")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Barriers and Facilitators to Utilization of Community Drug Distribution Points Among People Living with HIV in Bushenyi District, South-Western Uganda: A Qualitative Study
Authors Oyet D, Niyonzima V , Akol G, Onyait E, Twinomugisha D, Kawala Wambera D, Wakida EK , Obua C
Received 19 May 2023
Accepted for publication 12 October 2023
Published 16 October 2023 Volume 2023:15 Pages 633—640
DOI https://doi.org/10.2147/HIV.S422040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
David Oyet,1 Vallence Niyonzima,1 Gideon Akol,2 Emmanuel Onyait,1 Daphine Twinomugisha,3 Doreen Kawala Wambera,4 Edith K Wakida,5,6 Celestino Obua7
1Department of Nursing, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Medical Laboratory Sciences, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 3Department of Pharmaceutical Sciences, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 4Department of Physiotherapy, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 5Department of Medical Education, California University of Science and Medicine, Colton, CA, USA; 6Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 7Mbarara University of Science and Technology, Mbarara City, Uganda
Correspondence: Vallence Niyonzima, Department of Nursing, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda, Tel +256777842830, Email [email protected]
Introduction: People living with HIV (PLHIV) still have challenges in accessing HIV services in low- and middle-income countries (LMIC). In Uganda, community drug distribution points (CDDPs) are part of interventions to improve access to anti-retroviral medications. However, there is still low enrollment in CDDPs among PLHIV in south-western Uganda, particularly in Bushenyi district. This study explored the barriers and facilitators to the utilization of CDDPs among PLHIV.
Methods: This was a descriptive qualitative study utilizing a qualitative approach. We purposively recruited 24 PLHIV and 6 Primary healthcare providers as key informants. We conducted in-depth interviews with PLHIV and key informant interviews with Primary healthcare providers using an interview guide. The audio recordings were transcribed verbatim to Rukiga-Runyankore and then translated into English. Data were coded and analyzed using thematic analysis.
Results: Seven themes were developed describing drivers for the utilization of CDDPs. These were broadly categorized into facilitators and barriers. The main facilitators of the utilization of CDDPs were peer support, positive Primary healthcare providers’ attitudes, satisfaction with HIV services, and accessibility of ART services. The main barriers were stigma, lack of physical infrastructure, and lack of comprehensive services.
Conclusion and Recommendation: Utilization of CDDPs is facilitated by accessibility and Primary healthcare providers’ attitude. Stigma is still a limitation to the utilization of HIV services. We recommend that Ministry of Health and other development partners should improve physical infrastructural facilities at the CDDP sites so that the privacy and confidentiality of the PLHIV are protected. Focus on interventions to eliminate stigma by Primary healthcare providers and other stakeholders at CDDP sites is urgently needed.
Keywords: community drugs distribution points, barriers, facilitators, Southwestern Uganda, qualitative study, people living with HIV
Introduction
The Global HIV and AIDS statistics fact sheet1 reported that HIV is still a public health concern with a global prevalence of 37.7 million people living with HIV (PLHIV) of which 95.2% are adults. In sub-Saharan Africa, by 2020, the new HIV infections had declined by 38%. However, only 72% of PLHIV were on ART, and only 65% had suppressed viral load.2 Delivery of HIV services is still a burden especially in low-income countries where not all PLHIV have access to ART. In 2020, the ART coverage was at 73% globally and 83% for Uganda, which is still below the UNAIDS, target. In Uganda, the prevalence of HIV is 6.2% among adults which is approximately 1.2 million adults.3
Changes in service delivery models can improve program quality and efficiency in HIV care4 and the UNAIDS target of enrolling 95% of PLHIV on ART are achievable even in resource-constrained settings with a high HIV burden.5,6 Models used to provide ART services to PLHIV include a differentiated service delivery model (DSDM), community ART group, community client-led ART delivery (CCLAD), fast-track drug pick up, and community drug distribution points (CDDP).7 CDDP model is where ART services are delivered and distributed at community-based site by primary healthcare providers. This model was introduced in 2006 to decongest health facilities and increase ART adherence and ART coverage.8 The World Health Organisation recommended that community-based models of ART delivery be used to support ART expansion and retention in resource-limited settings.9
