")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Application of Modified Kite Flap in Reconstruction of Facial Wounds After Operation and Case Series
Authors He G, Yang Q, Shen Y, Zhang L, Wu J, Cheng H
Received 11 January 2024
Accepted for publication 16 March 2024
Published 23 March 2024 Volume 2024:17 Pages 725—730
DOI https://doi.org/10.2147/CCID.S456997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Guanjin He,1,* Qifeng Yang,2,* Yuyang Shen,3 Lanzhi Zhang,2 Jingping Wu,2 Hongbin Cheng1
1Dermatology Department, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Medical Aesthetic Department, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 3Traditional Chinese Medicine Department, The Third People’s Hospital of Chengdu, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingping Wu; Hongbin Cheng, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39, Shi-Er-Qiao Road, Jinniu District, Chengdu, People’s Republic of China, Tel +86 15928747715 ; +86 13880848134, Email [email protected]; [email protected]
Abstract: Our team used a new kite flap preparation method to repair wounds after the removal of a benign facial tumor with satisfactory aesthetic results. Thus, this modified kite flap has significant value in facial trauma repair.
Keywords: facial wound repair, modified kite flap, experience, case series
Introduction
It remains a significant challenge for surgeons to reconstruct facial wounds after complete tumor resection.1 Treating facial wounds is highly challenging, as it requires not only the repair of wounds but also a comprehensive consideration of facial aesthetics and functionality. Otherwise, these defects can significantly impact the patient’s appearance, quality of life, and work, and may even endanger their physical and mental health. It is therefore essential to achieve patient satisfaction with facial aesthetic results. However, there are various methods of wound repair, such as direct primary closure and skin grafting. In the case of a large wound, a direct suture will excessively stretch the surrounding tissue, resulting in obvious deformation and asymmetry in appearance. In terms of aesthetic effect, whether it is split-thickness grafts full-thickness grafts, or other skin grafts surgery, their aesthetic effect is not satisfactory. In addition, due to the lack of reliable blood supply, the possibility of the necrosis of the flap is likely to be greater than that of the flap with reliable blood supply. At the same time, the skin-grafting operation has certain requirements for the technique and equipment of the surgeons.2 However, the local flap is similar to the wound with the texture of the adjacent flap, the local flap has a more ideal aesthetic effect and can meet most of the requirements of the facial defect. It is the first choice for the repair of facial soft tissue defects.3 The commonly used rotating skin flap may cause swelling of the flap pedicle and affect the cosmetic effect. As an modified V-Y skin flap, the kite flap has no problem of bloated of the pedicle and has important application value in facial wound repair.
Patient Information and Therapeutic Intervention
Case 1
A 75-year-old male with a history of facial basal cell carcinomas, a 3.2cm*2.8cm black superficial mass in the left temporal region formed for several years and gradually grew, without any manifestations such as rupture. However, in view of the previous medical history, the mass was finally extended resection with a 3mm, and the intraoperative frozen-section examination report was seborrheic keratosis. The skin source in this part was limited, and the left side was the eyelid. The right side is hairy skin, which is not suitable for the donor area of skin flap. Therefore, we made two kite flaps to cover the wound, with good blood supply, no obvious difference in color and texture, and no obvious deformation in appearance. The two black scab near the incision were the result of high frequency electrical treatment of seborrheic keratosis around the incision and were not a sign of poor incision healing (Figure 1).
