")
Back to Journals » International Journal of Women's Health » Volume 16
Association Between Composite Dietary Antioxidant Index and the Risk of Endometriosis-Related Rheumatoid Arthritis in Women of Childbearing Age: A Cross-Sectional Study Based on the National Health and Nutrition Examination Survey Database
Authors Hu H, Wang X, Ren Y, Zhang T, Sun L
Received 6 December 2023
Accepted for publication 9 April 2024
Published 23 April 2024 Volume 2024:16 Pages 717—726
DOI https://doi.org/10.2147/IJWH.S453602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Haiyang Hu, Xiaoxiao Wang, Yangsheng Ren, Tishuo Zhang, Lin Sun
Department of Gynecology, Affiliated Hospital of Jining Medical University, Jining, Shandong, 272029, People’s Republic of China
Correspondence: Lin Sun Department of Gynecology, Affiliated Hospital of Jining Medical University, 89 Guhuai Road, Jining, Shandong, 272029, People’s Republic of China, Tel +86 18678760870 ; +86-05372908731, Email [email protected]
Purpose: To evaluate the association between Composite Dietary Antioxidant Index (CDAI) and the risk of endometriosis (EM)-related rheumatoid arthritis (RA) in women of childbearing age.
Methods: Using the data from the National Health and Nutrition Examination Survey database, this cross-sectional study included women of childbearing age. The CDAI was obtained by summing the standardized Z-values of the dietary intakes. EM was diagnosed based on a questionnaire-based survey. The outcome of this study was the presence of RA, which was defined by a questionnaire. The associations of CDAI and EM with the risk of RA were determined using weighted logistic analysis. Additive interaction was evaluated using the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP), and the synergy index (S).
Results: In total, 3803 patients were included, of which 74 patients (1.99%) were with RA. A lower CDAI [odds ratio (OR): 1.85, 95% confidence interval (CI): 1.12 to 3.04, P= 0.015] and the presence of EM (OR: 3.05, 95% CI: 1.19 to 7.81, P= 0.023) was associated with the risk of RA. The result demonstrated an additive interaction of a lower CDAI and the presence of EM on the risk of RA (OR: 6.19, 95% CI: 2.33 to 16.43, P < 0.001, P of trend =0.007). Nevertheless, there was no significant additive interaction after being assessed by the RERI, AP, and S. However, a joint effect of a lower CDAI and EM on the risk of RA (OR: 3.94, 95% CI: 1.35 to 11.51, P= 0.013) was observed.
Conclusion: Our study identified EM, and lower CDAI, was related to the risk of RA. Lower CDAI score was also associated with the risk of EM-related RA. This study indicates the importance of antioxidant intake in daily diet for the management of EM-related RA.
Keywords: composite dietary antioxidant index, endometriosis, rheumatoid arthritis, cross-sectional study
Introduction
Endometriosis (EM) is a chronic, complex, estrogen-dependent, and progressive gynecological disorder presented as the growth of endometrial tissue outside the uterine cavity.1,2 The origins of EM remain intricate and unexplored, however, the immune system abnormalities observed in women with EM have consistently been proven, potentially indicating a persistent inflammatory reaction to the existence of ectopic endometrium.3,4 Rheumatoid arthritis (RA) is an autoimmune, chronic, and inflammatory joint and systemic disease mediated by autoantibodies targeting immunoglobulin G (rheumatoid factor) and/or citrullinated proteins, characterized by synovial inflammation, pannus formation, articular cartilage destruction, and bone erosion.5–7 RA mainly occurs in people aged 20 to 50 years, and approximately 1% of the world’s population has RA, with a female preponderance.8 RA imposes a substantial burden on patients, resulting in ranging from pain and disability to premature mortality, associated comorbidities, decreased quality of life, and increased financial costs.9 Therefore, exploring the factors associated with EM-related RA in women is very important for the management of RA in the future.
