")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 14
Antileishmanial Activity of Tamoxifen by Targeting Sphingolipid Metabolism: A Review
Authors Zewdie KA , Hailu HG , Ayza MA , Tesfaye BA
Received 13 October 2021
Accepted for publication 27 January 2022
Published 21 February 2022 Volume 2022:14 Pages 11—17
DOI https://doi.org/10.2147/CPAA.S344268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Kaleab Alemayehu Zewdie, Haftom Gebregergs Hailu, Muluken Altaye Ayza, Bekalu Amare Tesfaye
Department of Pharmacology and Toxicology, School of Pharmacy, Mekelle University, Mekelle, Ethiopia
Correspondence: Kaleab Alemayehu Zewdie, Department of Pharmacology and Toxicology, School of Pharmacy, Mekelle University, PO Box 1871, Mekelle, Ethiopia, Tel +251 921546562, Email [email protected]
Abstract: Leishmaniasis is a widespread group of neglected parasitic diseases caused by protozoa of the genus Leishmania. Around 2 million new cases are reported each year and around 12 million people are at risk of being infected. Although various therapies have been used to treat leishmaniasis, they have been associated with increased cytotoxicity and drug resistance problems. Hence, the present review was intended to show the potential of tamoxifen as an alternative option for the treatment of leishmaniasis. Tamoxifen is a known selective estrogen receptor modulator and has been widely used for the treatment of early-stage breast cancer. Various experimental and clinical studies revealed that it has an antileishmanial effect by decreasing parasitic burden, with low cost and few side effects. The antileishmanial action of tamoxifen has been related to its potential effect on sphingolipid metabolism. Besides, it affects mitochondrial function by inducing alterations in the plasma membrane potential. However, further detailed studies are required to show the ultimate effects on health outcomes.
Keywords: tamoxifen, leishmaniasis, sphingolipid metabolism, estrogen receptor modulator
Introduction
Overview of Leishmaniasis
Leishmaniasis is a widespread vector-borne parasitic disease caused by protozoan flagellates (from the genus Leishmania). It is transmitted by the bite of infected female phlebotomine sandflies.1–3 Around 1.5–2 million new cases are reported each year and about 12 million people are at risk.4 Even though leishmaniasis has the ninth largest disease burden among infectious diseases, it is largely ignored by the global health community and is documented as a neglected tropical disease.5,6 Recent reports showed that 97 countries are considered endemic for leishmaniasis, and it continues to be a major health problem in four eco-epidemiological regions of the world.6,7
Different species of Leishmania cause various clinical manifestations, ranging in severity from life-threatening visceral disease (visceral leishmaniasis) to self-curing cutaneous lesions (cutaneous leishmaniasis).8 Although treatments are available for curing leishmaniasis (including visceral leishmaniasis), most of the drugs are associated with increased cytotoxicity and augmented drug resistance.5 Therefore, drug repurposing is an attractive option for the discovery of new antileishmanial agents.9
The goal of repurposing is to expedite the drug development process by uncovering novel biological activity for existing pharmaceuticals and then employing them to treat new or existing ailments. Repurposing is a beneficial means of drug discovery since the medications have well-studied pharmacological and toxicological characteristics and are taken for an extended period.10 Hence, the goal of this study is to evaluate the potential of tamoxifen as an alternative medicine for the treatment of leishmaniasis using data from several experimental and clinical investigations.
