")
Back to Journals » Journal of Pain Research » Volume 17
Are There Any Advantages of the Low Opioid Anaesthesia and Non-Opioid Postoperative Analgesia Protocol: A Clinical Observational Study
Authors Kościuczuk U, Tarnowska K, Rynkiewicz-Szczepanska E
Received 13 November 2023
Accepted for publication 23 February 2024
Published 8 March 2024 Volume 2024:17 Pages 941—951
DOI https://doi.org/10.2147/JPR.S449563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Urszula Kościuczuk, Katarzyna Tarnowska, Ewa Rynkiewicz-Szczepanska
Department of Anaesthesiology and Intensive Therapy, Medical University in Bialystok, Bialystok, Poland
Correspondence: Urszula Kościuczuk, Department of Anaesthesiology and Intensive Therapy, Medical University of Bialystok, Kilinskiego Street 1, Bialystok, Poland, Email [email protected]
Purpose: The methods of perioperative analgesia and pain control have changed. The principle of opioid-based analgesia has been modified to multimodal analgesia, followed by LOA (low opioid anaesthesia) and OFA (opioid-free anaesthesia). The aim was to describe the effects of LOA on nausea, vomiting, and pain control during general anaesthesia and postoperative period after laparoscopic cholecystectomy.
Patients and Methods: The protocol included the study group-40 patients received low-opioid anaesthesia (LOA), and the control group-40 patients received general anaesthesia with opioid analgesia (OA). The scheme of LOA was based on ketamine, lidocaine, magnesium sulfate, paracetamol, and metamizole. The OA was based on standard opioid (fentanyl) administration in induction and maintenance phase due to clinical observation. Postoperative analgesia included 1g of paracetamol and 1g of metamizol intravenously, with a 6-hour interval between doses.
Results: Significant differences in the pain score in the periods of 2– 6, 6– 12, and 12– 24 hours after anaesthesia between the groups were noticed (p < 0.001). Moreover, a significant difference in the frequency of nausea (p = 0.005) and vomiting (p = 0.04) between groups were presented. Nausea occurred in 54.05% of OA group, while in the LOA group, it occurred in a 23.08%. Vomiting occurred in 32.43% of control group, while in the study group, it occurred in 12.82% of patients.
Conclusion: The LOA protocol was more beneficial in reducing nausea and vomiting than the opioid-based method of anaesthesia. The LOA protocol of general anaesthesia during laparoscopic cholecystectomy and non-opioid postoperative analgesia have better outcomes in pain control, as well as nausea and vomiting, and improve postoperative patient comfort. The LOA protocol during anaesthesia and non-opioid postoperative analgesia should be considered in routine practice.
Keywords: analgesia, coanalgesics, perioperative safety
Introduction
The analgesia is essential element of general anaesthesia, and the postoperative period. Definition of general anaesthesia and the principles of the analgesic ladder present that strong opioids are the basic substances dedicated to perioperative analgesia.1–3 The opioid side-effects (sedation, respiratory depression, constipation, cognitive and social dysfunctions) are well known and widely described.4–9 Recently, many publications have highlighted new aspects of opioid therapy - opioid-induced immunomodulation, as well as carcinogenesis processes and oxidative imbalance.10–15
The principles of perioperative acute pain management have changed.1,3,16,17 The original principle of high-dose opioid analgesia has been modified to multimodal analgesia. Recent years have presented LOA (low-opioid anaesthesia) and OFA (opioid-free anaesthesia). The LOA provides analgesia using one dose of opioid for the induction of anaesthesia, followed by non-opioid anaesthesia in the next stages. From the pharmacological perspective, the LOA protocol is based on typical analgesics (paracetamol, metamizole, nonsteroidal anti-inflammatory drugs (NSAIDs)), and coanalgesics (lidocaine, ketamine, magnesium sulfate, dexmedetomidine, clonidine, steroids, gabapentinoids). OFA is completely method without opioid analgesics during anaesthesia and the postoperative period.18–22 Premedication with benzodiazepines, as well as gabapentinoids, regional analgesia (peripheral nerve blockades) and local analgesia (wound infiltration) are crucial of LOA/OFA.23–30 LOA is successfully used in different types of surgical procedures, and it is important element of the ERAS protocol. The advantages of LOA also meet the expectations of increased perioperative safety and reduction in postoperative symptoms—pain, nausea and vomiting.31–34
In our study, we chose elective laparoscopic cholecystectomy, because this type of surgery, despite the minimally invasive surgical technique, presents very intense pain stimulation due to anatomical reasons, peritoneal innervation and pneumoperitoneum formation. Additionally, laparoscopic cholecystectomy is the dominant part of the surgery methods for chronic gallbladder stones and it consists 90% of surgical procedures.31,35,36
The aim of study was to describe the role of the unique protocol of LOA in the main aspects of postoperative symptoms—nausea, vomiting, and pain control during general anaesthesia for laparoscopic cholecystectomy. The scheme of LOA was based on ketamine, lidocaine, magnesium sulfate, paracetamol, and metamizole. Statistical analysis was used to present the incidence and severity of nausea, vomiting, and pain within 24 hours, postoperatively. Moreover, the point was to determine the influence of patient anthropometric data and surgical and anaesthesiological factors on the incidence of nausea and vomiting. This study was used to assess the effectiveness of the proposed method of analgesia to minimise postoperative nausea and vomiting syndrome (PONV) and provide postoperative analgesia. Despite the clinical aspect, the study tried to present the risk factors (personal, surgical, and connected with anaesthesia) of postoperative symptoms.
