")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Standardized Physical Examination Method for Joints to Determine Rheumatoid Arthritis Activity Using the Modified RAND/UCLA Appropriateness Method
Authors Medina YF , Ruiz AJ, Rondon MA
Received 11 November 2022
Accepted for publication 25 January 2023
Published 8 May 2023 Volume 2023:16 Pages 1287—1299
DOI https://doi.org/10.2147/JMDH.S397038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yimy F Medina,1,2,* Alvaro J Ruiz,1,* Martin A Rondon1
1PhD Program in Clinical Epidemiology, Department of Clinical Epidemiology and Biostatistics, Pontificia Universidad Javeriana, Bogotá, Colombia; 2Rheumatology Unit, Internal Medicine, Universidad Nacional de Colombia, Bogotá, Colombia
*These authors contributed equally to this work
Correspondence: Yimy F Medina, Email [email protected]
Introduction: Rheumatoid arthritis activity is evaluated based on a physical examination of each of the joints. However, the joint examination is not standardized, and the techniques are variable and difficult to reproduce due to disagreements among examiners.
Objective: To recommend standardized joint examination techniques based on the modified RAND-UCLA appropriateness method.
Methods: A review of the literature was conducted to determine the items to be included in the joint examination; subsequently, a consensus of rheumatologists was achieved with the modified RAND-UCLA methodology to issue the recommendations. The diagnosis of RA and differential diagnoses were excluded.
Results: Two hundred fifteen rheumatologists were invited to participate. Five were included in the core group and 26 in the group of clinical experts. Clinical experience ranged between 2 and 25 years (mean 15.6 years; standard deviation 6.3 years). Most rheumatologists participated in all rounds (Round 1: 100%, Round 2: 61%, and Round 3: 61%). Of the 45 statements in the questionnaire assessing the examination techniques, 28 (62%) were retained. In addition, 6 other statements were included during the face-to-face meeting for a total of 34 final statements.
Conclusion: Physical examination techniques for joints that determine RA activity are heterogeneous and differ markedly in terms of several characteristics. A list of recommendations is proposed as a guide to improve and standardize the method for the physical examination of the joints. This standardization will improve the diagnosis and results for patients with RA and help health caregivers provide better treatment.
Keywords: rheumatoid arthritis, physical examination, joints, diagnosis, disease activity, consensus
Plain Language Summary
- The joint examination techniques proposed by consensus in this study describe the unified criteria for physical articular examination to assess the activity of patients with rheumatoid arthritis.
- The unified techniques of the physical examination of the joints will make it possible to improve their validity and reproducibility.
- This will allow patients with rheumatoid arthritis to be better diagnosed and therefore receive appropriate treatment.
- This consensus examination method may be useful for health professional as a standardized method for improving patient evaluation, as support for evidence-based decision-making, and as an educational tool.
Introduction
Rheumatoid arthritis (RA) is an autoimmune, chronic, systemic, and multifactorial disease1 characterized by inflammation, pain, and joint destruction that limits movement and functionality, decreases the quality of life and increases the risks of death and extra-articular manifestations.2,3
During follow-up or clinical monitoring of RA activity, each joint must be examined for swelling or pain.4,5 The objective of the periodic clinical follow-up of patients with RA is to evaluate the activity of the disease, which plays key roles in the treatment and the prognosis.6–8 Although the examination and counting of the 28 joints is the most frequently used method in clinical practice, the same examination and counting have been developed in clinical experiments, but others are added, for a total of 66/68 joints.8–10
In a systematic review of the physical examination of joints for the control of RA in patients, a lack of description of the techniques and explicit details was observed.11 Therefore, the joint evaluation is not standardized, leading to highly variable and poorly reproducible results.12,13 Consensus exercises have been proposed to improve the evaluation of the joints and the agreement between evaluators to standardize the technique.14–16 However, the methods for the joint examination are still not standardized.16,17
Given the complexity and variability of the joint examination in the follow-up of patients with RA, our objective was to identify the important elements that should be included in the joint examination techniques during the follow-up of patients with RA and to develop a standardized method using the modified RAND/UCLA (the RAND Corporation and the University of California Los Angeles) appropriateness method.
This exercise refers to physical examination of the joints to define them as inflamed (which is based on determining whether they are swollen or tender) when defining whether rheumatoid arthritis is active or not during follow-up. This exercise does not refer to scales to measure the activity of rheumatoid arthritis.
