")
Back to Journals » Open Access Journal of Clinical Trials » Volume 15
A Multidomain Intervention Program for Older People with Dementia: A Pilot Study
Authors Xuan Nguyen T , Thi Thanh Vu H , Nguyen T, Esterman A , Viet Tran L, Thillainadesan J, Naganathan V, Brodaty H, Trung Nguyen A
Received 1 January 2023
Accepted for publication 29 March 2023
Published 17 April 2023 Volume 2023:15 Pages 1—10
DOI https://doi.org/10.2147/OAJCT.S403282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Thanh Xuan Nguyen,1,2 Huyen Thi Thanh Vu,1,2 Tuan Nguyen,3– 6 Adrian Esterman,5 Luc Viet Tran,1,2 Janani Thillainadesan,7,8 Vasikaran Naganathan,7,8 Henry Brodaty,9 Anh Trung Nguyen1,2
1Scientific Research Department, National Geriatric Hospital, Hanoi, 10000, Vietnam; 2Department of Geriatrics, Hanoi Medical University, Hanoi, 10000, Vietnam; 3Division of Social Gerontology, National Ageing Research Institute, Parkville, VIC, 3050, Australia; 4School of Health Sciences, Swinburne University of Technology, Hawthorn, VIC, 3122, Australia; 5UniSA Clinical & Health Sciences, University of South Australia, Adelaide, SA, 5001, Australia; 6Health Strategy and Policy Institute, Ministry of Health of Vietnam, Hanoi, 10000, Vietnam; 7Department of Geriatric Medicine and Centre for Education and Research on Ageing (CERA), Concord Hospital, Sydney, NSW, Australia; 8Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia; 9Centre for Healthy Brain Ageing (CHeBA), Discipline of Psychiatry and Mental Health, UNSW, Sydney, NSW, Australia
Correspondence: Thanh Xuan Nguyen, Scientific Research Department, National Geriatric Hospital, 1A, Phuong Mai, Dong Da, Hanoi, 10000, Vietnam, Tel +84 983277646, Email [email protected]
Background: Multidomain interventions have been shown to be effective in improving cognition, quality of life, reducing neuropsychiatric symptoms and delaying progression of functional impairment or disability in dementia patients. To investigate the multidomain intervention in other populations and diverse cultural and geographical settings, this pilot study will assess the feasibility of a multidomain intervention for older people with dementia in nursing homes in Vietnam.
Methods: Participants will be randomized into two equal groups, to receive either a multidomain intervention (intervention group) or regular health advice (control group). The intervention will include physical, cognitive, and social interventions as well as management of metabolic and vascular risk factors. We will hypothesize that the multidomain intervention will be feasible in Vietnam, and participants who receive the intervention will show improvement in quality of life, behaviors, functional ability, cognitive function, sleep, and in reduction of falls, use of healthcare services, and death rate compared to those in the control group during the 6 months intervention period and after the 6 months extended follow-up.
Discussion: This is the first study to evaluate the feasibility of a multidomain intervention program for older people with dementia in nursing homes in Vietnam. The results from the trial will inform clinicians and the public of the possibility of comprehensive treatment beyond simply drug treatments for dementia. This paves the way for further studies to evaluate the long-term effects of multidomain interventions in dementia patients. Furthermore, the research results will provide information on the effectiveness of multidomain interventions which will inform policy development on dementia.
Trial Registration: The trial is registered with ClinicalTrials.gov identifier: NCT04948450 on 02/07/2021.