Materials and Methods
This study was approved by the Bioethics Committee of the Medical University of Bialystok, Poland (R-I-002/105/2019), and all patients were informed and provided written consent. The study was conducted in compliance with the Declaration of Helsinki. The study was conducted during the period from September 2019 to December 2019.
The study included a total of 80 adult patients qualified for general anaesthesia for laparoscopic cholecystectomy due to chronic cholecystitis calculosa with a preoperative health assessment according to the American Society of Anaesthesiologists Scale (ASA) I and II. The criteria for excluding a patient from the study and the control group included refusal to participate in the study, health status according to ASA III and IV, a history of cancer or initial cancer diagnosis, and chronic pain, liver cirrhosis, and epilepsy. Moreover, the study did not include patients with an addiction to drugs, alcohol and psychoactive substances or a history of postoperative nausea and vomiting, allergic reactions or contraindications to analgesics.
This study included 80 adult patients divided into two groups according to the method of anaesthesia: the study group—40 patients who received general anaesthesia with the low-opioid protocol (low-opioid anaesthesia—LOA)—and the control group—40 patients who received general anaesthesia with the use of the opioid drug fentanyl (opioid anaesthesia—OA). Postoperative analgesia included the administration of 1g of paracetamol and 1g of metamizol intravenously, with a 6-hour interval between doses. Depending on the degree of pain control, patients could opt out of the planned doses of analgesics or receive additional analgesics, and in the case of nausea or vomiting, ondansetron at a dose of 4 mg intravenously was administered.
The primary endpoint was the incidence of postoperative nausea, vomiting and pain within 2 hours after surgery. Secondary endpoints included most severe intensity of the nausea, vomiting and pain within next postoperative periods: 2–6, 6–12, 12–24 h after surgery.
Both methods of anaesthesia are equal in perioperative safety. Firstly, the study group was recruited, and then the control group with the maintenance of the same surgical and anaesthesiological team. Similarly, in the group of surgeons, the team consisted of 5 specialists performing laparoscopic surgeries using the same technique. During the study, no conversion to laparotomy was recorded. The preliminary analysis did not present any statistically significant differences in the duration of the operation. The recruiting data and patient management and pharmacotherapy during anaesthesia in both groups are presented in Figure 1.
 |
Figure 1 The schedule of general anaesthesia and analgesia. The bold black text is characteristic of the study group, and the bold red text is characteristic of the control group. Abbreviations: ECG, electrocardiography; BP, blood pressure; SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure; HR, heart rate; SpO2, oxygen saturation; TOF, Train of Four; TOFR, Train-of-Four Ratio; p.o, per os. |
The anthropometric parameters: sex, age, weight, height, BMI (Body Mass Index), BSA (body surface area) by Dubois formula, duration of anaesthesia, duration of pneumoperitoneum and duration of surgery were recorded. Additionally, the total dose of fentanyl used during anaesthesia in the control group was noted.
The occurrence and severity of nausea and vomiting were controlled during the first 2 hours after surgery and between 2 and 6, 6 and 12 and 12 and 24 hours after surgery using a postoperative questionnaire based on a numerical scale from 0 to 2, where 0 = no nausea or no vomiting, 1 = nausea, and 2 = vomiting, and a verbal analogue scale was used to present the intensity of nausea or vomiting (mild, moderate, strong). The pain intensity was also assessed in subsequent time intervals using the Verbal Analogue Scale (mild, moderate, strong). In order to assess the correlation between the pain and the use of planned analgesics in the postoperative period, the mean NRS (Numerical Rating Scale) value (sum of pain numerical value NRS in the periods of 0–2, 2–6, 6–12, 12–24 h divided by the number of measurements) was counted.
