")
Back to Journals » Clinical Interventions in Aging » Volume 19
A Retrospective Study: Clinical Characteristics and Lifestyle Analysis of Chinese Senile Gluteal Dermatosis Patients
Authors Tang C, Lin P, Zhao Y, Wang P, Wang P
Received 28 November 2023
Accepted for publication 14 February 2024
Published 26 February 2024 Volume 2024:19 Pages 333—338
DOI https://doi.org/10.2147/CIA.S448026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Chenyu Tang,1 Ping Lin,2 Yige Zhao,1 Panpan Wang,1 Ping Wang3
1Department of Dermatology, Hangzhou Third People’s Hospital, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Gerontology, Hangzhou Third People’s Hospital, Hangzhou, People’s Republic of China; 3Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Ping Wang, Department of Dermatology, Hangzhou Third People’s Hospital, Xihu Avenue No. 38, Hangzhou, Zhejiang, 310009, People’s Republic of China, Tel +86-13588812862, Email [email protected]
Purpose: To summarize the clinical, histopathological and therapeutic features of senile gluteal dermatosis.
Patients and Methods: Retrospective analysis of 230 cases who visited the outpatient clinic of Hangzhou No. 3 People’s Hospital for skin lesions on the buttocks and hips from 2018.8– 2023.8 were included in the study, basic clinical information was collected, and they were subjected to physical examination of the buttocks and hips, and 36 cases were senile gluteal dermatosis, of which 7 underwent histopathological biopsy.
Results: A total of 230 patients were included, of which 36 were diagnosed with geriatric buttock dermatosis, with a mean age of (84.2± 12.6) years, mean body mass index of (21.7± 3.8) kg/m2, and a male to female ratio of 2:1. There was a significant correlation between the occurrence of the disease and age, gender, body mass index, sedentary time, type of chair used, and hypertension (P< 0.05). The severity of the lesions may be associated with longer sitting time and prolonged use of bamboo chairs (P< 0.05). Histopathologic changes were not specific. The skin lesions could subside after general treatment such as improvement of lifestyle, use of pressure-reducing air mattresses, salicylic acid cream, and moisturizing creams.
Conclusion: Senile gluteal dermatosis is a common senile physical dermatosis, mainly manifested as brownish scaly plaques, erythema and crusted ulcers, which can often be cured under reasonable treatment.
Keywords: skin diseases, physical, gluteal dermatosis, pressure injury, friction
Introduction
Senile Gluteal Dermatosis (SGD) is a common skin disease in the elderly, which was first reported by Yamamoto in Japan as a hyperkeratotic, mossy skin disease. The etiology of SGD is unclear and may be related to friction, shear and pressure. The characteristic lesions are brown scaly plaques above the gluteal cleft and on both sides of the buttocks, forming the typical “three corners of a triangle”.1 Previous studies have focused on elderly people in Japan and Korea, with a few reports from the West, but few studies have been conducted on Chinese people. Therefore, we collected 230 cases from the outpatient clinic of the Third People’s Hospital of Hangzhou City who visited the clinic because of skin lesions on the buttocks and hips, and evaluated them for SGD according to the characteristics of the skin lesions, of which 36 cases were diagnosed with SGD, and we analyzed and summarized their clinical, histopathological, and therapeutic characteristics.
Materials and Methods
Study Design
To analyze and draw conclusions on the clinical traits and way of life of Chinese elderly patients with gluteal dermatosis, a clinical retrospective study was conducted. We collected patients who sought treatment for lesions on their buttocks and hips at Hangzhou No. 3 People’s Hospital’s dermatology outpatient from August 2018 to August 2023. Approval for this study was obtained from the Ethics Committee of Hangzhou Third People’s Hospital (2021KA001). Based on a retrospective design of the study, the Ethics Committee of Hangzhou Third People’s Hospital waived informed consent and de-identified patient information.
Participants
Age, gender, height, weight, and underlying medical conditions were noted for 230 patients. Individuals with a history of autoimmune disorders, malignant tumors, or extended bed rest (eg apoplexy patients) were not accepted. Every participant underwent a thorough physical examination of their hips and buttocks and SGD assessment were conducted. Patients with lichen planus, cutaneous amyloidosis, or neurodermatitis were also disqualified.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation. All tests were two-sided, and a p-value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS 27.0 software. The patients were divided into SGD group and non-SGD group, and the data of sex, age, body mass index (BMI), daily sedentary time, and seat use (Chinese bamboo chair/sofa) were compared between the infected group and the control group using t–test and Chi-square test. SGD group was divided into ulcer group and non-ulcer group. t–test and Fisher exact test were used to analyze the relationship between BMI, daily sedentary time, seat use and skin lesions severity. SPSS 27.0 software was used for the above analysis.