Materials and Methods
The study was approved and followed the ethical standards of the Ethical Research Committees of the Pontifical Xavierian University, San Ignacio University Hospital, Simón Bolívar Hospital, and Colombian National University Hospital and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Design and Summary of the Study
This study was conducted in the following stages:
- Review and summary of the literature.
- Conformation of the core group.
- Sending the literature review to the members of the core group.
- Construction of the initial questionnaire about the examination of the joints by the core group.
- Composition of the group of clinical experts participating in the ratings to whom the literature synthesis and the initial questionnaire were sent.
- Two rounds of qualification using the RAND-UCLA methodology.
- A third round of qualification outside of the RAND/UCLA methodology to enable a consensus to be reached for some joints that remained without a consensus among the total of the joints considered.
- Analysis and presentation of the results.
- Preparation of the final document.
The RAND-UCLA method is used to determine the appropriate use of an intervention or technology and combines a critical review of the literature with the opinions of clinical experts. It is based on the creation of necessary conditions for decision-making, the selection of the core group, and the definition of the preliminary document. Likewise, it is based on the clinical experts evaluating the questions and rating the questionnaire during the different rounds of the procedure. The use of the RAND-UCLA appropriateness method is justified by the scarcity of information and the uncertainty about the techniques for the physical examination of joints to define disease activity in adult patients with RA.18
Review and Summary of the Literature
A summary of the data obtained was based on the following collected evidence:
- A systematic review of the literature, that was published in 2018, was conducted. Articles that provided a detailed description of the physical examination or a description of the components of the joint examination of adult patients with RA were included. The criteria presented for the scrutiny were gathered from Medline, Embase, Lilacs, SciELO, Web of Science, National Technical Reports Library, and the resulting reference lists of relevant articles. No restrictions were established for the language or date of publication. Of 8322 references, 74 studies were included according to the selection criteria, and 6 references were finally included at the end of the review.11 A recent update of the search was performed, and no relevant articles published up to October 2022 were identified (Figure 1).
- The primary studies obtained from the systematic review of the literature published that presented the joint examination with some specification of the technique were analyzed.15,19–23 In addition, other studies were tracked by reviewing the reference lists of the retrieved studies.
- A survey of rheumatologists in Colombia about the concepts of a joint examination was conducted at the National Congress of Rheumatology.24
- Two secondary resources were obtained from the systematic review: the Eular Handbook of Clinical Assessment in Rheumatoid Arthritis25 and audiovisual material from the disease activity score of 28 joints (DAS28) quick reference guide for health professionals.26
- An article published by the principal investigator described the involvement of the pannus in the examination of the joint to determine RA activity.27
- Subsequently, the core group structured a final report, determined a concise definition of terms, and developed the questionnaire with the initial list of items.
 |
Figure 1 PRISMA flow diagram showing search updating. |
Composition of the Core Group and the Group of Clinical Experts
Rheumatologists who were members of the Colombian Association of Rheumatology (CAR) with at least one year of practice after graduation, of different ages and from various cities were summoned. Emails were sent through the CAR mail to those who met the eligibility criteria and were invited to participate in the core group and in the group of clinical experts.
Participant inclusion criteria: Rheumatologists of different ages residing in different cities who were members of the CAR with at least one year of practice in the profession after graduation in Colombia and with experience in studies of patients with RA were included in the core group.
For the group of clinical experts, rheumatologists of different ages residing in different cities who were members of the CAR with at least one year of practice in the profession after graduation in Colombia were recruited.
The focus of the core group was to identify the necessary elements for the performance of the joint examination in patients with RA, while that of the group of clinical experts was the evaluation, discussion, and rating of the proposals. The voluntary acceptance of the group members to the invitation implied implicit consent to participate. The members of the groups were formed between May 2020 and September 2020.
