")
Back to Journals » Vascular Health and Risk Management » Volume 19
Anatomical Distribution Patterns of Peripheral Arterial Disease in the Upper Extremities According to Patient Characteristics: A Retrospective Cohort Study
Authors Al-Sharydah AM , AlZahrani KS, Alghanimi IA, AlAnazi MM, AlHarbi RE
Received 10 October 2023
Accepted for publication 21 December 2023
Published 29 December 2023 Volume 2023:19 Pages 871—883
DOI https://doi.org/10.2147/VHRM.S440408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Abdulaziz Mohammad Al-Sharydah,1 Khaled Saud AlZahrani,2 Ibrahim Abobaker Alghanimi,1 Maha Mukhlef AlAnazi,1 Razan Essam AlHarbi1
1Diagnostic and Interventional Radiology Department, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Al Khobar City, Eastern Province, Saudi Arabia; 2Radiology Department, King Fahad General Hospital-Jeddah, Ministry of Health, Al Andalus, Jeddah, 23325, Saudi Arabia
Correspondence: Abdulaziz Mohammad Al-Sharydah, Assistant Professor and Consultant of Radiology; Imam Abdulrahman Bin Faisal University, Diagnostic and Interventional Radiology Department, King Fahd Hospital of the University, P.O. BOX: 4398 (31952), Khobar City, Eastern Province, Saudi Arabia, Email [email protected]
Purpose: Peripheral arterial disease (PAD) greatly affects the patients’ quality of life. We aimed to investigate the affected anatomical sites and distribution patterns in upper extremity PAD using computed tomography angiography (CTA). Furthermore, we sought to identify the correlations between patient characteristics and the identified patterns.
Patients and Methods: This was a retrospective chart review of upper limb CTA findings from patients with symptomatic PAD aged > 18 years. Significant variables from univariate logistic regression analysis were further tested using multivariate logistic regression analysis. Statistical significance was set at p < 0.05, with confidence intervals of 95%.
Results: The mean age of the 102 included patients with upper extremity PAD was 55.45 years. Laterality analysis revealed that the upper left limb segments were more affected than the upper right limb segments (42 vs 63; left-to-right ratio, 3:2). The forearm was the segment most affected by stenotic PAD (62 segments, 3.37%). The arm was the segment most affected by occlusive PAD (14 segments, 0.76%). Diabetes mellitus (DM) and hypertension (HTN) were significant predictors of PAD (p = 0.046). In patients with DM, the occlusive form of PAD was dominant in the arm (18.18%); however, the stenotic form prevailed in the forearm (72.72%). In patients with HTN, the occlusive form of PAD was predominant in the arm (45.45%); however, the stenotic form tended to occur in the arm and forearm (90.90%).
Conclusion: The distribution patterns of upper extremity PAD are linked to its underlying pathophysiology. HTN and DM are the most frequent comorbidities in patients with upper extremity PAD. Angiographically, PAD in these patients is likely to present as stenosis rather than as occlusion. This is vital for interventionists who deviate from radial arterial access in patients with PAD. Therefore, targeted screening standards are required, and further studies on PAD are warranted.
Plain Language Summary: In this study, we focused on discovering the link between site selectivity in upper extremity peripheral arterial disease (PAD) and the associated risk factors. This is one of the few studies, particularly from Saudi Arabia, that has provided the best available evidence on the topographical distribution patterns of PAD in the upper extremities according to variable heritable patient characteristics and associated comorbidities. Among the segments studied, the upper left limb segments were the most affected by PAD. Existing evidence indicates that angiographically, (whether with cross-sectional imaging or catheterized contrast-enhanced fluoroscopy imaging), PAD in patients with hypertension and in those with diabetes mellitus is probably observed as stenosis rather than as occlusion. Hypertension and diabetes mellitus were identified as the independent predictors of PAD in the arms and forearms, respectively. This is an important finding for interventionalists who opt for upper extremity access (eg, radial artery access) in patients with upper extremity PAD. To prevent complications, particularly upper limb amputation, screening procedures for and early detection of PAD require the identification of its distribution patterns.