Results
Patient Characteristics
Thirty-six patients, aged 59 to 101, 24 of whom were male and 12 of whom were female, were diagnosed with SGD out of the 230 total. The SGD group’s BMI was 21.7±3.8, and mean age was 84.2±12.6 years. Between the SGD group and the non-SGD group, there were statistically significant differences in age, BMI, male-to-female ratio, daily sitting time, and hypertension (P<0.05). Patients with ulcers were also found to spend more time sitting and using traditional bamboo chairs (P<0.05). (Tables 1 and 2) BID silver nitrate application.
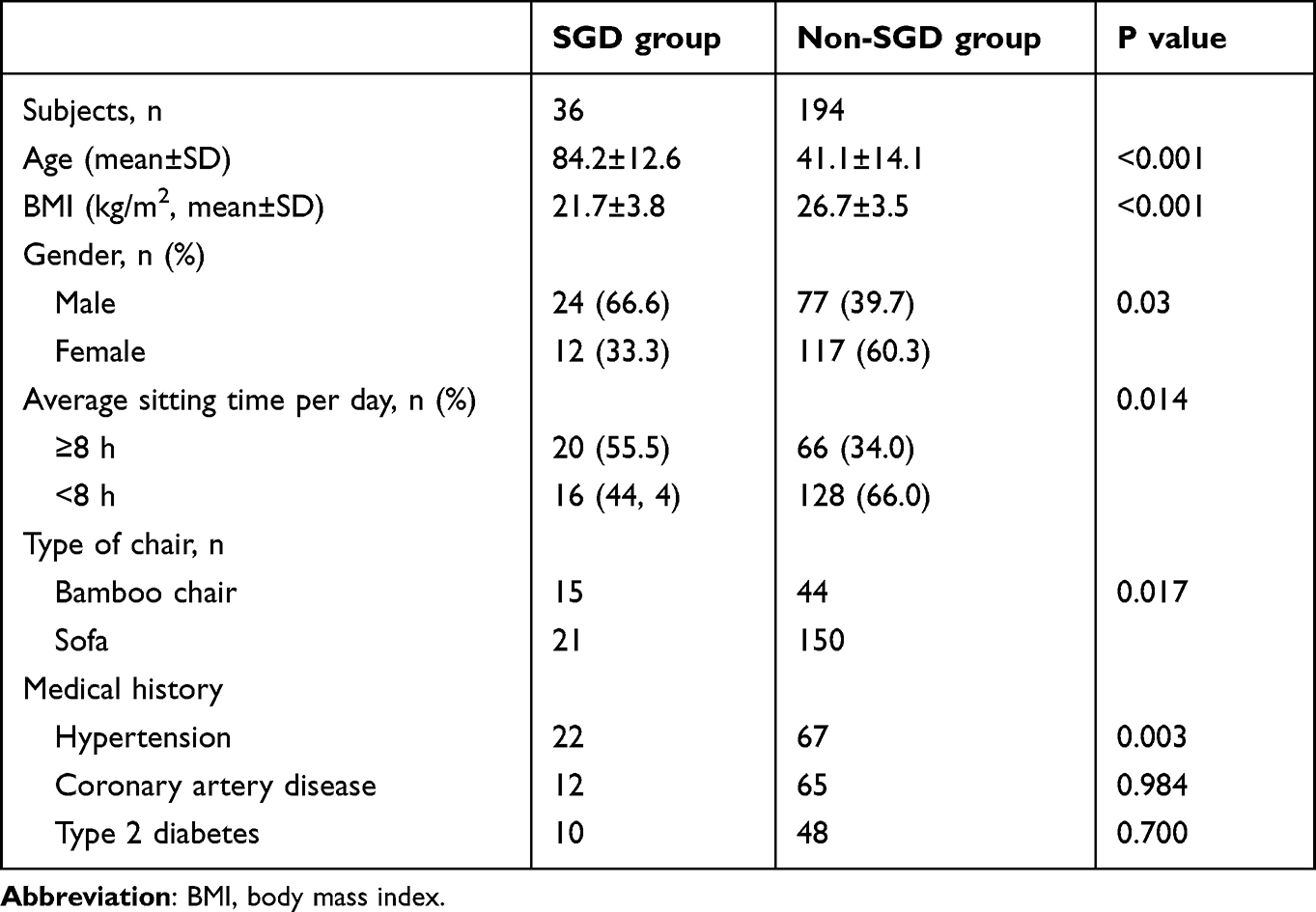 |
Table 1 Clinical Features of SGD Group and Non-SGD Group |
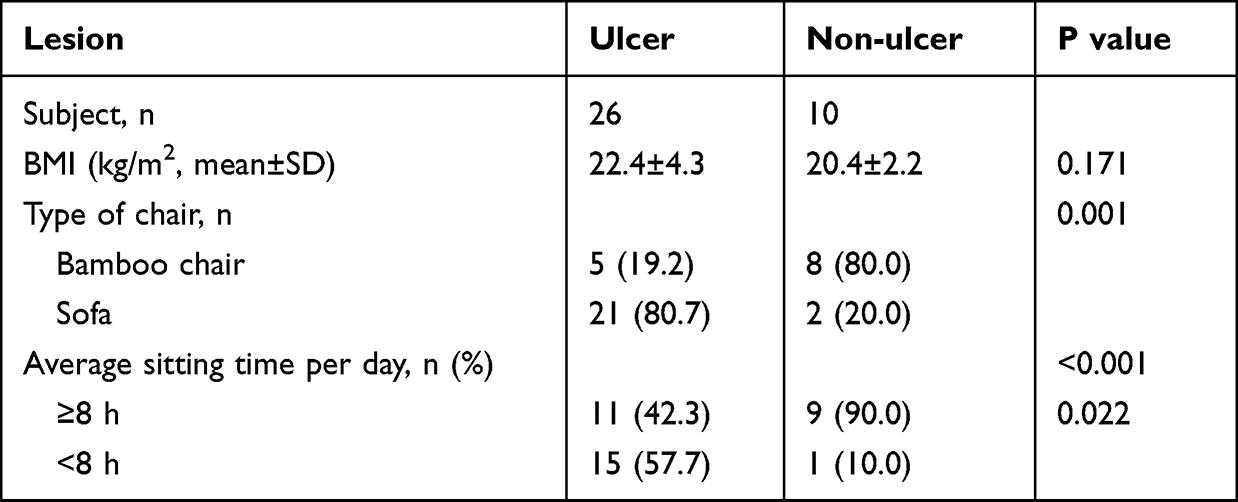 |
Table 2 Clinical Features of Ulcer Group and Non-Ulcer Group (Brownish Scaly Patch and Erythema) |
Clinical Features and Prognosis
Three lesions were observed in individuals with SGD: Thickened brownish scaly patches in 20 (55.5%) (Figure 1A), bleachable erythema in 6 (16.7%) (Figure 1B), and ulcers in 10 (27.8%) patients (Figure 1C). The skin corresponding to the coccyx (41.7%), Ischial tubercles (58.3%), the anterior superior iliac spine (2.8%) and the greater trochanter of the femur (2.8%). Six cases showed as “three corners of a triangle” (Figure 1A). Five patients (22.7%) and eight patients (22.2%) reported having mild pain and itching, respectively.
 |
Figure 1 Lesions of senile gluteal dermatosis (A) Thickened brownish scaly patches on gluteal cleft apex and both sides of the buttocks form “three corners of a triangle” with distinct horizontal ridges; (B): brownish scaly patches, erythema and shallow ulcers were seen in one patient; (C): A crusted ulcer can be seen on the skin corresponding to the greater trochanter of the femur. |
All patients included in the study had the ability to move autonomously and had no long history of immobilization. More than half (55.5%) of the cases diagnosed with SGD had sedentary habits (daily sitting time>8h), 13 patients used traditional Chinese bamboo chair for a long time. Two patients with lesions on the greater trochanter of femur and the anterior superior spine of iliac preferring lying on their side and prone at night.