Performing Two Rounds Using the RAND/UCLA Method
Application and Consolidation of the Results
The questionnaire covering three domains was presented to the clinical experts: 1. general items about RA joint inflammation; 2. items about the general joint examination; and 3. items about the examination technique for each of the joints. This process was anonymized (see Appendix 1 and Supplementary Material). For each question, participants were asked to rate each indication on a scale of 1 to 9 points, where 1 corresponds to expected harm exceeding the expected benefits; therefore, it is considered inappropriate or irrelevant. A score of 9 corresponds to the expected benefits that exceed the expected damages; therefore, it would be appropriate or relevant. A score in the middle or 5 points indicates that the damages and benefits are approximately equal or that the evaluator cannot make a judgment for the patient described in the specific scenario; therefore, it is considered uncertain.18
Clarifications
The following clarifications were included in the initial document:
- By examining each joint, the questions are aimed at determining the RA activity, which indicates the presence of edema (swelling) or joint pain.25,28
- Disease activity in the joint is considered any clinical manifestation of pain on examination or edema, which is the same as inflammation of the joint.25,28,29
- In the qualification rounds, the options for diagnosing RA or its differential diagnosis are not considered.
First Round
Each of the clinical experts independently received and answered the 40 initial questions defined by the core group through email. They were asked to provide a rating, observations, and comments on the questionnaire along with the justification for their responses (see Appendix 1 and Supplementary Material).
Second Round
In this face-to-face round, the comments, the anonymized individual scores, and the distribution of the group scores from the first round were presented to the group of clinical experts. During the meeting, the members of the group discussed the results, and disagreements were emphasized. In addition, the need for some indicators or recommendations to be modified, reformulated, divided, or clarified was discussed, resulting in 45 questions from the original 40 questions, and the questions were rated again individually as recommended by the RAND/UCLA manual.
Third Round
The RAND/UCLA method was applied until the second round, but some questions had uncertain results or more than one question was relevant (question 16 remained uncertain without disagreement, questions 29 and 30 about the MCF joints were relevant without disagreement, questions 34 and 36 about the examination of the hips were uncertain and without disagreement), and thus a third round of qualifications outside the RAND/UCLA method was conducted. Through email, participants were asked to vote on the ends of the scale to determine the possibility of including the techniques for assessing the joints that were yet to be included (see Appendix 3 and Supplementary Material).
The rounds of qualification were conducted between January 2021 and October 2021.
Results
Analysis of the Results
An exploratory analysis was performed to identify possible errors or inconsistencies in the information. The variables were described and presented using summary measures. The qualitative variables are presented as percentages. The quantitative variables are presented as the averages or the medians, as appropriate, in addition to the standard deviations or the interquartile ranges, respectively.
Each recommendation or indication was classified into three levels of appropriateness according to the median rating, “appropriate” (6.5–9), “uncertain” (3.5–6.0), or “inappropriate” (1–3.5), as the size of the group is not a multiple of 3 and is even, and based on the most common approach described in the RAND/UCLA manual (which is biased toward having appropriate indications and thus favoring the autonomy of the physician).
In each recommendation, the interpercentile range (IPR) and the interpercentile range adjusted for symmetry (IPRAS) were considered disagreement criteria. The recommendation is classified as disagreement if IPR>IPRAS and no disagreement is indicated if IPR<IPRAS, according to the method described in the RAND/UCLA manual.18
Then, according to the RAND/UCLA membership method, a procedure is classified as “appropriate”, “uncertain” or “inappropriate” for a recommendation based on two criteria: 1) the median of the group scores and 2) a measure of the dispersion of the group scores, which is used as an indicator of the level of agreement with which the ratings were made (IPR - IPRAS).
In the present study, the criteria of the RAND/UCLA manual were used, as described below.
A recommendation (question) is appropriate if the median score is > 6 and no disagreement exists, the recommendation is inappropriate if the median score is <3.5 and no disagreement exists, and all other recommendations with a median score of 3.5–6 (uncertain appropriateness) or with an IPR>IPRAS (the measure of the dispersion of the scores that indicates that the group members do not agree on the recommendation) are classified as uncertain. However, all indications rated as “disagree”, regardless of the median, are classified as uncertain. “Disagreement” basically indicates a lack of consensus, either due to polarization of the group or because the judgments are distributed throughout the entire rating scale from 1 to 9 points (see Table 1).
 |
Table 1 A Statistical Approach to Defining the Appropriateness and Non-Disagreement of the Items on the Joint Examination Questionnaire. |
The data were analyzed with Stata (v15, StataCorp) between January and February 2022.