The Shapiro‒Wilk test was used to check the normality of the data distribution. Continuous variables were presented with descriptive parameters (mean, median, min-max, interquartile ranges), categorical variables with absolute numbers and percentages. The Mann–Whitney U-test was used to present differences between groups in continuous variables. Spearman’s rank test was used to describe correlations between variables. Chi-square was used to compare groups in terms of the categorical variables without normal distribution. All calculations were performed in Statistica 13.1 software (StatSoft, Krakow, Poland). The level of significance was p <0.05. This was a pilot prospective study; therefore, the sample size was determined as 40 subjects in the experimental group.
Results
A total of 39 patients (26 women and 13 men) from the LOA group and 37 patients (26 women and 11 men) from the OA group were included in analysis. The LOA group consisted of 11 patients with ASA 1 and 28 patients with ASA 2. In the OA group, there were 11 patients with ASA1 and 26 patients with ASA 2. Hypertension arteralis, diabetes mellitus, nicotinism, asthma, and arrhythmias were the most common clinical conditions in ASA 2. The groups did not differ in anthropometric parameters: age, weight, BSA, and BMI. There were no events of surgical conversion to laparotomy.
In the analysis, no statistically significant differences were noticed between the groups in pain intensity up to 2 hours after surgery. The analysis showed significant differences in the VAS scale in the periods of 2–6, 6–12, 12–24 hours between the groups (p < 0.001).
The dynamics of pain intensity were more favourable in the LOA group. In the period 2–6 hours after surgery, the number of patients with strong pain increased in the OA group, while in the LOA group, it was stable. In the next period 6–12 h, the number of patients with mild pain increased, while the number of patients with moderate pain decreased in LOA. In the same period in the OA, the number of patients with moderate pain was increased compared with that in the LOA group and remained constant. At the end of the first day after surgery, the number of patients without pain was higher than that at the beginning of the observation in the LOA group. The mean NRS value in first postoperative day was 2.34 in the LOA group, while it was 4.11 in the OA, respectively. Additional analgesics were administered only in the OA after 12 h in cases of moderate pain (tramadol was used in 10 patients) and strong pain (oxycodone was used in one patient).
The trajectory of analgesia in the postoperative period in both groups and the numbers of patients without pain and with mild pain, moderate pain, and strong pain are presented in Figure 2.
 |
Figure 2 The trajectory of analgesia in the postoperative period in both groups. The numbers of patients without pain, and with mild pain, moderate pain, and strong pain are noted. |
The analysis confirmed a significant difference of incidence of nausea (p = 0.005) and vomiting (p = 0.04) between groups. Nausea occurred in 54.05% of the patients in the OA group, while 23.08% in the LOA group. Vomiting occurred in 32.43% of people in the control group, while in the study group, it occurred in 12.82% of patients. Moreover, 87.18% of the patients from the LOA group did not experience vomiting, and 76.92% of patients did not experience nausea.
The numbers of patients with nausea and vomiting and without symptoms in both groups and the significant differences are presented in Figure 3.
 |
Figure 3 The numbers of patients with nausea and vomiting, and without symptoms in the study and control groups. *p<0.05. |
The severity of nausea within 0–2 hours after surgery differed significantly (p = 0.04). In the OA group, the incidence of mild (6 patients, 85.71% of the group), moderate (3 patients, 75% of the group) and severe (1 patient) nausea was higher than that in the LOA group—1, 1 and 0, respectively. Significant differences between the groups were observed between 2 and 6 h (p = 0.025). In the OA group, the incidence of mild nausea (7 patients, 87.5%) was higher. In addition, moderate and severe nausea occurred only in the OA group. In the period 6–12 h and 12–24 h, there were no significant differences in the intensity of nausea between the groups. The incidence of mild nausea in the LOA group was lower than that in the OA group, while moderate nausea occurred only in the OA group. In addition, no moderate or severe nausea was noted in the LOA group.
The numbers of patients without nausea symptoms in the postoperative period in both groups and the significant differences are presented in Figure 4.
