")
Back to Journals » Journal of Blood Medicine » Volume 13
ABO and Rh Antigen Distribution Among Pregnant Women in South Western Uganda
Authors Mbalibulha Y , Natukunda B, Levix OA , Ononge S, Kalyango JN, Kajja I
Received 2 February 2022
Accepted for publication 14 June 2022
Published 22 June 2022 Volume 2022:13 Pages 351—355
DOI https://doi.org/10.2147/JBM.S360769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Yona Mbalibulha,1 Bernard Natukunda,1 Okwi Andrew Livex,2 Sam Ononge,3 Joan N Kalyango,4 Isaac Kajja5
1Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Pathology, College of Health Science, Makerere University, Kampala, Uganda; 3Department of Obstetrics & Gynaecology, Makerere University College of Health Sciences, Kampala, Uganda; 4Director Clinical and Epidemiology Unit, School of Medicine, College of Health Science, Makerere University, Kampala, Uganda; 5Deputy Principal College of Health Sciences, Makerere University, Kampala, Uganda
Correspondence: Yona Mbalibulha, Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda, Tel +256 773018980, Email [email protected]; [email protected]
Introduction: ABO and Rh are the major blood group systems in Transfusion Medicine, the ABO system based on two red cell antigens (A, B) while the Rh has about 50 antigens of which five are highly clinically significant (D, C, c, E, e). These vary among races and ethnic groups. Blood type phenotype incompatibility between mother and fetus may result in antigen mismatch, triggering alloimmunization, and thus causing hemolytic transfusion reaction (HTR), which results in hemolytic disease of fetus and newborn (HDFN). This study aimed to determine the frequencies of ABO and rhesus blood group antigen in the pregnant women in South Western Uganda.
Methods: A cross-sectional study was carried out on 1369 pregnant women who were recruited and provided consent to participate during their regular antenatal visits between August 2020 and July 2021. Four milliliters (4mL) of EDTA-anti-coagulated blood samples were collected and ABO and Rh-blood grouping including Rh antigen screening was done using the agglutination technology comprised of glass beads and reagent contained in a column of the Ortho Biovue ID Micro Typing System (Ortho Clinical Diagnostics, New Jersey, USA). The Rh antigen phenotypes and frequencies were then determined.
Results: There was percentage distribution of 99.8%, c 99.3%, D 94.3%, C 19.2% and E 15.9%, with Rh cDe/cDe (65.1%) being the most common phenotype followed by cDe/CDe (15%), cDe/cDE (10.8%) and cDE/cDE 0.1% least common. The ABO grouping frequency was obtained as O 49.4%, A 29.5%, B 17.0% and AB 4.1%, with D positivity at 94.3%.
Discussion: Population genetic variations result in varied expressions of red cell antigens that may have clinical complications. Knowledge of the presence of these Rh antigen distributions and phenotype frequencies during pregnancy help in rational management of the pregnancy, alloimmunization and better approach to safe blood transfusion.