Keywords: dementia, multidomain, intervention, feasibility
Background
Dementia is a syndrome characterized by cognitive decline interfering with daily function.1,2 Alzheimer’s disease and vascular dementia are the commonest causes of dementia separately or in combination accounting for over 80% of all dementia cases.3 Dementia is one of the major causes of disability and dependency among older people worldwide.4 The number of deaths due to dementia increased by 148% (140–157%) between 1990 and 2016.5 Dementia has significant social and economic implications in terms of direct medical and social care costs, and the costs of informal care. In 2020, the total global societal cost of dementia was more than 1 trillion USD.6
Medications for dementia are considered to be only modestly effective.7 The most commonly prescribed drugs are acetylcholinesterase inhibitors (AChEIs), and N-methyl-
In Vietnam, the older adult population is increasing rapidly in both absolute and relative numbers with the average lifespan increasing by four to 75 years in the last two decades. The prevalence of cognitive symptoms of dementia in adults aged 60 years and above is relatively high in Vietnam (14.4–46.4%)23,24 with an estimated 2.4 million people living with dementia in Vietnam by 2050.25 Advancing the mental health of older people in Vietnam is critical in the face of population growth and increased living standards resulting in longer lifespan. In the first Vietnam National Dementia Conference, dementia was recognized as a public health priority in Vietnam.26 The number of older people living in nursing homes is increasing in Vietnam, in which the percentage of people with dementia accounts for the majority. However, there was limited evidence on multifactorial intervention program for people with dementia in nursing homes in Vietnam. In order to improve treatment effectiveness, reduce symptoms and improve the quality of life of patients with dementia and their caregivers, we plan to conduct a pilot study to investigate the feasibility of a multidomain intervention program (physical; cognitive; social and management of metabolic and vascular risk factors) for older people with dementia in nursing homes.
Objectives
Primary
To assess the feasibility of a multidomain intervention program (physical, cognitive, social and management of metabolic and vascular risk factors) for older people with dementia in nursing homes.
Secondary
To investigate the effect of a multidomain intervention program on behavioral and psychological symptoms, quality of life, functional ability, falls and sleep, frailty, global cognition and the specific cognitive domains of attention, memory, fluency and executive function; utilization of healthcare services, and death rate for older people with dementia.
Method
Trial Design and Participants
This is a two-armed 12-month, multicenter, randomized controlled pilot study, based in nursing homes in Hanoi, Vietnam.
Inclusion Criteria
We aim to enroll participants aged over 60 years, living in nursing homes who have a diagnosis of major neurocognitive disorder (according to DSM 5 criteria),27 stage mild to moderate (according to Clinical Dementia Rating).28 Participants receiving pharmacological treatment for dementia must be on a stable dose for at least 3 months prior to the study. Eligible participants must be able to mobilize independently with or without a mobility aid and without physical assistance.
Exclusion Criteria are
- Acute and malignant diseases (eg, advanced cancers, end-stage chronic diseases, acute myocardial infarction, stroke)
- Symptomatic cardiovascular disease or coronary revascularization within 1 year
- Clinical evidence of schizophrenia, severe depression, psychiatric or bipolar disorder (according to DSM-V TR criteria)29
- Alcoholism or substance dependence (according to DSM-5 criteria),30 currently, or within the past 2 years
- Severe loss of vision, hearing or communicative ability (according to the interRAI Community Health Assessment)31
- Participant or family unwilling to participate in the study.
Recruitment
Participants will be recruited from November 2022 until December 2023.
Research Team
The research team consists of 5 researchers, 2 research assistants, 2 neurologists and 2 physiotherapy experts. Prior to recruiting participants, the research assistants will complete a training program in screening and data collection using the specific measures to be used in the study.
Sample Size Estimates
Assuming a standardised effect sizes (ES) of 0.232 for a pilot randomised trial, with 90% power and two-sided 5% significance, and allowing for a 10% dropout rate and 5% mortality, the final sample size to be recruited is 60 (30 per study arm).
Randomisation, Concealment, and Allocation
A concealed, computer-generated sequence of randomly permuted blocks (block size = 8), stratified by age (60–69, 70–79, 80 and over) and disease severity (mild or moderate) will be generated by a statistician not otherwise involved in the study. Randomization will occur at the completion of the entire baseline assessment.
Blinding
Participants will be informed that they will be randomly assigned to one of the two treatment groups by the research assistants. Investigators will be blinded to the intervention allocation. All outcome measures will be administered by blinded assessors.
Study Procedure
The study PI and/or researchers in the research team will contact adults aged 60 years and older in the nursing homes (Orihome, Nhan Ai, Dien Hong) to introduce the study. If they are interested in participating, the study PI and/or researchers in the research team will screen them for their eligibility. If they meet the inclusion criteria and are interested in participating, written informed consent will be obtained. Participants will be evaluated for capacity to give informed consent. If participants have the capacity to consent to the research project, they will receive a complete explanation of the purpose, risks, and procedures of the study and sign a written informed consent. Otherwise, a family member will consent for them.