Tamoxifen and Its Pharmacology
Tamoxifen is a selective estrogen receptor modulator (SERM) that is widely used for the treatment of early-stage breast cancer and the reduction of recurrences.11–13 It was discovered more than 40 years and remains one of the most effective therapies for the treatment of breast cancer.14 Tamoxifen belongs to the class of triphenylethylene molecules.15,16 It is a prodrug. After successive metabolic activation (mainly by CYP2D6), it is changed from pharmacologically inactive metabolites (tamoxifen and N-desmethyl) to active endoxifen, and finally results in the formation of 4-OH-tamoxifen,17 which has a high antiestrogenic potential.18 Genetic, environmental and/or drug-induced factors that change CYP2D6 enzyme activity affect the results of tamoxifen treatment. CYP2D6 comprises 2–3% of total liver CYPs and has several genetic polymorphisms.17 Based on an individual’s metabolic activity, they can be a poor metabolizer (PM, two non-functional CYP2D6 alleles), an intermediate metabolizer (IM, one functional allele or two reduced function alleles), an extensive (normal) metabolizer (EM, two functional alleles) or an ultra-rapid metabolizer (UM, duplication of functional alleles).18 Therefore, patients with PM will possibly derive less benefit from tamoxifen treatment, so dose adjustment is required. Furthermore, no variations in the incidence of adverse drug reactions were detected when the tamoxifen dose was increased, and a 40–60 mg dose of tamoxifen was generally well tolerated.17,18
SERMs have high bioavailability and are rapidly absorbed from the gastrointestinal tract. A high oral bioavailability reduces the risk of side effects and toxicity.11,12 Moreover, they are highly bound to plasma proteins (98–99%) and achieve equilibrium between the free drug and bound drug after reaching the systemic circulation. The free drug is then distributed throughout the body and reaches different parts of the body rapidly. Finally, SERMs are excreted through faeces, with small amounts in urine.19
Tamoxifen is a SERM, which binds and acts as an agonist and an antagonist with estrogen receptors (ERα or ERβ) depending on the tissue in which it acts.11,12 Normally, estrogen binds to the ER (nuclear receptor) and induces DNA synthesis and cell replication, which may lead to breast cancer.17 However, tamoxifen can treat breast cancer by competing with estrogen and preventing its binding to ERs, thereby inhibiting the growth-stimulating effect of estrogen in the breast. It can also inhibit tumour growth through other mechanisms, by regulating oncogene expression and growth factors, and inducing apoptosis.19 Besides, in recent years experimental and clinical studies have shown that tamoxifen is also active against several species of Leishmania (Trinconi et al, 2018).9
Tamoxifen and Leishmaniasis
Leishmaniasis can been treated with pentavalent antimonial meglumine antimonite, sodium stibogluconate and liposomal amphotericin B. However, the treatment is relatively expensive and usually requires additional medical supervision, such as ECG and liver function tests, owing to the side effects of the medication, such as vomiting, cardiotoxicity and hepatotoxicity.20,21 Because of differences in the effectiveness of antimonial agents against the various Leishmania species and emerging drug resistance, amphotericin B is currently recommended as first-line treatment.22,23 However, it has also side effects, including infusion reactions such as chills and fever, and serious toxicity has been reported in some patients.24 Therefore, drug repurposing is an attractive option for the discovery of newer antileishmanial drugs. Various in vivo and in vitro studies have revealed that tamoxifen is active against several species of Leishmania, with low cost and relatively few side effects.25–30