Keywords: ABO, Rh antigens, Rh phenotypes, pregnant women, South Western Uganda
Introduction
Blood groups are useful antigenic and genetic markers in the study of immune-haematological complications in a population. The Rh system, having many antigens, is easily classifiable into various phenotypes and genotypes in different populations and can be associated with particular complications.1 The distribution patterns of ABO and Rh blood group systems are complex around the world and their antigenic variations often occur in populations within one small particular area. A significant regional heterogeneity has been reported in the ABO and Rh blood group gene frequencies.2 However, one population may exhibit a high degree of similarity with a distant population that can be attributed to the common history of these populations.3
The frequency distribution of ABO group antigens varies across ethnic populations; for example, Asians have been found to have higher frequency occurrence of blood group B4 than White Europeans and among Africans, but the distribution of ABO blood groups is generally: B, 20%; A, 27%; AB, 4%; and O,:49%.5
The Rh blood group antigen has more than 50 antigens, including D, C, E, c, e, f, Cw, Cx, which have been linked to haemolytic diseases of the fetus and the newborn.6 Clinically, D antigen has high immunogenicity thus classified as D+ (Rh-positive) or D– (Rh-negative). Amongst the White population, d+ frequency occurrence is 85%, while amongst the Black population it is 92%.7,8 Most D– individuals will automatically produce anti-D when they are exposed to D+. The anti-D will then cause haemolysis of the recipient’s red cells, which is the alloimmune haemolytic disease.9 The other Rh antigens like C, c, E, and e are of less immunogenic activity. They only become important in patient care upon the development of the corresponding antibody. D and E antibodies are mainly IgG in nature, although there are some of them that are IgM in nature, and mostly react at 37°C with anti-human globulin.2
Blood group antigen data in a population is important for effective management of related conditions. A 2.2% maternal alloimmunization prevalence has been reported in Uganda, especially in the south west. This study was done with the aim of determining the prevalence and trends of ABO and Rh antigen among the pregnant women attending antenatal clinics in South Western Uganda. Blood group antigen data are important in guiding population genetic studies that are not easily captured by current screening methods during antenatal visits but important in some complications that may arise.10,11
Materials and Methods
This was a cross-sectional study where 1396 pregnant women attending antenatal clinic, not critically ill, were consented by use of informed consent system and recruited during their regular antenatal visits in the months of August 2020 to July 2021. 4mL of EDTA-anti-coagulated blood samples were collected, and ABO and Rh antigen testing was done using the agglutination technology comprised of glass beads and reagent contained in a column of gel to capture agglutinates in a semi-solid medium of the Ortho Biovue ID Micro Typing System (Ortho Clinical Diagnostics, New Jersey, USA).The gels column is about 75% packed gel and 25% liquid in micro-tubes embedded in a plastic card to allow ease of handling, testing, reading, and disposal.
Known positive and negative control samples were included in accordance with the relevant guidelines of quality assurance. ID cards were identified with the individual’s initials and study identification number. The aluminum foil was removed, 10µL red cell suspension of 5% concentration added to the respective micro-tubes and the ID cards centrifuged for 15 minutes. The ID cards were read visually for agglutination or hemolysis.
Results
A total of 1396 pregnant women were recruited and they had a median age of 25 years and a median parity of 2, with median gravidity of 3. Most of them (65%) were in their second trimester (Table 1).
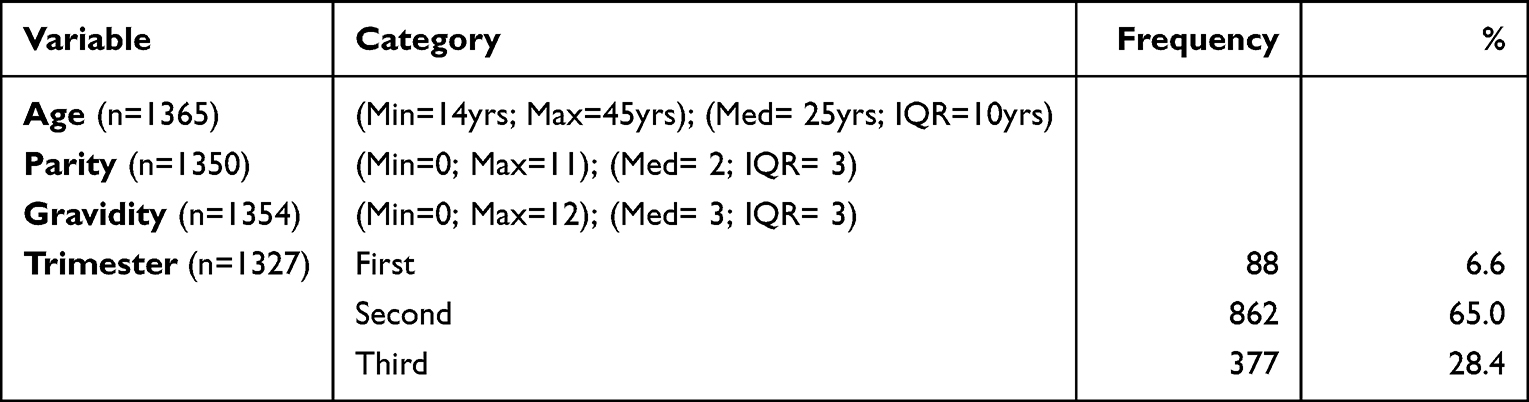 |
Table 1 Demographic Characteristics of the Participants (N=1369) |
The distribution of ABO antigens in the participants showed most pregnant women having blood group O (49.4%), followed by A (29.5%), in the order of O, A, B, AB. The D antigen was observed in 94.3% of the participants (Table 2).