Keywords: angiography, computed tomography, diabetes mellitus, hypertension, stenosis
Introduction
Peripheral arterial disease (PAD) includes various noncoronary arterial syndromes wherein the blood flow to the head, visceral organs, and limbs is restricted. Atherosclerosis is the most common disease of the aorta and its ramified arteries.1,2 PAD is considered chronic when it progresses to an advanced atherosclerotic form. It has several peripheral clinical presentations, including intermittent claudication, resting pain, ischemic ulcers, gangrene, and functional impairment.3,4
The limb-related manifestations of PAD are devastating. Furthermore, PAD can often manifest in any component of the vascular system, such as the cerebrovascular system (manifesting as ischemic stroke) and coronary arteries (manifesting as myocardial infarction).5–8 The quality of life of patients with PAD, particularly in terms of cardiovascular morbidity and mortality, may be significantly impaired.3,4,9,10
Large-artery atherosclerosis is the primary cause of lower extremity ischemia, whereas small-artery occlusive disease of the palmar and digital arteries remains the primary cause of upper extremity ischemia. PAD is a “silent” disease that manifests in only 5% of the patients with ischemic upper extremities.1,2,11
The prevalence of PAD varies according to the ethnicity and geographic location, with a higher prevalence reported in Australian, African-American, and Hispanic populations.12,13 Between 2000 and 2010, the global prevalence of PAD increased by 5% (approximately 200 million patients).14 The increase in prevalence was more commonly observed in low- and middle-income countries than in high-income countries, with the highest prevalence observed in the Southeast Asian and Western Pacific regions.14–16
Tobacco use, diabetes mellitus (DM), aging, dyslipidemia, hypertension (HTN), obesity, and chronic kidney disease (CKD) are risk factors for PAD.12,17,18 A single-center study found that HTN, DM, and obesity were the most prevalent risk factors for PAD in patients from Jeddah (Saudi Arabia).17
The 2017 European Society of Cardiology Guidelines on the diagnosis and treatment of patients with PAD recommend computed tomography angiography (CTA) and magnetic resonance angiography as the imaging modalities for assessing the structural morphology and perfusion in the regions affected by PAD.19 The effectiveness of these tools lies in their ability to both distinguish between anterograde and retrograde perfusion and estimate stenosis severity.19 Nonetheless, digital subtraction angiography remains the imaging modality of choice and is primarily used in conjunction with endovascular therapy.19
Risk factor control and the best medical therapy were initially advocated for controlling symptomatic upper extremity PAD and reducing its pertinent risks.18,19 Revascularization is recommended for significant stenosis or occlusion; it can be achieved through both open surgery and endovascular procedures. Treatment decisions should always be made in consultation with a healthcare provider and should take into consideration each patient’s individual condition.20–23
To the best of our knowledge, no studies have investigated the patterns of PAD in the upper extremities, the circulation in the upper extremity segments affected by PAD, and how specific factors affect the degree of disease severity and the extent of the affected area.
The primary purpose of this cohort study was to provide the best available evidence on the topographical distribution patterns of PAD in the upper extremities in terms of the variable heritable patient characteristics and associated comorbidities. An improved understanding of the underlying clinical relationships could considerably improve screening protocols, thereby leading to early disease detection, chronicity reduction, and a better understanding of the silent complications of PAD in the upper extremities. This in turn could allow practitioners to save diseased upper limbs from unnecessary amputation.
Materials and Methods
This study was performed in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” guidelines for cohort studies.
Study Setting and Design
This retrospective chart review was performed at the Radiology Department of the King Fahd Hospital of the University (KFHU; Khobar City, Saudi Arabia) between January 2015 and January 2021. KFHU is one of the largest academic hospitals in Al Khobar City (Eastern Province of Saudi Arabia), and its Radiology Department has been operational since 1981.
Study Population and Participants
The sample size was determined using G*Power v3.1.9.7. (RRID: SCR_013726, available at http://www.gpower.hhu.de/) to ensure sufficient statistical power (1–β = 0.80) and to prioritize outcomes based on parameters for independent means (α error: 0.05, effect size: 0.5).
The inclusion criteria were as follows: age >18 years, presentation to our health facility under an initial clinical suspicion of upper extremity PAD, and presumptive diagnosis of PAD confirmed using upper limb computed tomography (CT). The CT examinations were performed at the Radiology Department of KFHU using a commercially available 64-slice CT scanner (SOMATOM Definition AS, Siemens™, Germany).