A screening log will be kept to document number and reasons of participants who do not meet the inclusion criteria, decline to participate, or any other reasons.
Participants who agreed to participate in the study will be randomized into two equal groups, to receive either a multidomain intervention (intervention group) or regular health advice (control group). The intervention will include physical, cognitive, and social interventions, and management of metabolic and vascular risk factors.
The patients in the intervention group and the control group will be still participating in the usual care and activity, which were consistent across all three nursing homes in the study. The activities including quizzes and movement games will be held every 3 months. They will also be doing 15-minute morning exercise every day with light intensity. Participants in both the intervention and the control groups will be treated for dementia according to the recommendations of the Vietnam Alzheimer Disease and Neurocognitive Disorders Association.
All participants will meet the study physician to have an examination at baseline, 3 months and 6 months. At each examination, participants will undergo a physical examination, anthropometry (weight, and hip and waist circumference), blood pressure determination, pulse rate and rhythm check, assessment for cardiovascular risk factors and metabolic diseases (smoking, drinking, hypertension, coronary artery disease, dyslipidemia, atherosclerosis, diabetes) and assess blood test results (lipid profile, HbA1C and fasting glucose if patients have diabetes). Blood pressure measurements will be made on the left arm of the seated participants with a sphygmomanometer and an appropriately sized cuff; the average of 2 physician-obtained measures constitute the examination blood pressure. Metabolic and vascular risk factors will be ascertained by self-report (or caregivers report/nursing home report). Diabetes is defined as fasting glucose >7 mmol/l or use of insulin or oral hypoglycemic medications. Hypertension is defined as a systolic blood pressure of 140 mm Hg or more, or a diastolic blood pressure of 90 mm Hg or more, or taking antihypertensive medication. Dyslipidemia is defined as having an increased level of triglycerides, total cholesterol, or low-density lipoprotein cholesterol (LDL-C) or decreased level of high-density lipoprotein cholesterol (HDL-C). Results will be provided to participants and their doctors.
Interventions
The Intervention Group
In addition to what is given to both groups, the participants in the intervention group will receive three intervention components in 6 months: (1) physical activity; (2) cognitive intervention; and (3) social intervention as well as (4) management of metabolic and vascular risk factors. Physical activity and cognitive stimulation interventions will be performed at separate sessions.
Physical Activity Intervention
Progressive resistance training (PRT) for the physical intervention will be provided at the nursing home for 45 minutes twice a week. The sessions will be organized in groups (10 patients/group) and supervised by 2 physiotherapists. Within each small group (maximum 10) participants will follow the program tailored to their individual functioning level, with constant oversight by trainers.
The exercise program consists of progressive resistance training. Participants will progress through the 6-month intervention, guided by daily ratings of perceived exertion (15–18) on the Borg Scale.33
People with dementia and their care staff will be instructed to follow the prescribed PRT exercises for the rest of the week. Participants will be encouraged to exercise daily. Physiotherapists will determine progress subjectively based on the ability of the person with dementia. Training volume will be monitored by adding up the total minutes of participation during each day of the prescribed program.
Cognitive Intervention
The study subjects will receive cognitive intervention based on Cognitive Stimulation Therapy34 with rehabilitation experts. The intervention involves 14 sessions of themed activities, which typically run twice weekly. The sessions will be organized in groups (10 patients/group).
Each session lasts about 45 minutes. To make sure that there is continuity between the sessions they will follow the same structure: introduction (10 minutes), main activity (25 minutes) and conclusion (10 minutes). A total set of 14 exercises will be selected including physical games, sounds, childhood, food, current affairs, word association, being creative, categorising objects, orientation, using money, number game, word games, team quiz, which will be culturally adapted in Vietnam. Necessary activities related to daily lives will also be included. People with dementia and their care staff will be instructed on how to practice the various activities at their nursing home for the rest of the week in a separate room. Training volume (multiplying the number of repetitions performed/day by the number of days) will be monitored using a training diary.