We advised all patients to improve their lifestyle as much as possible, such as reducing sedentary time, using soft cushions to reduce pressure on lesions, and applying urea creams. The lesions of the patients with hyperkeratosis brownish scaly plaques were improved after application of 5% salicylic acid ointment, and the mean remission time was 2 months. After treatment with erythromycin ointment, and kangfuxin liquid, the mean remission time for erythema and ulcer patients was 2.8 and 3.4 months, respectively. One of the patients presented with resistant ulcers, which healed after 15 days by spraying 0.5% silver nitrate twice a day.
Histopathology
Seven skin biopsies were performed. Histopathologic changes were nonspecific and consisted mainly of epidermal hyperkeratosis, superficial dermal lymphocytic infiltration and dilatation and hyperplasia of small blood vessels. In patients with ulcers, superficial dermal lymphocytic infiltration as well as edema of dermal papillae were more pronounced, with pseudoepitheliomatous hyperplasia in two of them (Figure 2A–C). Pigment granules were seen in the superficial dermis of two patients, which stained positively for iron-containing hemorrhagic yellow.
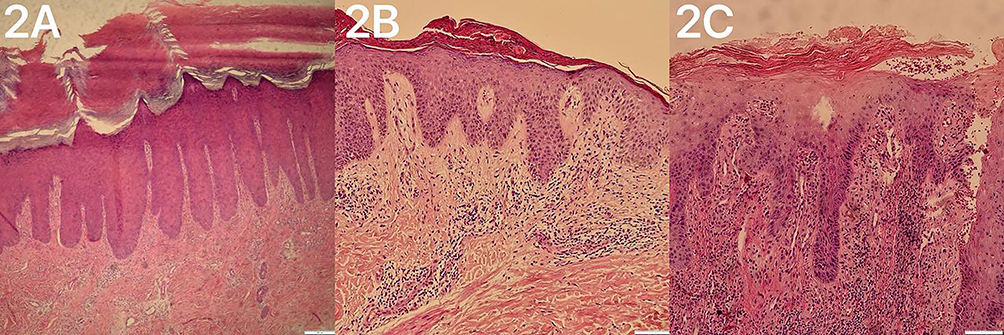 |
Figure 2 Pathological findings of SGD. (A) The brownish scaly plaque patients showed significant hyperkeratosis, some with epidermal psoriatic hyperplasia, and perivascular lymphocyte infiltration. (B) The pathological manifestations of erythema patients include mild hyperkeratosis, focal hyperkeratosis, focal mild spongy edema of the epidermis, and small to moderate amount of lymphocyte infiltration around superficial vessels of the dermis; (C) Pseudoepitheliomatous hyperplasia and massive perivascular lymphocyte infiltration were seen in patients with ulcers. |
Discussion
SGD is more common in East Asia, especially in Koreans and Japanese, and has been associated with repeated friction caused by their daily use of tatami mats and Korean mattresses.1,2 It was previously suggested that SGD is a form of cutaneous amyloidosis; however, most current studies have shown that SGD is a senile skin change, which is essentially a skin response to prolonged mechanical stimulation.3
SGD predominantly involves the gluteal cleft and both the sides of the buttocks and can also accumulate in the hips. Remarkably, unlike previous findings,1 all lesions involving the gluteal cleft were located at the apex of the gluteal cleft corresponding to the tailbone in this study. Lesions at other sites were in the skin at the bony prominences, as described above. Elderly males were the predominantly affected population, which may be attributed to physical differences between the genders. There is less subcutaneous fat at the bony prominences, and the proportion of fat in the gluteofemoral region is lower in men than in women,4 which makes them less well cushioned against external mechanical shocks and more susceptible to the effects of friction.2
Brownish scaly patch is the typical lesion of SGD, which is essentially a form of hyperkeratosis,3 with a rough, hard surface and visible horizontal ridges, which is a normal protective response of the skin to chronic friction.5,6 Liang et al 7 found that microischemia in the pressure zone of the bony prominence due to prolonged sitting stimulates reactive vascular proliferation in SGD, and we therefore hypothesized that the bleachable erythema may be caused by vascular proliferation and dilatation. Although the clinical and pathologic aspects of SGD are similar to those of early decubitus ulcer,1 the erythema of decubitus ulcers is often persistent and suggestive of necrosis of subcutaneous tissues,8 which is a key point of differentiation.