The exclusion criteria were as follows: presence of nonatherosclerotic lesions (eg, dissection; n = 8), iatrogenic etiologies (including previous vascular interventions or presence of surgically created arteriovenous fistulas for dialysis vascular access [n = 13] and upper extremity amputations [n = 10]), age <18 years (n = 10), and poorly documented or incomplete data (n = 7). The participant selection flowchart is shown in Figure 1. Data from other imaging modalities for PAD, such as ultrasound imaging and magnetic resonance imaging, were not included owing to the study scope.
 |
Figure 1 Patient selection flowchart displays the included and excluded cases as well as the final sample size. |
Study Variables
The collected data were categorized into patient characteristics (independent variables) and segmental artery involvement patterns (dependent variables). Data on patient characteristics comprised basic demographic information (eg, age and sex) and factors suspected to be associated with PAD (eg, risk factors and metabolic comorbidities).
Data on segmental artery involvement patterns comprised the sites of the affected arterial segments (ie, the name of the artery and its segmental localization [proximal, middle, or distal]) and the severity of stenosis (mild = 30%, moderate = 30–70%, severe = 70–99%, and total occlusion = 100%). This classification system for stenosis and occlusion was derived not only from existing literature in endovascular and interventional radiology but also from a 2011 diagnostic study.24 Napoli et al graded PAD using data from a similar 64-section CT angiography machine.24 Patients with a current or previous smoking history were defined as “smokers”.
Data Collection
Vascular and interventional radiology consultants (AMA, KSZ, and IAG) reviewed the radiological findings and reported on the presence of stenotic atherosclerotic lesions. These lesions were classified according to the following three anatomical partitions after referring to the methodology of similar previous studies on lower extremity PAD.25–27
- Proximal:
Shoulder (proximal quarter): subclavian and axillary arteries.
Arm (second quarter): superficial and deep brachial arteries.
Forearm (third quarter): ulnar and radial arteries.
Hand (distal quarter): superficial and deep palmar arches and digital arteries.
Statistical Analysis
Statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Patient characteristics recorded during the first radiological examination were subjected to a descriptive analysis. Categorical variables were expressed as percentages; these were compared using the chi-square test. Continuous variables were expressed as mean ± standard deviation; these were compared using an unpaired t-test. The hypotheses were tested at a significance level of 5%.
A univariate logistic regression analysis was performed to evaluate the relationships between patient characteristics (independent variables) and the anatomical distribution patterns of PAD (dependent variables). Significant variables from the univariate analysis were entered into a parsimonious binary forward stepwise logistic regression model to identify the independent predictors of PAD distribution. Nonsignificant variables were excluded from the analysis. A multivariate logistic regression analysis was also performed to assess the correlations between PAD distribution in both upper limbs and patient characteristics. The confidence interval was set at 95%; statistical significance was determined at p <0.05.
Ethical Consideration
The Institutional Review Board of Imam Abdulrahman Bin Faisal University granted ethical approval for this study to be conducted at the King Fahd Hospital of the University (approval no.: IRB-2023-01-325).
Results
Demographics
A total of 150 patients with PAD presented to our facility during the study period. Among these, 102 patients (204 upper limbs) who presented between January 2018 and January 2023 met our eligibility criteria and were included for further analyses. Their CTA data were analyzed for PAD (Figure 1).
An average of 19 cases of upper extremity PAD were newly diagnosed annually at our hospital. The clinical characteristics of the patients are summarized in Table 1. The mean age of the patients was 55.45 ± 27.17 years (range, 28–83 years). Most patients were male (66.7%), with a male-to-female ratio of 2:1.
 |
Table 1 Most Common Clinical Presentations in the Study Population (Listed in the Descending Order of Prevalence) |
Comorbidity Analysis
No family history of PAD was observed in any case. The most prevalent comorbidities were DM and HTN, followed by hyperlipidemia and obesity (body mass index [BMI] >30 kg/m2). Data on CKD severity (based on dialysis requirement) and obesity are summarized in Figure 2. Findings on the correlations between segmental involvement and DM, HTN, hyperlipidemia, obesity (BMI >30 kg/m2), CKD (dialysis or no dialysis), connective tissue disease, ischemic heart disease, smoking status, and family history are summarized in Table 2.
 |
Table 2 Patient Characteristics According to the Segments Affected by Peripheral Arterial Disease |
 |
Figure 2 Prevalence and severity of chronic kidney disease (a) and obesity (b) in patients with upper extremity peripheral arterial disease. |
In patients with DM, the occlusive form of PAD prevailed in the second quarter (ie, the arm; four segments [18.18%]); this indicated a trend towards the involvement of the intermediate part. However, the stenotic form of PAD prevailed in the third quarter (ie, the forearm; 16 segments [72.72%]). Thus, both the ulnar and radial arteries were evenly involved in patients with DM (eight segments [36.36%]; Figure 3).