A study in East and Central Uganda found that more PLHIV enrolled in CDDP than in other differentiated service delivery models.10 During the COVID-19 lockdown, ART delivery was best done by community-based ART delivery models due to patients’ demand.11 Currently, ART coverage in Uganda is currently at 83%, and some facilities are overcrowded with PLHIV seeking ART services. This may be due to some challenges that the CDDP model may have where, for example, studies done in Uganda8 and South Africa12 found that stigma was a barrier to the utilization of the CDDP model among PLHIV. Stigma can potential be reduced through forming ART groups as was done in South Africa and Ghana, and by providing counseling and education to the patients and the community.13
South Western Uganda has HIV prevalence of 6.7% and a 4.2% incidence rate14 which is higher than the national prevalence of 6.2%. In addition, there is reduced enrollment of stable PLHIV into the CDDP models in South Western Uganda. For example, a review of HIMS records at Kyabugimbi health Centre IV (HCIV), Bushenyi District, out of the 387 PLHIV who were categorized as stable in their files, only 57 were enrolled in CDDP. This low enrolment to the CDDP in addition to overcrowding in the ART clinics still occurs and yet the model was introduced to take HIV services closer to the patients with the ultimate goal to decongest the health facilities. Therefore, this study explored the barriers and facilitators to the utilization of CDDP among PLHIV in Southwestern Uganda.
Methods
Study Design and Setting
This was a descriptive qualitative study conducted at Bushenyi Health Centre IV, and Kyabugimbi Health Centre IV in Bushenyi district south-western Uganda. There are 45 health facilities, with 29 government owned (2 HCIVs, 11 HCIIIs, and 16 HCIIs) and 13 private owned (3 hospitals, 3 HCIIIs and 7 HCIIs) (Bushenyi District Local Government, 2021). The two health centres were chosen because they serve a large number of HIV clients.
Population and Sample Size
The study was conducted at three health facilities that provided CDDP ART services in the district. All Primary healthcare providers (Key informants) in the selected facilities that participate in the CDDP program were all included. These were eligible for the study because of their experience in implementing the CDDP model. Additionally, 24 PLHIV accessing ART services from the CDDPs linked to the selected health facilities were also included in the study.
Sampling and Eligibility Criteria
We selected the health facilities that provided CDDP services to their clients; purposively included the primary healthcare providers who directly participated in the provision of the ART services; and the PLHIV who utilized the CDDP points and had been accessing therapy from these sites for at least 10 weeks.
Data Collection Procedure
Data were collected using two separate tools, an in-depth interview guide for PLHIV and a key informant interview guide for primary healthcare providers. The data collection tools were developed using information from previous published studies guided by the study objectives.15–17 The tools were pretested at a health facility not included in the study and adjusted prior to field data collection. Data from the pretest was used to refine the data collection tools. Data was collected by two research assistants with a background in social science and previous experience in conducting qualitative studies. The key informant interview guide collected data on the following areas; socio-demographic characteristics, quality of HIV care with the CDDP, and the drivers of utilization of the CDDP model such accessibility, attitudes of health workers, availability of drugs among others. The in-depth interview guide collected data on socio-demographic characteristics, barriers and facilitators of CDDP utilization for ART services.
Data collection was conducted by two research assistants who were trained on the study protocol and study tools prior to field data collection. A written informed consent was obtained from each study participant (Primary healthcare providers and PLHIV) prior to recruitment into the study.
Data Management and Analysis
Interviews were audio-recorded on a digital voice recorder, and field notes were taken during the interviews. At the end of each day of data collection, researchers listened to recorded interviews. The interviews were transcribed verbatim into Microsoft word documents. The transcripts were read and re-read for familiarization and compared with the recordings for consistency. To ensure quality, a different person who was not involved in interviewing the participants translated, cleaned and coded the transcripts. Three researchers (DO, VN and EO) reviewed and harmonized the codes. Similar codes were grouped to form sub-themes. Disagreement between the reviewers was resolved through discussion and consensus. Finally, related sub-themes were merged to form themes that describe the drivers of the utilization of CDDPs. Data were analyzed using thematic analysis.