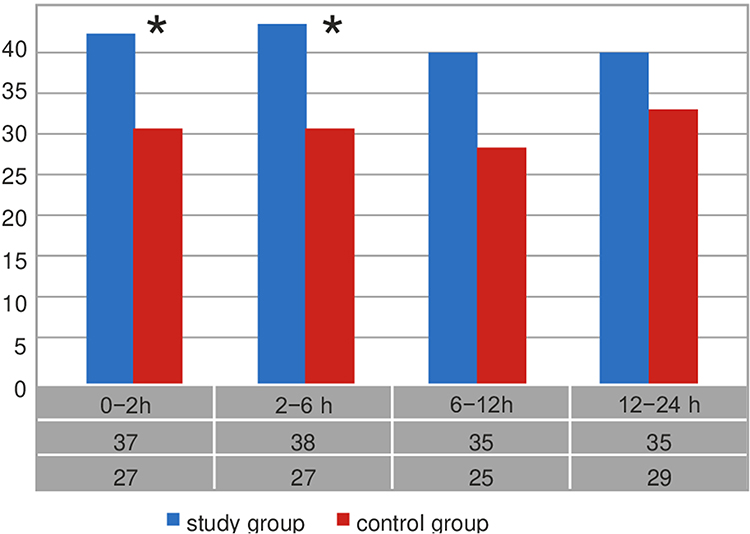 |
Figure 4 The numbers of patients without nausea symptoms in the study and control groups.*p<0.05. |
The analysis presented no significant differences between the groups in the incidence of vomiting up to 2 hours after the operation; in 97.44% of the patients in the LOA group and in 91.89% of the patients in the OA group, no vomiting was reported. However, mild and moderate vomiting occurred only in the OA group, in three patients (8.11% of the group).
In the periods of 2–6, 6–12, and 12–24 hours after surgery, no significant differences in the severity of vomiting between the groups were described, and severe vomiting was observed only in the OA group in the period of 6–12 hours (1 patient, 2.7% of the group).
The numbers of patients without vomiting symptoms in the postoperative period in both groups and the significant differences are presented in Figure 5.
 |
Figure 5 The incidence of vomiting symptoms in the postoperative period in the study and control groups. The numbers of patients without vomiting symptoms are noted. |
The mean total dose of fentanyl in the control group for the patients who did not experience nausea was 0.24mg, while for those who experienced nausea, it was 0.25 mg, and no statistical significance was noted. In addition, there was no significant correlation between fentanyl and nausea and vomiting.
The statistical analysis did not present correlation between the duration of pneumoperitoneum and nausea (study group, p = 0.205; control group, p = 0.156). The mean duration of pneumoperitoneum among the patients who did not experience nausea (38.77 minutes) was similar to that in the control group with nausea (38.30 minutes). LOA provided better postoperative comfort in nausea protection. In the OA group, a significant correlation was shown between nausea between 12 and 24 hours after surgery and the duration of pneumoperitoneum (p = 0.028).
There was no significant correlation between the duration of surgery and the duration of anaesthesia and the occurrence of nausea. Therefore, it was observed that the duration of anaesthesia was longer in those who did not experience nausea in the LOA group.
The analysis did not present a correlation between gender and the occurrence of nausea. Nausea occurred more often among women (61.54%) than among men (36.36%) in the OA group. There was also no correlation between gender and the occurrence of vomiting. In the analysis, no correlations were noted between anthropometric factors (age, BMI, BSA) and the occurrence of nausea.
Discussion
The main goal of our study was to determine whether the reduction in the use of opioid drugs during anaesthesia and postoperative period will maintain the patient’s comfort of analgesic control, nausea and vomiting. In the proposed study, LOA protocol based on the use of a single dose of fentanyl in the induction phase of anaesthesia with multimodal analgesia based on pharmacotherapy with coanalgesics—ketamine, lidocaine, magnesium sulfate, and repeated doses of paracetamol and metamizole in the postoperative period was used.