Social Intervention
Social intervention will be combined with physical and cognitive interventions through doing these interventions in a group, ie, playing group games during exercises (eg, dancing, throwing ball to each other) or doing cognitive stimulation therapy in a group.
Management of Metabolic and Vascular Risk Factors
In the intervention group, metabolic and vascular risk factors will be evaluated by cardiologists and endocrinologists in the study.
Study physicians will assess change in blood pressure, weight and BMI, and hip and waist circumference, blood tests (glucose, lipid parameters, fasting glucose and HbA1C if the person with dementia has diabetes) at 3 and 6 months.
Participants in the intervention group will be provided with information on the importance of reducing risk factors, guidance on lifestyle changes and prescribing treatment if necessary by the cardiologists and endocrinologists. The target for blood pressure is less than 120/90 mmHg and the target for HbA1c is less than 8%.
The Control Group
The control group will receive general health advice every 3 months based on their physical examination and blood findings. They will be provided usual care plus health education materials.
Outcome Measurements
All outcome measures will be administered at baseline, 6 months and extended follow-up at 12 months. The outcomes are shown in Table 1.
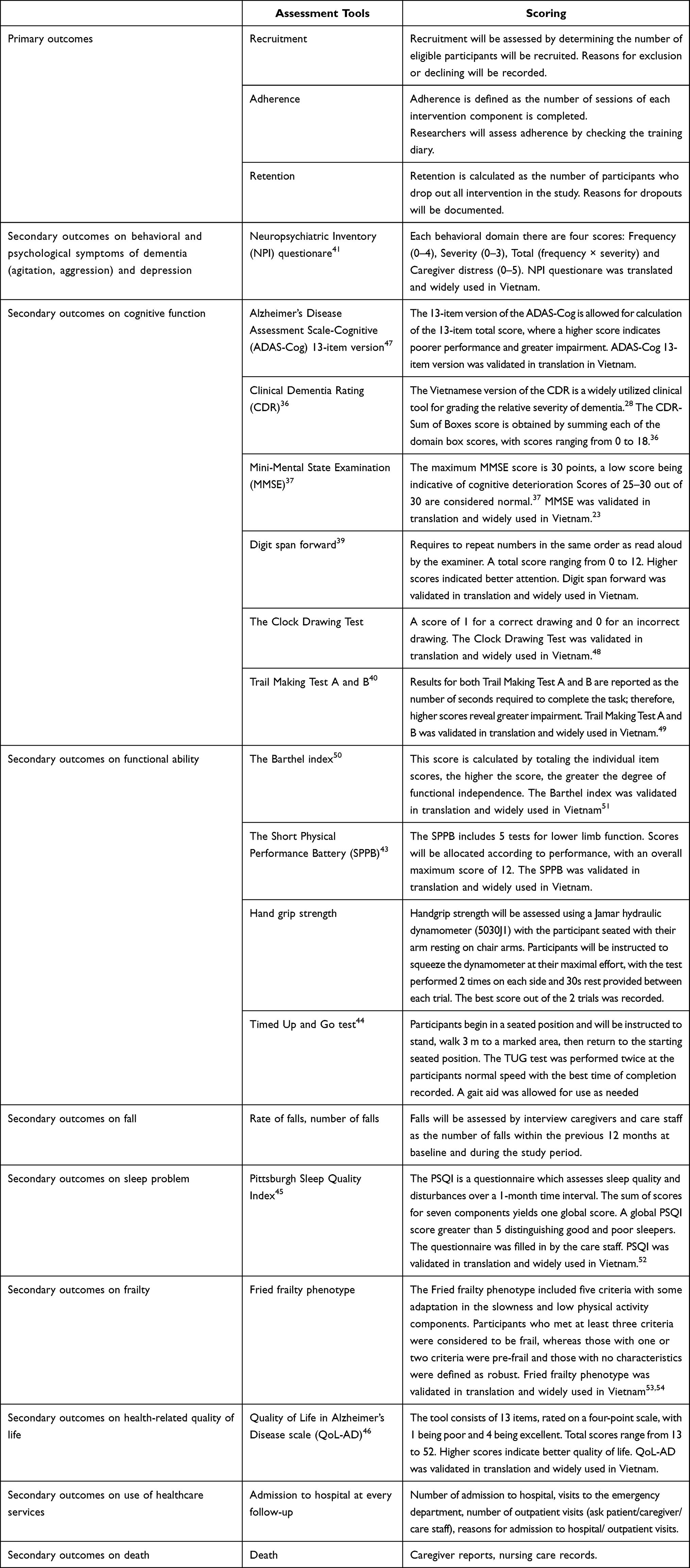 |
Table 1 Primary and Secondary Outcome Measures for Patients |
Primary Outcome
The primary outcome of the study is the feasibility of the intervention which will be assessed via the recruitment, adherence and retention.
