")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Alopecia with Vitamin D-Dependent Rickets Type 2 A: A Case Report
Authors Bin Rubaian NF, Al-Awam BS , Aljohani SM, Almuhaidib SR
Received 27 September 2023
Accepted for publication 13 December 2023
Published 3 January 2024 Volume 2024:17 Pages 13—16
DOI https://doi.org/10.2147/CCID.S438505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Nouf F Bin Rubaian,1 Bashayer S Al-Awam,2 Samah M Aljohani,1 Serene R Almuhaidib3
1Department of Dermatology, King Fahad University Hospital, Al Khobar, Saudi Arabia; 2Department of Pediatrics, King Fahad University Hospital, Al Khobar, Saudi Arabia; 3Department of Dermatology, Dammam Medical Complex, Dammam, Saudi Arabia
Correspondence: Serene R Almuhaidib, Department of Dermatology, Dammam Medical Complex, Dammam, Saudi Arabia, Email [email protected]
Abstract: Vitamin D-dependent rickets type II (VDDR2) is a rare inherited autosomal recessive disorder wherein the genetic mutation results in a defect in the vitamin D receptor (VDR), thus leading to target resistance to 1.25-dihydroxy vitamin D. This results in hypocalcemia, hypophosphatemia, secondary hyperparathyroidism, and rickets. We report a case of a four-year-old female child with diffuse alopecia starting 2 weeks after birth, along with frontal bossing, hypoplastic teeth, and an unusual presentation of multiple skin-colored papules over the back. Genetic testing confirmed vitamin D-dependent rickets type 2A.
Keywords: pseudovitamin D-deficiency, rickets-alopecia syndrome, hypocalcemic vitamin D-resistant rickets, genetic mutation
Introduction
Vitamin D-dependent rickets type II (VDDR2) is an inherited rare autosomal recessive disorder.1 This condition is also known as pseudovitamin D-deficiency Type 2, hypocalcemic vitamin D-resistant rickets, or rickets-alopecia syndrome.1 The genetic mutation in chromosomes 12q12-q14 leads to a defect in the vitamin D receptor (VDR), resulting in a target resistance to 1.25-dihydroxyvitamin D, resulting in hypocalcemia, hypophosphatemia, secondary hyperparathyroidism, and rickets.1 Two decades ago, the prevalence of vitamin D-dependent rickets, in all of its types, was approximately 30%; however, in the present time, it has reduced to 0.8%.2
The condition is characterized by a diminished response of organs to vitamin D. Its typical manifestation involves complete body hair loss and the development of rickets in the latter part of the first year of life. Individuals with this disorder may exhibit ongoing rachitic alterations in bones, leading to weakened bones, which in turn contribute to delayed growth, bone discomfort, reduced height, and bowed legs.3 Depending on the presence or absence of alopecia, it is further classified as VDDR type IIA or IIB, respectively.3
Case Report
A four-year-old female child was brought by her family complaining of hair loss over the scalp that started 2 weeks after delivery, with a history of diffuse hair loss over eyebrows and eyelashes. The patient has also been diagnosed with rickets due to walking difficulties in the first year of life. The patient’s parents are cousins, and these abnormalities were not detected among the parents or the younger sibling.
On clinical examination, both height and weight were below the third percentile, and alopecia was observed including loss of hair on the scalp, eyelids, and the entire body with few terminal hairs observed over the vertex, eyebrows, and eyelashes (Figure 1). The patient had features of rickets including frontal bossing (Figure 2A) and hypoplastic teeth (Figure 2B). The patient developed these multiple skin-colored papules over the back (Figure 2C) 1 month ago which was confusing for congenital atrichia with papules. Trichoscopy findings showed absent follicular hair ostia (Figure 3). A hair examination was done under light microscopy to exclude other hair shaft disorders before genetic testing. Hair pull test to exclude loose anagen phase.