 |
Table 2 The ABO, Rh Antigen Distribution in the Study Participants (N=1369) |
The Rh antigens c and e were common in most participants (99.3% and 99.8%, respectively), while E was least prevalent (15.9%). The Rh profile cDe/cDe (65.1%) was most common, followed by cDe/cDE (10.8%) while cDE/cDE (0.1%) was the least common (Tables 3 and 4). There was no significant difference in the distribution of antigens among the respective blood groups. The most common antigens were highly prevalent in those groups with high appearance (Table 5).
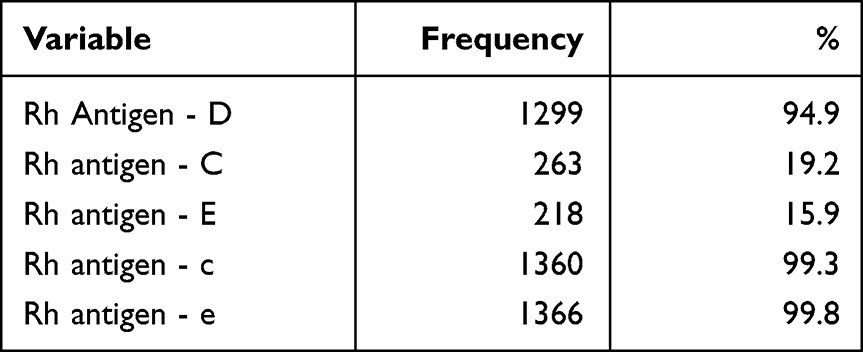 |
Table 3 The Rh Antigen Distribution (N=1369) |
 |
Table 4 The Rh Antigen Phenotype Combination Distribution (N=1369) |
 |
Table 5 Distribution of Rh Antigens by ABO Blood Groups |
Discussion
Variability in genetics of different populations results in varied expression of red cell antigens. The distribution of the ABO blood group in this study was in the order of O > A > B > AB, which is similar to that obtained in other studies. Mbalibulha et al,12 Apecu et al13 and Natukunda et al14 also reported similar findings amongst pregnant women and the general population in this area. This is the same order of blood group distribution in Ogoni ethnic group in Nigeria and North India, as reported by Christian et al6 and Mungwana,15 respectively.
Prevalence of D-positive in this study was 94.3%, which is similar to previous reports by Mangwana (94.5%)15 and Mbalibulha et al (96%)12 in India and Africa, respectively. There are variations in prevalence of D in populations worldwide that range from 83–89% in European and American populations and up to 100% in Far East populations. This variation in the distribution of population groups has significant clinical impact as regards the potential for hemolytic disease of newborn and of hemolytic transfusion reaction as a result of alloimmunization from these antigens.
The highest prevalence among the Rh antigens was shown by e antigen (99.8%) followed by c, D, C, (99.3%, 94.3%, 19.2%, respectively) and E (19.66%) being the lowest. These findings are very similar to studies in Nigeria by Mukhter1 and Erhabo et al8 but different when compared to those studies by Gupta et al,16 Dholakiya et al,17 and Gundrajukuppam et al18 done in India and other Far East populations. This difference is mainly attributed to the difference in ethnic and multi-racial group composition of these populations around the world.
