")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Air Pollution Alleviation During COVID-19 Pandemic is Associated with Renal Function Decline in Stage 5 CKD Patients
Authors Wu CY , Hsu CT, Chung MC, Chen CH, Wu MJ
Received 6 May 2022
Accepted for publication 10 August 2022
Published 31 August 2022 Volume 2022:15 Pages 1901—1908
DOI https://doi.org/10.2147/JMDH.S371815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chun-Yi Wu,1,2 Chia-Tien Hsu,1 Mu-Chi Chung,1,3 Cheng-Hsu Chen,1,4– 6 Ming-Ju Wu1,3– 5,7– 9
1Division of Nephrology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Department of Nursing, Asia University, Taichung, Taiwan; 3PhD Program in Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 4Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan; 5School of Medicine, China Medical University, Taichung, Taiwan; 6Department of Life Science, Tunghai University, Taichung, Taiwan; 7School of Medicine, Chung Shan Medical University, Taichung, Taiwan; 8Graduate Institute of Clinical Medical Sciences, School of Medicine, China Medical University, Taichung, Taiwan; 9RongHsing Research Center for Translational Medicine, National Chung Hsing University, Taichung, Taiwan
Correspondence: Ming-Ju Wu, Division of Nephrology, Department of Internal Medicine, Taichung Veterans General Hospital, No. 1650, Sec. 4, Taiwan Blvd., Xitun Dist, Taichung City, 407219, Taiwan, Email [email protected]
Introduction: Air pollution is a novel environmental risk factor for chronic kidney disease (CKD). Air quality improved during COVID-19 lockdowns; however, the effects of these lockdowns on PM2.5 concentrations and renal function remain unclear.
Methods: We conducted a retrospective cohort study to compare air pollution and estimated glomerular filtration rate (eGFR) decline in patients with stage 5 CKD between a year-long period of lockdown (2020; n = 724) and a similar period before lockdown (2019, n = 758).
Results: Compared with 2019, a 17.5% reduction in the average PM2.5 concentration (from 17.36% to 14.32%; P < 0.001) and a 45.1% reduction (from 20.56% to 11.25%; P < 0.001) in cumulative days with PM2.5 concentration > 35 μg/m3 were noted in 2020. Moreover, a 93% reduction in PM2.5 air quality index > 150 per station-day (from 0.43% to 0.03%) was observed in 2020. From 2019 to 2020, the yearly incidence of eGFR decline ≥ 5 mL/min/1.73 m2 decreased by 33.7% (24.6% vs 16.3%; P < 0.001). Similarly, the proportion of patients who started undergoing regular dialysis also decreased by 32.7% in 2020 (from 20.8% to 14.0%; P = 0.001).
Conclusion: Our findings suggest that fewer events of renal function decline during the COVID-19 pandemic may be associated with a decline in PM2.5 concentrations, supporting the global strategy of reducing air pollution to prevent CKD progression.
Keywords: COVID-19 pandemic, chronic kidney disease, air pollution, PM2.5, air quality index
Introduction
According to recently published World Health Organization (WHO) data, 99% of the global population breathes air that exceeds WHO air quality limits, thereby causing several diseases.1 Particulate matter (PM), one of the air pollutants, is a complex mixture of solid and liquid particles that are contributed by various sources, including industrial manufacturing processes, fossil fuel burning, road dust, and other natural sources.2–4 Breathing fine PM with a diameter <2.5 μm (PM2.5) causes detrimental health effects, because these particles reach the distal alveoli and trigger a systemic inflammatory response and oxidative stress. Moreover, they enter the systemic circulation and damage distal organs,5,6 such as the heart, blood vessels, and kidneys.6–17
Chronic kidney disease (CKD) is recognized as a global public health issue because of the increasing number of cases.18 The overall CKD mortality increased by 31.7% over the last 10 years, making it one of the fastest rising causes of death, alongside diabetes and dementia.19 Air pollution is the second leading cause of death from noncommunicable diseases (NCDs) after tobacco smoking.18 The third United Nations high-level meeting on NCDs in 2018 recognized indoor and outdoor air pollution as a risk factor for NCDs.20 Several traditional metabolic risk factors and modifiable behaviors have been identified for CKD. Moreover, several studies have reported the association between CKD and air pollution, specifically PM2.5 pollution. Therefore, air pollution is considered a novel environmental risk factor for the development and progression of CKD.15–17
COVID-19, which emerged in early 2020, continues to threaten the lives of people worldwide. Pandemic lockdowns are known to improve air quality.21–24 Studies based in a Chinese megacity have reported an association between the improved air quality during COVID-19 lockdown and reduced mortality.24,25 Similar to other countries, Taiwan has made considerable efforts to combat COVID-19. The food, hospitality, transportation, and manufacturing industries were hit hard by the pandemic. In 2020, a marked reduction in air pollution was also reported in Taiwan.25 Chiu et al noted the high prevalence and incidence of CKD in Taiwan26 and conducted a study to report an association between high PM2.5 concentrations and an increased risk of acute lung edema in patients with stage 5 CKD who were not undergoing dialysis.27 Few studies have focused on the effect of reduced PM2.5 concentrations on the renal function of patients with CKD. Therefore, we evaluated the association between air pollutant concentrations and renal function in patients with stage 5 CKD during the 2-year COVID-19 period.
