")
Back to Journals » International Journal of General Medicine » Volume 15
An Overview of Systematic Reviews: Acupuncture in the Treatment of Essential Hypertension
Authors Zhou M , Bu H , Wang D, Wang M, Guan Y, Sun X, Tian Z, Wang H
Received 2 September 2022
Accepted for publication 26 October 2022
Published 8 November 2022 Volume 2022:15 Pages 8093—8109
DOI https://doi.org/10.2147/IJGM.S387490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mi Zhou, Huaien Bu, Dongjun Wang, Mengyang Wang, Yuanyuan Guan, Xuan Sun, Zhikui Tian, Hongwu Wang
School of Public Health, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China
Correspondence: Hongwu Wang, Email [email protected]
Objective: Acupuncture treatment is widely used for essential hypertension (EH), and numerous systematic reviews on acupuncture for EH have been published. This article provides an overview of the effectiveness and safety of acupuncture for EH and assesses the quality of reports, methodological bias, quality of evidence and risk of bias for inclusion in the evaluation.
Methods: Two researchers independently computer searched Pubmed, EMbase, The Cochrane library, WOS, CBM, CNKI, Wangfang Data, VIP and other Chinese and English databases with a search time frame from the date of creation to 13th October 2022; and independently screened systematic reviews of acupuncture therapy for EH; and finally The Report Quality Assessment Tool (PRISMA 2020), Methodological Quality Assessment Tool (AMSTAR2), Grading of Evidence Assessment Tool (GRADE), and Bias Assessment Tool (ROBIS) were used independently to assess the bias of the included literature.
Results: A total of 11 systematic reviews were included. The included studies mainly reported on outcome indicators such as efficiency rate, end SBP, end DBP, SBP change value, DBP change value, etc. Deficiencies in the quality of PRISMA 2020 reporting were mainly in the areas of independent screening by multiple researchers, use of GRADE for analysis, early registration, description of conflict of interest, and public access to information; the results of the AMSTAR 2 tool evaluation were mostly were very low, and of the 16 entries affecting the methodological quality of the systematic evaluation, entries 2/3/4/5/12/16 had the greatest methodological bias; GRADE assessed the quality of evidence for key outcome indicators, with a few being low and all others being very low; and ROBIS reported a high level of bias in the literature.
Conclusion: Current acupuncture has some efficacy in the treatment of essential hypertension, but its quality of evidence is low. It is hoped that the quality of relevant literature reporting, methodological quality, quality of evidence, and bias will improve.
Keywords: acupuncture, essential hypertension, systematic review, overview
Essential hypertension (EH) is a chronic condition characterized by high blood pressure, tinnitus, and dizziness as the primary clinical symptoms, and accounts for more than 95% of people with hypertension. Hypertension is a leading cause of unnatural death, and chronically high blood pressure can harm the brain, heart, kidneys, and other organs, bringing down quality of life.1 It has been reported that in 2025, 1.5 billion people worldwide will suffer from hypertension, accounting for one-third of the global population.2 The prevalence, treatment, and control rates of hypertension in Chinese adults are 46.9%, 40.7%, and 15.3% respectively, according to the Clinical Application Guidelines for the Treatment of Essential Hypertension with Proprietary Chinese Medicines (2021),with treatment and control rates remaining low compared to those in developed countries;3 the incidence among adults over the age of 80 is as excessive as 90%.4 The definition of hypertension varies from country to country; in the USA5 and China3, for example.
The prevailing hypertension treatment has a considerable duration and treatment regimen. Western drugs are effective but easily resistant, have toxic side effects on the liver and kidneys when taken for a long time, and are not as effective in controlling blood pressure as they should be, and this can be a incremental waste of medical resources.6 As a result, researchers are currently investigating how to improve the therapy procedure. Hypertension is classified as “vertigo” and “headache” in Chinese medicine. Long-term activation of the sympathetic nervous system (SNS) is now linked to the development of EH, according to a growing body of research,7 and that acupuncture may produce antihypertensive effects through neuroendocrine regulation,8 making it a potentially safer and more effective antihypertensive therapy. In recent years, evidence-based medicine and clinical research on acupuncture have become increasingly intertwined,9 and systematic review are the best evidence to guide therapeutic practice from an evidence-based viewpoint. The authors found through a preliminary search that several systematic views exploring the efficacy of acupuncture therapy on EH have been published, but only one review of the methodological quality of these systematic evaluations has been published.10 The quality of the evidence provided should be updated accordingly. Currently, there are many tools to overview systematic reviews, such as PRISMA 2020, GRADE, AMSTER2, ROBIS. This study utilizes systematic reviews to overview the quality of evidence from current systematic reviews in order to further clarify the efficacy of acupuncture in the treatment of EH and provide ideas and evidence to support better research and treatment of EH in clinical practice, for the for the benefit of patients.
Information and Methods
Inclusion Criteria
Study Population
Patients who met the diagnostic criteria of the country’s hypertension guidelines,3,5 regardless of gender, age and race.
Interventions
The test group was treated with acupuncture (including acupuncture, electroacupuncture, warm acupuncture, etc.), The selected acupuncture points are the 12 main meridian points, and the control group with relevant non-acupuncture treatments (including sham acupuncture, placebo, western medicine, life interventions, etc.).
Outcome Indicators
At least one pre-reported outcome: effective rate, end-of-life SBP, end-of-life DBP, change in SBP value, change in DBP value, adverse effects.
Type of Study Design
A systematic review based on a randomised controlled trial (RCT), with or without quantitative Meta-analysis. The language was English and Chinese.
Exclusion Criteria
Acupuncture as a non-primary intervention in the treatment group, for examples include Ashi point, ear needle, head needle and ankle acupuncture points other than the 12 main meridians, sham acupuncture, acupressure, moxibustion, Tuina and wet cupping or acupuncture as an intervention in the control group, ② Inclusion of non-RCT literature in the systematic review, ② Inclusion of non-RCT literature in the systematic review ③ duplicate publications, ④ non-systematic reviews/meta-analyses, reviews, conference abstracts, ⑤ studies for which data could not be identified, and ⑥ dissertations.