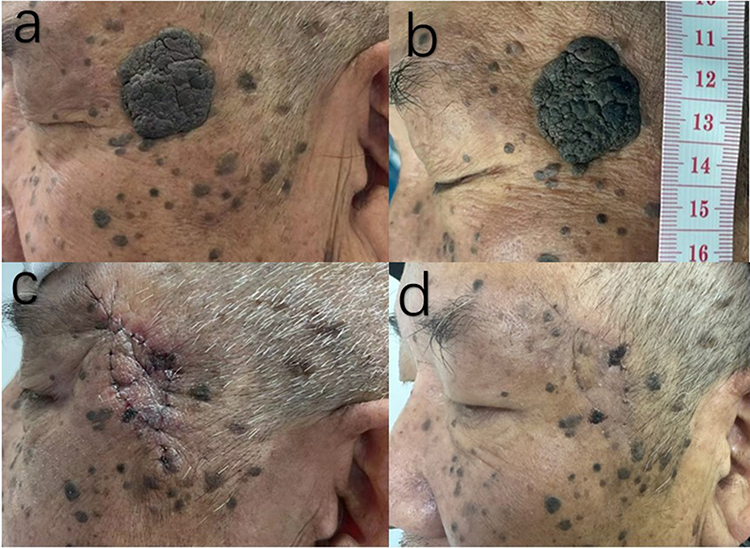 |
Figure 1 Case 1. Notes: Case 1, Two kite flaps were combined to repair the left temporal wound. A 75-year-old male with a history of facial basal cell carcinomas and intraoperative frozen-section examination report was seborrheic keratosis (a)and (b). Flaps of two kite flaps were used to cover the wound (c). Two weeks postoperative follow-up (d). |
Case 2
A 65-year-old male presented with a brown superficial mass on the dorsum of his nose that had been present for several years and had gradually increased in size. The dimensions of the mass were approximately 1.0cm * 1.2cm. The result of the intraoperative frozen-section examination showed a sebaceous gland or nevus sebaceous. We took advantage of the mobility of the paranasal skin and followed the skin’s texture to design a kite flap, which was approximately the same size as the wounds. Subsequently, the flap was advanced to cover the wound and interrupted sutured with nylon sutures after adequate anastomoses with absorbable suture. There is adequate blood supply to the skin flap, and there is no significant deformation in the appearance (Figure 2).
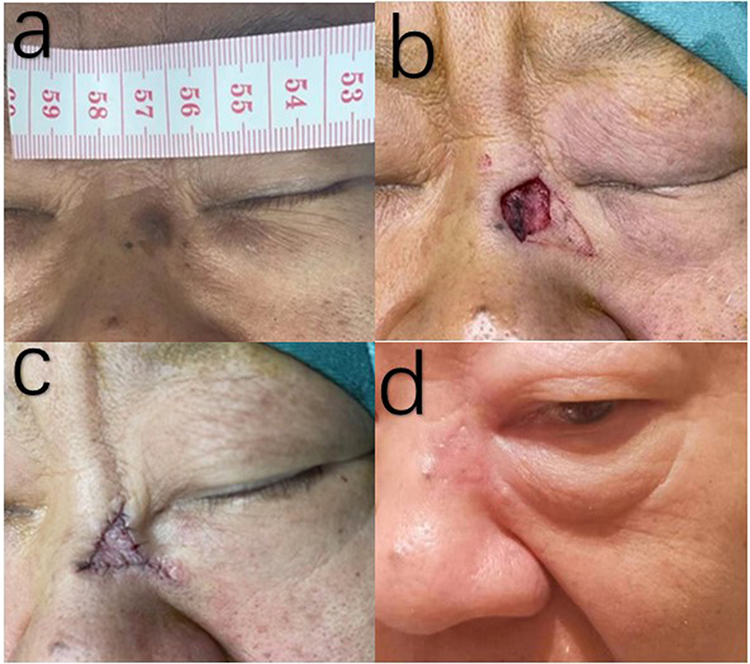 |
Figure 2 Case 2. Notes: Case 2, Kite flap to repair nasal dorsum defect. A 65-year-old male presented with a brown superficial mass on the dorsum (a). A kite flap was performed during the operation (b). The state after sutured (c). The status of more than 1 month after operation (d). |
Case 3
A young male with a nevus near the nasolabial folds measuring approximately 0.8 cm*0.6 cm was completely removed, and the wound was covered with an pushed forward kite flap, which was then closed intermittently with 7–0 nylon sutures after incision and anastomosis with 5–0 absorbable sutures. Blood supply to the flap was adequate and there was no obvious deformity of the facial appearance (Figure 3). When the wound at the nasolabial folds is too large direct suturing can lead to obvious deformity of the upper lip, and if a rotational flap is used, it is prone to bloat at the pedicle part of flap and form “dog-ears”. We resolved these problems perfectly using the modified kite flap advancement method to cover the wound.