Materials and Methods
Study Participants
This retrospective cohort study included patients with pre-end-stage renal disease (pre-ESRD) presenting to the Taichung Veterans General Hospital. In Taiwan, the nationwide pre-ESRD pay-for-performance program was implemented in 2006 to improve the care quality of patients with CKD stages 3B, 4, and 5. The program is coordinated by the Taiwan Society of Nephrology and Taiwan Health Promotion Administration, Ministry of Health and Welfare.28,29 Nephrologists, along with a multidisciplinary kidney care team consisting of renal nurses, renal pharmacists, and dietitians, play the central role in the pre-ESRD program. Enrollment in the program can only be initiated by the nephrologist. Follow-up and education on a regular 3-month basis are mandated for case payment.30,31 According to the 2020 annual report, 63.9% of all patients undergoing dialysis were enrolled in the pe-ESRD program before dialysis initiation.32
We included patients with stage 5 CKD who were not undergoing dialysis presenting in 2019 and 2020. Patients aged <20 years; without complete residential address; who were enrolled in the pre-ESRD program before January 1, 2019, and after December 31, 2020; not residing in Taichung City, Changhua County, or Nantou County; and without eGFR records for both baseline and advanced CKD stages were excluded. To protect patient privacy, all personal identification data were encrypted and anonymized before the database was analyzed. The study protocol was approved by the Research Ethics Committee of Taichung Veterans General Hospital, Taichung, Taiwan (CE19222B-1), and the protocol complies with the Declaration of Helsinki principles. The institutional review board waived the requirement to obtain informed consent due to the minimal risk of harm to participants. Data was acquired from the Taichung Veterans General Hospital Research Database with the permission of the hospital’s Clinical Informatics Research and Development Center. We first collected clinical information from electronic medical records and laboratory reports, including data on the International Classification of Diseases diagnosis code, body mass index, blood urea nitrogen, serum creatinine, estimated glomerular filtration rate (eGFR), hemoglobin, albumin, sodium, potassium, phosphate, uric acid, cholesterol, low-density lipoprotein (LDL), triglyceride, fasting sugar, hemoglobin A1c (HbA1c), systolic blood pressure, and diastolic blood pressure. Patients were stratified into two groups on the basis of their presentation year, that is, 2019 or 2020.
eGFR Outcomes of Patients with Pre-ESRD
The Modification of Diet in Renal Disease‐4 equation was used to calculate eGFR levels. Data on eGFR decline occurring during the observation period for patients with pre-ESRD who were not receiving dialysis were obtained. According to the Patient Care and Health Education Plan criteria of the Taiwan Society of Nephrology, an eGFR decrease of ≥5 mL/min/1.73 m2 in 1 year is defined as an event of eGFR decline. The percentages of eGFR decline in the observation period of 6 months and 12 months were calculated for each of the two groups. Data on patients who were initiated to receive regular dialysis were also collected.