Search Strategy
Two researchers (Mi Zhou and Dongjun Wang) independently and systematically searched Pubmed, CNKI, WANGFANG, VIP and other Chinese and English databases, all from the date of creation to 13 Oct 2022, for the Chinese keywords “acupuncture”, “electro acupuncture”, “needle warming”, “hypertension”, “systematic review”, in English “hypertension” “acupuncture” “needle warming” “electro acupuncture” “systematic review”, the search was carried out using a combination of subject terms and free words. Using Pubmed as an example, the search strategy is shown in Figure 1. after checking using the ENDNOTE software, two researchers independently screened according to exclusion criteria.
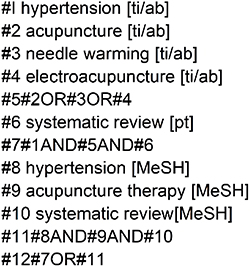 |
Figure 1 Search strategy for Pubmed. |
Study Inclusion and Data Extraction
Two evaluators (Mi Zhou and Yuanyuan Guan) alone included studies that met the requirements according to the inclusion criteria, and extracted data from the final included studies, mainly on study title, authors, year of publication, number of included studies, interventions, controls, original study methodological quality assessment tools, outcome indicators, and conclusions. In case of disagreement, a third person (Dongjun Wang) ruled.
Relevant Assessments
Two evaluators (Mi Zhou and Xuan Sun), with the names of the authors withheld, assessed the quality of reporting of the included studies by PRISMA 2020, the methodological quality of the included studies by AMSTAR 2, the quality of evidence of the included studies by GRADE, and the bias of the included studies by ROBIS, respectively, and in case of disagreement, the third person (Dongjun Wang) ruled.
Study Results
Literature Screening Process and Results
The computer database yielded a total of 256 items, including 79 in Chinese and 177 in English. After duplicating 38, reviewing the titles and abstracts 183 were deleted, leaving 35. Finally, after manual checking and careful reading of the full text, 11 articles met the requirements.(Figure 2).
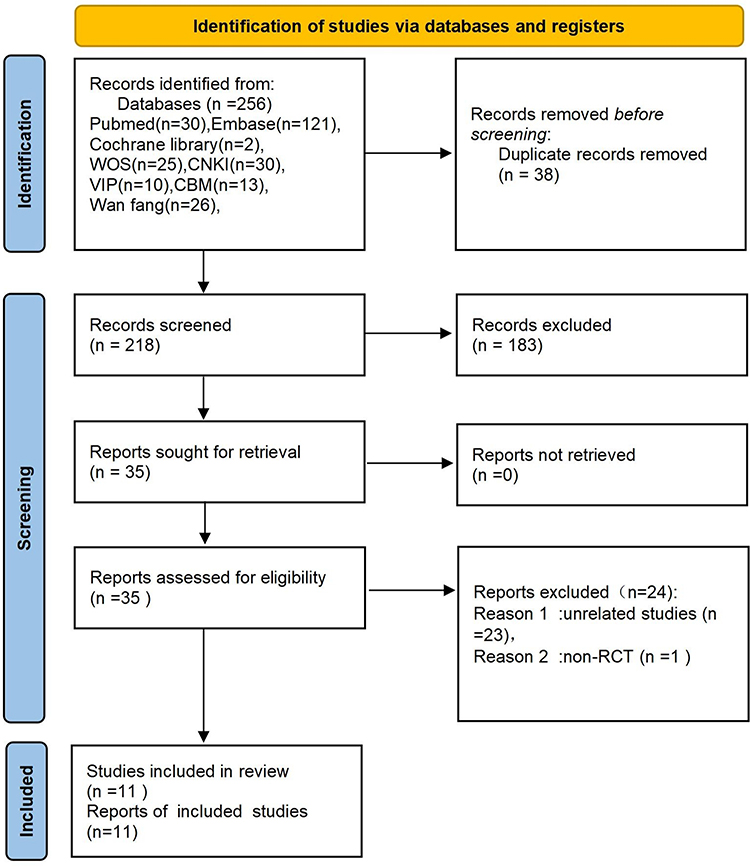 |
Figure 2 Identification of studies via databases and registers. |
Basic Characteristics of Included Studies
A total of 11 included studies,6,11–20 of which 3 were in English6,11,12 and 8 in Chinese,13–20 with the earliest and most recent published in 201113 and 2018.19,20 Of the 116,11–20 papers, seven6,11,12,16,18–20 used the risk of bias tool recommended by the Cochrane system for assessing the methodological quality of original studies and four13–15,17 used the modified Jadad scale, the number of included studies ranged from 5 to 53, with the main treatment modalities in the treatment group being acupuncture, acupuncture plus Western medicine, electroacupuncture, and electroacupuncture plus Western medicine, and in the control group being western medicine, sham acupuncture plus western medicine, and lifestyle, etc. The specific characteristics of the included studies are detailed in Table 1 below.