Epidemiological evidence indicates a correlation between EM and an elevated risk of developing RA in women, and inflammation and oxidative stress may be one of the possible pathological mechanisms between EM and RA.4,10,11 Antioxidants possess the capability to eliminate free radicals and impede lipid peroxidation, thereby safeguarding the body against oxidative damage.12 Vitamin A, vitamin C, vitamin E, zinc, selenium, and magnesium are essential nutrients that function as antioxidants in the human body.13 A previous study indicated that a higher magnesium intake may be inversely associated with the risk of RA among US adults.14 Another study found that vitamin E supplementation can improve symptoms of RA and improve patients’ quality of life.15 However, dietary nutrients tend to be simultaneously present, and it is more clinically relevant to study the intake of multiple dietary antioxidants than to study a single antioxidant. The Composite Dietary Antioxidant Index (CDAI) is a composite estimate of an individual’s overall pro- and antioxidant exposure status.16 A previous study has shown that CDAI was significantly negatively correlated with levels of markers of oxidative stress and inflammation such as interleukin-1beta (IL-1β) and tumor necrosis factor-alpha (TNF-α).17 The association between CDAI and RA warrants evaluations. In addition, studies focusing on the association between CDAI and the risk of EM-related RA in women of childbearing age were limited.
The aim of the study was to analyze the association between EM, CDAI and RA risk in women of childbearing age and evaluate the role of CDAI in EM-related RA risk in women of childbearing age. This study may provide a reference for the management of EM-related RA in women of childbearing age.
Methods
Study Design and Population
This study is a cross-sectional analysis utilizing data from the National Health and Nutrition Examination Survey (NHANES) database spanning 1999 to 2006. NHANES, conducted by the National Center for Health Statistics (NCHS), is an ongoing, independent, nationally representative cross-sectional survey of non-institutionalized US civilian populations. It is administered every two years and primarily aims to assess the health and nutritional status of adults and children in the United States. Details of study implementation are available for online access NHANES Questionnaires, Datasets, and Related Documentation (cdc.gov). For this study, participants were selected based on the following criteria: (1) women of childbearing age (between 20 and 44 years old) with assessments of EM; (2) individuals with assessments of RA; (3) individuals with complete dietary intake information in the NHANES database. The exclusion criteria consisted of (1) individuals with extremely low or high total energy intake (<500 kcal/day or >5000 kcal/day); and (2) individuals with missing information on key covariates. Data collection procedures for NHANES were authorized by the NCHS Ethics Review Board, and participants provided written informed consent.
Data Collection and Variable Assessments
Data extracted from the database included: (1) baseline characteristics: age (years), race, educational level, body mass index (BMI, kg/m2), marital status, poverty-to-income ratio (PIR), drinking and smoking status, physical activity, age at menarche, gravidity, and pregnancy status; (2) comorbidities: uterine fibroids, diabetes, hypertension, and dyslipidemia; (3) family history: family history of arthritis; (4) treatments: surgery, and female hormones use; (5) dietary intakes: energy (kcal), protein (gm), carbohydrate (gm), total fat (gm), and CDAI.