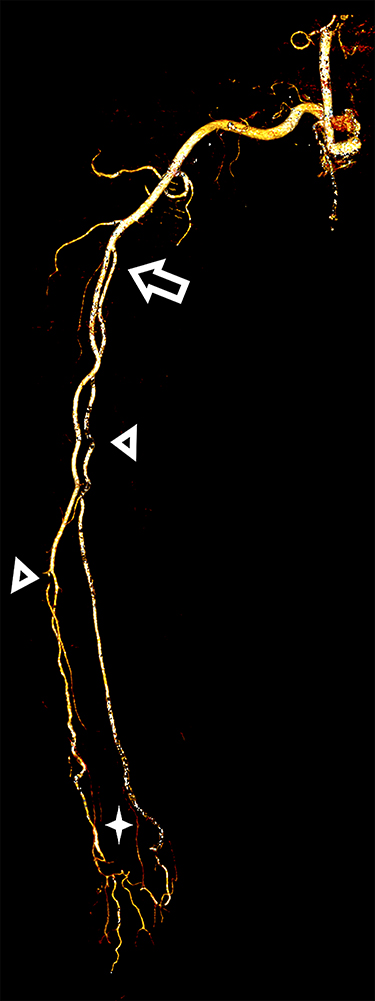 |
Figure 3 Radiological image from a 47-year-old man with type 2 diabetes mellitus and upper extremity peripheral arterial disease. Three-dimensional, reformatted, volume-rendered computed tomography angiography image shows the high origin of the brachioradial branch (arrow), which represents a higher bifurcation point of the brachial artery. The atherosclerotic and multifocal atherosclerotic segments (arrowheads), leading to attenuated hypoperfusion of the palmar arcs (asterisks), are observed. |
In patients with HTN, the occlusive form of PAD was prevalent in the second quarter (ie, the arm; 10 segments [45.45%]); this indicated a trend towards the involvement of the intermediate part. The stenotic form of PAD also tended to occur in the intermediate part in these patients (20 segments [90.90%]). The brachial artery was the most involved artery in PAD in patients with HTN (10 segments [45.45%]; Figure 4). The upper limb PAD profile, severity, and sites of arterial involvement in patients with DM and in those with HTN are summarized in Table 3.
 |
Table 3 Characterization of the Distribution Pattern and Severity of Peripheral Arterial Disease Involvement in Patients with Diabetes Mellitus and in Those with Hypertension |
 |
Figure 4 Radiological images from a 45-year-old man with hypertension and upper extremity peripheral arterial disease. The patient reported that the right upper limb felt cold and pained for a week prior to presentation. Upon examination, the radial pulse was absent. (a) A three-dimensional, reformatted, volume-rendered computed tomography angiography (CTA) image acquired from the same patient, with the left arm abducted and externally rotated, shows atherosclerotic changes (arrowheads) with an abrupt cut in the distal part of the brachial artery just before the antecubital fossa (arrow). (b and c) Catheter-directed angiogram confirms the CTA findings of an occluded brachial artery (arrowheads). (d) Further characterization of the distal reconstitution of the radial artery by small collaterals. (e) The thrombus is crossed successfully. (f) The interventionalist used catheter-directed thrombolysis to lyse the thrombus and prevent a distal embolic shower through endovascular manipulation. (g) Final angiographic examination reveals restored flow in the upper right extremities; the patient’s symptoms resolved subsequently. However, a partial filling defect (indicating residual thrombosis) is seen to have persisted in the brachial artery (arrow); this required a more conservative management. |
Laterality and Pattern Analyses
Compared with the upper right limb segments, the upper left limb segments were more affected by PAD (42 vs 63 diseased segments); the left-to-right upper extremity involvement ratio was 3:2. Compared with the subclavian artery in the left shoulder, the subclavian artery in the right shoulder was more affected by PAD (four vs eight segments); conversely, the remaining upper limb arterial segments (ie, the axillary, brachial, deep brachial, radial, ulnar, superficial, deep palmar, and digital arteries) on the left side were more affected by PAD than were those on the right side.