Calculation of PM2.5 Concentrations and Air Quality Index
Air pollution data were extracted from official records of the Taiwan Air Quality Monitoring Network (https://airtw.epa.gov.tw/CHT/Themes/LinkOut.aspx) and the Air Quality Report of Environmental Protection Bureau of Taichung City Government (https://www.epb.taichung.gov.tw/1714222/post). Data are recorded at hourly intervals for the pollutants, NO2, NO, PM2.5, PM10, CO, SO2, and O3. We selected data collected at remote stations, as they were more accurate and were relatively free of local pollutants and changes due to COVID-19-related restrictions.
Statistical Analysis
Data are presented as percentage for categorical variables and mean ± standard deviation for continuous variables. A chi-squared test was used for comparing categorical variables, and continuous variables were compared using the analysis of variance and post hoc Bonferroni test. Statistical analyses were performed using SAS software 9.4 (SAS Institute, Cary, NC, USA). The significance level for all statistical tests was set at a two-sided P value of <0.05.
Results
A total of 1482 patients meeting the inclusion criteria were enrolled and classified into two year-based groups: the 2019 group (n = 758) and 2020 group (n = 724). In the 2019 and 2020 groups, 50.4% and 51.2% of participants, respectively, were men. At baseline, participants’ overall mean age was 69.4 ± 14.3 years, and the mean eGFR was 10.4 ± 3.8 mL/min/1.73 m2. Participants’ demographic characteristics, biochemistry data, and underlying diseases are listed in Table 1. No statistically significant difference in these aspects was observed between the two groups.
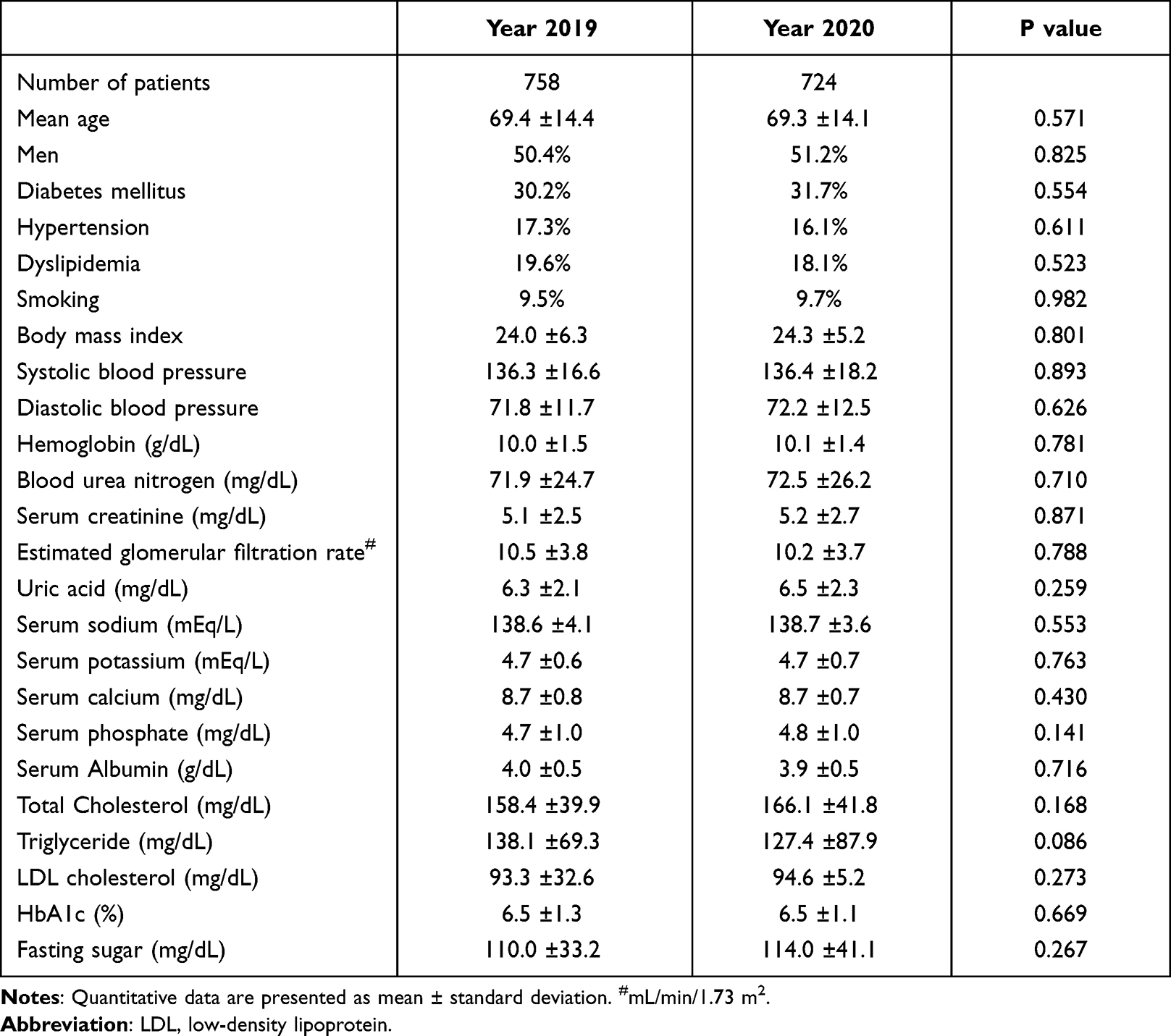 |
Table 1 Demographic and Health Characteristics of Patients with Stage 5 Chronic Kidney Disease Presenting in 2019 and COVID-19 Pandemic Year 2020 |