Results
Sociodemographic Characteristics of Study Participants
In this study, in-depth interviews were conducted among 24 PLHIV receiving ART from the CDDPs. Additionally, key informant interviews were conducted amongst all the Primary healthcare providers (06) from health facilities in Bushenyi who participate in the provision of HIV care extension services to communities (06). The majority (60%) of the participants were in the age range of 20–40 years and the age ranged from 18 to 83 years. The mean age was 36.4 (standard deviation 2.6). Over a half (57%) of the participants were female (Table 1).
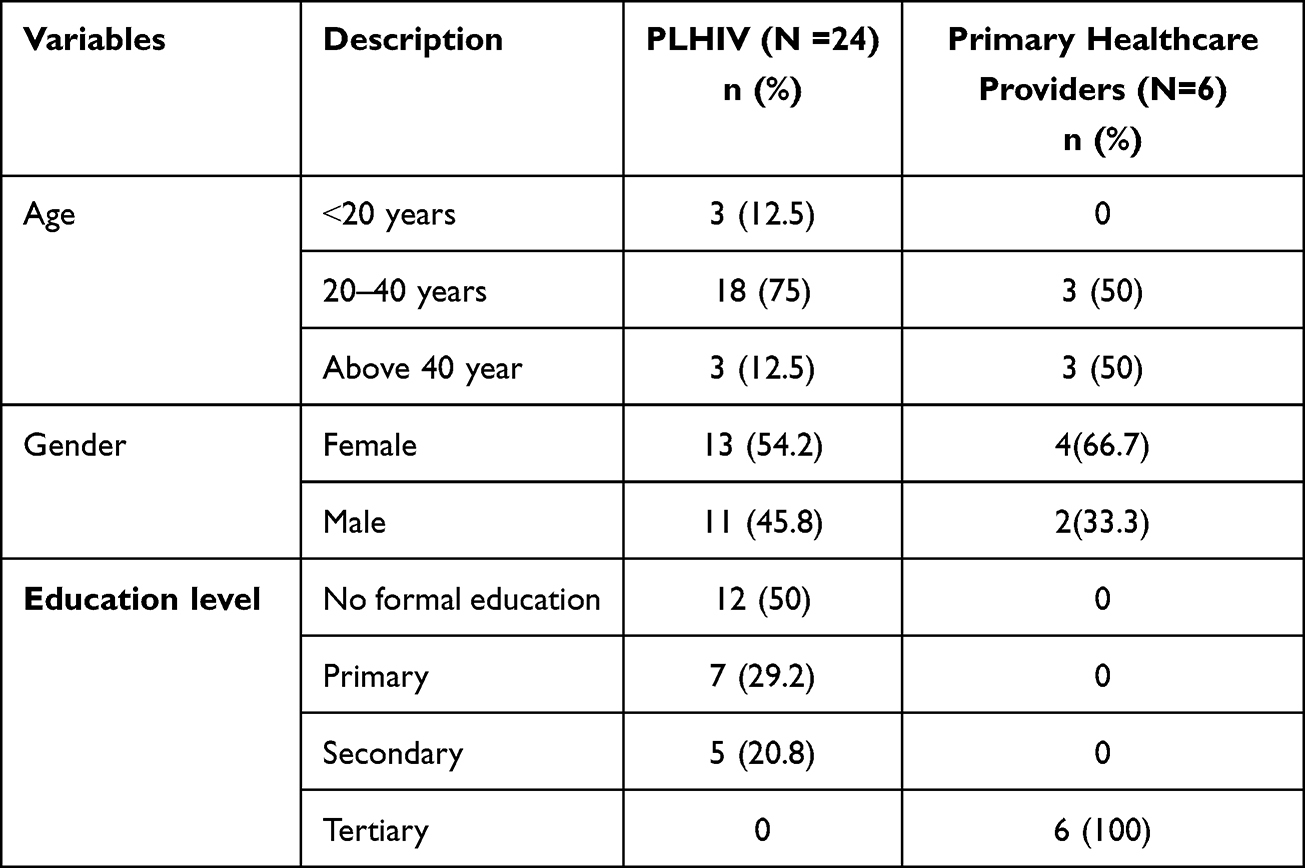 |
Table 1 Sociodemographic Characteristics of PLHIV Accessing ART Services in CDDP Points (N = 24) and Primary Healthcare Providers in the Linked Facilities (N = 6) in Bushenyi District |
Drivers of CDDP Utilization by PLHIV in Bushenyi District South Western Uganda
From the analysis of data, seven themes were developed. These themes were broadly classified into barriers and facilitators of CDDP utilization.