Tamoxifen is a multi-target drug interfering in sphingolipid (SL) metabolism.31 SLs are an essential component of the cell membrane of Leishmania and are important mediators of cell signalling and control several cell biological processes, such as endocytosis, cell growth, differentiation, apoptosis and oncogenesis.31–33 Inositol phosphorylceramide (IPC) is the most abundant SL in Leishmania, but is not present in mammalian cells, which is of help for selective toxicity.9,28,29 It also interacts with the parasites’ mitochondria, which results in mitochondrial dysfunction by inducing alterations in the plasma membrane potential, leading to depolarization of the membrane, with no disruption of the integrity,34 and inducing apoptosis.30,33 Reimão and Uliana (2018) showed that tamoxifen caused mitochondrial damage, with loss of membrane potential, and also led to plasma membrane depolarization without general membrane disruption or permeabilization. Therefore, the effect of tamoxifen on Leishmania is mediated, in part, by disorder in the parasite’s membranes, which triggers a series of lethal events.34
Preclinical and Clinical Studies on the Effect of Tamoxifen on Leishmaniasis
As shown in Table 1, several experimental studies have demonstrated the activity of tamoxifen against different species of Leishmania (Table 1). An in vitro study by Miguel et al (2007) showed the effectiveness of tamoxifen against several species of Leishmania: L. braziliensis, L. major, L. chagasi, L. amazonensis and L. donovani.35 In 2008, an in vivo study was conducted on L. amazonensis-infected BALB/c mice to assess the potential effect of tamoxifen in cutaneous leishmaniasis. In this study, a significant decrease in the total parasite number per lesion was observed in tamoxifen-treated groups when evaluated immediately after the interruption of treatment (7 weeks after infection) and 6 weeks later (13 weeks after infection). At the end of the experiment, the average number of parasites was reduced by at least 99.7% in treated groups, in comparison to untreated animals.26
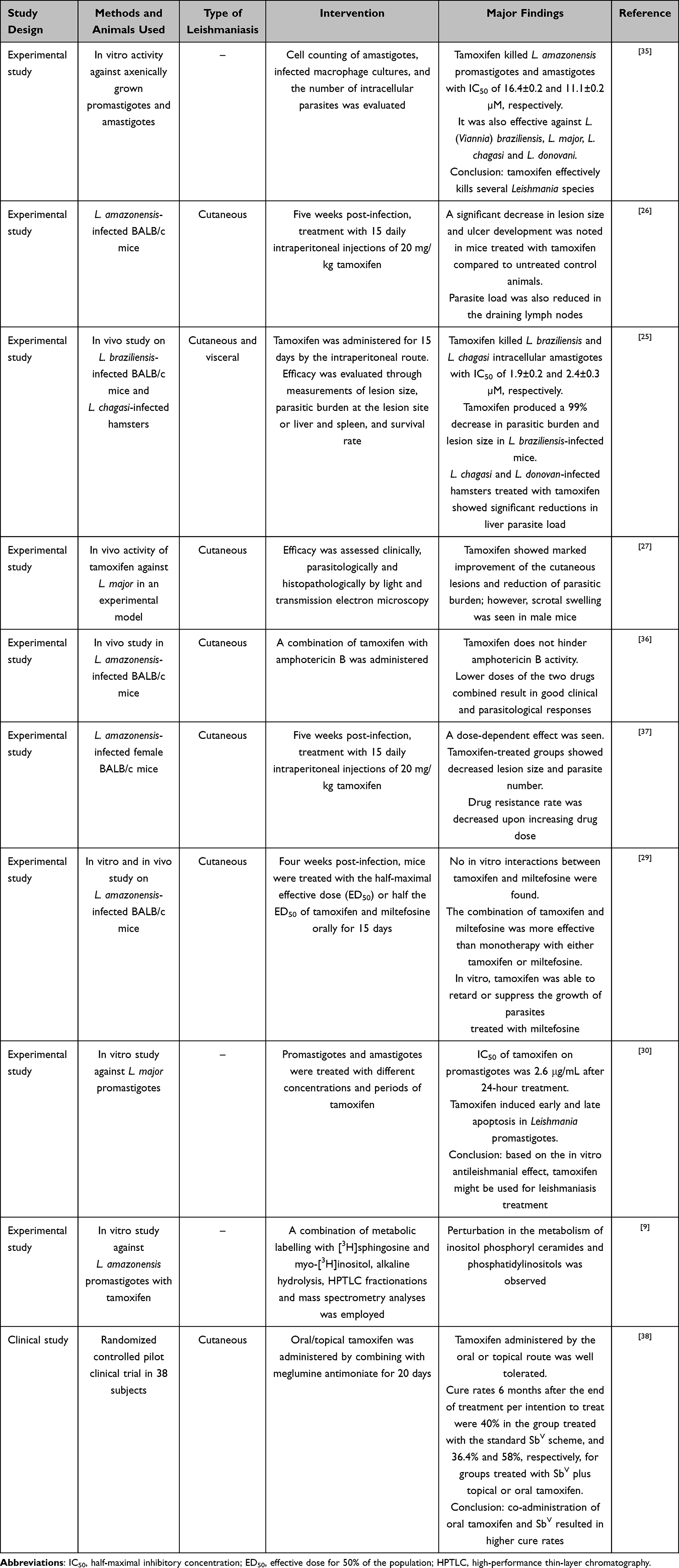 |
Table 1 Experimental Studies Revealing the Activity of Tamoxifen Against Different Species of Leishmania |
Another study, by Trinconi et al (2018), revealed that L. amazonensis promastigotes treated with tamoxifen showed a meaningful perturbation of SL metabolism, leading to the reduction of IPCs and phosphatidylinositols (PIs), and accumulation of acyl ceramide. Two hypotheses were formulated to explain the reduction of PIs and IPC levels in tamoxifen-treated parasites: 1) tamoxifen interferes with inositol and/or ceramide availability, both of which are critical elements for IPC synthesis; or 2) tamoxifen inhibits IPC and/or PI synthesis.9
An in vivo study by Coelho et al (2015) showed that Leishmania is not likely to develop tamoxifen resistance. In this study, treatment with tamoxifen was initiated after 5 weeks of infection. Intraperitoneal injections of 30.4 mg tamoxifen citrate/kg/day (equivalent to 20 mg/kg/day tamoxifen) were administered to the infected mice for 15 days. Sixty days after the end of treatment, mice were euthanized and amastigotes were purified from lesions. In this study, the resistance pattern of tamoxifen in leishmaniasis was also investigated by comparing it with miltefosine. These findings are consistent with a multi-target mode of action to explain the leishmanicidal properties of tamoxifen, and support the proposition of using tamoxifen as a partner in drug combination schemes for the treatment of leishmaniasis.37
Another study, by Abbasi et al (2015), demonstrated the in vitro antileishmanial effect of tamoxifen. Promastigotes and amastigotes were cultured and treated with various concentrations of tamoxifen after 24, 48 and 72 hours of culture. The number of parasites was 1.07×106 per mL in the control group, and the parasite numbers in the concentrations of 1 and 50 µg/mL tamoxifen were 0.95×10 and 0.06×106, respectively. The IC50 value of tamoxifen was 2.64 μg/mL.39
