")
Back to Journals » Journal of Blood Medicine » Volume 14
Acute Basophilic Leukemia Arising from Chronic Myeloid Leukemia with +8, I(17q)(q10) and der(22)t(9;22) After Imatinib Therapy
Received 16 March 2023
Accepted for publication 11 August 2023
Published 6 September 2023 Volume 2023:14 Pages 513—517
DOI https://doi.org/10.2147/JBM.S412837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Peng Shan,1,2 Hang Dong,1,2 Shilan Li3
1Department of Laboratory, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230036, People’s Republic of China; 2Core Unit of National Clinical Research Center for Laboratory Medicine, Hefei, Anhui, 230036, People’s Republic of China; 3Department of Pathology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230036, People’s Republic of China
Correspondence: Shilan Li, Department of Pathology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230036, People’s Republic of China, Tel +86-0551-62284147, Email [email protected]
Abstract: Acute basophilic leukemia (ABL) arising from chronic myeloid leukemia (CML) with abundant mast cells (MCs), coexisting with a complex karyotype is rare. Here, we report an 81-year-old man admitted to our hospital with a history of ABL. He was diagnosed with CML in the chronic phase in January 2018, and Imatinib was used at a daily dose of 400mg. Then, transformation to ABL with abundant MCs in the bone marrow and complex karyotypes including 48,XY, trisomy 8 (+8), isochromosome 17(q10) [i(17)(q10)], and derivative chromosome 22 t(9;22) [der(22)t(9;22)] were discovered simultaneously in January 2022. In conclusion, the increased number of MCs in our case is a reminder that they might play an important role in the prognosis of CML and trigger the development of complex karyotypes. Moreover, this is the first case report of ABL arising from CML with abundant MCs, coexisting with 48,XY, +8, i(17)(q10), and der(22)t(9;22), during Imatinib treatment. Further studies are needed to better characterize this rare condition.
Keywords: CML, TKIs, MCs, ABL, complex karyotype
Introduction
Acute basophilic leukemia (ABL) is an uncommon form of acute myelogenous leukemia (AML), characterized by blasts with basophilic granules. Different from mast cells (MCs), basophils show toluidine blue positivity on cytochemical staining, an immunophenotype on flow cytometry with the expression of myeloid markers, such as CD13, CD33, CD34, HLA-DR and a diverse group of cytogenetic abnormalities.
Acute basophilic leukemia arising from chronic myeloid leukemia (CML) is uncommon, and the simultaneous development of complex karyotypes in the same patient, including 48,XY, +8, i(17)(q10), and der(22)t(9;22), has not been reported previously. Here, we report an 81-year-old man diagnosed with acute basophilic leukemia arising from CML. The patient was diagnosed with CML in the chronic phase in January 2018 and treated with Imatinib at a daily dose of 400mg. Under this treatment, the disease progressed four years later in January 2022. Toluidine blue positivity on cytochemical staining demonstrated there were 51% basophils in peripheral smear, of which 22% resembled basophilic precursors. Acute basophilic leukemia was suspected. Then the patient underwent bone marrow biopsy. Immunophenotype on flow cytometry and immunohistochemistry demonstrated 30% MCs in the marrow biopsy. Chromosome analysis revealed an abnormal karyotype, including 48,XY, +8, i(17)(q10), and der(22) t(9; 22). No ABL-associated fusion genes, elevated serum tryptase levels, or KIT D816V were found. As a result, a diagnose of acute basophilic leukemia arising from CML was made.
Case Presentation
An 81-year-old man with a history of chronic myeloid leukemia (CML) was readmitted to our hospital with leukocytosis, serious anemia and thrombocytopenia. In January 2018, bone marrow fluorescence in situ hybridization (FISH) analysis revealed the BCR::ABL1 fusion gene and cytogenetic analysis revealed t(9;22). An initial diagnosis of CML in the chronic phase was made. He was treated with Imatinib at a daily dose of 400 mg. The patient was readmitted to our hospital because of a rising white blood cell (WBC) count and increased number of circulating blasts in February 2022. Blood work-up showed marked leukocytosis (66.48 × 109/L), anemia (7.9 g/dl), and thrombocytopenia (94 × 109/L), and blast crisis was suspected. A peripheral blood film showed that 51% of cells had the characteristics of basophils, of which 22% resembled to basophilic precursors, with a medium-sized, round nucleus and moderately basophilic cytoplasm containing a variable number of coarse basophilic granules (Figure 1a), which were positive for toluidine blue (Figure 1b) and negative for peroxidase (Figure 1c).