The Rh phenotype distribution observed in this study among the pregnant women shows the order of commonest phenotypes to be cDe/cDe, CDe/cDe and then cDe/cDE. Similar findings have been observed in various studies in Africans.19,20 However, similar results are observed in a few white populations and about 2.9% of the Indian population.1,21,22 These findings are not similar to those obtained by Sarkar,23 Makroo et al24 Prinja et al25 and Basu et al,4 who observed the order of prevalence to be CDe/CDe, CDe/cDe, CDe/cDe, and cDe/cDE. This is possibly due to the ethnic differences in the populations in these areas.
It’s evident that the Rh antigen frequency in this population is unique to this population and would be helpful in serological investigations and transfusion support to pregnant women. Knowledge of varied frequency and phenotypic expression of major clinically relevant antigens in these blood group systems are helpful in more rational approach for pregnancy management, monitoring the initiation of alloimmunization by the antigens and its follow-up. This will help in the decision of who receives RhIG prophylaxis, thus minimizing costs. Methodological studying of these Rh antigens and blood group data in relation to alloimmunization in this population continues to be worthwhile.
Ethical Approval
All the participants were taken through consenting procedures to provide a written informed consent and the study was conducted following the participant protection procedures in conformity with the Helsinki Declaration. Ethical clearance was obtained from the ethical review board of the school of medicine, College of Health Science Makerere University (REC Ref No 2019-114) and the Uganda National Council for Science and Technology (HS508ES).
Funding
This study was funded in part by the Swedish International Development Cooperation Agency (Sida) and Makerere University under Sida contribution No: 51180060.
Disclosure
The authors declare having no competing conflicts of interest relevant to the work presented in this article.
References
1. Mukhtar I, Abdulkadir A. Frequencies of ABO and Rhesus (D) blood group phenotypes among pregnant women attending antenatal clinic at Murtala Muhammad Specialist Hospital, Kano, Nigeria. J Med Trop. 2019;21(1):31–36. doi:10.4103/jomt.jomt_4_19
2. Reid ME, Lomas-Francis C, Olsson ML. RH - Rh Blood Group System, in the Blood Group Antigen FactsBook . Boston: Academic Press; 2012:147–262.
3. Halima AB, Esther Esteban RB, Esteban E, Moral P, Chaabani H. Pedro moral and hassen chaabani, variation of rhesus haplotype frequencies in North Africans and in worldwide population analyses. Int J Hum Genet. 2015;15(1):21–31. doi:10.1080/09723757.2015.11886247
4. Basu D, Datta SS, Montemayor C, et al. ABO, Rhesus, and Kell Antigens, Alleles, and Haplotypes in West Bengal, India. Transfus Med Hemother. 2018;45(1):62–66. doi:10.1159/000475507
5. Rudmann SV. Blood Banking and Transfusion Medicine.
6. Christian SG, Rhesus E, Rhesus D, et al. blood groups distribution among indigenes of ogoni ethnic group of Rivers State, Nigeria. Int J Res Rep Hematol. 2020;5:1–7.
7. Dorothea Evers RAM, Masja de H, Zalpuri S, et al. Red-blood-cell alloimmunisation in relation to antigens’ exposure and their immunogenicity. Lancet Haematol. 2016;3:23–67.
8. Erhabor O, Yakubu A. KSA, Shehu CE. Rh (D) phenotype among pregnant women in Sokoto, North Western Nigeria. Implications on haemolytic disease of the new-born and haemolytic transfusion reaction. Health Sci Res. 2014;1(2):19–24.