The stenotic form of PAD was the most common among all patients (62 segments). Furthermore, the forearm (arterial segments in the third quarter) was the most affected by PAD in all patients, followed by the arm (58 segments [3.15%]). However, the arm was the most affected in terms of the occlusive form of the disease (14 segments), followed by the forearm (one segment). Tables 2 provides a detailed summary of these findings.
Analysis of PAD Predictors
Univariate logistic regression analysis revealed DM and HTN as the significant predictors of PAD according to the anatomical arterial segments involved (p = 0.046 for both). Furthermore, multivariate logistic regression analysis revealed that DM and HTN were the independent predictors of total occlusion in the intermediate part of the upper extremities. In patients with DM, the forearm was particularly affected (radial artery: odds ratio [OR] = 3.053, 95% confidence interval [CI] = 1.313–11.710, p = 0.010). Furthermore, in patients with HTN, the arm was particularly affected (superficial brachial artery: OR = 2.419, 95% CI = 0.969–6.039, p = 0.041; deep brachial artery: OR = 4.063, 95% CI = 1.393–11.850, p = 0.020; Table 4).
 |
Table 4 Independent Predictors of Total Occlusion Secondary to Peripheral Arterial Disease (PAD) from Among the Patient Characteristics Correlated with Disease Distributiona |
Discussion
This study is a continuum sub-study of another observational cohort study conducted by Alghanimi et al on lower extremity involvement and anatomical distribution of PAD with different comorbidities in the Saudi population (2023).25 The present study focused on elucidating the relationship between anatomical sites or distribution patterns in upper extremity PAD and the associated risk factors and comorbidities.
Our findings are consistent with existing literature in that most of our patients with upper extremity PAD were male (male-to-female ratio: 2:1).28 This can be explained by the fact that women have higher levels of estrogen and progesterone than do men. Estrogen plays a protective role against PAD by improving the breakdown of low-density lipoproteins and cholesterol; furthermore, the elevated progesterone levels are thought to play an anti-atherosclerotic role, both directly in the blood vessel walls and indirectly through antioxidant activity.28
Interestingly, Pham et al studied the upper extremity vasculature using ultrasound mapping and found that the mean diameters of the brachial artery in the elbow and the radial artery in the wrist were significantly higher in men than in women.28 Thus, we speculate that the incidence of upper extremity PAD in women may have been underestimated and may actually be higher than that in men. Further studies must investigate the true incidence of PAD in women; in the interim, women should be made aware of their risk of developing the disease.28–30
Regarding the laterality of disease involvement, our study found that the left upper extremity vessels were generally the sites most affected by PAD (left-to-right ratio, 3:2); this is consistent with the findings of a previous analysis of the Proximal Upper Limb Artery Registry (2021).31 We hypothesize that having a slightly lower blood pressure and vessels of a longer course32–34 contributes to the accumulation of immune cells and uptake of circulating oxidized lipoproteins, which lead to the foundation for atheroma and fibroatheroma formation in PAD.32,35 However, further research is required to validate this hypothesis.
Our study also revealed that the subclavian artery in the right shoulder is more affected than the corresponding artery in the left shoulder. The remaining arterial segments in the upper extremities (ie, the axillary, brachial, deep brachial, radial, ulnar, superficial and deep palmar, and digital arteries) were more affected on the left side than on the right side; this may be attributed to anatomical reasons.
The left subclavian artery is relatively long with a larger diameter at its aortic origin; the diameter progressively narrows distally. Conversely, the right subclavian artery has a shorter length, a smaller vascular diameter at its origin, and a slightly larger diameter at its distal end. This may explain the higher incidence of PAD in the proximal right subclavian artery than in the proximal left subclavian artery.31–36
Our study revealed that HTN and DM were significant risk factors for PAD, whereas tobacco use, aging, dyslipidemia, obesity, and CKD were not (Table 2). In patients with DM, the intermediate part was the site most involved in upper extremity PAD; this is consistent with the observation made by Alghanimi et al that the femoropopliteal segment is the site most involved in PAD in patients with DM.25 The present study found that PAD coexisting with HTN and DM likely manifests in a stenotic form rather than as an occlusive disease.
In patients with HTN, the intermediate part was the site most affected by PAD as well. In these patients, the total occlusion form of PAD was more likely to affect the brachial artery segments, as in patients with DM. However, unlike the superficial brachial artery, the deep brachial artery was more frequently involved in patients with HTN than in those with DM (Table 3).