A study conducted by Eissa et al (2011) investigated groups of infected mice that were given tamoxifen, orally, at a dose of 20 mg/kg/day for 15 days. The results showed that tamoxifen caused a marked improvement in the cutaneous lesions and reduction of the parasitic burden. However, the untreated infected mice suffered from autoamputation of the inoculated foot pad.27 Similarly, Trinconi et al (2014) showed that the lesion size was reduced by 55% in the group assigned to low-dose combined therapy, by 25% in the 6.5 mg/kg/day tamoxifen group and by 0% in the 1.2 mg/kg/day amphotericin B group. When parasitic burdens were considered, a 75% reduction was noted in the group treated with the low-dose combined therapy and a 36% reduction in the 6.5 mg/kg/day tamoxifen group, but an increase in the 1.2 mg/kg/day amphotericin B group. So, in both cases, the effect of combined therapy was superior to the sum of effects of the individual drugs, and therefore tamoxifen and amphotericin B have additive and possibly synergistic behaviour in vivo.36
Doroodgar et al (2016) showed 2% apoptosis in the control group after 48 hours, and 59.7% apoptosis with a 50 µg/L concentration of tamoxifen. Therefore, the parasite’s growth rate was decreased by increasing the dose and duration of the drug; by increasing the concentration and duration of the drug, the viability of the promastigotes and intracellular amastigotes decreased.30
A clinical study by Machado et al (2018) involved a total of 38 subjects, of whom 23 were treated with the combination of tamoxifen and meglumine antimoniate and 15 with standard meglumine antimoniate. Of those treated with combined therapy, 12 received tamoxifen orally and 11 were treated with topical tamoxifen. Tamoxifen administered by the oral or topical route was well tolerated. After 6 months of treatment, a 40% cure rate was reported in the group treated with standard meglumine antimoniate, compared with 36.4% in the group treated with meglumine antimoniate plus topical tamoxifen and 58% in the group treated with meglumine antimoniate plus oral tamoxifen.40
In a study by Trinconi et al (2018), infected BALB/c mice were treated with tamoxifen cream as monotherapy or in combination with pentavalent antimonial. At the end of treatment, the combined scheme containing tamoxifen and pentavalent antimonial was found to be more effective in reducing lesion size and parasitic burden than monotherapy.41
Conclusion and Future Perspectives
Overall, this article provides a review of the use of tamoxifen as an alternative agent for the management of leishmaniasis. Tamoxifen has been used for the treatment of breast cancer in clinical practice. Although several agents have been used for the management of leishmaniasis, they have been associated with various detrimental effects. More recently, various clinical and animal studies have revealed that tamoxifen has antileishmanial activity. It is a selective estrogen receptor modulator with high bioavailability, low cost, high safety and a low resistance profile. Its main mechanism of action is through interfering with distinct cell pathways (sphingolipid metabolism). In addition, it causes mitochondrial dysfunction by interfering with the parasites’ mitochondria. However, more information and further detailed understanding are needed to show the ultimate effects on health outcomes.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Pace D. Leishmaniasis. J Infect. 2014;69(Suppl 1):S10–8. doi:10.1016/j.jinf.2014.07.016
2. Regina S, Soares DC, Hirata CF. Cell death mechanisms in Leishmania amazonensis triggered by methylene blue-mediated antiparasitic photodynamic therapy. Photodiagnosis Photodyn Ther. 2018. doi:10.1016/j.pdpdt.2018.05.005
3. Tabbabi A. Review of Leishmaniasis in the Middle East and North Africa. Afr Health Sci. 2019;19:1329–1337. doi:10.4314/ahs.v19i1.4
4. Celes FS, Trovatti E, Khouri R, et al. DETC-based bacterial cellulose bio-curatives for topical treatment of cutaneous leishmaniasis. Sci Rep. 2016;6:1–11. doi:10.1038/srep38330
5. Jawed J, Majumdar S. Recent Trends in Leishmania Research: a Therapeutic Perspective. J Infect. 2018;1:1–4. doi:10.29245/2689-9981/2018/3.1120
6. Ruiz-Postigo JA, Jain S, Mikhailov A, et al. Global leishmaniasis surveillance: 2019–2020, a baseline for the 2030 roadmap. Wkly Epidemiol Rec. 2021;35:401–420.