Facilitators of CDDP Utilization
The major facilitators to the utilization of CDDPs reported by most participants (both PLHIV and Primary healthcare providers) were presented under the following themes: patients’ satisfaction, peer influence, positive Primary healthcare providers’ attitude, and accessibility.
Perceived Patients’ Satisfaction with ART Services at the CDDP Sites
Patients’ satisfaction with the services at the CDDP sites made them continue getting services from the CDDPs. Most participants reported that the services are accessible, drugs were always available, and they get enough drugs for HIV and other care like counselling. Counselling gave them comfort and hope to live. Some PLHIV also reported that they get sufficient time with primary healthcare providers and the waiting time is generally short. Some participants also expressed that they are going to live longer because of the services they are getting from the CDDPs. Even the Primary healthcare providers also reported that the patients have trust in them and like their services.
If maybe you feel dizzy after taking the medicine you tell him and he gives you his time and attention, so you feel really happy. From the time I came here no health worker has ever treated me badly because if I ask you something that I hadn’t understood and you explain it well for me, I appreciate. Participant 14
Peer Support
From in-depth interviews, PLHIV highlighted that peer support motivated them to be enrolled in the CDDP. Some PLHIV reported that they were convinced by their friends to go and enrol in the CDDP. Some PLHIV also said it was their friends who encouraged them to be tested from CDDP and after testing positive, they were enrolled in CDDP. PLHIV also expressed that they normally tell their colleagues in the village to come for a refill from the CDDP. Primary healthcare providers also reported that PLHIV normally go and tell their friends in the community about the services at the CDDP and that is why they are many who have enrolled in CDDP.
It is our clients that are attracting more people to come after telling them about the good services and we also try to incorporate HIV testing so that we can also identify new patients. Key informant 03
Primary Healthcare Providers’ Attitude
From in-depth interviews, PLHIV reported that they were motivated to continue receiving services from the CDDPs because of Primary healthcare providers’ positive attitudes. PLHIV expressed that the Primary healthcare providers are good, friendly, kind, and polite to them.
Primary healthcare providers of the CDDP program are so good, friendly, faster and they treat us very well even though some of us patients are not well behaved and we inconvenience Primary healthcare providers while doing their work. Participant 02
Accessibility to the CDDP Sites by PLHIV
The CDDPs were closer to the closer to the PLHIV and thus would incur low out of pocket expenditure such as low transport costs. The Primary healthcare providers also reported that PLHIV used to miss visits at the facility due to the long distance to the facility from their homes.
People are poor meaning they could not afford the high transport costs that were involved, a lot of people in this community are poor and they even cannot afford to support themselves in terms of financial stability. Key informant 03.
Barriers to CDDP Utilisation
The barriers identified include stigma, lack of infrastructure, and lack of comprehensive services.
Stigma
Our study participants reported that stigma exists among some patients who do not want to disclose their status. Participants expressed that this stigma discouraged some patients from being enrolled in the CDDP so that their peers do not see them. Furthermore, participants expressed that whenever they are seen coming from the CDDP, they are associated with PLHIV. Both in-depth and key informant interviews highlighted the fact that some PLHIV have not disclosed their positive HIV status and are always stigmatized when they visit the CDDP sites. Some PLHIV reported that community members talk ill about them whenever they visit the CDDP sites.
…. Such people talk a lot when they see us at the CDDP points, they always associate you with HIV and it somehow scares us…. We usually line outside in the open with too much sun and sometimes it rains on us, it is somehow discouraging and demotivating … (18-year Female participant 1)
Lack Physical Infrastructure
From the in-depth and key informant interviews, the respondents commonly highlighted the lack of infrastructure at the CDDP sites as a major barrier to access of ART services.