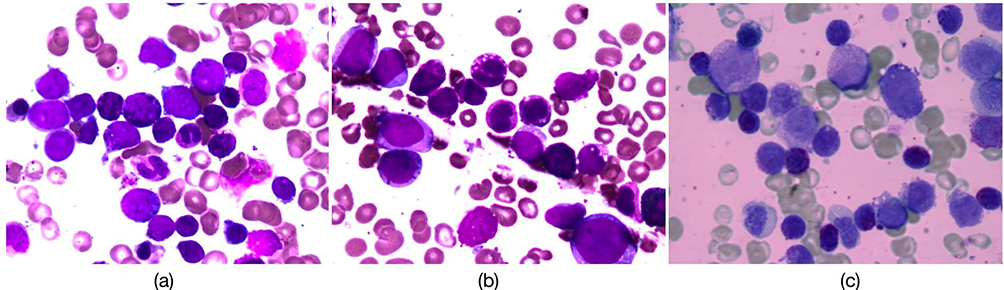 |
Figure 1 Morphology and cytochemistry of peripheral and bone marrow smear of tumor cells. Basophilic precursors with medium-size, round nucleus and moderately basophilic cytoplasm containing a variable number of coarse basophilic granules (a). Marrow smear showed these atypical basophils were positive for toluidine blue (b) and negative for peroxidase (c). |
Bone marrow biopsy revealed a large proportion (more than 30%) of unexpected small round cells with sparse granules (Figure 2a). The most challenging thing was the classification of these cells. Immunohistochemistry (IHC) revealed that 10% were CD34-positive myeloblasts (Figure 2b), and more than 30% of the cells were most likely a mastocytic differentiation, because they showed strong expression of CD117 (Figure 2c) and were negative for CD25. Immunophenotyping up on flow cytometric study in bone marrow aspiration demonstrated that the neoplastic cells were subsequently revealed to exhibit a bi-differentiation. In which group one accounting for 13.8%, expressing CD13 and CD33 (Figure 3a) resemble to basophilic precursors; and group two accounting for 28.8%, strongly expressing CD117 and CD25 (Figure 3b), demonstrating they were MCs lineage.
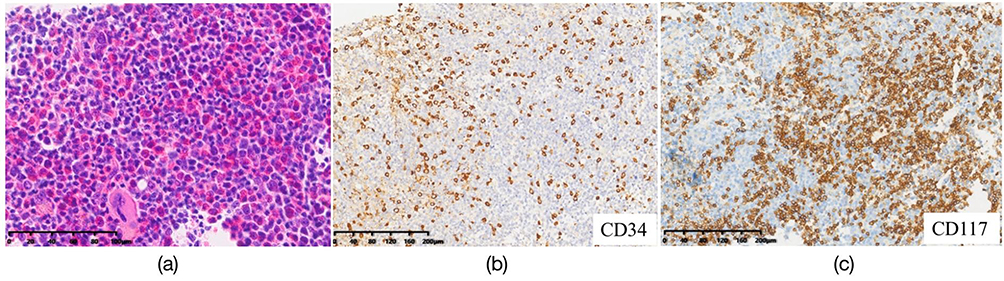 |
Figure 2 Morphology and immunohistochemistry of bone marrow biopsy. Biopsy showed a hypercellularity BM. The tumor cells shared similar histology morphology characteristics with the myeloid blast cells. And a large proportion of unexpected small round cells with sparse basophilic granules was discovered (a). Myeloblast showed positive for CD34 (b). Immunostaining revealed there were more than 30% of cells strongly positive for CD117 (c). |
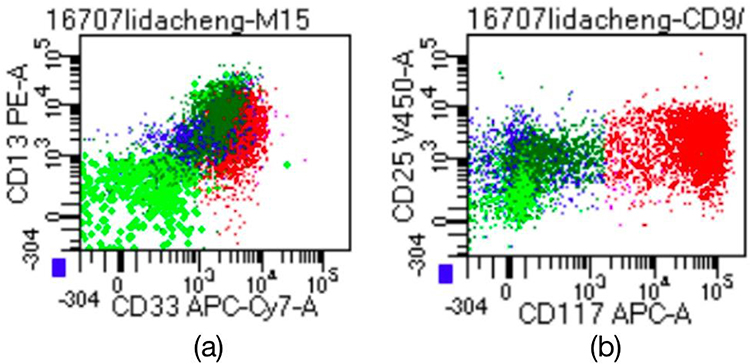 |
Figure 3 Immunophenotyping up on flow cytometric study in bone marrow aspiration demonstrated that the neoplastic cells were subsequently revealed to exhibit a bi-differentiation. Basophilic precursors accounting for 13.8%, expressing CD13 and CD33 (a); and mast cells accounting for 28.8%, strongly expressing CD117 and CD25 (b). |
However, lymphadenopathy, cutaneous involvement, signs of hyperhistaminemia, or KIT D816V mutation were not detected.