Various pharmacological models of LOA or OFA have been described. In premedication, benzodiazepines, gabapentinoids, alpha 2 agonists, dexmedetomidine, and clonidine were presented. Additionally, paracetamol, metamizole, anti-inflammatory non-steroid drugs, and steroids were also presented in the analgesic method. Toleska et al proposed an OFA protocol based on combined general anaesthesia with intravenous induction (propofol) and volatile maintenance (sevoflurane) with preoperative dexamethasone at 0.1 mg/kg and 1.0 g of paracetamol, followed by a lidocaine infusion at 2 mg/kg/h and magnesium sulfate at 1.5 mg/h in the maintenance phase. The authors did not observe statistical significance in the occurrence of postoperative nausea and vomiting. However, it was indicated that the pain score was significantly higher both at rest and coughing at 1 and 24 hours after surgery in the group with opioid anaesthesia.35,36
Multimodal techniques for OFA anaesthesia were also developed by Jan Mulier and Igor Zadonsky. The newest 2020 modifications suggest premedication with 150 µg p.o. of clonidine or 150–300 µg p.o. of gabapentin. The MULIMIX syringe means composition of 50 µg of dexmedetomidine, 50 mg of ketamine or 25 mg of s-ketamine, 500 mg of lidocaine, 2.5 g of magnesium sulfate filled up to 50 mL with NaCl. Preinduction means a bolus of 0.25 µg/kg of dexmedetomidine 10–20 minutes before anaesthesia. The induction phase of anaesthesia is an infusion of 1–1.5 mL/10 kg connected with propofol infusion followed by a bolus of 25–50 mg of ketamine before the skin incision is made. Moreover, 75 mg of diclofenac, 40 mg of parecoxib, or 30 mg of ketorolac are recommended before laparoscopy. Local infiltration with 1% lidocaine with a maximum dose of 200 mg, as well as wound infiltration at the end of surgery with the long-acting local anaesthetic ropivacaine, with a maximum dose of 3 mg/kg are recommended. The infusion of 1 mL/10 kg/h of the mixture Mulimix is dedicated in maintenance phase of anaesthesia. The authors suggest continuing analgesia in the Post-Anaesthesia Care Unit (PACU) and surgical department with a mixture infusion of 0.5 mL/10 kg/h, and even patient-controlled intravenous analgesia (PCIA) with boluses of 1mL every 15 min. The use of non - opioid analgesia in general anaesthesia based on target-controlled intravenous infusion (TCI) of propofol (Schnider protocol) increases the advantages of this method through the antiemetic effect of propofol.23,37
The goals of perioperative non-opioid analgesia are widely used in many surgical procedures, specifically endoscopic techniques, such as gynaecological procedures, bariatric surgery, general surgery and neurosurgery.38–40 LOA and OFA meet the principles of modern perioperative safety resulting from the ERAS protocol.22,24,41
Female gender, PONV in medical history, motion sickness, non-smoking status, a young age, general anaesthesia with volatile agents and nitrous oxide, opioid-postoperative analgesia, laparoscopic surgery, gynaecological procedures, and the duration of anaesthesia were described as a risk factors.42–44 Postoperative nausea and vomiting were less common with alfentanil than with fentanyl or sufentanil.45
The Apfel scale in dedicated to predict the occurrence of PONV. The modified scale presents five risk factors that each take a numerical value of one point (female gender, history of PONV, age <50, opioid use in the PACU, nausea in the PACU). The occurrence of 0, 1, 2, 3, 4, and 5 risk factors corresponds to PONV risks of approximately 10%, 20%, 30%, 50%, 60%, and 80%, respectively. A score of 0–1 points indicates a 10–20% low risk of PONV, a score of 2 points indicates a 40% medium risk factor, and a score of 3–5 points indicates a 60–100% high risk of PONV.43,46–49 In our study, we used 4 mg of ondansetron at the patient’s request, and we did not routinely use it as a perioperative management.
In our study, we used verbal classification to assess the intensity of nausea, vomiting, and pain perception by describing subjective symptoms as mild, moderate, or severe. Circulatory symptoms—tachycardia and increased blood pressure or haemodynamic instability—are clinical symptoms of inadequate analgesia. Many technological solutions based on other clinical changes as a peripheral (skin) sympathetic tone, galvanic response (sympathetic tone), plethysmographic pulse waves (sympathetic vascular tone), temperature, and peripheral vascular and cardiac sympathetic tone are available for pain detection during general anaesthesia.50–52
Effective analgesia is crucial for perioperative safety. Uncontrolled postoperative pain disturbs the reconvalescence process and induces pulmonary and circulatory complications and postoperative stress. Opioid drug therapy in acute postoperative pain should be particularly balanced and controlled because poorly controlled acute pain is modified into chronic pain. At the same time, the excessive prescription of opioid drugs leads to prolonged use and an increased risk of addiction and tolerance.53,54.
The conclusions of our study are promising and have clinical value. In the presented model, we proposed the use of LOA for laparoscopic cholecystectomy, and we analysed the impact of various elements on the occurrence and intensity of pain, nausea and vomiting—individual, surgical and anaesthesia factors. The proposed protocol of general anaesthesia significantly reduced the incidence of nausea and vomiting on the first postoperative day, with particular reduction in these symptoms during the period 2–12 hours after surgery. In addition, the advantage of the proposed analgesic model was a significant reduction in pain from 2 to 24 hours after surgery. We showed that the LOA protocol was more beneficial in reducing nausea and vomiting during a longer duration of pneumoperitoneum than the fentanyl dose-based method of anaesthesia. However, we are aware of the limitations of the study. The study based on a larger study group should be conducted. In the study, pharmacotherapeutic aspects were focused on. We did not use complementary methods, such peripheral nerve blocks or infiltration of the postoperative wound.