…. The biggest challenge here is that we do not have a shelter, we are so many and exposed to passers-by near the road, and we need some kind of privacy, safety, and confidentiality. Participant 04
Lack of Comprehensive Services
From both in-depth and key informant interviews, participants highlighted the lack of comprehensive services at the CDDP sites as a barrier to ART access. Some PLHIV reported that they would wish to have other services like TB screening and treatment for other conditions at the CDDP point. Primary healthcare providers also reported that they are unable to take a comprehensive service to the community because of limited resources such as staff shortages, limited finances, and lack of transport means.
…there are costs in delivering the CDDP model like transport, then also is fuel and facilitation of staff. We cannot have other services at the site because we lack enough staff so we advise them to come to the facility where different services are offered. Key informant 02
Discussion
The PLHIV and key informants in this study identified some barriers to CDDP utilization including stigma, lack of infrastructural facilities, and lack of comprehensive services. Such barriers must be mitigated to improve CDDP utilization in rural communities in rural South Western Uganda.
Our study found that stigma was commonly reported as a barrier to utilisation of ART services at the CDDP sites in Bushenyi district. There was internalized stigma among some PLHIV who did not want to disclose their positive HIV status. This finding is consistent with those of previous studies done in South Africa and Uganda.17–19 This means stigma still limits some PLHIV from accessing HIV services and hence the low ART coverage in sub-Saharan Africa. Stigma at the individual level makes it difficult to implement care for patients by the Primary healthcare providers highlighting the need for targeted interventions against stigma among PLHIV accessing SRT care at the CDDP sites.
In addition, our study found that lack of physical infrastructure at the CDDP sites was a major limitation to the utilization of the CDDP by PLHIV. This finding is in line with those of previous studies done in Uganda.18,20 However, studies done in South Africa and Zimbabwe21,22 reported contrary findings, which could be an indicator of the challenges in the implementation of the CDDP model in the low- and middle-income country settings. This is likely to affect utilisation of CDDP sites as access points for ART services in most low- and middle-income countries.
Our study found that positive health workers’ attitudes are a facilitator of CDDP utilization. This is consistent with the findings of Opio et al.23 However, other authors12,22 reported that Primary healthcare providers had negative attitudes towards PLHIV. The difference in the results could be attributed to the fact that these studies reporting negative Primary healthcare providers’ attitudes were conducted when the model was just introduced. Positive Primary healthcare providers’ attitude is due to motivation in terms of incentives by the facility. This, therefore, implies that the motivation of Primary healthcare providers is important in the implementation of HIV care models.
Our study found that accessibility to ART services also facilitate the utilization of CDDPs. This is consistent with the findings of other previous studies in South Africa and Uganda.17,18,24 In addition, this study has highlighted the perceived satisfaction PLHIV get from interacting with Primary healthcare providers regularly within community settings. This concurs with findings from previous studies.9,25 CDDPs have therefore relieved from out-of-pocket expenses in terms of transport costs since ART services are brought closer to the community. However, this may imply that the cost of transport has been shifted to health facilities, which may be a challenge for health facilities with limited resources. Hence, it is not possible to implement the CDDP model of ART delivery.
Our study was limited by the fact that we collected from participants receiving services utilizing CDDP points and therefore we could have missed out views of those who do not utilize CDDPs. However, this did not significantly affect our findings since PLHIV using CDDPs and those who do not, live in the same community and constantly share views regarding choice on the point of ART access and the associated barriers and facilitators. In addition, the study involved only those who were accessing services from the CDDP points and therefore we are likely to have missed information regarding barriers from those who do not use the CDDP points.
Conclusions and Recommendations
Patients’ utilization of the CDDP as a strategy for HIV service delivery is facilitated by the positive attitude of Primary healthcare providers, low transport fares, and satisfaction with HIV services available at the CDDP site. Barriers such as lack of facility infrastructure, overcrowding, and stigma limit some PLHIV to access HIV services from CDDPs. We recommend that MOH and other development partners should improve physical infrastructural facilities at the CDDP sites so that the privacy and confidentially of the PLHIV who come for HIV services at the CDDP sites are protected. Focus on interventions to eliminate stigma by Primary healthcare providers and other stakeholders at CDDP sites is urgently needed.