Race was categorized into three groups: White, Black, and Other. Education level was divided into three groups: middle school, high school, and university. Marital status included the categories of “Married” and “Unmarried”. PIR is a ratio of family income to the poverty threshold; out of which two levels of PIR were derived: <5, and ≥5. Drinking status was defined based on answers to questions regarding having had at least 12 drinks in the past year (ALQ101). According to ALQ120Q and ALQ120U, the drinking status was divided into <1 time/week, ≥1 time/week, No, and Yes. Participants who answered “yes” to question SMQ020 “Have you/Has SP smoked at least 100 cigarettes in your/his/her entire life?” was a smoker; otherwise, smoking status was defined as No. Physical activity was converted to metabolic equivalent (MET), which was calculated according to the physical activity questionnaire (PAQ) in NHANES. Energy expenditure (MET·min)= recommended MET x exercise time of corresponding activity (min). The age of menarche was extracted according to RHQ010. Gravidity was determined by the questionnaire RHQ170- pregnancies resulting in live births. “Has a doctor or other health professional ever told you that you had uterine fibroids?” (RHQ380) was used to determine uterine fibroids. RHQ140/RHQ141/RHD143 or pregnancy test-urine (URXPREG) was used to determine the current status of pregnancy. Laboratory tests, self-reports, and medication history were used to determine whether the subjects had diabetes or hypertension. Diabetes was defined as fasting blood glucose ≥ 7.0 mmol/L or Glycosylated Hemoglobin (HbAlc) ≥ 6.5% or self-reported diabetes or receiving hypoglycemic therapy. Hypertension was defined as a systolic blood pressure >130 mmHg or diastolic blood pressure >80 mmHg, or self-reported hypertension, or taking antihypertensive drugs. Dyslipidemia was diagnosed by fasting total cholesterol (TC) ≥5.2 mmol/L, low-density lipoprotein cholesterol (LDL-C) ≥3.4 mmol/L, high-density lipoprotein cholesterol (HDL-C) <1.0 mmol/L, or triglycerides (TG) ≥1.7 mmol/L, and/or receiving lipid-lowering medications.
Assessments of CDAI and EM
The CDAI was calculated based on six dietary antioxidant micronutrients, including vitamin A, vitamin C, vitamin E, zinc, magnesium, and selenium.18 The CDAI was obtained by summing the standardized Z-values of the dietary intake amounts of vitamin A, vitamin C, vitamin E, zinc, magnesium, and selenium, calculated as follows:

The calculated combined CDAI were categorized into two groups according to the median Q2 (−0.65): <Q2 (lower level intake), ≥Q2 (higher level intake). EM was diagnosed based on a questionnaire-based survey asking: “Has a doctor or other health professional ever told you that you had EM (age at interview 20–54 years)?”
Outcome
The outcome of this study was the presence of RA. RA was defined as a positive response to the question: “Has a doctor or other health professional ever told you/SP that you/s/he had arthritis?” “Which type of arthritis was it”.
Statistical Analysis
Weighted analysis was conducted on all data using WTMEC2YR, SDMVPSU, and SDMVSTRA from the NHANES database. WTMEC2YR represented the two-year sample weighed. SDMVPSU was a masked variance unit pseudo-PSU variable for variance estimation. SDMVSTRA was a masked variance unit pseudo-stratum variable for variance estimation. Continuous data were described by Mean and standard error Mean (S.E), and group comparisons were made using a weighted t-test. Counting data were presented as the number of cases and their proportion (N (%)), with group comparisons performed using the chi-square (χ2) test.
A propensity score matching (PSM) analysis with a 1:3 ratio and a caliper of 0.1 was conducted to balance significant differences in characteristics between patients with and without RA. PSM was employed to mitigate selection bias in retrospective observational studies.19 The univariate and multivariable weighted logistic analyses were performed to explore the association between EM, CDAI and RA, and the interaction association of CDAI and EM with RA. In the multivariable weighted logistic model, Model 1 was not adjusted for any confounders. Age, drinking status, smoking status, pregnancy status, and diabetes were adjusted in Model 2. Additive interaction was evaluated using three indicators: the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP), and the synergy index (S). RERI > 0, AP > 0, or S > 1 were considered indicative of significant additive interaction.20 The odds ratio (OR) and its 95% confidence interval (CI) were chosen as evaluation indices. Statistical significance was set at alpha = 0.05. A P-trend test was used to determine if there was a statistically significant trend among disease category groups. Data cleaning and data analysis using R version 4.3.0 (2023–04-21 ucrt); the baseline table was generated using SAS 9.4.