FISH analysis confirmed BCR::ABL fusion, and cytogenetic analysis revealed complex karyotypes: 48,XY, +8, i(17)(q10), and der(22)t(9;22). All these changes were discovered after the transformation of CML to ABL. It is unknown if these abnormalities arose secondary to the Imatinib therapy, or if they accelerated the blast transformation of CML presenting with basophilic differentiation. Further studies are needed to better characterize this rare condition.
As a result, a diagnosis of acute basophilic leukemia secondary to CML in blast crisis with a complex karyotype coexisting with abundant MCs was made. After this diagnosis, the patient was treated with Dasatinib at a daily dose of 200mg. At the time of writing, the patient was well, and his WBC count had decreased to 5.16×109/L.
Discussion
Acute basophilic leukemia (ABL) is a rare form of acute leukemia, first described by Joachim in 1906.1 It was recognized as a distinct entity by the most recent World Health Organization classification of myeloid malignancies. However, to date, no generally accepted criteria have been agreed for the diagnosis and classification of ABL. Acute basophilic leukemia cases secondary to chronic myeloid leukemia (CML) are rare and often represent blast transformation.2 In some patients, basophilia may be excessive and may even produce a clinical picture resembling (secondary) to basophilic leukemia.
Morphologically, basophilic blasts are typically characterized by a high nucleus-to-cytoplasm ratio, round to indented nuclei with an open chromatin pattern, and abundant basophilic granules. Cytochemical staining shows a unique pattern of metachromatic positivity with toluidine blue or Giemsa, but are negative with myeloperoxidase. Different from basophilic blasts, basophils expressing myeloid markers, including CD13, CD33, CD34, and HLA-DR.
Mast cells (MCs) exert immunosuppression and stimulate immune tolerance and tumor promotion. Xu et al found that the number of MCs in CML patients increased significantly compared with the healthy group. The increasing number of MCs in the bone marrow along with the development of CML may herald the transformation of CML into AML. The number of MCs may have an important inverse relationship with the prognosis of CML. They might also act as a new therapeutic target for the treatment of tumors.3 In our present case, the bone marrow biopsy showed more than 30% MCs, which is an increase in the number of MCs compared with the patient’s bone marrow biopsy from 2018. This suggests that MCs might participate in tumor development.
In our present case, the most challenging thing was differentiating basophils and MCs because of their similar morphological, phenotypic and functional characteristics. Basophils and tissue MCs represent two distinct lineages within the hematopoietic cell family. In contrast to MCs, basophils usually develop and complete their differentiation in the bone marrow (BM) and are released into the peripheral blood (PB) after maturation. Toluidine blue activity can be observed in basophils, while the same reaction is negative in MCs.4 Mature basophils are positive for CD25 and negative for CD117. Diffuse and confluent CD117 positivity and CD25 negativity in our case demonstrated that the cells were mature MCs.
Ninety percent of patients have a typical t(9;22), resulted in the formation of the fusion gene BCR::ABL1; while 5% have variant translocations, which can be simple (involving chromosome 9 and a chromosome other than chromosome 22), or complex (involving one or more chromosomes in addition to chromosomes 9 and 22). Additional chromosomal abnormalities are reported in 5% 10% of cases, including double Ph, trisomy 8, isometric 8, isochromosome 17, and isometrics of chromosomes 19 and 20.5,6 Our case was first diagnosed with CML in the chronic phase in January 2018 and was treated with Imatinib at a daily dose of 400mg. He visited our hospital in February 2022, when bone marrow biopsy demonstrated progression to ABL, and chromosome genetic analysis revealed a complex karyotype 48,XY, +8, i(17)(q10), and der(22)t(9; 22). ABL- associated fusion genes, elevated serum tryptase levels and KIT D816V mutation were not found.