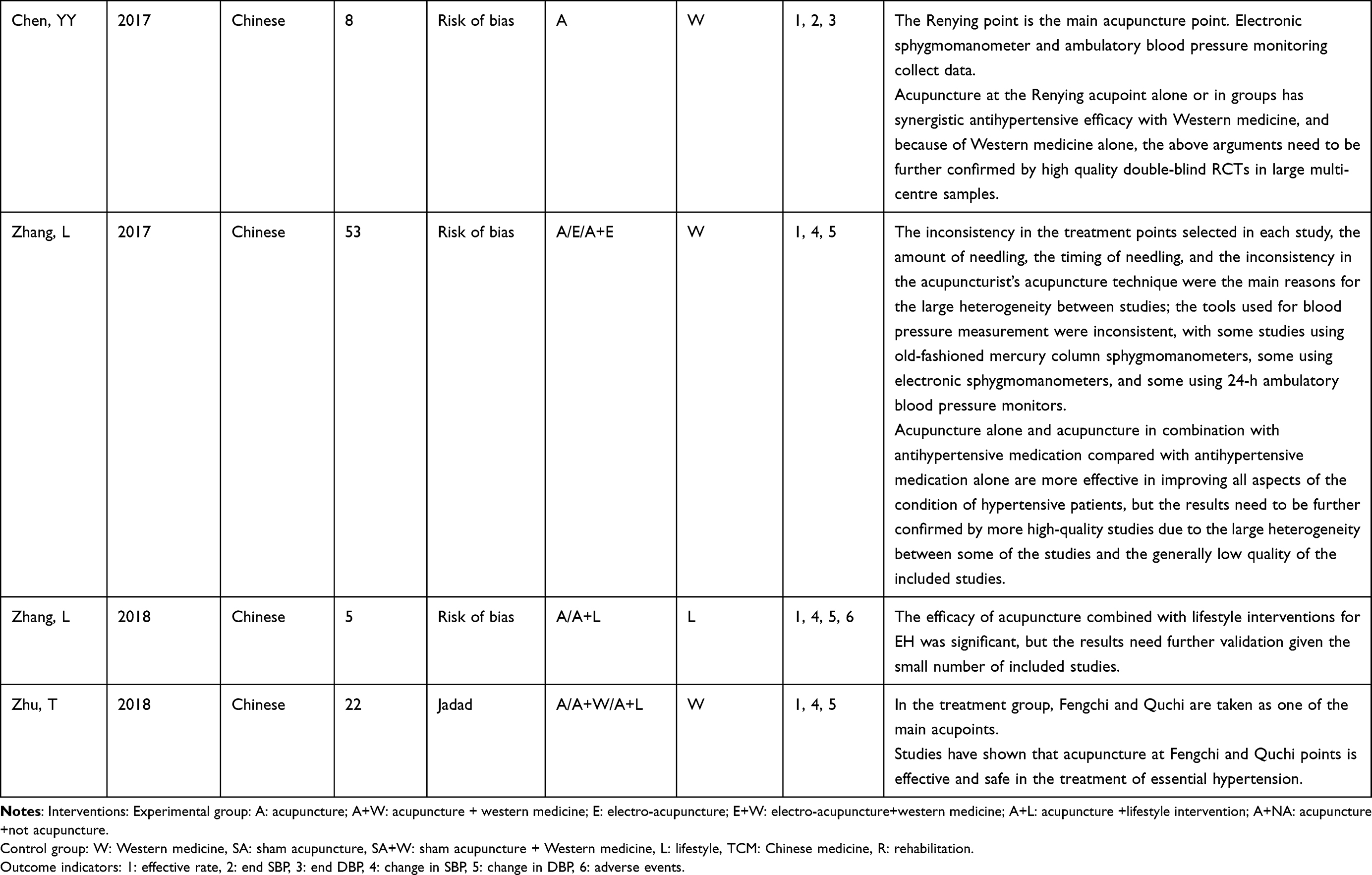 |
Table 1 Basic Characteristics of the Included Studies |
PRISMA Statement for Evaluation of Report Quality of Included Studies
The quality of reports from the included systematic reviews was evaluated using the PRISMA 2020, with each entry judged to be normative and correctly reported rated as 1, partially reported as 0.5, and not reported or incorrectly scored as 0; the total score was 27, with scores of 22–27 indicating a more complete report, followed by those of 16–21, and less than 15 indicating a more flawed report.21 The scores showed that only one12 study was more complete, 4 studies were more flawed13,14,16,20 and the rest were of average quality. The main points lost were in 8, 15, 22, 24, 26, 27, which shows that there were some deficiencies in independent screening by multiple researchers, using GRADE for analysis, registering in advance, stating conflicts of interest, and public access to information. The quality assessment of evaluation reports (based on PRIMSA 2020) are detailed in Table 2 below.
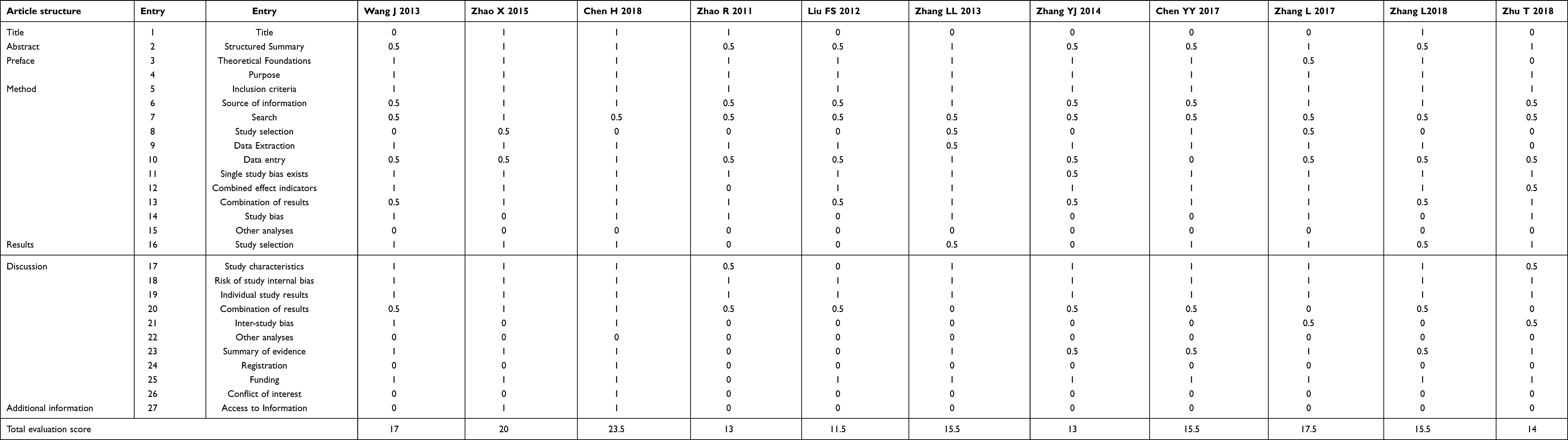 |
Table 2 Quality Assessment of Evaluation Reports (Based on PRIMSA 2020) |
AMSTAR2
Evaluated the methodological quality of systematic reviews through 16 entries.22 96,11,13–17,19,20 studies were considered very low, they all had more than one critical flaw (entries 2/4/7/9/11/13/15) and multiple non-critical flaws, 118 were rated low and 1 was rated medium level.12 As shown in Table 3.