Results
Basic Characteristics of the Included Population
In total, 4970 women of reproductive age from 1999 to 2006 were collected from the NHANES database. Based on the inclusion and exclusion criterion, 3803 patients were included in this study. The diagram flow of the patients’ collection is depicted in Figure 1. Table 1 shows the basic information of the included study population and compares the differences in population with and without EM. The mean age of the included population was 31.68 (0.17) ages. In terms of racial composition, White individuals constitute 65.75%, Black individuals account for 12.36%, and other racial groups make up 21.89%. More than half of the individuals (62.72%) possessed a university-level education. The total number of married population in the study is 1420, representing 38.20% of the total participants. The number of participants with RA is 74, representing 1.99% of the total group. There were significant differences in age, race, education, marital status, gravidity, uterine fibroids, surgery, diabetes, female hormone use, family history of arthritis, and RA between populations with and without EM (All P <0.05).
 |
Table 1 The Basic Information of the Included Study Population |
 |
Figure 1 A diagram flow describing the patients’ selection. NHANES, National Health and Nutrition Examination Survey. |
Association of CDAI and EM with the Risk of RA
The associations of CDAI, and EM with RA are presented in Table 2. A lower CDAI (OR: 1.85, 95% CI: 1.12 to 3.04, P= 0.015) and the presence of EM (OR: 3.05, 95% CI: 1.19 to 7.81, P= 0.023) was associated with the risk of RA.
 |
Table 2 Association of CDAI, and EM with the Risk of RA |
Coexistence of CDAI and EM on the Risk of RA
The results of the interaction between CDAI and EM on the risk of RA are shown in Table 3. The result demonstrated an additive interaction of a lower CDAI and the presence of EM on the risk of RA (OR: 6.19, 95% CI: 2.33 to 16.43, P <0.001, P of trend =0.007). Nevertheless, there was no significant additive interaction after being assessed by the RERI, AP, and S (Table 4). We further assessed the joint effect of CDAI and EM on the risk of RA. A lower CDAI and the presence of EM were associated with the risk of RA (OR: 3.94, 95% CI: 1.35 to 11.51, P= 0.013). The joint effect of CDAI and EM on the risk of RA is shown in Table 5.
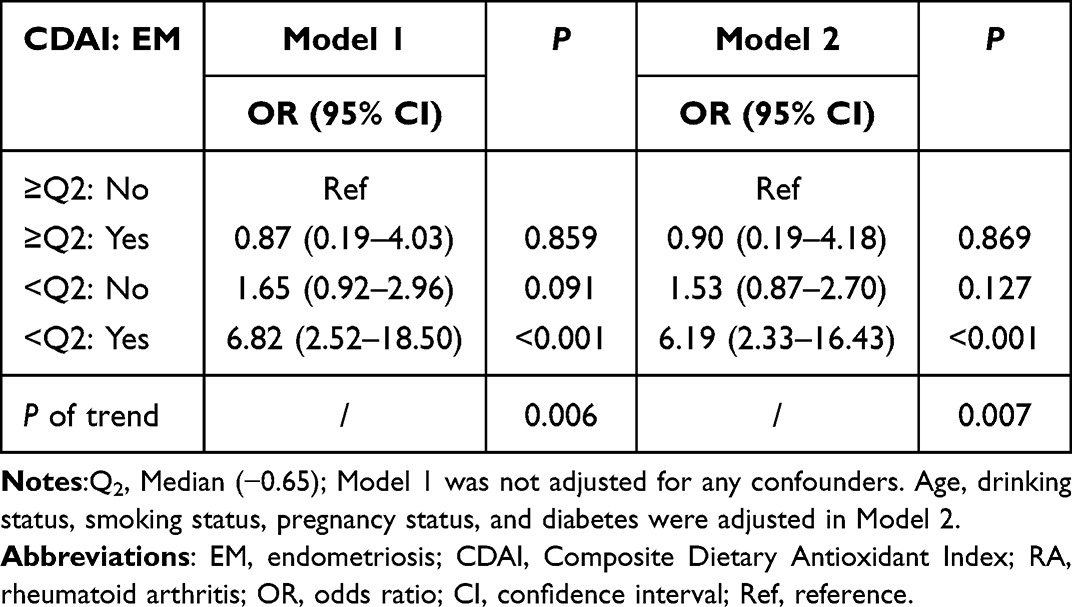 |
Table 3 The Interaction Between CDAI and EM on the Risk of RA |
 |
Table 4 Evaluations of the Additive Interaction Results |
 |
Table 5 Coexistence of CDAI and EM on the Risk of RA |
Discussion
In the current research, utilizing a public database, we assessed both the individual and combined impacts of CDAI and EM on RA risk among women of childbearing age. The study revealed a correlation between a lower CDAI score and an increased risk of RA, and an association between EM and risk of RA. Our study also identified that the coexistence of EM and low CDAI score was related to the risk of RA among women of childbearing age, and there may be a synergistic effect.