Presentation of the Results
All 215 rheumatologists affiliated with the CAR were invited to participate. Six rheumatologists responded to the invitation for the core group: one declined to participate, and the other five accepted. Twenty-eight rheumatologists responded to the invitation to participate in the group of clinical experts: two declined to participate, 26 participated in the first round, and 16 members of those who participated in the first round participated in the second round. The 16 rheumatologists who participated in the two rounds were 62% of the total of 26 rheumatologists. The median age of this group of 26 rheumatologists was 45 years (IQR: 42, 65), the youngest was aged 35 years and the oldest was aged 72 years. The group had a mean experience of 15.6 years (standard deviation: 6.3 years) with a minimum experience of 2 years and a maximum of 25 years (see Table 2).
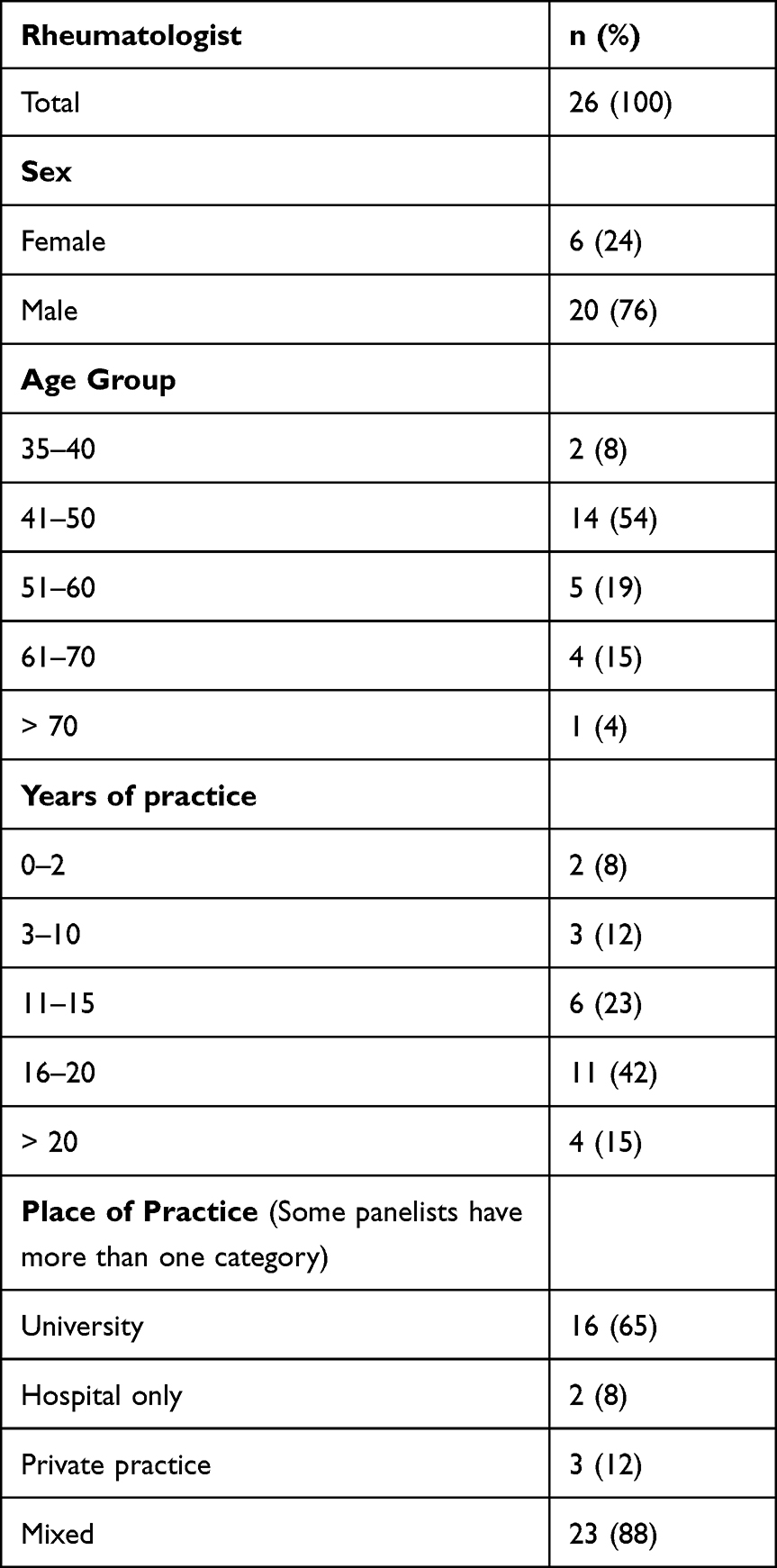 |
Table 2 Demographics of Delphi Participants |
All the rheumatologists came from different centers/hospitals/clinics and from different areas of the country, the majority were men and more than half were between 41 and 50 years of age. Eighty percent of rheumatologists had 11 or more years of experience caring for patients with rheumatoid arthritis.