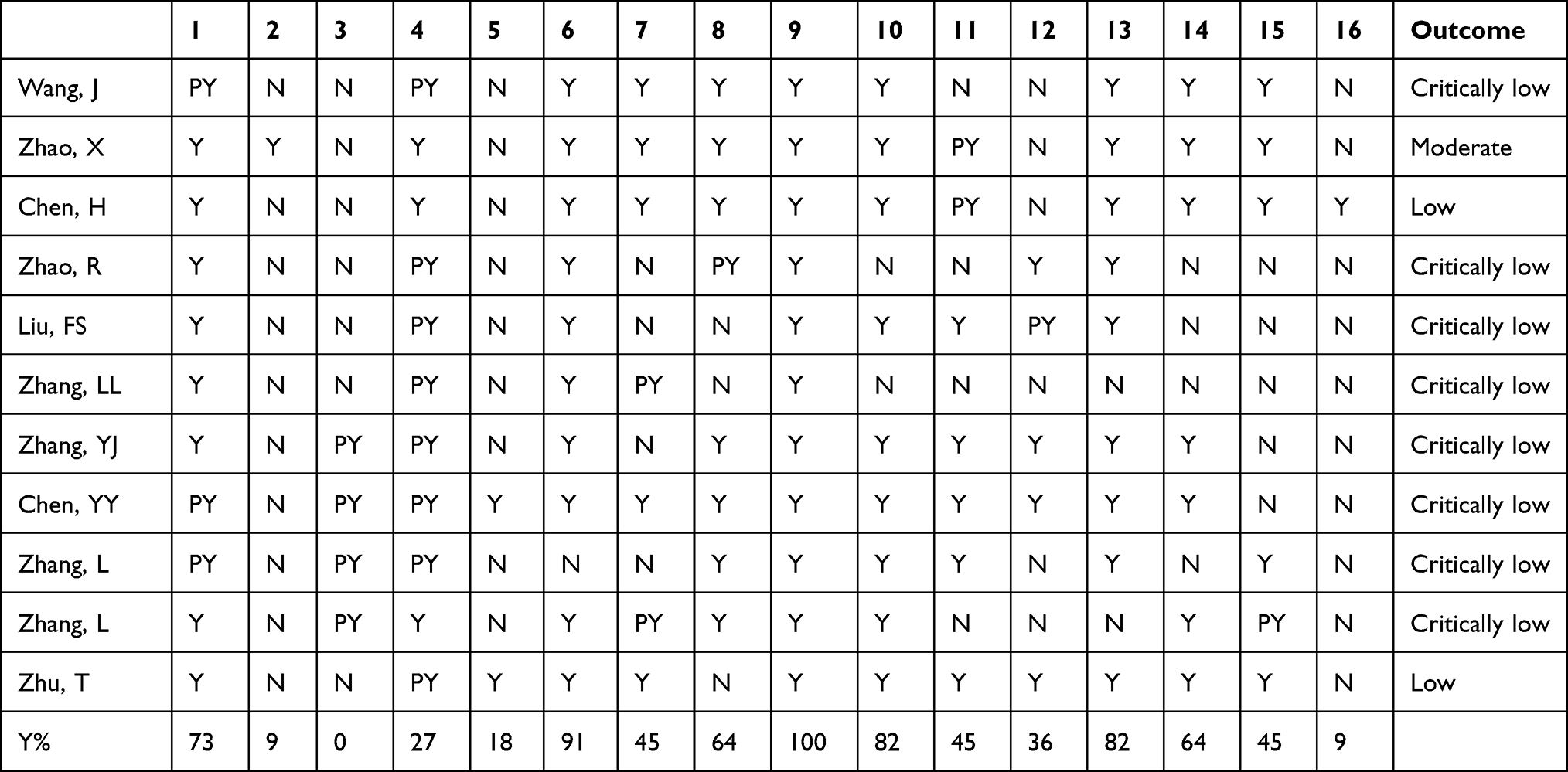 |
Table 3 Analysis of Methodological Quality (Based on the AMSTAR2) |
Grading of Evidence Evaluation
GRADE system grading criteria generated in 2004 are more appropriate for grading the evidence for the development of Chinese medicine.10 In this study, the quality of evidence was assessed based on the GRADE system methodology23 for the 11 outcome indicators reported in the included systematic reviews, with a total of 40 items, with 5 items (13.5%) being low grade and all the rest being very low grade (86.5%), with risk bias (100%) and publication bias (100%) being the main reasons for downgrading. The assessment table (Table 4) shows that the quality of evidence for a few of the above outcome indicators was low, with the remainder downgraded to very low due to poor methodological quality, consistency and precision of the included studies.