Previous studies have confirmed the association between antioxidant intake/consumption/level and the risk of RA. In a cross-sectional analysis involving 87 individuals suffering from active RA, certain antioxidant micronutrients alleviate inflammatory conditions and improve the function of antioxidant enzymes in these individuals.21 In a Mendelian randomization analysis carried out by Cheng et al, higher blood magnesium levels were associated with an 8.94 times greater risk of developing RA.22 In research utilizing data from NHANES spanning 2003 to 2018, increased magnesium consumption might be inversely related to RA risk in the adult population of the United States.14 This study demonstrated that the composite measurement of dietary total antioxidant consumption from food (CDAI) was associated with an increased risk of RA. Earlier investigations have also documented links between CDAI and diverse diseases. A study using data from the NHANES database reported that CDAI was inversely associated with gout in US adults.23 Results from the Singapore Chinese Health Study indicated that an elevated CDAI correlated with a reduced likelihood of colorectal cancer onset.16 The research by Chen et al demonstrated a negative correlation between CDAI and diabetes incidence.24 The underlying process is intimately connected to oxidative stress. CDAI, which assesses total dietary antioxidant intake from food, shows an inverse relationship with the levels of inflammatory cytokines like IL-1β and TNF-α.17 This implies that the impact of CDAI might be mediated through its anti-inflammatory properties. However, the exact molecular mechanisms remain unclear, necessitating further investigation.
In the present study, the presence of EM was associated with the risk of RA, which was supported by the previous studies. In a nationwide population-based cohort study, individuals with EM were found to have a heightened risk of developing RA.11 A study systematically reviews the literature on population-based studies exploring the relationship between EM and autoimmune diseases and notes a correlation between EM and such diseases.4 Epidemiological data have suggested similarities observed in molecular and cellular pathways of EM and RA,10 which may indicate a partially shared genetic background between the two diseases. The systemic inflammation is also believed to provide an outline of the association between RA and EM.25 To gain deeper insights into the relationship between EM and RA, it is essential to conduct comprehensive prospective studies on a large scale that incorporate robust controls for confounding variables and include precise quantification of mediation. Additionally, detailed genetic and biological research is necessary. This approach will help clarify whether EM acts as a risk factor for RA, is a result of RA, or if these conditions have overlapping pathophysiological mechanisms.
Although an additive interaction of a lower CDAI and the presence of EM on the risk of RA was not observed, the coexistence of EM and low CDAI score was related to an increased risk of RA. The direct connection between EM, low CDAI scores, and an increased risk of RA has not been explicitly confirmed in the literature. However, based on current research, it can be hypothesized that the relationship between EM, low CDAI scores, and increased RA risk may be attributed to the individual relationships of EM and low CDAI scores with the risk of RA. To accurately establish this association, more specialized research and data are required. This finding may indicate the benefit of appropriate antioxidant intake to the risk of EM-associated RA.