The average annual concentration of PM2.5 was 17.36 ± 1.63 μg/m3 in 2019 and 14.32 ± 1.34 μg/m3 in 2020, revealing a 17.5% decrease in PM2.5 concentration in 2020 (P < 0.001, Figure 1A). Cumulative days with PM2.5 concentration >35 μg/m3 were 20.56 ± 7.07 days (range 11–32 days) in 2019 compared with 11.25 ± 3.96 days (range 4–17 days) in 2020, corresponding to a 45.1% reduction in 2020 (P < 0.001, Figure 1B). Moreover, the percentage of PM2.5 air quality index >150 was 0.43% per station-day in 2019 compared with only 0.03% per station-day in 2020, corresponding to a 93% reduction in 2020 (Figure 1C).
 |
Figure 1 Comparison of PM2.5 concentrations in 2019 and 2020 in Taichung area. The average annual concentration of PM2.5 (A), Cumulative days with PM2.5 concentration >35 μg/m3 (B), the percentages of PM2.5 air quality index >150 per station-day (C) in 2019 and 2020. |
In the study period (2019 and 2020), 259 (17.5%) patients started undergoing regular dialysis. Sixty-seven (4.5%) patients exhibited an eGFR decline ≥ 5 mL/min/1.73 m2 in 6 months, whereas 305 (20.6%) patients exhibited an eGFR decline ≥ 5 mL/min/1.73 m2 in 12 months. Table 2 lists the outcomes of patients with stage 5 CKD in 2019 and 2020. Regarding renal function, the mean eGFR decline was 0.41 ± 0.14 mL/min/1.73 m2 in the 2019 group and 0.30 ± 0.11 mL/min/1.73 m2 in the 2020 group (P = 0.043). Given that the event of eGFR decline is defined as an eGFR decrease of ≥5 mL/min/1.73 m2 in 1 year, the event of eGFR decline in 6 months was 6.1% in the 2019 group versus 2.9% in the 2020 group (P = 0.002). Moreover, the event of eGFR decline in 12 months was 24.6% in the 2019 group versus 16.3% in the 2020 group (P < 0.001). The proportion of patients who started undergoing regular dialysis in 1 year was 20.8% in the 2019 group versus 14.0% in the 2020 group (P = 0.001). Figure 2 compares the percentage of patients with eGFR decline ≥ 5 mL/min/1.73 m2 between the two groups (P = 0.002).