Results from the First Round of Qualifications
The results according to the appropriateness criteria proposed were classified as follows:
Appropriate items without disagreement for 29 of the 40 questions (2, 4, 5, 7, 8, 12, 13, 14, 15, 17, 18, 19, 20, 21, 22, 23, 24, 25, 27, 28, 29, 30, 32, 35, 36, 37, 38, 39 and 40); uncertain items: appropriate and with disagreement for 4 questions (9, 11, 26 and 33) and 7 items with a median score of 3.5 to 6 (1, 3, 6, 10, 16, 31, and 34), and no inappropriate questions.
(See Appendix 1 and Supplementary Material).
Results from the Second Round of Qualifications
During the meeting of the group in the second round, the concepts listed below were discussed and defined with high appropriateness (median = 9) and without disagreement.
- The group recommends exploring joints for pain or swelling (soft tissue edema of the joint, effusion, or synovial fluctuation) as signs of joint inflammation, since other inflammatory signs are usually not present (flushing or redness, heat or increased temperature) when the joint is inflamed, which may confuse examiners; however, if these signs are present, they should be recorded.25,30 The two distinct characteristics of joint inflammation are swelling and pain when pressing on the joint.9,15 Joint swelling or edema indicates edema of the soft tissues of the joint that can be detected along the joint margins during the examination. Fluctuation or joint effusion (synovial effusion) is a characteristic of a swollen joint. Joint edema may influence the range of motion. Joint swelling does not occur when bone edema or edema in the tissues around the joint is present.25,28
- Joint pain should be considered when it is present under specific circumstances. The pain is present at rest with joint pressure (for example, in the metacarpophalangeal joints), with the passive movement of a joint (for example, in the shoulder, hip, and tarsus), or can be evaluated by asking about spontaneous joint pain (for example, in the hip).25
- Pannus should not be defined during the clinical examination because it is a histological term (rather than clinical) that refers to the proliferation of synovial tissue or invasion into the articular cartilage and involves an active cellular component that generates and perpetuates inflammation and, therefore, the disease.31 These changes have been attributed to a condition called synovitis, which is simply the inflammation of the synovial tissue evaluated clinically.27
- The articular margin should be considered the anatomical reference where the synovial membrane is inserted into the joint, although it is not exactly defined in each joint; it is generally inserted at the interface between the cartilage and the bone.25
- When applying the “rule of thumb”, the minimal pressure necessary to be applied with the thumb (also the index or ring finger) on the joint that triggers pain should be considered.16,23
- Applying the “Joint Compression Test” in the metacarpophalangeal (MCF) or metatarsophalangeal joints helps to define the involvement of one or more of these joints.32–35 Therefore, it may add value to the classification of the activity of these joints in the follow-up of patients with RA.
During the second round of qualifications, the results from the questionnaire were rated as follows:
29 of 45 appropriate items and without disagreement (2, 3, 4, 5, 6, 7, 8, 9, 12, 13, 14, 15, 17, 18, 19, 20, 21, 22, 23, 27, 28, 29, 30, 33, 36, 37, 39, 43 and 45); 16 uncertain items: 2 inappropriate questions with disagreement (10 and 16), and 14 items with a median score of 3.5 to 6 and with disagreement (1, 11, 24, 25, 26, 31, 32, 34, 35, 38, 42, 41, 42 and 44). See Appendix 2 and Supplementary Material.
Results from the Third Round of Qualifications
Items 16, 29, 30, 34, and 36 were rated. The items with inappropriate or disagreeing results were 16, 2, 9 and 34. The items with relevant results and no disagreement were 30 and 36 (See Appendix 3 and Complementary Information).
Statement of Final Recommendations
Of the 45 initial statements on the examination techniques, 28 (62%) were retained. In addition, another 6 statements were included during the face-to-face meeting for a total of 34 final statements (see Table 3).
 |
Table 3 The Final Recommendations with Appropriateness and No Disagreement Results |
Discussion
The main objective of this study was to describe and clarify the techniques for the physical examination of the joints of patients with RA to facilitate their standardization. The objective was achieved by gathering for the first time a group of participants at the national level to evaluate the problem.