9. Koelewijn JM, Slootweg YM, Folman C, et al. Diagnostic value of laboratory monitoring to predict severe hemolytic disease of the fetus and newborn in non-D and non-K-alloimmunized pregnancies. Transfusion. 2020;60(2):391–399. doi:10.1111/trf.15631
10. Willy F. Molecular genetics and clinical applications for RH. Transfus Apher Sci. 2011;44(1):81–91. doi:10.1016/j.transci.2010.12.013
11. Ghesquière L, Garabedian C, Coulon C, et al. Management of red blood cell alloimmunization in pregnancy. J Gynecol Obstet Hum Reprod. 2018;47(5):197–204. doi:10.1016/j.jogoh.2018.02.001
12. Mbalibulha Y, Natukunda B, Mugyenyi G, et al. Occurrence of anti-D alloantibodies among pregnant mothers in Kasese District, Western Uganda. J Blood Med. 2015;6:125–129. doi:10.2147/JBM.S80977
13. Apecu RO, Mulogo EM, Bagenda F, et al. ABO and Rhesus (D) blood group distribution among blood donors in rural south western Uganda: a retrospective study. BMC Res Notes. 2016;9(1):1–4. doi:10.1186/s13104-016-2299-5
14. Natukunda B, Mugyenyi G, Brand A, et al. Maternal red blood cell alloimmunization in South Western Uganda. Transfus Med. 2011;21(4):262–266. doi:10.1111/j.1365-3148.2011.01073.x
15. Mangwana S, Simon N, Sangwan L. RH phenotype, ABO and kell antigens, alleles and haplotypes frequencies in North Indian blood donor population. Glob J Transfus Med. 2021;6(1):81.
16. Gupta GK, Balbuena-Merle R, Hendrickson JE, et al. Immunohematologic aspects of alloimmunization and alloantibody detection: a focus on pregnancy and hemolytic disease of the fetus and newborn. Transfus Apher Sci. 2020;59(5):102946. doi:10.1016/j.transci.2020.102946
17. Dholakiya SK, Bharadva S, Vachhani J, et al. Red cell alloimmunization among antenatal women attending tertiary care center in Jamnagar, Gujarat, India. Asian J Transfus Sci. 2021;15(1):52. doi:10.4103/ajts.AJTS_72_17
18. Gundrajukuppam DK, Vijaya SB, Rajendran A, Sarella JD. Prevalence of principal rh blood group antigens in blood donors at the blood bank of a tertiary care hospital in Southern India. J Clin Diagn Res. 2016;10(5):Ec07–Ec10.
19. Al-Dughaishi T, Al Harrasi Y, Al-Duhli M, et al. Red cell alloimmunization to Rhesus antigen among pregnant women attending a tertiary care hospital in Oman. Oman Med J. 2016;31(1):77. doi:10.5001/omj.2016.15
20. Christian SG, Eze EM, Badom BM, et al. Frequency occurrence and percentage distribution of Rh C, Rh c, Rh E and Rh e blood group amongst pregnant women attending antenatal clinic in Port Harcourt, Nigeria. Eur J Med Health Sci. 2021;3(3):50–54. doi:10.24018/ejmed.2021.3.3.808
21. Jourdren G, Berveiller P, Rousseau A. Practices for RhD alloimmunization prevention: a vignette-based survey of midwives. J Matern Fetal Neonatal Med. 2021;25:1–11. doi:10.1080/14767058.2021.1957822
22. Moise K, Management of pregnancy complicated by Rhesus (D) alloimmunization: 2016:3.
23. Sarkar RS, Philip J, Mallhi RS, et al. Proportion of Rh phenotypes in voluntary blood donors. Med J Armed Forces India. 2013;69(4):330–334. doi:10.1016/j.mjafi.2013.05.004
24. Makroo RN, Bhatia A, Gupta R, et al. Prevalence of Rh, Duffy, Kell, Kidd & MNSs blood group antigens in the Indian blood donor population. Indian J Med Res. 2013;137(3):521–526.
25. Prinja N, Narain R. ABO, Rh, and kell blood group antigen frequencies in blood donors at the tertiary care hospital of Northwestern India. Asian J Transfus Sci. 2020;14(2):179–184. doi:10.4103/ajts.AJTS_34_19
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.