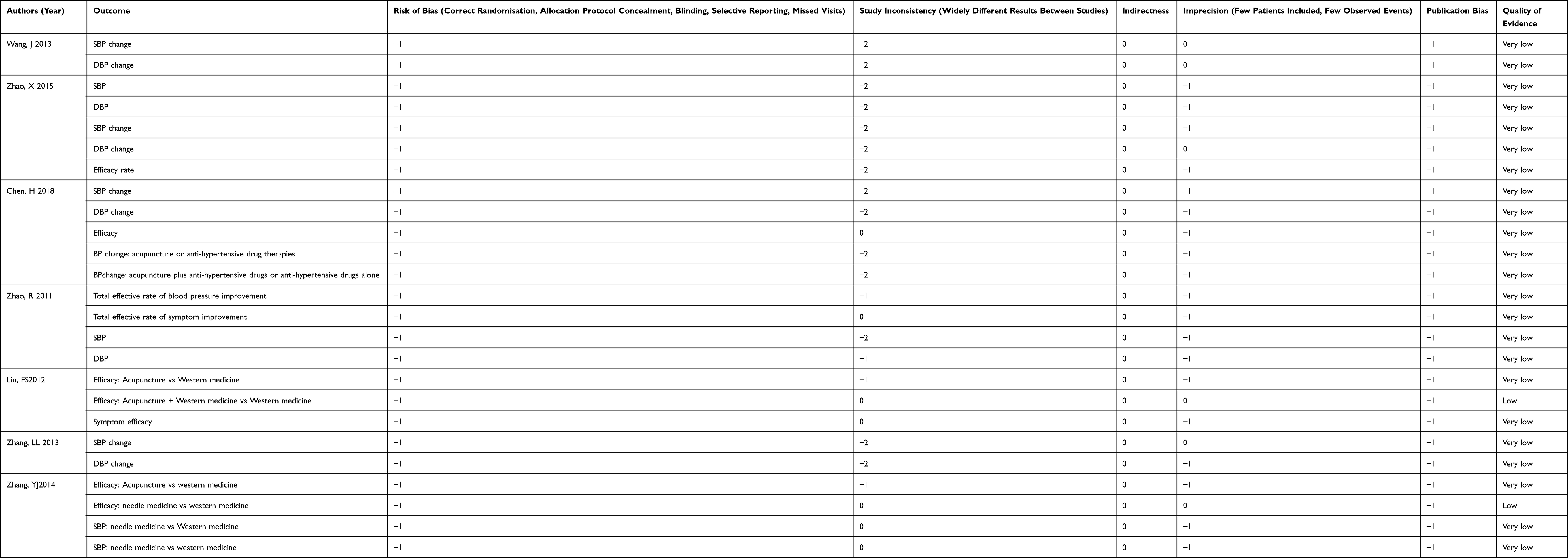 |
Table 4 Level of Evidence Ratings (Based on the GRADE) |
Risk of Bias Assessment
ROBIS is a new tool published by the University of Bristol, UK, in 2014 to assess the risk of bias for inclusion in studies,24 and there are 3 main stages to the assessment process, which are assessed in this paper for stages 2 and 3. The first assesses the degree of bias in the inclusion exclusion criteria and shows that all (100%) of the inclusion exclusion criteria are low risk; the second assesses the degree of risk of bias in the retrieval and screening of studies and shows that very few (18.1%) are low risk, the third assesses the degree of bias in data extraction and quality assessment and shows that the majority (90.9%) are low risk and the fourth assesses the degree of bias in data synthesis and presentation of results The fourth item assessed the degree of bias in data synthesis and presentation of results and showed that very few (18.1%) were low risk, and the fifth item assessed the risk of bias in systematic evaluation and showed that few (27.3%) were low risk. It is inferred that there was a degree of bias in the included studies. As shown in Table 5.
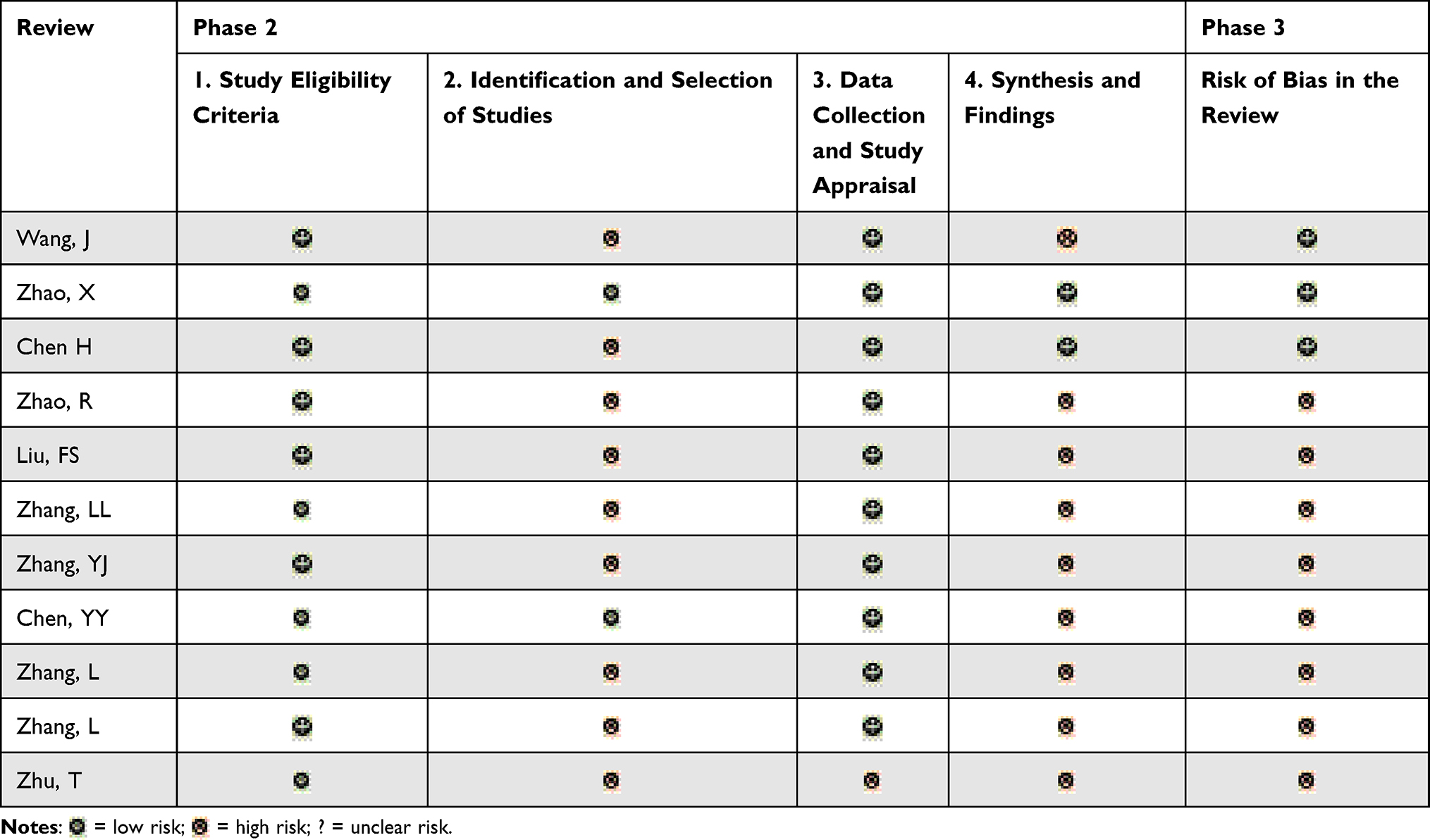 |
Table 5 Suggested Tabular Presentation for ROBIS Results |
Adverse Reactions
Only brief descriptions of adverse effects were offered in none of the studies that were included.