 |
Figure 1 Diffuse alopecia with few terminal hairs. (A) Fronal view, (B) Vertex view. |
 |
Figure 2 (A) Frontal bossing, (B) Hypoplastic teeth, (C) Multiple skin-colored papules over the back. |
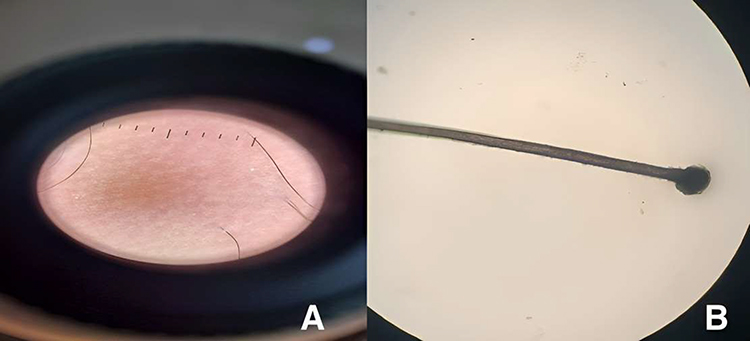 |
Figure 3 Trichoscopy findings. (A) Preserved follicular Ostia but empty (B) The anagen hair root is pigmented and covered by sheath. |
On investigations, initial calcium level revealed hypocalcemia (serum calcium levels: 6.8 mg/dL; reference range: 8.8–10.6 mg/dL) and increased alkaline phosphatase levels were observed (580 IU/L; reference range: 50–155 IU/L). Phosphorus (3.8 mg/dl; reference range: 3.4–4.5 mg/dL), parathyroid hormone level (225 pg/mL). The patient was started on 1-Alpha 1 mcg twice per day in addition to Calcic 5 mL twice per day. After 6 months of treatment, serum calcium was found to increase to normal levels. On the other hand, alkaline phosphatase level decreased and parathyroid hormone levels increased.
X-ray of both hands showed ossification of the capitate, hamate, triquetrum, and trapezium bones only. Delayed appearance of lunate bone (2–4 years). All metacarpal heads, lower end of ulna, and lower end of radius are fused, and these X-ray findings are compatible with bone age of 4 years old. Lower limbs and hips x-ray exhibited normal configuration of both femoral heads, acetabula, and joint spaces of both hip joints with no obvious degenerative changes. Touch both knee joints. No obvious fracture line. No evidence of erosive, destructive, or sclerotic lesion, or periosteal reaction was observed. Genetic testing was done which showed a homozygous pathogenic variant identified in the VDR gene. The genetic diagnosis of autosomal recessive vitamin D-dependent rickets type 2A (VDDR2A) is confirmed.
Discussion
In 1978, Brooks et al reported the first case of a 22-year-old woman with hypocalcemia, secondary hyperparathyroidism, osteomalacia, and osteitis fibrosa cystica along with normal levels of serum 25-hydroxyvitamin D and markedly elevated levels of serum 1.25-dihydroxy vitamin D, later, Brooks et al named this disorder as VDDR2.4 Since then, few reports have been published with patients presenting with similar findings.
VDDR2 may cause a wide range of clinical features, including growth delay, early-onset rickets, weakness of muscles, seizures, alopecia, as well as several other dental defects.5 Alopecia usually presents at birth or in the first few months of life, and advances to alopecia totalis by childhood. Typically, it is refractory to management.6 Symptoms may vary between patients; nonetheless, early diagnosis is essential to optimize development and growth. Interestingly, our patient had multiple skin-colored papules involving the back in addition to the typical symptoms of growth delay, rickets, dental defects, and alopecia totalis except for a few terminal hairs over the vertex.
