1–14. doi:10.1186/s13012-018-0780-3
42. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to implementation science for the non-specialist. BMC Psychol. 2015;3:1–12. doi:10.1186/s40359-015-0089-9
43. Moses H 3rd, Matheson DH, Cairns-Smith S, George BP, Palisch C, Dorsey ER. The anatomy of medical research: US and international comparisons. JAMA. 2015;313(2):174–189. doi:10.1001/jama.2014.15939
44. Geng EH, Peiris D, Kruk ME. Implementation science: relevance in the real world without sacrificing rigor. PLoS Med. 2017;14(4):1–5. doi:10.1371/journal.pmed.1002288
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.