Discussion
Main Outcome
A systematic review is a comprehensive overall analysis of primary data and is one of the best sources of evidence for evidence-based clinical practice. It is at a high level in the hierarchy of evidence, and the quality of the systematic review determines whether it can truly provide a scientific and theoretical basis for clinicians and policy makers. The overview of this systematic review concludes that acupuncture has been shown to be effective in improving EH without major adverse effects. However the quality of the included studies was generally low with very few exceptions. The main findings of the studies were as follows:
The methodological quality of all the included systematic reviews on the use of acupuncture in EH was very low, as indicated by AMSTAR 2 scale in the current work. A few6,12 described searches and grey literature searches. In addition, 214,20 systematic reviews did not describe in detail the essential characteristics of the included studies, and one15 with incomplete basic features, which prevented us from comparing studies at baseline. 3 reviews did not provide a list of excluded literature or did not provide information on excluded literature.13–15 Only 112 mentioned a relevant conflict of interest. Only 112 assessed the risk of bias for each included study at the time of Meta-analysis and only 56,11,12,18,20 conducted quantitative analyses that adequately investigated publication bias, all of which compromise the strength of the argument for outcome indicators and suggest that the current original study design of acupuncture therapy for EH is flawed and lacks scientific and standardised methodological guidance. At this point medical researchers should pay more attention to the above issues and improve their work and methodological quality in order to provide high quality findings to inform guideline development and clinical decision making.
In this work, The GRADE evidence rating system was used to rate the quality of individual outcome indicators. Based on the results obtained, the quality of evidence for 35 outcome indicators was very low, 5 were of low quality and there was little variation in the quality of individual indicators, the very low quality of evidence for most indicators indicates that there is variation in study outcomes. Typically, imprecision and publication bias in studies were the main reasons for most downgrades, followed by inconsistency and limitations. Of these, imprecision was mainly attributed to wide confidence intervals (CIs) or inadequate sample sizes for the included studies, as well as poor overlap of CIs. In addition, publication bias was mainly reflected in asymmetric funnel plots, insufficiently narrow confidence intervals, and the inclusion of studies that did not meet the criteria for potentially publication biased studies. On the other hand, inconsistency was reflected in the low overlap of CIs between studies, small p and high heterogeneity (I 2 > 50%). Limitations were due to the inclusion of original studies at risk of randomisation, blinding and hidden implementation allocation. The degradation in the quality of evidence for outcome indicators has decreased considerably over the past 5 years, suggesting that researchers are increasingly focusing on randomisation, blinding, allocation concealment, and study design aspects of study design. Therefore, to address the issues of imprecision and publication bias, the author recommends that researchers should estimate sample size, standardise the design and conduct of clinical trials, and enhance the search for grey areas to reduce bias.
The first of the ROBIS bias scenarios, the degree of bias in the inclusion and exclusion criteria, a small number of inclusion criteria were less clear and the results showed that the majority of inclusion and exclusion criteria were low risk. The fourth assessed the degree of bias in the synthesis of data and presentation of results, as most studies were heterogeneous and some did not use sensitivity analysis, the results showed less low risk and more uncertainty, the fifth assessed the risk of bias in the systematic reviews, most studies did not explain the risk of bias in the treatment and few studies discussed the statistical significance and the results showed mostly high risk. It is inferred that there was some degree of bias in the included studies.
Limitations and publication bias were the main reasons for downgrading according to the GRADE quality grading, however, we did not find a steady improvement in the methodological quality of the projects over the last years, mainly because the main purpose of reporting guidelines is to help authors remember all the items to be reported, not to perform an overview.25 The results of this review are consistent with those of reviews in other areas (eg depression),26 where methodological quality and strength of evidence were low or very low. Furthermore, Chun27 reached the same conclusion in their study on the methodological quality and strength of evidence of reviews on acupuncture for COPD. Medical research suggests that there may be substantial methodological problems with acupuncture in the treatment of disease. We must therefore acknowledge that a double-blind approach to acupuncture trials is not feasible. However, the quality of the original studies included in the study is also very important and therefore some items may not be well reflected and covered in the GRADE system and the AMSTAR 2 tool, thus affecting the strength of the evidence. In addition, a number of methodological issues and the quality of outcome indicators are closely related to the quality of the included studies, including the listing and selection of inclusion/exclusion criteria, the description of baseline characteristics and conflicts of interest, the design of study pre-protocols, the assessment of study outcomes, and the interpretation of heterogeneity and publication bias.28 As previously mentioned, although double-blinding of acupuncture trials is not usually feasible, investigators need to combine diagnostic and therapeutic features with modern clinical RCTs.