 |
Table 2 Outcomes of Patients with Stage 5 Chronic Kidney Disease Presenting in 2019 and COVID-19 Pandemic Year 2020 |
 |
Figure 2 Comparison of patients with eGFR decline ≥5 mL/min/1.73 m2 in 2019 and 2020. |
Discussion
Our principal finding is that the events of eGFR decline in patients with stage 5 CKD who were not undergoing dialysis were significantly fewer in the COVID-19 pandemic year 2020 than in 2019. The PM2.5 concentration was also lower in 2020 than in 2019. However, we are yet to provide evidence to support the causal relationship between declines in PM2.5 concentration and such renal events. The etiology of renal function decline is multifactorial; high PM2.5 concentration may be a risk factor for eGFR decline as it induces systemic inflammatory responses. Severe air pollution (air quality index > 150) results in prominent unhealthy consequences. Several experimental and clinical findings have indicated such a biologic plausibility, supporting the hypothesis that environmental exposure to air pollutants, especially high concentrations of PM2.5, is associated with an increased risk of systemic diseases affecting several organs, including the kidneys.2,3,5–9
Several studies have reported the association between air pollution or PM2.5 and CKD. In the United States, long-term exposure to high concentrations of PM2.5 in veterans was associated with a higher risk of incident CKD that progressed to ESRD.12 Among older men, year-long exposure to high concentrations of PM2.5 was associated with a lower eGFR.13 Similar findings have been reported in the Taiwanese population. Exposure to particulate and acidic gas air pollution is associated with a higher risk of CKD and ESRD.33 A higher risk of acute lung edema in Taiwanese patients with stage 5 CKD who were not undergoing dialysis was also associated with high concentrations of PM2.5.27 These findings are consistent with the results of our study on patients with stage 5 CKD. The effect of the COVID-19 pandemic was higher in 2020 than in 2019, and the lower concentrations of PM2.5 and better outdoor air quality are likely to cause fewer events of rapid eGFR decline in patients with advanced CKD. Lockdowns during the COVID-19 pandemic dramatically decreased the social and economic activity worldwide.34 Several studies have reported a significant reduction in air pollution concentrations during lockdowns in most polluted cities, such as New York, Milan, Bangkok, Delhi, and Wuhan;35–37 this reduction may be because of less motor vehicle traffic and suspended manufacturing. According to data provided by the Freeway Bureau, Ministry of Transportation and Communications of Taiwan, a decrease in motor vehicle traffic was noted during the lockdown period.38 In addition, the Department of Statistics, Taiwan, revealed a sharp decrease in the numbers of heavily polluting industries, such as chemical, petroleum, and coal industries.39 The above findings are consistent with global trends. However, other possible causes of reduction in pollution readings besides the lockdown may exist. Compared with 2019, 2020 witnessed reduced rainfall. The mean temperature was higher in 2020.40 Both decreased rainfall and increased temperature does not cause a negative effect on PM2.5 concentrations and is unlikely to confound the results. The main sources of PM2.5 pollution in Taiwan are traffic (36%), overseas imports from the mainland (27%), industries (25%), and nature (12%).41 However, in the Taichung region, where the study was conducted, a large coal-fired power plant with a heavy smokestack is the largest source of air pollution. Moreover, PM2.5, sulfur oxides, and nitrogen oxides account for 14.5%, 63.6%, and 39.2%, respectively, of the total emissions of Taichung City.
Our research suggests that controlling air pollution is crucial for reducing the events of renal function decline. In fact, the major finding of our study is not the decrease in average PM2.5 concentration or average air quality index but rather the dramatic reduction in cumulative days with critical concentrations of air pollution. The average annual concentration of PM2.5 decreased only by 13.0% in 2020; however, cumulative days with PM2.5 concentration >35 μg/m3 decreased by 30.4% in 2020. Moreover, the percentage of PM2.5 air quality index >150 (unhealthy level) decreased by 93% in 2020. Those fewer days with critical levels of air pollution have more realistic effects as reflected by our study results.