Conclusions
In conclusion, the LOA protocol as a main element of general anaesthesia during laparoscopic cholecystectomy and postoperative acute pain management is feasible and independently associated with a better outcome, in particular for pain, as well nausea and vomiting outcomes. The effects are better than those of traditional opioid-based anaesthesia. The lower rate of postoperative complications improves perioperative safety and patient comfort. A unique protocol for LOA and opioid-reduced postoperative analgesia should be considered in routine surgical practice.
Data Sharing Statement
Data are available upon request to U Kosciuczuk.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
This study was approved by the Bioethics Committee of the Medical University of Bialystok, Poland (R-I-002/105/2019), and all patients were informed and provided written consent. The study was conducted in compliance with the Declaration of Helsinki.
Acknowledgments
The study was conducted with cooperation with prof. Hady Razak Hady (Department of General Surgery, Medical University of Bialystok, Poland) and Dr Komorowska – Wojtunik Ewa.
Author Contributions
All authors made a significant contribution to the work reported, conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mulier JP, Hunter JM, de Boer HD. Seventy-five years since the birth of the Liverpool anaesthetic technique. Br J Anaesth. 2021;126(2):343–347. doi:10.1016/j.bja.2020.10.020
2. Robinson DH, Toledo AH. Historical development of modern anesthesia. J Invest Surg. 2012;25(3):141–149. doi:10.3109/08941939.2012.690328
3. Ellis TA 2nd, Narr BJ, Bacon DR. Developing a specialty: J.S. Lundy’s three major contributions to anesthesiology. J Clin Anesth. 2004;16(3):226–229. doi:10.1016/j.jclinane.2003.07.005
4. Brown EN, Pavone KJ, Naranjo M. Multimodal general anesthesia: theory and practice. AnesthAnalg. 2018;127(5):1246–1258. doi:10.1213/ANE.0000000000003668
5. Rogobete AF, Sandesc D. General anesthesia as a multimodal individualized clinical concept. Medicina. 2022;58(7):956. doi:10.3390/medicina58070956
6. Kosciuczuk U, Jakubow P, Tarnowska K, Rynkiewicz-Szczepanska E. Opioid therapy and implications for oxidative balance: a clinical study of Total Oxidative Capacity (TOC) and Total Antioxidative Capacity (TAC). J Clin Med. 2023;13(1):82. doi:10.3390/jcm13010082
7. Small C, Laycock H. Acute postoperative pain management. Br J Surg. 2020;107(2):e70–e80. doi:10.1002/bjs.11477
8. Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;74(5):651–662. doi:10.1111/anae.14582
9. de Boer HD, Detriche O, Forget P. Opioid-related side effects: postoperative ileus, urinary retention, nausea and vomiting, and shivering. A review of the literature. Best Pract Res Clin Anaesthesiol. 2017;31(4):499–504. doi:10.1016/j.bpa.2017.07.002
10. Kosciuczuk U, Knapp P, Lotowska-Cwiklewska AM. Opioid-induced immunosuppression and carcinogenesis promotion theories create the newest trend in acute and chronic pain pharmacotherapy. Clinics. 2020;75:e1554. doi:10.6061/clinics/2020/e1554
11. Kosciuczuk U, Jakubow P, Czyzewska J, Knapp P, Rynkiewicz-Szczepanska E. Plasma brain-derived neurotrophic factor and opioid therapy: Results of Pilot Cross-Sectional Study. Clin Med Res. 2022;20(4):195–203. doi:10.3121/cmr.2022.1731
12. Wei G, Moss J, Yuan CS. Opioid-induced immunosuppression: is it centrally mediated or peripherally mediated? Biochem Pharmacol. 2003;65(11):1761–1766. doi:10.1016/s0006-2952(03)00085-6
13. Bissell BD, Sturgill JL, Bruno MEC, Lewis ED. Assessment of opioid-induced immunomodulation in experimental and clinical sepsis. Crit Care Explor. 2023;5(1):e0849. doi:10.1097/CCE.0000000000000849
14. Sacerdote P. Opioid-induced immunosuppression. CurrOpin Support Palliat Care. 2008;2(1):14–18. doi:10.1097/SPC.0b013e3282f5272e
15. Malofoglia V, Ilari S, Vitiello L, et al. The interplay between chronic pain, opioids, and the immune system. Neuroscientist. 2022;28:613–627. doi:10.1177/10738584211030493
16. O’Neil A, Lirk P. Multimodal analgesia. Anesthesiol Clin. 2022;40(3):455–468. doi:10.1016/j.anclin.2022.04.002