Secondary Outcomes
Cognitive Function
Global cognition will be measured by Alzheimer’s Disease Assessment Scale-Cognitive (ADAS-Cog) 13-item version.35 Dementia severity will be assessed by the sum of boxes method of the Clinical Dementia Rating scale (CDR).36 Cognition will be assessed globally by the Mini-Mental State Examination (MMSE)37; executive function by the Clock drawing plus Trails B38; and attention by digit span forward39 and Trials A test.40
Behavioral and Psychological Symptoms of Dementia (BPSD) (Agitation, Aggression, Depression)
Researchers will interview care staff using the Neuropsychiatric Inventory (NPI) questionnaire to assess BPSD.41
Functional Ability
Functional ability will be assessed by using the Activities of Daily Living Scale (ADL), the Instrumental Activities of Daily Living Scale (IADL),42 the Short Physical Performance Battery (SPPB),43 handgrip strength, Timed Up & Go (TUG) test.44
Falls
Falls will be assessed by number of falls within the previous 12 months at baseline and during the study period.
Sleep Problem
Sleep Problem will be assessed with the Pittsburgh Sleep Quality Index.45
Health-Related Quality of Life
Health-related quality of life will be assessed with the Quality of Life in Alzheimer’s Disease scale (QoL-AD).46
Use of Healthcare Services
Use of healthcare services will be assessed through the number of admissions to hospital and visits to the emergency department.
Death
Death will be assessed through caregiver reports or nursing home records.
Statistical Analysis
The adherence rate for each intervention will be calculated by adding the number of sessions completed and dividing by the total number of intervention sessions assigned to each intervention component: physical activity intervention, cognitive intervention, vascular and metabolic risk factor management. The total adherence rate will be calculated by adding the number of sessions completed across all intervention components and dividing by the total number of intervention sessions assigned without modifying the weight of each intervention component. Regarding the participants who drop out of the study, adherence rates will be calculated until the dropout point. Chi-square test will used for categorical variables and a one-way analysis of variance for continuous variables to compare baseline characteristics between the groups. The chi-square test will be used to compare the retention rates between the intervention and control groups.
The secondary outcomes will be analyzed using a mITT population. Simple and multivariate linear and logistic regression models will be used to assess the relationships and risk factors for changes in secondary outcomes. Statistical analyses were performed using SPSS 26.0 (SPSS, Chicago, IL, USA). P < 0.05 was considered significant.
Discussion
This is the first study to evaluate the feasibility of a multidomain intervention program for older people with dementia in nursing homes in Vietnam. Participants will be followed-up for 6 months after the end of the 6-month intervention; and longer if further funding becomes available. The results from the trial will inform clinicians and the public of the possibility of comprehensive treatment beyond simple drug treatments for dementia. This will pave the way for further studies to evaluate the long-term effects of multidomain interventions in dementia patients. Furthermore, the research results will provide information on the effectiveness of multidomain interventions which will inform policy development on dementia.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent
Ethical approval has been performed in accordance with the Declaration of Helsinki and have been approved from the Hanoi Medical university (IRB00003121) on December 31, 2020. Participants will be evaluated for capacity to give informed consent. If participants have the capacity to consent to the research project, they will receive a complete explanation of the purpose, risks, and procedures of the study and sign a written informed consent. Otherwise, a family member will consent for them. The trial is registered with ClinicalTrials.gov identifier: NCT04948450 registered on 02/07/2021.
