")
Back to Journals » Cancer Management and Research » Volume 14
Beyond Surgical Treatment in Adenoid Cystic Carcinoma of the Head and Neck: A Literature Review
Authors Atallah S, Marc M, Schernberg A, Huguet F, Wagner I, Mäkitie A , Baujat B
Received 24 December 2021
Accepted for publication 24 April 2022
Published 4 June 2022 Volume 2022:14 Pages 1879—1890
DOI https://doi.org/10.2147/CMAR.S355663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matthew Witek
Sarah Atallah,1,2 Morgane Marc,1 Antoine Schernberg,3 Florence Huguet,3 Isabelle Wagner,1 Antti Mäkitie,4,5 Bertrand Baujat1
1Department of Otorhinolaryngology–Head and Neck Surgery, Sorbonne University, Tenon Hospital, AP-HP, Paris, France; 2Doctoral School of Public Health, University of Paris Sud, CESP, INSERM U1018, University of Paris-Saclay, UVSQ, Villejuif, France; 3Department of Radiotherapy, Sorbonne University, Tenon Hospital, AP-HP, Paris, France; 4Department of Otorhinolaryngology - Head and Neck Surgery, University of Helsinki and Helsinki University Hospital, Helsinki, Finland; 5Research Program in Systems Oncology, Faculty of Medicine, University of Helsinki, Helsinki, Finland
Correspondence: Sarah Atallah, Hôpital Tenon, AP-HP, 4 rue de la Chine, Paris, 75020, France, Tel +33 156016417, Email [email protected]
Introduction: Adenoid cystic carcinoma (AdCC) is a rare tumour as it accounts for about 10% of all salivary gland neoplasms. It occurs in all age groups with a predominance of women, but no risk factors have been identified to date. Although AdCC behaves as a slow-growing tumour, it is characterized by multiple and late recurrences. Therefore, we aim to update the knowledge of the treatment options in advanced and recurrent cases.
Materials and Methods: We performed a systematic literature review to provide a synthesis of the practical knowledge required for AdCC non-surgical management. Altogether, 99 out of the 1208 available publications were selected for analysis.
Results: AdCC is described as a basaloid tumour consisting of epithelial and myoepithelial cells. Immunohistochemistry is useful for diagnosis (PS100, Vimentin, CD117, CKit, muscle actin, p63) and for prognosis (Ki67). Identified mutations could lead to therapeutic opportunities (MYB-NFIB, Notch 1). The work-up is mainly based on neck and chest CT scan and MRI, and PET-CT with 18-FDG or PSMA can be considered. Surgical treatment remains the gold standard in resectable cases. Post-operative intensity modulated radiotherapy is the standard of care, but hadron therapy may be used in specific situations. Based on the available literature, no standard chemotherapy regimen can be recommended.
Conclusion: There is currently no consensus on the use of chemotherapy in AdCC, either concomitantly to RT in a postoperative setting or at a metastatic stage. Further, the available targeted therapies do not yet provide significant tumour response.
Keywords: adenoid cystic carcinoma, salivary glands, head and neck neoplasm, epidemiology, therapeutics
Summary
Head and neck Adenoid Cystic Carcinoma (AdCC) is a relatively rare tumour originating in the minor and major salivary glands. The large number of publications over the last 30 years contains contradictory information on its management. Our aim is to provide a synthesis of the literature for the diagnosis and the different non-surgical therapeutic options.
Introduction
Adenoid cystic carcinoma (AdCC) is a rare tumour accounting for only 1% of all head and neck cancers and about 10% of all salivary gland tumours.1 It is a malignancy of the secretory epithelial cells of the main salivary glands (MSG), accessory (ASG) and ectopic glands.2
This tumour occurs in all age groups including children, with a slightly higher rate in middle-aged patients (50–60 years), and a predominance of women.3,4 No etiological risk factors have been identified to date.
It behaves as a slow-growing tumour, yet it is characterized by multiple and late recurrences.5 Its imprecise limits and its tendency for perineural invasion contribute to making it a tumour of unpredictable evolution.6
AdCC is described as a basaloid tumour consisting of epithelial and myoepithelial cells. Immunohistochemistry is useful for diagnosis and for prognosis. Identified mutations could lead to therapeutic opportunities. The work-up is mainly based on neck and chest CT scan as well as MRI, but PET-CT with 18-FDG or PSMA can be considered.