Our study has some limitations. First, our datasets had no information on patients’ time spent in traffic or outdoors. Therefore, the accurate determination of patients’ exact exposure remains challenging. Second, the majority of all patients undergoing dialysis were enrolled in the pre-ESRD program before dialysis initiation (63.9%). However, currently no data exists between enrolled and unenrolled patients. We cannot be certain if pre-ESRD program enrollees can fully represent patients with advanced CKD. Third, our cohort included only patients with stage 5 CKD who were not undergoing dialysis. Therefore, the findings may not be generalized to patients with other stages of CKD. Because this is a retrospective study, the possibility of unmeasured residual confounding exists. A recently published study revealed both linear and nonlinear associations between PM2.5 and NO2 concentrations and the incidence of eGFR decline in patients with CKD stages 3B, 4, and 5.42 More evidence from detailed longitudinal and direct causal research is required to clarify the cause-and-effect relationship between specific types of air pollution and kidney injury.
Conclusion
The COVID-19 pandemic provided a unique opportunity to study the relationship between air pollution and CKD progression. Although we could not demonstrate a cause-and-effect relationship, our findings support the global strategy of reducing air pollution to prevent CKD progression. Our findings can be used as reference in future kidney care.
Data Sharing Statement
Weather data were obtained from official records of the Taiwan Air Quality Monitoring Network of Environmental Protection Administration, and the meteorological conditions can be obtained online at https://airtw.epa.gov.tw/CHT/Themes/LinkOut.aspx accessed on January 10, 2022.
Institutional Review Board Statement
This study was approved by the Research Ethics Committee of Taichung Veterans General Hospital, Taichung, Taiwan (CE19222B-1).
Informed Consent Statement
This was a retrospective study, and data were acquired from the Taichung Veterans General Hospital Research Database with the permission of the hospital’s Clinical Informatics Research and Development Center.
Acknowledgments
Authors thank the Clinical Informatics Research and Development Center of Taichung Veterans General Hospital for assistance in data collection and Miss Lin, Fen-Yi for assistance in data preparation. The authors thank the Biostatistics Task Force of Taichung Veterans General Hospital and Mr. Chen, Jun-Peng for their assistance in performing statistical analysis. This manuscript was edited by Wallace Academic Editing.
Funding
This was a principal investigator–initiated research and no funding or grant support was received.
Disclosure
Authors declare no competing interests.
References
1. Billions of people still breathe unhealthy air. 4 April 2022; 2022. Available from: https://www.who.int/news/item/04-04-2022-billions-of-people-still-breathe-unhealthy-air-new-who-data.
2. Valavanidis A, Fiotakis K, Vlachogianni T. Airborne particulate matter and human health: toxicological assessment and importance of size and composition of particles for oxidative damage and carcinogenic mechanisms. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2008;26(4):339–362. doi:10.1080/10590500802494538
3. Harrison RM, Yin J. Particulate matter in the atmosphere: which particle properties are important for its effects on health? Sci Total Environ. 2000;249(1–3):85–101. doi:10.1016/s0048-9697(99)00513-6
4. Solomon PA, Sioutas C. Continuous and semicontinuous monitoring techniques for particulate matter mass and chemical components: a synthesis of findings from EPA’s Particulate Matter Supersites Program and related studies. J Air Waste Manag Assoc. 2008;58(2):164–195. doi:10.3155/1047-3289.58.2.164
5. Chin MT. Basic mechanisms for adverse cardiovascular events associated with air pollution. Heart. 2015;101(4):253–256. doi:10.1136/heartjnl-2014-306379