The evidence obtained to determine the list of procedures for the joint examination was based on an exhaustive search of the literature. Thus, this study relied on the best possible information with a well-defined research question for a health problem lacking information according to the guidelines of the RAND-UCLA method, with the purpose of improving patient care and health outcomes.
Disagreements were observed among the group members during the process, probably because their perceptions depended to some extent on what they experienced in their clinical practice; however, the consensus allowed the ratings to be concordant. A wide variety of possibilities were included to have representativeness of the clinical practice of the examination of the synovial joints for the evaluation of RA activity.
On the other hand, possible disagreement was expected because some patients treated in clinical practice were not represented or had different characteristics than the clinical circumstances presented. Nevertheless, we were able to unify the concepts.
The elements presented for the examination of the joints in this study can be used by health providers and health insurance payers to improve the quality of patient care, in addition to serving as input for the implementation of protocols and quality reports. This approach will avoid wasting resources. For example, this guideline can be proposed as a quality criterion of the Colombian Fund for High-Cost Diseases (a nongovernmental technical organization created by the Ministry of Finance and the Ministry of Health) that defines some elements of the quality of care for patients with RA, such as the use of activity scales, quality of life and other indicators.
There is a potential application of this consensus document and that is health providers (physicians from different specialties and subspecialties, nurses, physiotherapists, etc.), institutions or universities, become aware of the standardized method to examine the joints and that they may use to improve patient assessment, to support decision making process or as an educational tool.
As a unified method for joint examinations to control RA in adult patients is unavailable, in addition to the disagreement between the examiners, this standardized method seeks to solve this knowledge gap. This document has another potential application in providing physicians with standardized method they can use to improve patient evaluations, to support decision-making, or as an educational tool.
This study has some limitations. First, it is possible that even though definitions were provided both orally and in writing and the experts were provided with the opportunity for discussion and clarification, comprehension might have varied among experts. Second, even though the questions were selected to represent a wide range of situations that could be encountered when examining a patient with RA, the relevant questions might still differ from clinical practice. Third, the participating rheumatologists might have perceptions that are different from other rheumatologists. However, the participating rheumatologists were selected to represent other specialties as much as possible, since they are experts with extensive clinical practice. Fourth, this appropriateness method was applied in Colombia and may not represent rheumatologists and their practices in other regions. However, our findings should be reproducible in other countries since clinical practices are similar worldwide. This study was conducted in compliance with the practices and regulations of the Colombian healthcare system; as such, one of the purposes of the document is its adoption in the country. Fifth, low representativeness may occur because not all the experts participated in all three rounds; nevertheless, most (62%) of the experts did participate in all three rounds, and the RAND/UCLA Appropriateness Method User’s Manual recommends a minimum of 15 participants for the rounds.18 Sixth, appropriateness consensus commonly addresses policy or costs, but these aspects were outside the scope of this study.
Conclusions
The physical joint examination techniques that determine RA activity are heterogeneous and differ markedly in several characteristics. A list of recommendations derived from a RAND/UCLA consensus exercise is proposed as a guide to improve and standardize the method of physical examination of joints. This standardization would improve diagnosis and outcomes for patients with RA and help clinicians provide better treatment.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were following the ethical standards of the Ethical Committee of Medicine Faculty of Pontificia Universidad Javeriana, San Ignacio University Hospital, Simón Bolívar Hospital, Hospital Universitario Nacional de Colombia and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Consent was obtained by the consensus study participants prior to study commencement.
Acknowledgments
Thanks to the rheumatologists who participated in this consensus, especially Dr. Philippe Chalem for his support in the process.
Consensus contributors’ group
Adriana Beltrán, Antonio Iglesias, Aura Domínguez, Carlos Jaime Velásquez, Claudia Mora, Diego jaimes, Edwin Jauregui Elias Forero, Eybar Diaz, Gerardo Ramírez, Gloria Vasquez, Javier Cajas, Juan Manuel Bello, Juan Pablo Restrepo, Lina M. Saldarriaga-Rivera, Mario Diaz, Oscar Jair Felipe, Paul Méndez Patarroyo, Pedro Santos-Moreno, Philippe Chalem, Reynaldo Badillo, Rita Sierra-Merlano, Tomas Caicedo, William Puche, Wilson Bautista-Molano.