Ulcers may be related to the patient sitting for longer periods of time each day and the softness or hardness of the contact surfaces. The accumulation of external stresses deforms the tissues and poses a threat to the structural integrity of the tissues,9 and these factors promote skin dehiscence as well as the development of ulcers. However, we must emphasize that ulcers in SGD are generally shallow ulcers, and there is no obvious ischemia or necrosis of the deep tissues in terms of clinical manifestations and histopathology. Notably, there is often only one type of lesion in the same patient. While with the simultaneous presence of brownish scaly patch, erythema, and shallow ulcers in one patient (Figure 2B), we hypothesized that SGD lesions can evolve from mild to severe.
Studies have shown that surface friction is the main cause of skin lesions resembling class II pressure ulcers, and pressure and shear forces often cause deep tissue damage in class III or IV pressure ulcers.10 We believe that friction plays a dominant role in the pathogenic factors of SGD. There are many friction-related dermatosis in clinic, such as frictional melanosis, prayer markers,11 friction dermatitis, and clothing-related dermatitis.12 In these diseases, hyperpigmentation and hyperkeratosis are common, and ulcers are occasional. Some scholars have summarized and classified these diseases,12 and according to the classification basis, SGD is more like a primary friction dermatosis involving the gluteofemoral region.
Skin aging is a key factor in a variety of age-related dermatosis. Extensive studies have shown that the ability of the epidermis and dermis to resist external injuries and damage changes with age, especially the flattening of the epidermal dermal junction (DEJ), which reduces the ability of epidermal cells to proliferate, and there is an increase in skin brittleness,13 as well as an increase in the risk of skin tears14 and ulcers.15 Pressure-induced vasodilation (PIV) is a phenomenon in which cutaneous vasodilatation increases tissue perfusion in response to mechanical stresses caused by tissue compression,16 and the skin’s ability to PIV declines during skin aging. In addition, body fat is redistributed with age, with a general increase in trunk fat (mainly abdominal fat) and a decrease in subcutaneous fat.17 All of the above suggests that the skin of the elderly is more fragile and more vulnerable to friction, shear and pressure.
In this study, hypertension was significantly associated with SGD. We hypothesized that it might be related to the impaired skin microvascular responsiveness and dysfunction of vascular endothelial cells in hypertensive patients,18 which are more prone to microischemia in local tissues when stimulated by repeated mechanical stresses. Diabetes mellitus has also been previously found to be associated with SGD, with diabetic patients having reduced vascular reactivity to sympathetic nerves, and therefore to thermal and mechanical stress, and being more susceptible to injury from mechanical stimulation.2
In most cases of SGD, the histopathologic changes are more consistent and consist mainly of hyperkeratosis, echinodermal hyperplasia, superficial vascular proliferation, and dermal papillary dilatation with lymphocytic infiltration.1,2 In our study, pseudoepitheliomatous hyperplasia and massive lymphocytic infiltration could be seen in the more severe cases, and two patients showed positive staining for iron-containing hemosiderin granules, but Congo red staining was negative for amyloid deposition in all cases. We believe that all these histopathologic changes were nonspecific due to repetitive friction.
Previous case reports have reported that the application of retinoic acid and calcitriol improved SGD,19 and decompression devices such as inflatable or water-filled pads can also provide assistance.1 Our study showed that hyperkeratotic brown scaly plaques responded to 5% salicylic acid cream and relieved pruritus. The effect of silver nitrate on resistant ulcers may be due to its antibacterial properties, promoting angiogenesis and accelerating healing.20 In addition to medications, lifestyle improvements such as avoiding prolonged sitting and lying on the side to compress an area of the body, using soft cushions, moisturizing the skin, and ensuring that intimate clothing is soft and smooth are also important.
Conclusion
SGD is a prevalent skin condition among the elderly. In order to enhance the quality of life for the aged, dermatologists, geriatricians, community physicians, and nurses should focus more on SGD and do a good job of educating and realizing early diagnosis and treatment.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical standards of the Helsinki Declaration of 1975. This study was approved by the institutional review board of Hangzhou Third People’s Hospital (2021KA001). Based on a retrospective design of the study, the Ethics Committee of Hangzhou Third People’s Hospital waived informed consent and de-identified patient information. The study was conducted in accordance with relevant guidelines and regulations.
Acknowledgments
Thanks to Dr Ping Wang and Dr Ping Lin for providing the cases and figures.