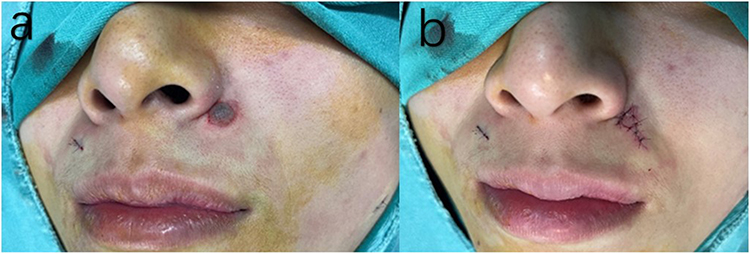 |
Figure 3 Case 3. Notes: Case 3, The kite flap was used to repair the nasolabial groove defect. A young male with a nevus near the nasolabial folds measuring approximately 0.8 cm*0.6 cm (a). The wound was covered by a kite flap and the state after being sutured (b). |
Discussion
The limitation is that the wounds of our cases with complete preservation of preoperative and postoperative photographs were not particularly large, and short follow-up time after surgery but this work will be ongoing and reporting more cases like this is our plan for the future. In addition, the following are some of the insights we would like to express. The depth of the flap pedicle we did was to reach the fat layer, and the range of motion was limited, which meant that our method was not suitable for repairing particularly large wounds. But, if the surrounding tissue source is sufficient, the dual kite flap can be advanced to cover the wound. For a specific case, we can refer to our case 1. For large wounds, the application of double kite flap has more reliable blood supply and can reduce the tension on the tip of the flap to a certain extent. Under particular circumstances it is necessary to cut into the fascial or muscular layers to obtain greater range of motion, but this also means greater damage.
Design of Kite Flap
The kite flap belongs to the V-Y advancement flap. The subcutaneous pedicle contains unknown arteries and veins, which are supplied by the vascular network of the facial subcutaneous tissue. The facial blood supply is rich, the blood supply of the pedicle is reliable. And there is usually no disturbance of blood supply. The application of kite flaps is significant for the repair of facial wounds, as long as the kite flap is appropriately designed, it is less likely to form “dog-ears” than the flap that needs to be rotated,4 so it is usually not necessary to overextend the incision and resection of a lot of normal skin. In addition, especially for the wound near the nasolabial groove and nose, compared with the flap that needs to be rotated, the kite flap does not have the problem of bloating the pedicle, so it has a better cosmetic effect.
The depth of the flap prepared by our team is usually free to the fat layer, which not only ensures that the flap has sufficient blood supply but also ensures that the flap has sufficient ductility and less damage. The width of the flap should be larger than the width of the wound defect to facilitate advancement without resistance. If the flap is too small to cover the wound, forced suture in the later stage, and the tension is too high, it may lead to ischemic necrosis of the flap. In addition, if the wound is too large, the source of the donor area of the flap is limited, and the flap in multiple directions can be considered to cover the wound together, such as dual kite flap. This practice can be referred to in our case 1. Appropriate flap design, tension-reduced suture is critical for repairing facial defects, which is related to the cosmetic effect of postoperative facial scars. If the flap is directly sutured to the wound without tension reduction suture, excessive tension may lead to ischemic necrosis at the edge of the flap, which will also lead to more obvious scar. Therefore, decompression suture is a key step in improved cosmetic results. After full tension reduction suture, the incision of the face can be sutured intermittently with 7–0 nylon thread. In this way, the needle footprint can hardly be seen after the suture is removed.
Our Team ‘S Operating Methods and Characteristics
First, We have some special designs for angles and directions. When removing superficial tumors, we do not go under the knife at a vertical angle, but at an angled angle. This is for holding the kite flap stay upright during the skite flap cover of the wound later, to reduce the tension on the flap and to avoid excessive tension and obvious scarring. Previously, Jianzhong Peng’s5 team reported the application of a modified kite flap in repairing skin defects after facial tumor resection, and our method of preparing a kite flap is very different from theirs. First, we have some special designs for angles and directions. When removing superficial tumors, we do not go under the knife at a vertical angle, but at an angled angle. That means the defect was tilted in the same direction as the flap, and the pedicle of the kite flap is directly consistent with the recipient area of the flap. This is for holding the kite flap stay upright during the skite flap cover of the wound later. Secondly, we retained a wider flap pedicle, and the pedicle of the flap was almost the same as the width of the flap, ensuring sufficient blood supply, avoiding avascular necrosis of the tip, and less trauma. So there was no need to install drainage strips after surgery, and no hematoma occurred after sufficient electrocoagulation during the operation. The biggest difference in our approach is that we changed the direction of the resection of the superficial mass as well as angle of the pedicle of the free flap, not vertically down, but oblique to the flap recipient area. At the same time, when the flap advances forward to cover the wound, the pedicled part remains vertical, so the flap receives less tension. Therefore, the tension of the flap is smaller during suture. Figures 4 and 5 shows the preparation of kite flap.