Acknowledgments
Research is supported and helped by the Board of Directors and medical staff at the Dien Hong, Nhan Ai and Orihome nursing care in Vietnam. We are grateful to Hoa L. Nguyen for valuable suggestions on this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Thanh Xuan Nguyen was funded by Vingroup JSC and supported by the Master, PhD Scholarship Programme of Vingroup Innovation Foundation (VINIF), Institute of Big Data, code VINIF.2021.TS.139. Research reported in this publication was supported by the National Institute of Aging (NIA) of the National Institutes of Health (NIH) under award number R01AG064688 (Hinton/Nguyen MPI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIA and the NIH. The sponsors had no role in the design and conduct of the study, in the collection, analysis, and interpretation of data, in the preparation of the manuscript or in the review or approval of the manuscript.
Disclosure
Professor Henry Brodaty reports personal fees from Biogen, Eisai, Roche, Skin2Neuron, and Cranbrook Care, outside the submitted work. All authors declare no other conflicts of interest in this work.
References
1. Emmady PD, Tadi P. Dementia. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC; 2022.
2. Duong S, Patel T, Chang F. Dementia: what pharmacists need to know. Can Pharm J. 2017;150(2):118–129. doi:10.1177/1715163517690745
3. Ott A, Breteler MM, van Harskamp F, et al. Prevalence of Alzheimer’s disease and vascular dementia: association with education. The Rotterdam study. BMJ. 1995;310(6985):970–973. doi:10.1136/bmj.310.6985.970
4. Vu K, Claggett BL, John JE, et al. Depressive symptoms, cardiac structure and function, and risk of incident heart failure with preserved ejection fraction and heart failure with reduced ejection fraction in late life. J Am Heart Assoc. 2021;10(23):e020094. doi:10.1161/JAHA.120.020094
5. Nichols E, Szoeke CEI, Vollset SE; Collaborators GBDD. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88–106. doi:10.1016/S1474-4422(18)30403-4
6. Wimo A, Guerchet M, Ali G-C, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2016;13:1–7.
7. Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimer’s Dis. 2020;76(2):579–589. doi:10.3233/JAD-200133
8. van de Glind EM, van Enst WA, van Munster BC, et al. Pharmacological treatment of dementia: a scoping review of systematic reviews. Dement Geriatr Cogn Disord. 2013;36(3–4):211–228. doi:10.1159/000353892
9. Yiannopoulou KG and Papageorgiou SG. Current and Future Treatments in Alzheimer Disease: An Update. J Cent Nerv Syst Dis. 2020;12. doi:10.1177/1179573520907397
10. Boongird C, Tearneukit W, Wongpipathpong W, McKay GJ, Thakkinstian A. Efficacy of pharmacotherapy and non-pharmacotherapy of Alzheimer dementia: a protocol for systematic review and meta-analysis. Medicine. 2022;101(50):e32382. doi:10.1097/MD.0000000000032382
11. Zucchella C, Sinforiani E, Tamburin S, et al. The multidisciplinary approach to Alzheimer’s disease and dementia. A narrative review of non-pharmacological treatment. Front Neurol. 2018;9:1058. doi:10.3389/fneur.2018.01058
12. Kallio E-L, Öhman H, Kautiainen H, Hietanen M, Pitkälä K, Pike K. Cognitive training interventions for patients with Alzheimer’s disease: a systematic review. J Alzheimer’s Dis. 2017;56:1349–1372. doi:10.3233/JAD-160810
13. Cafferata RMT, Hicks B, von Bastian CC. Effectiveness of cognitive stimulation for dementia: a systematic review and meta-analysis. Psychol Bull. 2021;147(5):455–476. doi:10.1037/bul0000325
14. Bahar‐Fuchs A, Martyr A, Goh AMY, Sabates J, Clare L. Cognitive training for people with mild to moderate dementia. Cochrane Database Syst Rev. 2019;(3). doi:10.1002/14651858.CD013069.pub2
15. Li X, Guo R, Wei Z, Jia J, Wei C. Effectiveness of exercise programs on patients with dementia: a systematic review and meta-analysis of randomized controlled trials. Biomed Res Int. 2019;2019:2308475. doi:10.1155/2019/2308475
16. Huntley JD, Gould RL, Liu K, Smith M, Howard RJ. Do cognitive interventions improve general cognition in dementia? A meta-analysis and meta-regression. BMJ Open. 2015;5(4):e005247. doi:10.1136/bmjopen-2014-005247