Author Contributions
Dr. Yimy F. Medina contributed to the conception of the study. All authors made a significant contribution to the work reported, whether that is in study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Pan American League of Rheumatology Associations (PANLAR) through the PANLAR 2019 Innovation Award and by the Colombian Association of Rheumatology through an unrestricted scholarship conferred by laboratories Abbvie.
Disclosure
Dr Yimy F Medina reports grants from Pan American League of Associations for Rheumatology (PANLAR), during the conduct of the study. The authors declare no other competing interests in this work.
References
1. Gibofsky A. Overview of epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis. Am J Manag Care. 2012;18(13 Suppl):S295–302.
2. Gabriel SE. The epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am. 2001;27(2):269–281. doi:10.1016/S0889-857X(05)70201-5
3. Turesson C, O’Fallon WM, Crowson CS, Gabriel SE, Matteson EL. Extra-articular disease manifestations in rheumatoid arthritis: incidence trends and risk factors over 46 years. Ann Rheum Dis. 2003;62(8):722–727. doi:10.1136/ard.62.8.722
4. Farheen K, Agarwal SK. Assessment of disease activity and treatment outcomes in rheumatoid arthritis. J Manag Care Pharm. 2011;17(9Suppl B):9–13.
5. Sokka T, Pincus T. Quantitative joint assessment in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23(Suppl 39):S58–S62.
6. Smolen JS, Eberl G, Breedveld FC, et al. Validity and reliability of the twenty‐eight‐joint count for the assessment of rheumatoid arthritis activity. Arthritis Rheum. 1995;38(1):38–43. doi:10.1002/art.1780380106
7. Ringold S, Singer N. Measures of disease activity in rheumatoid arthritis: a clinician’s guide. Curr Rheumatol Rev. 2008;4:259–265. doi:10.2174/157339708786263951
8. Balsa A, Villaverde V. Índices de actividad y mejoría en la artritis reumatoide. Rev Esp Reumatol. 2002;1(1):4–8.
9. Scott IC, Scott DL. Joint counts in inflammatory arthritis. Clin Exp Rheumatol. 2014;32(4):S7–12.
10. Sokka T, Pincus T. Joint counts to assess rheumatoid arthritis for clinical research and usual clinical care: advantages and limitations. Rheum Dis Clin North Am. 2009;35(4):713–722. doi:10.1016/j.rdc.2009.10.004
11. Medina YF, Ruíz-Gaviria RE, Buitrago-Lopez A, Villota C. Physical articular examination in the activity of rheumatoid arthritis: a systematic review of the literature. Clin Rheumatol. 2018;37(6):1457–1464. doi:10.1007/s10067-018-4015-4
12. Cheung PP, Ruyssen-Witrand A, Gossec L, et al. Reliability of patient self-evaluation of swollen and tender joints in rheumatoid arthritis: a comparison study with ultrasonography, physician, and nurse assessments. Arthritis Care Res. 2010;62(8):1112–1119. doi:10.1002/acr.20178
13. Walsh CAE, Mullan RH, Minnock PB, Slattery C, FitzGerald O, Bresnihan B. Consistency in assessing the disease activity score-28 in routine clinical practice. Ann Rheum Dis. 2008;67(1):135–136. doi:10.1136/ard.2007.076885
14. Şenocak Ö̈, Ünsal E, Akalin E, Ergör G. Interobserver reliability of articular examination in juvenile idiopathic arthritis. Turk J Pediatr. 2003;45(1):29–32.
15. Grunke M, Antoni CE, Kavanaugh A, et al. Standardization of joint examination technique leads to a significant decrease in variability among different examiners. J Rheumatol. 2010;37(4):860–864. doi:10.3899/jrheum.090195
16. Cheung PP, Dougados M, Andre V, et al. Improving agreement in assessment of synovitis in rheumatoid arthritis. Jt Bone Spine. 2013;80(2):155–159. doi:10.1016/j.jbspin.2012.07.014
17. Stamp L, Harrison A, Frampton C, Corkill M, Frampton C, Michael M. Does a joint count calibration exercise make a difference? Implications for clinical trials and training. J Rheumatol. 2012;39(4):877–878. doi:10.3899/jrheum.111224
18. Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual. Santa Monica, CA: RAND Corporation; 2001.