This study found that the lower intake level of the combination of various dietary antioxidants is associated with the risk of EM-related RA, providing a reference for the antioxidant intake in daily management of the risk associated with EM-related RA. This contributes to the reduction of the incidence of EM-related RA and minimizes its adverse impacts. In addition, the estimation of the CDAI offers further insights, as it can identify and categorize potential antioxidant sources in a complex diet, thereby enabling the classification of diets and individuals based on antioxidant intake.
This study possesses the following advantages: first, this study investigates the intake of multiple dietary antioxidants, which, compared to previous studies focusing on single antioxidants, offers greater clinical relevance; second, the NHANES samples were obtained through multi-stage complex sampling, ensuring better representativeness. This study also has limitations. First, as with all cross-sectional studies, we only observed the relationship between CDAI and the risk of RA, and causality cannot be determined. Second, the questionnaire survey was inevitably subject to recall bias. Third, the lifestyle of the study subjects, especially their diet, may change, but due to database limitations, it is not possible to assess the potential impact of these changes on the outcomes. Future well-designed prospective studies are still needed to validate our results.
Conclusion
The CDAI, and EM individually was associated with the risk of RA in women of reproductive age. An association between a lower CDAI and the risk of EM-related RA was also observed. This study elucidates the importance of daily antioxidant intake for EM-related RA.
Ethics Approval and Informed Consent
The requirement of ethical approval for this was waived by the Institutional Review Board of Affiliated Hospital of Jining Medical University, because the data was accessed from NHANES (a publicly available database). The need for written informed consent was waived by the Institutional Review Board of Affiliated Hospital of Jining Medical University due to retrospective nature of the study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quesada J, Härmä K, Reid S, et al. Endometriosis: a multimodal imaging review. Eur J Radiol. 2023;158:110610. doi:10.1016/j.ejrad.2022.110610
2. Zizolfi B, Foreste V, Gallo A, Martone S, Giampaolino P, Di Spiezio Sardo A. Endometriosis and dysbiosis: state of art. Front Endocrinol (Lausanne). 2023;14:1140774. doi:10.3389/fendo.2023.1140774
3. Lamceva J, Uljanovs R, Strumfa I. The main theories on the pathogenesis of endometriosis. Int J Mol Sci. 2023;24(5):4254. doi:10.3390/ijms24054254
4. Shigesi N, Kvaskoff M, Kirtley S, et al. The association between endometriosis and autoimmune diseases: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(4):486–503. doi:10.1093/humupd/dmz014
5. Finckh A, Gilbert B, Hodkinson B, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. 2022;18(10):591–602. doi:10.1038/s41584-022-00827-y
6. Smolen JS, Aletaha D, Barton A, et al. Rheumatoid arthritis. Nat Rev Dis Primers. 2018;4:18001. doi:10.1038/nrdp.2018.1
7. Jang S, Kwon EJ, Lee JJ. Rheumatoid arthritis: pathogenic roles of diverse immune cells. Int J Mol Sci. 2022;23(2):905. doi:10.3390/ijms23020905
8. Gowhari Shabgah A, Shariati-Sarabi Z, Tavakkol-Afshari J, Ghasemi A, Ghoryani M, Mohammadi M. A significant decrease of BAFF, April, and BAFF receptors following mesenchymal stem cell transplantation in patients with refractory rheumatoid arthritis. Gene. 2020;732:144336. doi:10.1016/j.gene.2020.144336