17. Yorozuya K, Kubo Y, Tomiyama N, Yamane S, Hanaoka H, Systematic A. Review of multimodal non-pharmacological interventions for cognitive function in older people with dementia in nursing homes. Dement Geriatr Cogn Disord. 2019;48(1–2):1–16. doi:10.1159/000503445
18. He W, Wang M, Jiang L, Li M, Han X. Cognitive interventions for mild cognitive impairment and dementia: an overview of systematic reviews. Complement Ther Med. 2019;47:102199. doi:10.1016/j.ctim.2019.102199
19. Rosenberg A, Mangialasche F, Ngandu T, Solomon A, Kivipelto M. Multidomain interventions to prevent cognitive impairment, Alzheimer’s disease, and dementia: from FINGER to World-Wide FINGERS. J Prevent Alzheimer’s Dis. 2020;7(1):29–36. doi:10.14283/jpad.2019.41
20. Kim HJ, Yang Y, Oh JG, et al. Effectiveness of a community-based multidomain cognitive intervention program in patients with Alzheimer’s disease. Geriatr Gerontol Int. 2016;16(2):191–199. doi:10.1111/ggi.12453
21. Barbera M, Ngandu T, Levälahti E, et al. Effect of multidomain interventions on estimated dementia and cardiovascular risk reduction: an individual‐participant data meta‐analysis from FINGER, MAPT, and pre‐DIVA: prevention: ADRD prevention research: who is at risk and who benefits more? Alzheimer’s Dement. 2020;16. doi:10.1002/alz.039287
22. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358(6):580–591. doi:10.1056/NEJMoa0706245
23. Ngoc-Bich N, Dung N, Vu T, et al. Dementia and associated factors among the elderly in Vietnam: a cross-sectional study. Int J Ment Health Syst. 2019;13:13. doi:10.1186/s13033-019-0269-8
24. Nguyen T, Than T, McFarland P, et al. Dementia prevalence among older hospitalized patients in Vietnam and dementia understanding of their caregivers. Aging Med Healthcare. 2019;10:128–132. doi:10.33879/AMH.2019.123-1902.003
25. Nguyen TA, Pham T, Vu HTT, et al. Use of potentially inappropriate medications in people with dementia in Vietnam and its associated factors. Am J Alzheimer’s Dis Other Dement. 2018;33(7):423–432. doi:10.1177/1533317518768999
26. Nguyen TA, Pham T, Dang TH, et al. Towards the development of Vietnam’s national dementia plan-the first step of action. Australas J Ageing. 2020;39(2):137–141. doi:10.1111/ajag.12755
27. Hugo J, Ganguli M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. 2014;30(3):421–442. doi:10.1016/j.cger.2014.04.001
28. Nguyen VT, Quach THT, Pham AG, Tran TC. Feasibility, reliability, and validity of the Vietnamese version of the clinical dementia rating. Dement Geriatr Cogn Disord. 2019;48(5–6):308–316. doi:10.1159/000506126
29. Cosgrove VE, Suppes T. Informing DSM-5: biological boundaries between bipolar I disorder, schizoaffective disorder, and schizophrenia. BMC Med. 2013;11:127. doi:10.1186/1741-7015-11-127
30. Hasin DS, O’Brien CP, Auriacombe M, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170(8):834–851. doi:10.1176/appi.ajp.2013.12060782
31. Urqueta Alfaro A, Guthrie DM, Phillips NA, et al. Detection of vision and /or hearing loss using the interRAI Community Health Assessment aligns well with common behavioral vision/hearing measurements. PLoS One. 2019;14(10):e0223123. doi:10.1371/journal.pone.0223123
32. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057–1073. doi:10.1177/0962280215588241
33. Williams N. The Borg Rating of Perceived Exertion (RPE) scale. Occup Med. 2017;67(5):404–405. doi:10.1093/occmed/kqx063
34. Streater A, Spector A, Aguirre E, et al. Maintenance Cognitive Stimulation Therapy (CST) in practice: study protocol for a randomized controlled trial. Trials. 2012;13:91. doi:10.1186/1745-6215-13-91
35. Mohs RC, Knopman D, Petersen RC, et al. Development of cognitive instruments for use in clinical trials of antidementia drugs: additions to the Alzheimer’s Disease Assessment Scale that broaden its scope. The Alzheimer’s Disease Cooperative Study. Alzheimer Dis Assoc Disord. 1997;11(Suppl 2):S13–S21. doi:10.1097/00002093-199700112-00003
36. O’Bryant SE, Waring SC, Cullum CM, et al. Staging dementia using Clinical Dementia Rating Scale Sum of Boxes scores: a Texas Alzheimer’s research consortium study. Arch Neurol. 2008;65(8):1091–1095. doi:10.1001/archneur.65.8.1091
37. Mitchell A. The Mini-Mental State Examination (MMSE): an update on its diagnostic validity for cognitive disorders. In: Cognitive Screening Instruments: A Practical Approach. Vol. 339. Springer; 2013:15–46.