Abbreviations
ART, Anti-retroviral therapy; CCLAD, Community Client-Led ART Delivery; CDDP, Community Drug Distribution Points; DHO, District Health Officer; DSD, Differentiated Service Delivery; HC, Health Centre; MOH, Ministry of Health; MUST, Mbarara University of Science and Technology; PEPFAR, President’s Emergency Plan for AIDS Relief; PLHIV, People Living with HIV; UNCST, Uganda National Council for Science and Technology.
Data Sharing Statement
The datasets generated and analyzed during the study are available from the corresponding author on request.
Ethical Approval and Consent to Participate
The protocol to conduct the study was approved by the Mbarara University of Science and Technology Research Ethic Committee (MUST -2021-279), and additional clearance to conduct the study was obtained from Uganda National Council for Science and Technology (UNCST). Administrative clearance was obtained from the district health officer (DHO) of Bushenyi district and the health facility in-charges of the selected health facilities. Written informed consent was obtained from each participant before the start of the interview. Participants also consented to publication of anonymized responses. The study was conducted following UNCST guidelines and the declaration of Helsinki.
Acknowledgments
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC) and the President’s Emergency Plan for AIDS Relief (PEPFAR)) of the National Institutes of Health under Award Number R25TW011210. We thank the participants who participated in this study, the District Health Officer Bushenyi District, and the administration of Ishaka Adventist Hospital, Bushenyi Health Center IV, and Kyabugimbi Health Center IV who contributed to the success of this study. We also acknowledge the contribution of Gabriel Nuwagaba, our research assistant, who helped to collect the data.
Funding
This study was funded by a grant from the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC) and the President’s Emergency Plan for AIDS Relief (PEPFAR)) of the National Institutes of Health under Award Number R25TW011210.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Global H. AIDS statistics—fact sheet| UNAIDS. Dostopno na; 2021. Available from: https://www.unaids.org/en/resources/fact-sheet.
2. Bain LE, Nkoke C, Noubiap J. UNAIDS 90–90–90 targets to end the AIDS epidemic by 2020 are not realistic: comment on “Can the UNAIDS 90–90–90 target be achieved? A systematic analysis of national HIV treatment cascades”. BMJ Glob Health. 2017;2(2):e000227.
3. Musumari PM, Techasrivichien T, Srithanaviboonchai K, et al. HIV epidemic in fishing communities in Uganda: a scoping review. PLoS One. 2021;16(4):e0249465. doi:10.1371/journal.pone.0249465
4. Kandasami S, Shobiye H, Fakoya A, et al. Can changes in service delivery models improve program quality and efficiency? A closer look at HIV programs in Kenya and Uganda. J Acquir Immune Defic Syndr. 2019;81(5):533. doi:10.1097/QAI.0000000000002064
5. Heath K, Levi J, Hill A S Reaching UNAIDS 95-95-95 targets worldwide: predicted benefits and treatment costs with generic manufacture. SSRN 3696865; 2021.
6. Gaolathe T, Wirth KE, Holme MP, et al. Botswana’s progress toward achieving the 2020 UNAIDS 90-90-90 antiretroviral therapy and virological suppression goals: a population-based survey. Lancet HIV. 2016;3(5):e221–e230. doi:10.1016/S2352-3018(16)00037-0
7. Grimsrud A, Bygrave H, Doherty M, et al. Reimagining HIV service delivery: the role of differentiated care from prevention to suppression. J Int AIDS Soc. 2016;19(1). doi:10.7448/IAS.19.1.21484
8. Zakumumpa H, Bennett S, Ssengooba F. Modifications to ART service delivery models by health facilities in Uganda in promotion of intervention sustainability: a mixed methods study. Implement Sci. 2017;12(1):1–14.
9. Adjetey V, Obiri-Yeboah D, Dornoo B. Differentiated service delivery: a qualitative study of people living with HIV and accessing care in a tertiary facility in Ghana. BMC Health Serv Res. 2019;19(1):1–7. doi:10.1186/s12913-019-3878-7
10. Baleeta K, Muhwezi A, Tumwesigye N, et al. Factors that influence satisfaction of People Living with HIV (PLHIV) with differentiated ART delivery models in East Central Uganda: a cross-sectional study; 2021.