Limitations
The current methods of measuring hypertension values are mainly divided into in-office blood pressure (OBPM), 24-hour ambulatory blood pressure (ABPM), and home self-measured blood pressure (HBPM).5 OBPM is currently the main method of diagnosing hypertension, grading blood pressure levels, and observing the efficacy of antihypertensive therapy in China, but there are cases of incorrect posture of patients, unclear clinic environment, resulting in biased measurement values, and ABPM is regarded as the gold standard for blood pressure monitoring and management, with high predictive value, better reflecting patients’ blood pressure levels and fluctuations, and closely related to target organ damage indicators such as left ventricular hypertrophy, facilitating the detection of nocturnal hypertension and covert hypertension; however, it is more expensive, time-consuming and requires special computer software assistance, and reliable thresholds for diagnosing hypertension and criteria for lowering blood pressure need further exploration. HBPM is not affected by patient stress and avoids white-coat hypertension, but has the disadvantages of an irregular detection method, low accuracy, and inability to obtain nocturnal hypertension. Overall, OBPM dominates the diagnosis of hypertension, but with the intensive research and widespread use of ABPM and HBPM, the status of OBPM has declined and diversified blood pressure measurement methods will play a crucial role in blood pressure diagnosis and management.29 However, only a few of the papers included in this paper clarify the specific measurement of blood pressure values, and according to the descriptions, there is no agreement on the measurement methods and the data are subject to error, which may bias the final conclusions. In the most recent study, different blood pressure measurement modalities yielded different conclusions regarding the specific clinical efficacy of acupuncture in improving hypertension: OBPM, daytime ABPM, and SBP measured by a 6-week acupuncture cycle were significantly reduced and persisted for at least the first 2 months after completion, whereas DBP values detected by nighttime ABPM did not appear to change as a result of acupuncture treatment.30
In addition, acupuncture points, practitioner’s technique, duration of acupuncture, and frequency of treatment in acupuncture treatment affect the outcome of treatment, and only half of the included literature specifically described acupuncture manipulation. The included studies could not be quantitatively fused as each outcome indicator was not standardised; and reporting of final scores on evaluation scales such as PRISMA2020, AMSTAR2, GRADE and ROBIS is highly subjective, and multiple scores can be subjective; thus creating bias. Due to language limitations, only literature published in Chinese and English was included in this study, and the authors of the three English-language publications included were Chinese. Korean and Japanese databases, which also have a strong background in TCM research, were not searched, and the search process could not actually be carried out manually, so there was some selective bias.
Outlook
EH is an important risk factor for cardiovascular disease, which can cause impairment or even failure of the heart, brain, kidney and other organs. However, there is a lack of observations and evidence on endpoint events in acupuncture for EH. Therefore, to confirm the efficacy of acupuncture for EH, it is recommended that future clinical trials should focus on endpoint events such as long-term cardiovascular and cerebrovascular events and target organ damage, in addition to routine observations of blood pressure values.
The current study found that there are few health economics studies related to acupuncture for EH, which lack a standardized body of evidence to provide guidance for evidence-based clinical practice of acupuncture. At present, there are more standardized research methods for health economics, and it is possible to draw on related methodologies to establish a system of economic evaluation methods for acupuncture clinical practice, which will be more conducive to the development of acupuncture clinical practice.
The treatment strategy for EH is still based on daily regulation combined with antihypertensive drugs, but due to drug resistance, drug side effects, et., there is also an increasing clinical interest in TCM, especially acupuncture, for the treatment of EH. This systematic overview also demonstrates that acupuncture for EH is a promising treatment modality, although the quality of reporting, methodological quality, quality of evidence and bias of the included studies are low, but it can be recommended that future investigators adopt uniform clinical reporting standards (CONSORT), and reporting standards for interventions (STRICTA2010), in order to improve the feasibility of clinical trials. A detailed description of the specific acupuncture operations (acupuncture points, needle specifications, doctor’s technique, whether qi is obtained, duration of needle retention, frequency of acupuncture, etc.) should also be given; the selection of acupuncture points should follow the results of the patient’s TCM diagnosis and treatment, and the selection of main acupuncture points and points should be standardised; blood pressure measurement methods should also be standardised in order to achieve a final quantitative score.
Conclusions
Acupuncture currently has some benefit in the treatment of EH, although the research is of poor quality. The quality of relevant literature reporting, methodological quality, evidence quality, and bias are all hoped to improve.
Data Sharing Statement
The data supporting this systematic review are available in the Supplementary Materials.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
First author: Mi Zhou, studying at Tianjin University of Traditional Chinese Medicine, Email: [email protected], major: Chinese Medicine Diagnosis.
Supplementary Materials
See Table S1 for the search strategy.
Funding
This study was funded by the National Key Basic Research and Development Program of China (973 Plan), Project No. 2011CB505406. Project title: Research on the method of identifying the essence and energy of the health state in Chinese medicine. Responsible person: Hongwu Wang.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Lisheng L. Hypertension chronic disease management and outlook. Chin J Hyperten. 2019;27(03):209–210.
2. Yang T, Zubcevic J. Gut-brain axis in regulation of blood pressure. Front Physiol. 2017;8:845. doi:10.3389/fphys.2017.00845
3. Fengqin X, Zonggui W. Clinical application guidelines for proprietary Chinese medicines in the treatment of essential hypertension (2021). Chin J Integr Trad Chin Western Med. 2022;2022:1–9.
4. Liu ZS, Dong M, Lin LW, Lan L. Interpretation of the Chinese guidelines for the management of hypertension in the elderly 2019. J Changchun Univ Trad Chin Med. 2020;36(05):1076–1079.