Based on current evidence, we strongly recommend the use of ultrasound guidance to obtain vascular access because of multiple complications related to the access site. In 2022, Levin et al reported that for endovascular interventions, radial artery access was associated with a lower rate of postoperative complications than were other access points.37 In 2021, Nardai et al reported that performing interventions targeting the upper extremities under ultrasound guidance using a distal radial approach was safe.31 Therefore, ultrasound imaging (instead of pulse palpation) is essential for obtaining endovascular access, particularly in diseased vessels.
In 2019, Jahic et al reported that the technical success rates of percutaneous endovascular procedures were higher in patients with the stenotic form of PAD than in those with the occlusive form of PAD.38 Our findings support this: the forearm segments were the most affected in all patients with the stenotic form of PAD.
We believe that the findings of the present study have considerable relevance in clinical practice because they allow us to advocate for the use of ultrasound guidance to safely obtain arterial access in ipsilateral and contralateral upper extremities during interventional procedures tailored to individual patient characteristics and the affected anatomical regions.31,38 Finally, recent evidence suggests that obtaining arterial access through a distal radial or snuff box is a safe and feasible technique with a more tolerable experience for patients (including pediatric patients).39,40
Strengths and Limitations
Our study is one of the few Saudi Arabian studies on the anatomical distribution patterns of PAD and their correlation with risk factors and comorbidities. However, this study has certain limitations. First, because of its retrospective design, it was subject to substantial observer bias, which may have contributed to the underestimation of some clinical data due to the inaccurate reporting of medical histories. Another possible source of bias is the nature of our study population, which was relatively small and included patients from a single academic care center.
Recommendations for Future Studies
Confirming the effects of risk factors on the anatomical distribution of atherosclerosis can enable the development of targeted screening guidelines for the early detection of PAD and prevention of adverse outcomes (such as limb amputation). Given the substantial cardiovascular comorbidity associated with PAD, identifying patients at the highest risk of cardiovascular events is pivotal for preventing such events.41 The authors suggest performing a prospective screening study using Doppler ultrasound for the positive diagnosis of PAD while collecting more data on the associated risk factors. Furthermore, randomized controlled interventional trials on the treatment of PAD in patients with highly calcified vessels are required to obtain further insights into this condition. Regular screening of the upper extremity vessels in patients with DM is also recommended.
Conclusion
This cohort study enabled us to distinguish among the various patterns of upper extremity PAD. Men, in whom the anti-atherosclerotic roles of estrogen and progesterone are absent, are more likely to be affected by PAD (with a predilection for the left upper extremities). Our findings also suggest a link between the underlying pathophysiology of this disease and certain patient characteristics in terms of the disease distribution patterns. HTN and DM were the most prevalent comorbidities in patients with upper extremity PAD. Angiographically, whether with cross-sectional imaging or with catheterized contrast-enhanced fluoroscopy imaging, PAD in patients with HTN and DM is probably observed as stenosis rather than as occlusion. HTN and DM were identified as independent predictors of PAD in the arms and forearms, respectively. This is an important finding for interventionalists who opt for upper extremity access (eg, radial artery access) in patients with upper extremity PAD. The methodology of the current study and the concepts discussed herein may pioneer future multicenter studies with larger sample sizes.
Abbreviations
BMI, body mass index; CI, confidence interval; CKD, chronic kidney disease; CT, computed tomography; CTA, computed tomography angiography; DM, diabetes mellitus; HTN, hypertension; OR, odds ratio.
Data Sharing Statement
Data supporting the results reported in the manuscript are not publicly available because of institutional restrictions (eg, patient privacy policies). However, anonymized unpublished data are available from the principal investigator and the corresponding author (A.M.A.; [email protected]) upon reasonable request.