38. Spenciere B, Alves H, Charchat-Fichman H. Scoring systems for the Clock Drawing Test: a historical review. Dement Neuropsychol. 2017;11(1):6–14. doi:10.1590/1980-57642016dn11-010003
39. Groth-Marnat G, Baker S. Digit span as a measure of everyday attention: a study of ecological validity. Percept Mot Skills. 2003;97(3_suppl):1209–1218. doi:10.2466/pms.2003.97.3f.1209
40. Arbuthnott K, Frank J. Trail making test, part B as a measure of executive control: validation using a set-switching paradigm. J Clin Exp Neuropsychol. 2000;22(4):518–528. doi:10.1076/1380-3395(200008)22:4;1-0;FT518
41. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory. Comprehen Assess Psychopathol Dement. 1994;44(12):2308.
42. Katz S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–727. doi:10.1111/j.1532-5415.1983.tb03391.x
43. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. doi:10.1093/geronj/49.2.M85
44. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
45. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
46. Kahle-Wrobleski K, Ye W, Henley D, et al. Assessing quality of life in Alzheimer’s disease: implications for clinical trials. Alzheimer’s Dement. 2017;6:82–90.
47. Cogo-Moreira H, Krance SH, Black SE, et al. Questioning the meaning of a change on the Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog): noncomparable scores and item-specific effects over time. Assessment. 2020;28(6):1708–1722.
48. Vu HTT, Nguyen TTH, Le TA, et al. Comprehensive geriatric assessment in older patients with diabetes mellitus in Hanoi, Vietnam. Gerontology. 2022;68(10):1132–1138. doi:10.1159/000521601
49. Beckham JC, Crawford AL, Feldman ME. Trail making test performance in Vietnam combat veterans with and without posttraumatic stress disorder. J Trauma Stress. 1998;11(4):811–819. doi:10.1023/A:1024409903617
50. Mahoney F, Barthel DW. Functional evaluation; the Barthel index. A simple index of the Independence useful in scoring improvement in the rehabilitation of the chronically ill. Md State Med J. 1965;14:61–66.
51. Vo THM, Nakamura K, Seino K, Nguyen HTL, Van Vo T. Fear of falling and cognitive impairment in elderly with different social support levels: findings from a community survey in Central Vietnam. BMC Geriatr. 2020;20(1):141. doi:10.1186/s12877-020-01533-8
52. To N, Nguyen N. Validity of the Vietnamese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2015;16:S52. doi:10.1016/j.sleep.2015.02.128
53. Vu HTT, Nguyen TX, Nguyen TN, et al. Prevalence of frailty and its associated factors in older hospitalised patients in Vietnam. BMC Geriatr. 2017;17(1):216. doi:10.1186/s12877-017-0609-y
54. Nguyen AT, Nguyen TX, Nguyen TN, et al. The impact of frailty on prolonged hospitalization and mortality in elderly inpatients in Vietnam: a comparison between the frailty phenotype and the Reported Edmonton Frail Scale. Clin Interv Aging. 2019;14:381–388. doi:10.2147/CIA.S189122
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.