7. Moein D, Masoud D, Saeed M, Abbas D. Epidemiological Aspects of Cutaneous Leishmaniasis during 2009–2016 in Kashan City, Central Iran. Korean J Parasitol. 2018;56:21–24.
8. Burza S, Croft SL, Boelaert M. Leishmaniasis. Lancet. 2018;392(10151):951–970. doi:10.1016/S0140-6736(18)31204-2
9. Trinconi CT, Miguel DC, Silber AM, et al. Tamoxifen inhibits the biosynthesis of inositolphosphorylceramide in Leishmania. Int J Parasitol Drugs Drug Resist. 2018;8:475–487.
10. Butts A, Martin JA, DiDone L, et al. Structure-Activity Relationships for the Antifungal Activity of Selective Estrogen Receptor Antagonists Related to Tamoxifen. PLoS One. 2015;10(5):1–16. doi:10.1371/journal.pone.0125927
11. Li F, Dou J, Wei L, Li S, Liu J. The selective estrogen receptor modulators in breast cancer prevention. Cancer Chemother Pharmacol. 2016;77:895–903. doi:10.1007/s00280-016-2959-0
12. Finney CA, Shvetcov A, Westbrook RF, Morris MJ, Jones NM. The selective estrogen receptor modulator tamoxifen protects against subtle cognitive decline and early markers of injury 24 h after hippocampal silent infarct in male Sprague-Dawley rats. Horm Behav. 2021;134:105016.
13. Pickar JH, Komm BS. Selective estrogen receptor modulators and the combination therapy conjugated estrogens/bazedoxifene: a review of effects on the breast. Post Reprod Heal. 2015;21:112–121. doi:10.1177/2053369115599090
14. Weinstock A, Gallego-Delgado J, Gomes C, et al. Tamoxifen activity against Plasmodium in vitro and in mice. Malar J. 2019;18:1–7. doi:10.1186/s12936-019-3012-7
15. Fanidi A, Pageaux JF, Courion C, Fayard JM, Laugier C. Growth inhibition and the regulation of cyclic AMP by the triphenylethylene anti-estrogen tamoxifen in the quail oviduct. Biol Cell. 1991;72:181–186. doi:10.1016/0248-4900(91)90092-2
16. Borgna JL. The elucidation of the antiestrogen and antitumoral mechanisms of tamoxifen. Bull Cancer. 1994;81:29–37.
17. Shahbaz K. Tamoxifen: pharmacokinetics and Pharmacodynamics. Open Access J Pharm Res. 2017;1:1–8.
18. Del Re M, Citi V, Crucitta S, et al. Pharmacogenetics of CYP2D6 and tamoxifen therapy: light at the end of the tunnel? Pharmacol Res. 2016;107:398–406. doi:10.1016/j.phrs.2016.03.025
19. Garg A, Singh B, Sharma R, Singh A, Kumar A. Selective Estrogen Receptor Modulators (SERMs): mechanistic Insights Against Microbial Infections. Curr Mol Med. 2019;20:102–115. doi:10.2174/1566524019666191014112133