Ethics Approval and Informed Consent
The non-experimental study protocol was approved by the Imam Abdulrahman Bin Faisal University licensing committee of the Institutional Review Board (approval no.: IRB-2023-01-325), who further granted approval for the study to be conducted at the King Fahd Hospital of the University. Informed consent was obtained from all the participants and/or their legal guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FGR.; for TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45:S5–S67. doi:10.1016/j.jvs.2006.12.037
2. Ross R. Cellular and molecular studies of atherogenesis. Atherosclerosis. 1997;131:S3–S4. doi:10.1016/s0021-9150(97)06114-5
3. Singh TP, Moxon JV, Healy GN, Cadet-James Y, Golledge J. Presentation and outcomes of indigenous Australians with peripheral artery disease. BMC Cardiovasc Disord. 2018;18:94. doi:10.1186/s12872-018-0835-z
4. Jones WS, Patel MR, Dai D, et al. High mortality risks after major lower extremity amputation in medicare patients with peripheral artery disease. Am Heart J. 2013;165:809–815.e1. doi:10.1016/j.ahj.2012.12.002
5. Murabito JM, Evans JC, Larson MG, Nieto K, Levy D, Wilson PW; for Framingham Study. The ankle-brachial index in the elderly and risk of stroke, coronary disease, and death: the Framingham study. Arch Intern Med. 2003;163:1939–1942. doi:10.1001/archinte.163.16.1939
6. Cotter G, Cannon CP, McCabe CH, et al. Prior peripheral arterial disease and cerebrovascular disease are independent predictors of adverse outcomes in patients with acute coronary syndromes: are we doing enough? Results from the Orbofiban in Patients with Unstable Coronary Syndrome Thrombolysis in Myocardial Infarction (OPUS-TIMI) 16 study. Am Heart J. 2003;145:622–627. doi:10.1067/mhj.2003.6
7. Golomb BA, Dang TT, Criqui MH. Peripheral arterial disease morbidity and mortality implications. Circulation. 2006;114:688–699. doi:10.1161/CIRCULATIONAHA.105.593442
8. Marrett E, DiBonaventura M, Zhang Q. Burden of peripheral arterial disease in Europe and the United States: a patient survey. Health Qual Life Outcomes. 2013;11:175. doi:10.1186/1477-7525-11-175
9. Ohman EM, Bhatt DL, Steg PG, et al. The Reduction of Atherothrombosis for Continued Health (REACH) Registry: an international, prospective, observational investigation in subjects at risk for atherothrombotic events study design. Am Heart J. 2006;151:786.e1–786.10. doi:10.1016/j.ahj.2005.11.004
10. Fowkes FG, Murray GD, Butcher I, et al. Ankle brachial index combined with Framingham risk score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300:197–208. doi:10.1001/jama.300.2.197
11. Porter JM, Taylor LM. Limb ischemia caused by small artery disease. World J Surg. 1983;7(3):326–333. doi:10.1007/BF01658080
12. Fowkes FGR, Aboyans V, Fowkes FJ, McDermott MM, Sampson UK, Criqui MH. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol. 2017;14:156–170. doi:10.1038/nrcardio.2016.179
13. Narula N, Olin JW, Narula N. Pathologic disparities between peripheral artery disease and coronary artery disease. Arterioscler Thromb Vasc Biol. 2020;40:1982–1989. doi:10.1161/ATVBAHA.119.312864
14. Peach G, Griffin M, Jones KG, Thompson MM, Hinchliffe RJ. Diagnosis and management of peripheral arterial disease. BMJ. 2012;
15. Song P, Rudan D, Zhu Y, et al. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019;7:e1020–e1030–e30. doi:10.1016/S2214-109X(19)30255-4
16. Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116:1509–1526. doi:10.1161/CIRCRESAHA.116.303849
17. Mufti Alsadiqi AI, Subki AH, Abushanab RH, et al. Peripheral artery disease risk factors in Jeddah, Saudi Arabia: a retrospective study. Int J Gen Med. 2019;12:49–54. doi:10.2147/IJGM.S176451
18. Al-Sheikh SO, Aljabri BA, Al-Ansary LA, Al-Khayal LA, Al-Salman MM, Al-Omran MA. Prevalence of and risk factors for peripheral arterial disease in Saudi Arabia. A pilot cross-sectional study. Saudi Med J. 2007;28:412–414.
19. Halliday A, Bax JJ. ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55:301–302. doi:10.1093/eurheartj/ehx095
20. Aboyans V, Criqui MH, McDermott MM, et al. The vital prognosis of subclavian stenosis. J Am Coll Cardiol. 2007;49:1540–1545. doi:10.1016/j.jacc.2006.09.055
21. Klitfod L, Jensen LP. Treatment of chronic upper limb ischaemia is safe and results are good. Dan Med J. 2014;61:A4859.