5. Yao JY, Li G. Introduction to the 2020 U.S. guidelines for the diagnosis and management of hypertension at the primary level. Chin J Hyperten. 2021;29(12):1176–1180.
6. Wang J, Xiong X, Liu W. Acupuncture for essential hypertension. Int J Cardiol. 2013;169:317–326. doi:10.1016/j.ijcard.2013.09.001
7. Grassi G, Mark A, Esler M. The sympathetic nervous system alterations in human hypertension. Circ Res. 2015;116(6):976–990. doi:10.1161/CIRCRESAHA.116.303604
8. Li M, Tjenalooi SC, Guo ZL, et al. Repetitive electroacupuncture attenuates cold-induced hypertension through enkephalin in the rostral ventral lateral medulla. Sci Rep. 2016;6:35791. doi:10.1038/srep35791
9. Chen H, Xu B, Gu YH, et al. Current status of clinical research on acupuncture under the guidance of evidence-based medicine model. J Nanjing Univ Trad Chin Med. 2012;28(1):95–97.
10. Xiaodong T, Yujing P, Wenbo J, Hao C. Re-evaluation of systematic evaluation of acupuncture for the treatment of essential hypertension. Chin J Evid Based Cardiovasc Med. 2018;10(07):794–799.
11. Zhao XF, Hu HT, Li JS, et al. Is acupuncture effective for hypertension? A systematic review and meta-analysis. PLoS One. 2015;10(7). doi:10.1371/journal.pone.0127019
12. Chen H, Shen FE, Tan XD, Jiang WB, Gu YH. Efficacy and safety of acupuncture for essential hypertension: a meta-analysis. Med Sci Monit. 2018;24:2946–2969. doi:10.12659/MSM.909995
13. Zhao R, Fu LX, Xiong J, et al. Systematic evaluation of the long-term efficacy of acupuncture in the treatment of essential hypertension. Acupunct Clin J. 2011;27(3):46–51.
14. Liu FS, Guo CQ, Jin XF. Meta-analysis of a randomized controlled trial of acupuncture for mild and moderate essential hypertension. Chin J Basic Chin Med. 2012;18(4):421–423.
15. Zhang LL, Kang H, Yang BY, et al. Analysis of the efficacy and frequency of acupuncture points in the treatment of essential hypertension. Liaoning J Trad Chin Med. 2013;40(10):2115–2119.
16. Yanjun Z, Zhenjie L, Yang G, et al. Meta-analysis of the efficacy of combined acupuncture and acupuncture-drug treatment for mild and moderate essential hypertension. Liaoning J Trad Chin Med. 2014;41(9):1802–1806.
17. Chen YY, Jingbo Z, Tao S, et al. Meta-analysis of clinical efficacy of acupuncture at Renying acupoint as the main treatment for essential hypertension. New Chin Med. 2017;49(1):184–188.
18. Zhang L, Xiantao Z, Guoxiang T, et al. Meta-analysis of the effect of acupuncture compared with taking antihypertensive drugs in the treatment of essential hypertension. Chin J Evid Based Cardiovasc Med. 2017;9(12):1420–1426.
19. Lei Z, Xiantao Z, Huamin Z, et al. Systematic evaluation of acupuncture combined with lifestyle modification intervention for essential hypertension. Chin J Trad Chin Med Inform. 2018;25(6):99–103.
20. Zhu T, Ding L. Meta-analysis of acupuncture at Fengchi and Quchi points for the treatment of essential hypertension. Clin J Trad Chin Med. 2018;30(03):461–465.
21. Gao Y, Liu M, Yang KL, et al. Systematic evaluation reporting specifications: a comparative analysis and example interpretation of PRISMA 2020 and PRISMA 2009. Chin J Evid Based Med. 2021;21(05):606–616.
22. Fangyuan Z, Aomei S, Xiantao Z, Wanmin Q, Yinhui J. Interpretation of AMSTAR 2, a systematic evaluation methodological quality assessment tool. Chin J Evid Based Cardiovasc Med. 2018;10(01):14–18.
23. Wang YF, He Shao R. A new literature evaluation system--GRADE evaluation system. Evid Based Med. 2018;18(05):309–315.
24. Qiongfang W, Hongfan D, Wei D, et al. ROBIS: a new tool to assess the risk of bias in systematic evaluation. Chin J Evid Based Med. 2015;15(12):1454–1457.
25. Moher D, Weeks L, Ocampo M, et al. Describing reporting guidelines for health research: a systematic review. J Clin Epidemiol. 2011;64(7):718–742. doi:10.1016/j.jclinepi.2010.09.013
26. Li M, Niu J, Yan P, et al. The effectiveness and safety of acupuncture for depression: an overview of meta-analyses. Complement TherMed. 2020;50:102202. doi:10.1016/j.ctim.2019.102202
27. Chun L, Li X, Feng Z, Xie Y, Li J, Role of acupuncture in the treatment of COPD: an overview of systematic reviews. Int J Gen Med. 2021;14:1079–1092. doi:10.2147/IJGM.S300270
28. Xu C, Furuya-Kanamori L, Kwong JSW, Li S, Liu Y, Doi SA, Doi SA. Methodological issues of systematic reviews and meta-analyses in the Methodological issues of systematic reviews and meta-analyses in the field of sleep medicine: a meta-epidemiological study. Sleep Med Rev. 2021;57:101434. doi:10.1016/j.smrv.2021.101434
29. Liu LS, Wu ZS, Wang JG, et al. Chinese guidelines for the prevention and treatment of hypertension 2018 revised edition. Cardiovasc Dis Control. 2019;19(1):1–44.
30. Migliarese C, Maloberti A, Gatto R, Algeri M, Scarpellini S, Giannattasio C. Acupuncture in arterial hypertension: evaluation of its efficacy with both office and ambulatory blood pressure measurements. High Blood Press Cardiovasc Prev. 2022;29(5):429–434. doi:10.1007/s40292-022-00530-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.