20. Monzote L. Current treatment of leishmaniasis: a review. Open Antimicrob Agents J. 2009;1:9–19.
21. DiPiro JT. Pharmacology & Therapeutics. Vol. 95. McGraw Hill Medical; 2008.
22. Mosimann V, Neumayr A, Paris DH, Blum J. Liposomal amphotericin B treatment of Old World cutaneous and mucosal leishmaniasis: a literature review. Acta Trop. 2018;182:246–250. doi:10.1016/j.actatropica.2018.03.016
23. van Griensven J, Diro E. Visceral Leishmaniasis: recent Advances in Diagnostics and Treatment Regimens. Infect Dis Clin North Am. 2019;33:79–99. doi:10.1016/j.idc.2018.10.005
24. Rodrigo C, Weeratunga P, Fernando SD, Rajapakse S. Amphotericin B for treatment of visceral leishmaniasis: systematic review and meta-analysis of prospective comparative clinical studies including dose-ranging studies. Clin Microbiol Infect. 2018;24:591–598. doi:10.1016/j.cmi.2017.11.008
25. Miguel DC, Zauli-Nascimento RC, Yokoyama-Yasunaka JKU, et al. Tamoxifen as a potential antileishmanial agent: efficacy in the treatment of Leishmania braziliensis and Leishmania chagasi infections. J. Antimicrob. Chemother. 2009;63:365–368. doi:10.1093/jac/dkn509
26. Miguel DC, Yokoyama-Yasunaka JKU, Uliana SRB. Tamoxifen is effective in the treatment of Leishmania amazonensis infections in mice. PLoS Negl Trop Dis. 2008;2. doi:10.1371/journal.pntd.0000249
27. Eissa MM, Amer EI, El Sawy SMF. Leishmania major: activity of tamoxifen against experimental cutaneous leishmaniasis. Exp Parasitol. 2011;128:382–390.
28. Machado PRL. Tamoxifen and meglumine antimoniate combined therapy in cutaneous leishmaniasis patients: a randomised trial. Trop Med Int Heal. 2018;23:936–942. doi:10.1111/tmi.13119
29. Trinconi CT, Reimão JQ, Coelho AC, Uliana SRB. Efficacy of tamoxifen and miltefosine combined therapy for cutaneous leishmaniasis in the murine model of infection with Leishmania amazonensis. J Antimicrob Chemother. 2016;71:1314–1322. doi:10.1093/jac/dkv495
30. Doroodgar M, Delavari M, Doroodgar M, et al. Tamoxifen Induces Apoptosis of Leishmania major Promastigotes in Vitro. Korean J Parasitol. 2016;54:9–14. doi:10.3347/kjp.2016.54.1.9
31. Morad SAF, Cabot MC. Tamoxifen regulation of sphingolipid metabolism–Therapeutic implications. Biochim Biophys Acta. 1851;1134–1145:2015.
32. Morad SAF, Tan SF, Feith DJ, et al. Modification of sphingolipid metabolism by tamoxifen and N-desmethyltamoxifen in acute myelogenous leukemia–Impact on enzyme activity and response to cytotoxics. Biochim Biophys Acta. 1851;919–928:2015.
33. Landoni M, Piñero T, Soprano LL, et al. Tamoxifen acts on Trypanosoma cruzi sphingolipid pathway triggering an apoptotic death process. Biochem Biophys Res Commun. 2019;516:934–940. doi:10.1016/j.bbrc.2019.06.149
34. Reimão JQ, Uliana SRB. Tamoxifen alters cell membrane properties in Leishmania amazonensis promastigotes. Parasitol Open. 2018;4:4–9. doi:10.1017/pao.2018.3
35. Miguel DC, Yokoyama-Yasunaka JKU, Andreoli WK, Mortara RA, Uliana SRB. Tamoxifen is effective against Leishmania and induces a rapid alkalinization of parasitophorous vacuoles harbouring Leishmania (Leishmania) amazonensis amastigotes. J Antimicrob Chemother. 2007;60:526–534. doi:10.1093/jac/dkm219
36. Trinconi CT, Reimão JQ, Yokoyama-Yasunaka JKU, Miguel DC, Uliana SRB. Combination therapy with tamoxifen and amphotericin B in experimental cutaneous leishmaniasis. Antimicrob Agents Chemother. 2014;58:2608–2613. doi:10.1128/AAC.01315-13
37. Coelho AC, Trinconi CT, Senra L, Yokoyama-Yasunaka JKU, Uliana SRB. Leishmania is not prone to develop resistance to tamoxifen. Int J Parasitol Drugs Drug Resist. 2015;5:77–83. doi:10.1016/j.ijpddr.2015.05.006
38. Machado PRL, Ribeiro CS, França-Costa J, et al. Tamoxifen and meglumine antimoniate combined therapy in cutaneous leishmaniasis patients: a randomised trial. Trop Med Int Heal. 2018;23:936–942.
39. Abbasi A, Tan SF, Feith DJ, et al. The effect of tamoxifen on the growth of Leishmania major promastigotes and amastigotes in vitro. KAUMS J. 2015;19:54–59.
40. Machado PRL, Ribeiro CS, França-Costa J, et al. Tamoxifen and meglumine antimoniate combined therapy in cutaneous leishmaniasis patients: a randomised trial. Trop Med Int Health. 2018;23:936–942.
41. Trinconi CT, Reimao JQ, Bonano VI, et al. Topical tamoxifen in the therapy of cutaneous leishmaniasis. Parasitology. 2018;145:490–496.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.