22. Daniel VT, Madenci AL, Nguyen LL, et al. Contemporary comparison of supra aortic trunk surgical reconstructions for occlusive disease. J Vasc Surg. 2014;59:1577–1582.e2. doi:10.1016/j.jvs.2013.12.017
23. Duran M, Grotemeyer D, Danch MA, Grabitz K, Schelzig H, Sagban TA. Subclavian carotid transposition: immediate and long-term outcomes of 126 surgical reconstructions. Ann Vasc Surg. 2015;29:397–403. doi:10.1016/j.avsg.2014.09.030
24. Napoli A, Anzidei M, Zaccagna F, et al. Peripheral arterial occlusive disease: diagnostic performance and effect on therapeutic management of 64-section CT angiography. Radiology. 2011;261:976–986.
25. Alghanimi IA, Al-Sharydah AM, Alqutub AA, et al. Anatomical distribution patterns of peripheral arterial disease according to patient characteristics: a unicentral cohort study. Vasc Health Risk Manag. 2023;19:447–457. doi:10.2147/VHRM.S416967
26. Haltmayer M, Mueller T, Horvath W, Luft C, Poelz W, Haidinger D. Impact of atherosclerotic risk factors on the an atomical distribution of peripheral arterial disease. Int Angiol. 2001;20:200–207.
27. Diehm N, Shang A, Silvestro A, et al. Association of cardiovascular risk factors with pattern of lower limb atherosclerosis in 2659 patients undergoing angioplasty. Eur J Vasc Endovas Surg. 2006;31:59–63. doi:10.1016/j.ejvs.2005.09.006
28. Pham XD, Kim JJ, Parrish AB, et al. Racial and gender differences in arterial anatomy of the arm. Am Surg. 2016;82:973–976. doi:10.1177/000313481608201025
29. Lowry D, Saeed M, Narendran P, Tiwari A. A review of distribution of atherosclerosis in the lower limb arteries of patients with diabetes mellitus and peripheral vascular disease. Vasc Endovascular Surg. 2018;52:535–542. doi:10.1177/1538574418791622
30. Golledge J. Update on the pathophysiology and medical treatment of peripheral artery disease. Nat Rev Cardiol. 2022;19:456–474. doi:10.1038/s41569-021-00663-9
31. Nardai S, Zafirovska B, Pataki Á, et al. Finding the optimal access for proximal upper limb artery (PULA) interventions: lessons learned from the PULA Multicenter Registry. Catheter Cardiovasc Interv. 2021;98:1375–1382. doi:10.1002/ccd.29967
32. Stary HC, Chandler AB, Dinsmore RE, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis: a report from the committee on vascular lesions of the council on arteriosclerosis, American Heart Association. Circulation. 1995;92(5):1355–1374.
33. Eguchi K, Yacoub M, Jhalani J, Gerin W, Schwartz JE, Pickering TG. Consistency of blood pressure differences between the left and right arms. Arch Intern Med. 2007;167(4):388–393.
34. Song BM, Kim HC, Shim JS, Kang DR. Comparison between right and left upper arms in detection of hypertension. Korean Circ J. 2019;49(3):267–277.
35. Lorey MB, Öörni K, Kovanen PT. Modified lipoproteins induce arterial wall inflammation during atherogenesis. Front Cardiovasc Med. 2022;9:841545.
36. Poonam JN, Singla RK, Sharma T. Anatomical considerations and clinical implications of subclavian artery. J Evol Med Dent Sci. 2013;2:5484–5491. doi:10.14260/jemds/1013
37. Levin SR, Carlson SJ, Farber A, et al. Percutaneous radial artery access for peripheral vascular interventions is a safe alternative for upper extremity access. J Vasc Surg. 2022;76(1):174–179.
38. Jahic E, Avdagic H, Iveljic I, Krdzalic A. Percutaneous transluminal angioplasty of subclavian artery lesions. Med Arch. 2019;73:28–31. doi:10.5455/medarh.2019.73.28-31
39. Alehaideb A, Ha W, Bickford S, et al. Can children be considered for transradial interventions? Prospective study of sonographic radial artery diameters. Circ Cardiovasc Interv. 2020;13(7):e009251. doi:10.1161/CIRCINTERVENTIONS.120.009251
40. Jiang F, Fan WL, Zheng W, Wu X, Hu H. Distal radial artery access is a safe and feasible technique in the anatomical snuffbox for visceral intervention. Medicine. 2023;102(24). doi:10.1097/MD.0000000000033987
41. Kourtidou C, Rafailidis V, Varouktsi G, et al. Evaluation of subclinical vascular disease in diabetic kidney disease: a tool for personalization of management of a high-risk population. J Pers Med. 2022;12:1139. doi:10.3390/jpm12071139
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.