Funding
Zhejiang Natural Science Foundation of China (LBZ22H160001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu H-N, Wang W-J, Chen -C-C, et al. Senile gluteal dermatosis: a clinical study of 137 cases. Int J Dermatol. 2014;53(1):51–55. doi:10.1111/j.1365-4632.2012.05702.x
2. H MS, K KB, H JK, et al. Analysis of clinical features and lifestyle in Korean senile gluteal dermatosis patients. Int J Dermatol. 2016;55(5):553–557. doi:10.1111/ijd.12838
3. Niiyama S, Sakurai S, Katsuoka K. Hyperkeratotic lichenified skin lesion of gluteal region. J Dermatol. 2006;33(11):779–782. doi:10.1111/j.1346-8138.2006.00186.x
4. DeFronzo RA, Tripathy D. Skeletal muscle insulin resistance is the primary defect in type 2 diabetes. Diabetes Care. 2009;32(Suppl 2):S157–163. doi:10.2337/dc09-S302
5. Freeman DB. Corns and calluses resulting from mechanical hyperkeratosis. Am Fam Physician. 2002;65(11):2277–2280.
6. Berke CT. Pathology and clinical presentation of friction injuries: case series and literature review. J Wound Ostomy Continence Nurs. 2015;42(1):47–61. doi:10.1097/WON.0000000000000087
7. W LM, L LJH, Y CH, et al. Reactive epidermal hyperplasia and angiogenesis of the rear (REAR): a proposed unifying name for senile gluteal dermatosis and prurigiform angiomatosis. Dermatopathology. 2022;9(4):343–354. doi:10.3390/dermatopathology9040040
8. E EL, M BJ, Goldberg M, et al. Revised national pressure ulcer advisory panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585–597. doi:10.1097/WON.0000000000000281
9. Wyatt T, Baum B, Charras G. A question of time: tissue adaptation to mechanical forces. Curr Opin Cell Biol. 2016;38:68–73. doi:10.1016/j.ceb.2016.02.012
10. Lahmann NA, Kottner J. Relation between pressure, friction and pressure ulcer categories: a secondary data analysis of hospital patients using CHAID methods. Int J Nurs Stud. 2011;48(12):1487–1494. doi:10.1016/j.ijnurstu.2011.07.004
11. A AA, Zouman A Y A, Al Hussaini H, et al. Prayer marks. Int J Dermatol. 2002;41(7):411–414. doi:10.1046/j.1365-4362.2002.01398.x
12. Arora G, Khandpur S, Bansal A, et al. Current understanding of frictional dermatoses: a review. Indian J Dermatol Venereol Leprol. 2023;89(2):170–188. doi:10.25259/IJDVL_519_2021
13. Bonifant H, Holloway S. A review of the effects of ageing on skin integrity and wound healing. Br J Community Nurs. 2019;24(Sup3):S28–S33. doi:10.12968/bjcn.2019.24.Sup3.S28
14. LeBlanc K, E CK, Wood E, et al. Best practice recommendations for prevention and management of skin tears in aged skin: an overview. J Wound Ostomy Continence Nurs. 2018;45(6):540–542. doi:10.1097/WON.0000000000000481
15. Leblanc K, Alam T, Langemo D, et al. Clinical challenges of differentiating skin tears from pressure ulcers. EWMA. 2016;16:17–23.
16. P R Z, S F M B, M C O, et al. A systematic review and meta-analysis of the pressure-induced vasodilation phenomenon and its role in the pathophysiology of ulcers. Plast Reconstr Surg. 2019;144(4):669e–681e. doi:10.1097/PRS.0000000000006090
17. Reinders I, Visser M, Schaap L. Body weight and body composition in old age and their relationship with frailty. Curr Opin Clin Nutr Metab Care. 2017;20(1):11–15. doi:10.1097/MCO.0000000000000332
18. Farkas K, Nemcsik J, Kolossváry E, et al. Impairment of skin microvascular reactivity in hypertension and uraemia. Nephrol Dial Transplant. 2005;20(9):1821–1827. doi:10.1093/ndt/gfh944
19. Wu X, Chong W-S. Not something to sit on: a case of senile gluteal dermatosis responding to calcipotriol ointment. Australas J Dermatol. 2022;63(3):e282–e284. doi:10.1111/ajd.13863
20. Martinez JD, Cardenas JA, Soria M. Role of silver nitrate spray for skin wound care in patients with toxic epidermal necrolysis: our experience in 4 patients. Life. 2023;13(12):2341. doi:10.3390/life13122341
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.