17. Egan TD. Are opioids indispensable for general anaesthesia? Br J Anaesth. 2019;122(6):e127–e135. doi:10.1016/j.bja.2019.02.018
18. Baboli KM, Liu H, Poggio JL. Opioid-free postoperative analgesia: is it feasible? Curr Prob Surg. 2020;57:100794. doi:10.1016/j.cpsurg.2020.100794
19. Carcamo-Cavazos V, Cannesson M. Opioid-free anesthesia: the pros and cons. Adv Anesth. 2022;40(1):149–166. doi. doi:10.1016/j.aan.2022.07.003
20. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
21. Vasilopoulos T, Wardhan R, Rashidi P, et al; Temporal Postoperative Pain Signatures (TEMPOS) Group. Patient and procedural determinants of postoperative pain trajectories. Anesthesiology. 2021;134(3):421–434. doi:10.1097/ALN.0000000000003681
22. Echeverria-Villalobos M, Stoicea N, Todeschini AB, et al. Enhanced Recovery After Surgery (ERAS): a perspective review of postoperative pain management under ERAS pathways and its role on opioid crisis in the United States. Clin J Pain. 2020;36(3):219–226. doi:10.1097/AJP.0000000000000792
23. Sultana A, Torres D, Schumann R. Special indications for opioid free anaesthesia and analgesia, patient and procedure related: including obesity, sleep apnoea, chronic obstructive pulmonary disease, complex regional pain syndromes, opioid addiction and cancer surgery. Best Pract Res Clin Anaesthesiol. 2017;31:547–560. doi:10.1016/j.bpa.2017.11.002
24. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) Guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
25. Thota R, Ramkiran S, Garg R, Goswami J, Baxi V, Thomas M. Opioid free onco-anesthesia: is it time to convict opioids? A systematic review of literature. J Anaesth Clin Pharmacol. 2019;35:441–452. doi:10.4103/joacp.JOACP_128_19
26. Morgenstern C, Ramírez-Paesano C, Galcerán AJ, Morgenstern R. Thoracolumbar interfascial plane block results in opioid-free postoperative recovery after percutaneous/endoscopic transforaminal lumbar interbody fusion surgery. World Neurosurg. 2021;153:e473–e480. doi:10.1016/j.wneu.2021.06.152
27. Williams L, Iteld L. Moving toward opioid-free breast surgery: regional blocks and a novel technique. Clin Plast Surg. 2021;48(1):123–130. doi:10.1016/j.cps.2020.09.003
28. Darmawikarta D, Sourour M, Couban R, et al. Opioid-free analgesia for supratentorial craniotomies: a systematic review. Can J Neurol Sci. 2019;46(4):415–422. doi:10.1017/cjn.2019.57
29. Chia PA, Cannesson M, Bui CCM. Opioid free anesthesia: feasible? Curr Opin Anaesthesiol. 2020;33(4):512–517. doi:10.1097/ACO.0000000000000878
30. Beloeil H. Opioid-free anesthesia. Best Pract Res Clin Anaesthesiol. 2019;33(3):353–360. doi:10.1016/j.bpa.2019.09.002
31. Jiang B, Ye S. Pharmacotherapeutic pain management in patients undergoing laparoscopic cholecystectomy: a review. Adv Clin Exp Med. 2022;31(11):1275–1288. doi:10.17219/acem/151995
32. Bugada D, Lorini LF, Lavand’homme P. Opioid free anesthesia: evidence for short and long-term outcome. Minerva Anestesiol. 2021;87(2):230–237. doi:10.23736/S0375-9393.20.14515-2
33. Salomé A, Harkouk H, Fletcher D, Martinez V. Opioid-free anesthesia benefit-risk balance: a systematic review and meta-analysis of randomized controlled trials. J Clin Med. 2021;10(10):2069. doi:10.3390/jcm10102069
34. Forget P. Why and how? A contextual analysis. Anaesth Crit Care Pain Med. 2019;38(2):169–172. doi:10.1016/j.accpm.2018.05.002
35. Toleska M, Dimitrovski A, Toleska-Dmitrovska N. Postoperative nausea and vomiting in opioid-free anesthesia versus opioid based anesthesia in laparoscopic cholecystectomy. Pril. 2022;43(3):101–108. doi:10.2478/prilozi-2022-0042
36. Toleska M, Dimitrovski A. Is opioid-free general anesthesia more superior for postoperative pain versus opioid general anesthesia in laparoscopic cholecystectomy? Pril. 2019;40(2):81–87. doi:10.2478/prilozi-2019-0018
37. Mulier JP. Is opioid-free general anesthesia for breast and gynecological surgery a viable option? Curr Opin Anaesthesiol. 2019;3: 257-262. Available from: https://www.researchgate.net/publication/356169952_OFAM_opioid_free_general_anesthesia_mixture_Mulimix_Multimodal_anaesthesia_developed.