Because of the patient’s poor clinical status and drug resistance, he was treated with Dasatinib, and the percentage of BCR::ABL1 positive cells decreased to 2.16% after eight months of treatment.
The therapeutic scheme currently used involves tyrosine kinase inhibitors (TKIs) associated with high-intensity systemic chemotherapy. Imatinib has long been the first-choice drug for CML therapy because of durable responses and prolonged patient survival. Unfortunately, clinical complications can occur during treatment, in particular the onset of resistance due to point mutation of BCR::ABL1.
Dasatinib is used to treat Imatinib resistant patients with BCR::ABL1 point mutations, except in the presence of T315I mutation.7 We suspect these changes might result from somatic mutation of blast cells during TKI therapy. It is unknown whether the complex karyotype and the presentation of basophilic precursors in this CML blast crisis were related to the Imatinib therapy, or if these changes accelerated this patient into blast crisis. There are no guidelines on treatment in this scenario because of the rarity of this presentation, and it is assumed that patients with this clinical presentation have a high rate of mortality after diagnosis. Further study is therefore needed to better characterize this rare condition, investigate prognostic factors, and define optimal management.
Conclusion
The treatment regimen for acute basophilic leukemia secondary to CML still present a great challenge for clinicians, especially when accompanied by complex karyotypes. The increasing number of MCs in our case is a reminder that they might play an important role in the prognosis of CML. Further studies are needed to better characterize this rare condition.
Data Sharing Statement
All authors have declared the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study complies with all relevant ethical regulations and the study protocol was approved by the Biomedical Ethics Committee of USTC (2022-RE-335). The specimens of paraffin sections used in this study were obtained in previous clinical diagnosis and treatment, which will not cause physical and mental suffering to the patient. Written informed consent has been provided by the patient to have the case details, including photographs, case history and details published. The privacy and personal information of the patient will be protected, and the specimens that subjects have explicitly refused to use will not be used.
Acknowledgments
We are grateful to Dr Hang Dong for the diagnosis of peripheral blood and bone marrow smear. We also thank the department of Flow Cytometry and the central laboratory of the First Affiliated Hospital of USTC for their work in the diagnosis of this case.
Author Contributions
We thank Peng Shan and Shilan Li for made a significant contribution to the work reported. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. All the authors declare that there is no conflict of interest.
References
1. Ber JGU. Mastzellenleukamien. Dtsch Arch Klin Med. 1906;87:437.
2. Gupta R, Jain P, Anand M. Acute basophilic leukemia: case report. Am J Hematol. 2004;76(2):134–138. doi:10.1002/ajh.10446
3. Xu P, Zhang C, Wang Y, et al. Increased number of mast cells in the bone marrow of chronic myeloid leukemia may herald the pending myeloid transformation—the mast cell is an indicator of myeloid transformation. Transl Cancer Res. 2019;8(5):2121–2129. doi:10.21037/tcr.2019.09.29
4. Peterson LC, Parkin JL, Arthur DC, Brunning RD. Acute basophilic leukemia. A clinical, morphologic, and cytogenetic study of eight cases. Am J Clin Pathol. 1991;96(2):160–170. doi:10.1093/ajcp/96.2.160
5. Rojas-Atencio A, Urdaneta K, Soto-Quintana M, Alvarez Nava F, Canizales J, Solis E. Trisomy 19 and t(9;22) in a patient with acute basophilic leukemia. Case Rep Pathol. 2011;2011:269491. doi:10.1155/2011/269491
6. Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2022 update on diagnosis, therapy, and monitoring. Am J Hematol. 2022;97(9):1236–1256. doi:10.1002/ajh.26642
7. Di Maria S, Picarazzi F, Mori M, et al. Novel pyrazolo[3,4-d]pyrimidines as dual Src/Bcr-Abl kinase inhibitors: synthesis and biological evaluation for chronic myeloid leukemia treatment. Bioorg Chem. 2022;128:106071. doi:10.1016/j.bioorg.2022.106071
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.