The diagnosis of this condition can be confirmed by assessing serum 1.25(OH)2 vitamin D levels, which tend to be elevated or within the normal range in VDDR2 patients. This serves as a distinguishing factor from vitamin D-dependent rickets type I, where individuals typically exhibit low serum 1.25(OH)2 vitamin D levels due to impaired function of the 1-alpha-hydroxylation enzyme in the kidneys. In general, VDDR2 patients show resistance to standard doses of vitamin D, necessitating the administration of larger doses for effective management of the cases.7 Mild-to-moderate cases are managed by high doses of oral calcitriol in addition to supplemental calcium, and severe cases will need the administration of high doses of intravenous calcium infusion. On the downside, these medications could lead to side effects due to hypercalcemia such as cardiac arrhythmias.5
VDDR2 appears to be more frequently documented in Arab populations, although the precise cause remains unclear. This prevalence could be attributed to a high incidence of the disease’s gene within Arab communities or the elevated rate of consanguineous marriages among Arabs.8 In 2003, Al-Khenaizan et al reported the initial case of VDDR2 in Saudi Arabia, involving two brothers exhibiting alopecia, severe hypotonia linked to hypocalcemia, extensive rachitic bone changes, and dental abnormalities. Despite being unresponsive to all forms of Vitamin D, their condition showed improvement with intravenous calcium infusion, addressing their rickets and subsequently enabling them to walk. Unfortunately, the alopecia did not respond to the medications administered.
Conclusion
Vitamin D-dependent rickets type II A is a very rare disorder, with only a few cases being reported in the English literature. We report a case of a 4-year-old Saudi female child with Vitamin D-dependent rickets type II A for its rarity and the presentation of unusual multiple skin lesions.
Abbreviations
VDDR2, Vitamin D-dependent rickets type II; VDR, vitamin D receptor.
Ethics Approval and Consent for Publication
Written informed consent for publication of this case report including photography and medical data was obtained and signed by the patient’s parents. Institutional ethical approval was not required to publish this case report.
Acknowledgments
The authors would like to thank all department colleagues who contributed to this case study.
Author Contributions
All authors made a crucial contribution to the reported work, contributing significantly to the conception, study design, execution, data acquisition, analysis, and interpretation. They actively participated in drafting, revising, or providing critical reviews of the article. All authors gave their final approval for the version to be published, reached an agreement on the journal to which the article has been submitted, and committed to being accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Levine MA. Diagnosis and management of vitamin D dependent rickets. Front Pediatr. 2020;8:315. doi:10.3389/fped.2020.00315
2. Vupperla D, Lunge SB, Elaprolu P. Vitamin D-dependent rickets type II with alopecia: a rare case report. Indian J Dermatol. 2018;63(2):176–179. doi:10.4103/ijd.IJD_434_17
3. Acar S, Demir K, Shi Y. Genetic causes of rickets. J Clin Res Pediatr Endocrinol. 2017;9(Suppl 2):88–105. doi:10.4274/jcrpe.2017.S008
4. Brooks MH, Bell NH, Love L, et al. Vitamin-D-dependent rickets type II. Resistance of target organs to 1,25-dihydroxyvitamin D. N Engl J Med. 1978;298(18):996–999. doi:10.1056/NEJM197805042981804
5. Thakur M. Familial Vitamin D-dependent rickets Type 2A: a report of two cases with alopecia and oral manifestations. J Oral Maxillofac Pathol. 2019;23(Suppl 1):130–133. doi:10.4103/jomfp.JOMFP_309_18
6. Malloy PJ, Hochberg Z, Tiosano D, Pike JW, Hughes MR, Feldman D. The molecular basis of hereditary 1,25-dihydroxyvitamin D3 resistant rickets in seven related families. J Clin Invest. 1990;86(6):2071–2079. doi:10.1172/JCI114944
7. Murali MV, Usharani T. Vitamin D dependent rickets type II with alopecia. J Life Sci. 2013;5:57–59.
8. Al-Khenaizan S, Vitale P. Vitamin D-dependent rickets Type II with alopecia: two case reports and review of the literature. Int J Dermatol. 2003;42(9):682–685. doi:10.1046/j.1365-4362.2003.01816.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.