6. Brook RD, Rajagopalan S, Pope CA, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010;121(21):2331–2378. doi:10.1161/CIR.0b013e3181dbece1
7. Afsar B, Elsurer afsar R, Kanbay A, Covic A, Ortiz A, Kanbay M. Air pollution and kidney disease: review of current evidence. Clin Kidney J. 2019;12(1):19–32. doi:10.1093/ckj/sfy111
8. Li G, Huang J, Wang J, et al. Long-term exposure to ambient PM(2.5) and increased risk of CKD prevalence in China. J Am Soc Nephrol. 2021;32(2):448–458. doi:10.1681/asn.2020040517
9. Blum MF, Surapaneni A, Stewart JD, et al. Particulate matter and albuminuria, glomerular filtration rate, and incident CKD. Clin J Am Soc Nephrol. 2020;15(3):311–319. doi:10.2215/cjn.08350719
10. O’Neill MS, Diez-Roux AV, Auchincloss AH, et al. Airborne particulate matter exposure and urinary albumin excretion: the Multi-Ethnic Study of Atherosclerosis. Occup Environ Med. 2008;65(8):534–540. doi:10.1136/oem.2007.035238
11. Xu X, Wang G, Chen N, et al. Long-term exposure to air pollution and increased risk of membranous nephropathy in China. J Am Soc Nephrol. 2016;27(12):3739–3746. doi:10.1681/asn.2016010093
12. Bowe B, Xie Y, Li T, Yan Y, Xian H, Al-Aly Z. Particulate matter air pollution and the risk of incident CKD and progression to ESRD. J Am Soc Nephrol. 2018;29(1):218–230. doi:10.1681/asn.2017030253
13. Mehta AJ, Zanobetti A, Bind MA, et al. Long-term exposure to ambient fine particulate matter and renal function in older men: the veterans administration normative aging study. Environ Health Perspect. 2016;124(9):1353–1360. doi:10.1289/ehp.1510269
14. Bowe B, Xie Y, Li T, Yan Y, Xian H, Al-Aly Z. Associations of ambient coarse particulate matter, nitrogen dioxide, and carbon monoxide with the risk of kidney disease: a cohort study. Lancet Planet Health. 2017;1(7):e267–e276. doi:10.1016/s2542-5196(17)30117-1
15. Chen SY, Chu DC, Lee JH, Yang YR, Chan CC. Traffic-related air pollution associated with chronic kidney disease among elderly residents in Taipei City. Environ Pollut. 2018;234:838–845. doi:10.1016/j.envpol.2017.11.084
16. Yang YR, Chen YM, Chen SY, Chan CC. Associations between long-term particulate matter exposure and adult renal function in the Taipei Metropolis. Environ Health Perspect. 2017;125(4):602–607. doi:10.1289/ehp302
17. Kim HJ, Min JY, Seo YS, Min KB. Association between exposure to ambient air pollution and renal function in Korean adults. Ann Occup Environ Med. 2018;30:14. doi:10.1186/s40557-018-0226-z
18. Neuen BL, Chadban SJ, Demaio AR, Johnson DW, Perkovic V. Chronic kidney disease and the global NCDs agenda. BMJ Glob Health. 2017;2(2):e000380. doi:10.1136/bmjgh-2017-000380
19. Global GB. Global, regional, and National life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–1544. doi:10.1016/s0140-6736(16)31012-1
20. Political declaration of the 3rd high-level meeting of the general assembly on the prevention and control of non-communicable diseases: resolution/adopted by the general assembly; 2018. Available from: https://digitallibrary.un.org/record/1648984/files/A_RES_73_2-EN.pdf.
21. Mishra R, Chauhan A, Singh RP, Mishra NC, Mishra R. Improvement of atmospheric pollution in the capital cities of US during COVID-19. Model Earth Syst Environ. 2021;1–18. doi:10.1007/s40808-021-01269-3
22. Acharya P, Barik G, Gayen BK, et al. Revisiting the levels of aerosol optical depth in South-Southeast Asia, Europe and USA amid the COVID-19 pandemic using satellite observations. Environ Res. 2021;193:110514. doi:10.1016/j.envres.2020.110514
23. Kumar P, Hama S, Omidvarborna H, et al. Temporary reduction in fine particulate matter due to ‘anthropogenic emissions switch-off’ during COVID-19 lockdown in Indian cities. Sustain Cities Soc. 2020;62:102382. doi:10.1016/j.scs.2020.102382