9. Shen H, Jin L, Zheng Q, et al. Synergistically targeting synovium STING pathway for rheumatoid arthritis treatment. Bioact Mater. 2023;24:37–53. doi:10.1016/j.bioactmat.2022.12.001
10. Zervou MI, Vlachakis D, Papageorgiou L, Eliopoulos E, Goulielmos GN. Increased risk of rheumatoid arthritis in patients with endometriosis: genetic aspects. Rheumatology. 2022;61(11):4252–4262. doi:10.1093/rheumatology/keac143
11. Chen SF, Yang YC, Hsu CY, Shen YC. Risk of rheumatoid arthritis in patients with endometriosis: a nationwide population-based cohort study. J Womens Health. 2021;30(8):1160–1164. doi:10.1089/jwh.2020.8431
12. Pisoschi AM, Pop A, Iordache F, Stanca L, Predoi G, Serban AI. Oxidative stress mitigation by antioxidants - An overview on their chemistry and influences on health status. Eur J Med Chem. 2021;209:112891. doi:10.1016/j.ejmech.2020.112891
13. Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst Rev. 2012;2012(3):Cd007176. doi:10.1002/14651858.CD007176.pub2
14. Fang J, Cao T, Liu C, et al. Association between magnesium, copper, and potassium intakes with risk of rheumatoid arthritis: a cross-sectional study from National Health and Nutrition Examination Survey (NHANES). BMC Public Health. 2023;23(1):2085. doi:10.1186/s12889-023-16906-y
15. Kou H, Qing Z, Guo H, Zhang R, Ma J. Effect of vitamin E supplementation in rheumatoid arthritis: a systematic review and meta-analysis. Eur J Clin Nutr. 2023;77(2):166–172. doi:10.1038/s41430-022-01148-9
16. Yu YC, Paragomi P, Wang R, et al. Composite dietary antioxidant index and the risk of colorectal cancer: findings from the Singapore Chinese health study. Int J Cancer. 2022;150(10):1599–1608. doi:10.1002/ijc.33925
17. Luu HN, Wen W, Li H, et al. Are dietary antioxidant intake indices correlated to oxidative stress and inflammatory marker levels? Antioxid Redox Signal. 2015;22(11):951–959. doi:10.1089/ars.2014.6212
18. Zhang R, Ni Z, Wei M, et al. Composite dietary antioxidant intake and osteoporosis likelihood in premenopausal and postmenopausal women: a population-based study in the United States. Menopause. 2023;30(5):529–538. doi:10.1097/GME.0000000000002173
19. Wen H, Niu X, Hu L, et al. Dietary copper intake and risk of myocardial infarction in US adults: a propensity score-matched analysis. Front Cardiovasc Med. 2022;9:942000. doi:10.3389/fcvm.2022.942000
20. Andersson T, Alfredsson L, Källberg H, Zdravkovic S, Ahlbom A. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20(7):575–579. doi:10.1007/s10654-005-7835-x
21. Arablou T, Aryaeian N, Djalali M, Shahram F, Rasouli L. Association between dietary intake of some antioxidant micronutrients with some inflammatory and antioxidant markers in active Rheumatoid Arthritis patients. Int J Vitam Nutr Res. 2019;89(5–6):238–245. doi:10.1024/0300-9831/a000255
22. Cheng WW, Zhu Q, Zhang HY. Mineral nutrition and the risk of chronic diseases: a Mendelian randomization study. Nutrients. 2019;11(2):378. doi:10.3390/nu11020378
23. Hu W, Ye Z, Li T, Shi Z. Associations between composite dietary antioxidant index and gout: national health and nutrition examination survey 2007–2018. Biol Res Nurs. 2024; 26(1);150–159. doi:10.1177/10998004231198166
24. Chen X, Lu H, Chen Y, Sang H, Tang Y, Zhao Y. Composite dietary antioxidant index was negatively associated with the prevalence of diabetes independent of cardiovascular diseases. Diabetology & Metabolic Syndrome. 2023;15(1):183. doi:10.1186/s13098-023-01150-6
25. Chen CJ, Livneh H, Chen WJ, et al. The prescription of Chinese herbal medicine and risk of endometriosis in women with rheumatoid arthritis: a population-based cohort study. Int J Womens Health. 2022;14:1603–1612. doi:10.2147/IJWH.S386134
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.