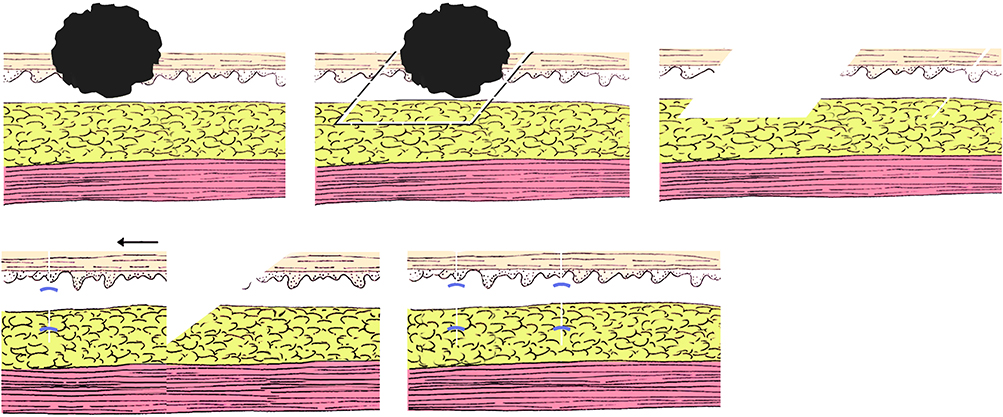 |
Figure 4 Schematic diagram of kite flap I. Notes: The order of operation is from left to right and from top to bottom. The direction of resection the superficial mass and the preparation of the kite flap, as well as the advancement and suturing of the flap are demonstrated. |
 |
Figure 5 Schematic diagram of the kite flap II. Note: This planar graph details the tumor resection, flap preparation, and suture. |
Conclusion
The design and the method of operation of kite flap may be different. However, kite flap is used to repair facial defects, because the color and texture of the flap are close to the recipient area of the flap, so it has good aesthetic result.
Informed Consent
Written informed consent for publication of their details was obtained from the patients and patients also provided informed consent for the images to be published.
Acknowledgments
Guanjin He and Qifeng Yang contributed equally to this work and are joint first authors.
Funding
This work was supported by grants from San Huang Zeng Mian Decoction Treatment Mild-to-Moderate SLE Randomized Controlled Clinical Studies, No. 2021ZD03; The mechanism and clinical evaluation of Qichu whitening cream for the treatment of melasma based on epidermal microecology theory, No. 2022YFS0416; Study on the sensitization mechanism and clinical verification of Sanhuang Zengmian Decoction combined with double immunotherapy in the treatment of malignant melanoma, No. 2023ZD019; And a randomized controlled clinical study on the treatment of diabetes-associated skin pruritus with Qiwei antipruritic San and its mechanism, No. 2022YFS0413.
Disclosure
No institutional approval was required for publication of this case details. The authors state that there is no underlying conflict of interest in this work.
References
1. Yan M, Xiaobo Z, Zhaoqi Y, et al. The kite flap for reconstructing tumour excision wounds in the middle and lower face: a retrospective study. J Wound Care. 2020;29(10):562–566. doi:10.12968/jowc.2020.29.10.562
2. Swaim SF. Skin grafts. The Veterinary Clinics of North America. Small Animal Pract. 1990;20(1):147–175. doi:10.1016/s0195-5616(90)50008-x
3. Guerrissi JO. Fasciocutaneous flap side-to-side V-Y: fish flap. J Craniofa Surg. 2020;31(5):1438–1440. doi:10.1097/SCS.0000000000006330
4. Djedovic G, Metzler J, Morandi EM, et al. Comparison of fasciocutaneous V-Y and rotational flaps for defect coverage of sacral pressure sores: a critical single-centre appraisal. Int Wound J. 2017;14(6):945–949. doi:10.1111/iwj.12736
5. Wu Y, Peng J, Luo X, et al. The application of modified kite flap in repairing facial skin defects after tumor resection. Annal Plastic Surg. 2022;88(1):59–62. doi:10.1097/SAP.0000000000003008
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.