24. Xu Z, Cao R, Hu X, et al. The improvement of air quality and associated mortality during the COVID-19 lockdown in one megacity of China: an empirical strategy. Int J Environ Res Public Health. 2021;18(16):8702. doi:10.3390/ijerph18168702
25. Lai IC, Brimblecombe P. Long-range transport of air pollutants to Taiwan during the COVID-19 lockdown in Hubei Province. Aerosol Air Qual Res. 2021;21(2):200392. doi:10.4209/aaqr.2020.07.0392
26. Tsai MH, Hsu CY, Lin MY, et al. Incidence, prevalence, and duration of chronic kidney disease in Taiwan: results from a community-based screening program of 106,094 individuals. Nephron. 2018;140(3):175–184. doi:10.1159/000491708
27. Chiu PF, Chang CH, Wu CL, et al. High particulate matter 2.5 levels and ambient temperature are associated with acute lung edema in patients with nondialysis Stage 5 chronic kidney disease. Nephrol Dial Transplant. 2019;34(8):1354–1360. doi:10.1093/ndt/gfy144
28. Lin MY, Cheng LJ, Chiu YW, et al. Effect of national pre-ESRD care program on expenditures and mortality in incident dialysis patients: a population-based study. PLoS One. 2018;13(6):e0198387. doi:10.1371/journal.pone.0198387
29. Hsieh HM, Lin MY, Chiu YW, et al. Economic evaluation of a pre-ESRD pay-for-performance programme in advanced chronic kidney disease patients. Nephrol Dial Transplant. 2017;32(7):1184–1194. doi:10.1093/ndt/gfw372
30. Wu C-Y, Liu J-S, Chen C-H, et al. Early comprehensive kidney care in dialysis-requiring acute kidney injury survivors: a populational study. Original research. Front Med. 2022;9:847462. doi:10.3389/fmed.2022.847462
31. Chou C-L, Chung C-H, Chiu H-W, et al. Association of pre-ESRD care education with patient outcomes in a 10-year longitudinal study of patients with CKD stages 3–5 in Taiwan. Sci Rep. 2021;11(1):22602. doi:10.1038/s41598-021-01860-9
32. Hsu C-C. 2020 kidney disease in Taiwan annual report National Health Research Institutes (NHRI), Taiwan; 2021.
33. Lin SY, Ju SW, Lin CL, et al. Air pollutants and subsequent risk of chronic kidney disease and end-stage renal disease: a population-based cohort study. Environ Pollut. 2020;261:114154. doi:10.1016/j.envpol.2020.114154
34. Miyah Y, Benjelloun M, Lairini S, Lahrichi A, Piantino Ferreira AJ. COVID-19 impact on public health, environment, human psychology, global socioeconomy, and education. ScientificWorldJournal. 2022;2022:5578284. doi:10.1155/2022/5578284
35. Liu F, Wang M, Zheng M. Effects of COVID-19 lockdown on global air quality and health. Sci Total Environ. 2021;755(Pt 1):142533. doi:10.1016/j.scitotenv.2020.142533
36. Venter ZS, Aunan K, Chowdhury S, Lelieveld J. COVID-19 lockdowns cause global air pollution declines. Proc Natl Acad Sci U S A. 2020;117(32):18984–18990. doi:10.1073/pnas.2006853117
37. Le T, Wang Y, Liu L, et al. Unexpected air pollution with marked emission reductions during the COVID-19 outbreak in China. Science. 2020;369(6504):702–706. doi:10.1126/science.abb7431
38. Freeway Bureau, Ministry of Transportation and Communications, Taiwan. Traffic volume survey 2022. Available from: https://www.freeway.gov.tw/Publish.aspx?cnid=1652.
39. Department of Statistics, Ministry of Economic Affairs, Taiwan. Yearbook of industrial production statistics 2020; 2021. Available from: https://www.moea.gov.tw/Mns/DOS/content/wHandMenuFile.ashx?file_id=25060.
40. Central Weather Bureau, Taiwan. Climate monitoring 2020 annual report; 2021. Available from: https://www.cwb.gov.tw/Data/service/notice/download/Publish_20210610120207.pdf.
41. Environmental Protection Administration Executive Yuan, Taiwan. 2021 annual report; 2021. Available from: https://www.epa.gov.tw/Page/B84B65A4FDDF5864.
42. Wu Y-H, Wu C-D, Chung M-C, et al. Long-term exposure to fine particulate matter and the deterioration of estimated glomerular filtration rate: a cohort study in patients with pre-end-stage renal disease. Original research. Front Public Health. 2022;10:858655. doi:10.3389/fpubh.2022.858655
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.