38. Sadowska D, Bialka S, Palaczynski P, et al. Opioid-free anaesthesia effectiveness in thoracic surgery—objective measurement with a skin conductance algesimeter: a randomized controlled trial. Int J Environ Res Public Health. 2022;19(21):14358. doi:10.3390/ijerph192114358
39. An G, Zhang Y, Chen N, Fu J, Zhao B, Zhao X. Opioid-free anesthesia compared to opioid anesthesia for lung cancer patients undergoing video-assisted thoracoscopic surgery: a randomized controlled study. PLoS One. 2021;16(9):e0257279. doi:10.1371/journal.pone.0257279
40. Ziemann-Gimmel P, Goldfarb AA, Koppman J, Marema RT. Opioid-free total intravenous anaesthesia reduces postoperative nausea and vomiting in bariatric surgery beyond triple prophylaxis. Br J Anaesth. 2014;112(5):906–911. doi:10.1093/bja/aet551
41. Ibrahim M, Elnabtity AM, Hegab A, Alnujaidi OA, El Sanea O. Combined opioid free and loco-regional anaesthesia enhances the quality of recovery in sleeve gastrectomy done under ERAS protocol: a randomized controlled trial. BMC Anesthesiol. 2022;22(1):29. doi:10.1186/s12871-021-01561-w
42. Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
43. Darvall J, Handscombe M, Maat B, So K, Suganthirakumar A, Leslie K. Interpretation of the four risk factors for postoperative nausea and vomiting in the Apfel simplified risk score: an analysis of published studies. Can J Anaesth. 2021;68(7):1057–1063. doi:10.1007/s12630-021-01974-8
44. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. AnesthAnalg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
45. Langevin S, Lessard MR, Trépanier CA, Baribault JP. Alfentanil causes less postoperative nausea and vomiting than equipotent doses of fentanyl or sufentanil in outpatients. Anesthesiology. 1999;91(6):1666–1673. doi:10.1097/00000542-199912000-00019
46. Apfel CC, Heidrich FM, Jukar-Rao S, et al. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br J Anaesth. 2012;109(5):742–753. doi:10.1093/bja/aes276
47. Rajan N, Joshi GP. Management of postoperative nausea and vomiting in adults: current controversies. Curr Opin Anaesthesiol. 2021;34(6):695–702. doi:10.1097/ACO.0000000000001063
48. Yayla A, Ilgin VE, Kılınç T, et al. Nausea and vomiting after laparoscopic cholecystectomy: analysis of predictive factors. J Perianesth Nurs. 2022;37(6):834–841. doi:10.1016/j.jopan.2022.01.002
49. Naemi AR, Kashanitabar V, Kamali A, Shiva A. Comparison of the effects of haloperidol, metoclopramide, dexmedetomidine and ginger on postoperative nausea and vomiting after laparoscopic cholecystectomy. J Med Life. 2020;13(2):206–210. doi:10.25122/jml-2019-0070
50. Shahiri TS, Richebé P, Richard-Lalonde M, Gélinas C. Description of the validity of the Analgesia Nociception Index (ANI) and Nociception Level Index (NOL) for nociception assessment in anesthetized patients undergoing surgery: a systematized review. J Clin Monit Comput. 2022;36(3):623–635. doi:10.1007/s10877-021-00772-3
51. Ledowski T. Objective monitoring of nociception: a review of current commercial solutions. Br J Anaesth. 2019;123(2):e312–e321. doi:10.1016/j.bja.2019.03.024
52. von Dincklage F, Ledowski T. Monitoring of nociception: is more always more? Br J Anaesth. 2021;126(2):352–354. doi:10.1016/j.bja.2020.11.014
53. Chapman CR, Vierck CJ. The transition of acute postoperative pain to chronic pain: an integrative overview of research on mechanisms. J Pain. 2017;18(4):359.e1–359.e38. doi:10.1016/j.jpain.2016.11.004
54. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.