19. Cheung PP, Dougados M, Andre V, et al. The learning curve of nurses for the assessment of swollen and tender joints in rheumatoid arthritis. Joint Bone Spine. 2014;81(2):154–159. doi:10.1016/j.jbspin.2013.06.006
20. Kane D, Balint PV, Sturrock RD. Ultrasonography is superior to clinical examination in the detection and localization of knee joint effusion in rheumatoid arthritis. J Rheumatol. 2003;30(5):966–971.
21. Kim HA, Kim SH, Seo Y. Ultrasonographic findings of the shoulder in patients with rheumatoid arthritis and comparison with physical examination. J Korean Med Sci. 2007;22(4):660–666. doi:10.3346/jkms.2007.22.4.660
22. Naredo E, Bonilla G, Gamero F, Uson J, Carmona L, Laffon A. Assessment of inflammatory activity in rheumatoid arthritis: a comparative study of clinical evaluation with grey scale and power Doppler ultrasonography. Ann Rheum Dis. 2005;64(3):375–381. doi:10.1136/ard.2004.023929
23. Stone MA, White LM, Gladman DD, et al. Significance of clinical evaluation of the metacarpophalangeal joint in relation to synovial/bone pathology in rheumatoid and psoriatic arthritis detected by magnetic resonance imaging. J Rheumatol. 2009;36(12):2751–2757. doi:10.3899/jrheum.080205
24. Medina-Velásquez YF, Narváez MI, Atuesta J, et al. Variation in the definition of joint examination for the clinimetry of rheumatoid arthritis: results of a survey of a group of Colombian rheumatologists. Rev Colomb Reumatol. 2020;27(3):149–154.
25. Van Riel PLCM, Van Gestel AM, Scott DL. Eular Handbook of Clinical Assessment in Rheumatoid Arthritis.
26. No JOB, By S, Client S, et al. DAS28 quick reference guide for healthcare professionals. Berkshire, England. Report No.: RCUKCOMM00066; 2011. Available from: www.nras.org.uk/DAS.
27. Cajas LJ, Casallas A, Medina YF, Quintana G, Rondón F. Pannus and rheumatoid arthritis: historic and pathophysiological evolution. Rev Colomb Reumatol. 2019;26(2):118–128.
28. Scott DL, Houssien DA. Joint assessment in rheumatoid arthritis. Br J Rheumatol. 1996;35(SUPPL. 2):14–18. doi:10.1093/rheumatology/35.suppl_2.14
29. Scott DL, Antoni C, Choy EH, van Riel PCLM. Joint counts in routine practice. Rheumatology. 2003;42(8):919–923. doi:10.1093/rheumatology/keg235
30. Tarner IH, Härle P, Müller-Ladner U, Gay RE, Gay S. The different stages of synovitis: acute vs chronic, early vs late and non-erosive vs erosive. Best Pract Res Clin Rheumatol. 2005;19(1):19–35. doi:10.1016/j.berh.2004.08.002
31. Ouboussad L, Burska AN, Melville A, Buch MH. Synovial tissue heterogeneity in rheumatoid arthritis and changes with biologic and targeted synthetic therapies to inform stratified therapy. Front Med. 2019;6:1–10. doi:10.3389/fmed.2019.00045
32. Vega-Morales D, Esquivel-Valerio JA, Garza-Elizondo MA. Do rheumatologists know how to squeeze? Evaluations of Gaenslen´s maneuver. Rheumatol Int. 2015;35(12):2037–2040. doi:10.1007/s00296-015-3354-6
33. De Jong PH, Weel AE, De Man YA, et al. To squeeze or not to squeeze, that is the question! Optimizing the disease activity score in 28 joints by adding the squeeze test of metatarsophalangeal joints in early rheumatoid arthritis. Arthritis Rheum. 2012;64(10):3095–3101. doi:10.1002/art.34568
34. Wiesinger T, Smolen JS, Aletaha D, Stamm T. Compression test (Gaenslen’s squeeze test) positivity, joint tenderness, and disease activity in patients with rheumatoid arthritis. Arthritis Care Res. 2013;65(4):653–657. doi:10.1002/acr.21863
35. Santosa D, Hidayat R, Prasetyo M, Nugroho P. Diagnostic values of DAS28 and DAS28-squeeze in evaluating rheumatoid arthritis disease. Indones J Rheumatol. 2018;8(2):10–14. doi:10.37275/ijr.v8i2.54
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.