11. Zakumumpa H, Tumwine C, Milliam K, Spicer N. Dispensing antiretrovirals during Covid-19 lockdown: re-discovering community-based ART delivery models in Uganda. BMC Health Serv Res. 2021;21(1):1–11. doi:10.1186/s12913-021-06607-w
12. Venables E, Towriss C, Rini Z, et al. Patient experiences of ART adherence clubs in Khayelitsha and Gugulethu, Cape Town, South Africa: a qualitative study. PLoS One. 2019;14(6):e0218340. doi:10.1371/journal.pone.0218340
13. Barker C, Dutta A, Klein KJ. Can differentiated care models solve the crisis in HIV treatment financing? Analysis of prospects for 38 countries in sub‐Saharan Africa. J Int AIDS Soc. 2017;20(Suppl 4):21648. doi:10.7448/IAS.20.5.21648
14. Munezero T, Mfitumukiza VJH. Utilization of HIV/AIDS Interventions and associated factors among young people aged 15–30 in Bushenyi District Uganda. Special J Public Health Nutr Diet. 2021;2(1):1–15.
15. Kintu TM, Ssewanyana AM, Kyagambiddwa T, et al. Patient and health worker experiences on utilization of community client Led ART delivery model in South-Western Uganda: a qualitative study; 2021.
16. Nakanwagi S, Matovu JK, Kintu BN, Kaharuza F, Wanyenze RK. Facilitators and barriers to linkage to HIV care among female sex workers receiving HIV testing services at a community-based organization in Periurban Uganda: a qualitative study. J Sex Transm Dis. 2016;2016:1–8. doi:10.1155/2016/7673014
17. Sharer M, Davis N, Makina N, Duffy M, Eagan S. Differentiated antiretroviral therapy delivery: implementation barriers and enablers in South Africa. J Assoc Nurses AIDS Care. 2019;30(5):511. doi:10.1097/JNC.0000000000000062
18. Zakumumpa H, Rujumba J, Kwiringira J, Katureebe C, Spicer N. Understanding implementation barriers in the national scale-up of differentiated ART delivery in Uganda. BMC Health Serv Res. 2020;20(1):1–16. doi:10.1186/s12913-020-5069-y
19. Kushemererwa J, Muwanguzi M, Atukunda EC, et al. Barriers and facilitators of male engagement in Community Client-Led Antiretroviral therapy Delivery groups (CCLADS) for HIV care and treatment in Southwestern Uganda: a qualitative study. BMC Health Serv Res. 2022;22(1):1–9.
20. Atuhaire L, Shumba CS, Nyasulu PS. “My condition is my secret”: perspectives of HIV positive female sex workers on differentiated service delivery models in Kampala Uganda. BMC Health Serv Res. 2022;22(1):1–13.
21. Duffy M, Sharer M, Davis N, et al. Differentiated antiretroviral therapy distribution models: enablers and barriers to universal HIV treatment in South Africa, Uganda, and Zimbabwe. J Assoc Nurses AIDS Care. 2019;30(5):e132. doi:10.1097/JNC.0000000000000097
22. Njuguna B, Vorkoper S, Patel P, et al. Models of integration of HIV and noncommunicable disease care in sub-Saharan Africa: lessons learned and evidence gaps. AIDS. 2018;32(Suppl 1):S33. doi:10.1097/QAD.0000000000001887
23. Opio M, Akello F, Twongyeirwe DK, et al. Perspectives on linkage to care for patients diagnosed with HIV: a qualitative study at a rural health center in South Western Uganda. PLoS One. 2022;17(3):e0263864. doi:10.1371/journal.pone.0263864
24. Kintu TM, Ssewanyana AM, Kyagambiddwa T, et al. Exploring drivers and barriers to the utilization of community client-led ART delivery model in South-Western Uganda: patients’ and health workers’ experiences. BMC Health Serv Res. 2021;21(1):1–14.
25. Camlin CS, Seeley J. Qualitative research on community experiences in large HIV research trials: what have we learned? J Int AIDS Soc. 2018;21(Suppl 7):e25173. doi:10.1002/jia2.25173
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.