The surgical treatment remains, when possible, a gold standard in this pathology. As this statement is not controversial, we will not extensively discuss it in this review. Post-operative intensity modulated radiotherapy is recommended but hadron therapy may be used in specific situations. There is currently no consensus on chemotherapy in AdCC, neither concomitantly to RT in a postoperative setting nor at a metastatic stage. Further, targeted therapies have not yet provided significant tumour response.
The main objective of this article is to provide a synthetic review of the practical knowledge required for AdCC non-surgical management. Furthermore, we discuss the current diagnostic principles as these might provide the basis for the future targeted therapies.
Materials and Methods
Using the PUBMED database, we carried out a systematic bibliography search between 2000 and 2021 using the key words: “head and neck” and “adenoid cystic carcinoma” and adding the MESH terms: “anatomy”, “histology”, “epidemiology”, “radiotherapy”, “surgery”, and “drug therapy”.
Altogether, we identified 1208 references in the search. The retrieved articles were further analyzed for possible duplicates and irrelevant studies. In addition, to further minimize the risk of omission of additional studies, we manually searched the reference lists of the eligible 387 articles to ensure that all the relevant studies were duly included. Finally, after further analysis of the articles, we selected 87 articles for this review. We added to the final version of the review 11 historical reference articles published before 2000 that could not be replaced as well as 1 methodological reference. (Figure 1).
 |
Figure 1 PRISMA flow diagram. Notes: Adapted from: Liberati A, Altman D, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10)e1-e34.100 Creative Commons. |
Results
Pathology
AdCC is defined as a basaloid tumour consisting of epithelial and myoepithelial cells in variable morphological configurations.7 Macroscopically, AdCC is a hard, non-encapsulated mass, snow-white or pinkish in appearance, and can present itself as either a circumscribed or an extended, poorly defined (more invasive) tumour. Microscopically, AdCC is composed of two types of cells: myoepithelial-like cells and duct-like cells. These cells can arrange into one of three architectural patterns: cribriform, tubular or solid.8 Most tumours display a combination of these patterns.9
Histoprognostic Classification
Szanto et al first proposed a histoprognostic classification in 1984.10 It is based on the proportion of solid components within the tumour and classifies AdCCs into three grades:
Grade I: well-differentiated tumours composed of tubular and cribriform areas without any solid component.
Grade II: tumours with a dominant cribriform structure and less than 30% solid areas.
Grade III: tumour with a predominantly solid architecture.
The importance of this grading system is debated. The grade may vary according to the anatomopathologist’s experience.11
The study by Van Weert et al shows that the mere presence of a solid type component is a poor prognostic factor. They note that for an anatomopathologist, indicating the presence of a solid component seems more reliable and reproducible than specifying its percentage. They therefore suggest merely noting the presence or absence of a solid component to simplify this classification.12
Immunohistochemistry
Immunohistochemistry is a useful diagnostic tool, which reveals the surface antigens expressed by tumour cells. It is not always carried out as a routine examination.
Various markers such as S 100 protein, muscle actin, p63, CD117 (Receptor tyrosine kinase C-Kit) and vimentin can be instrumental in identifying the myoepithelial cells that form AdCC pseudocysts.7,13
For example, polymorphous adenocarcinoma (formerly polymorphous low-grade adenocarcinoma) is very similar to AdCC both in histology and immunohistochemistry. Several immunohistochemical markers including c-Kit, S-100/ MG, Mcm-2 and Integrin β-1, −3, −4, are reported to be useful diagnostic aids in borderline cases.14 The monoclonal antibody MIB1ʹs recognition of the Ki-67 antigen is a useful tool for diagnosis and prognosis, with an index around 20% for AdCC and much lower for polymorphous adenocarcinoma.9
Oncogenesis
The research on AdCC oncogenesis has been delayed due to the lack of validated cell lines. Studying tumour tissue and recently, xenografts (mouse models) has made it possible to identify several possible therapeutic targets.15
Various differentiation, signaling and cell growth pathways are involved in AdCC oncogenesis: the Sox4 pathway, Wnt/b-catenin signaling pathway, C-Kit tyrosine kinase receptors, p53 protein, epidermal growth factor receptors (EGFR) and human epidermal receptors (HER).16–19
Genome-wise, AdCC has a lower mutation rate than other tumours. These mutations are more frequently somatic mutations with an average of 22 mutations per tumour.20,21 Deletions involving 12q, 6q, 9p, 11q, 14q, 1p and 5q and gains involving 1q and 22q are the most frequently identified.22
The reciprocal t(6; 9)(q22-23; p23-24) translocation is found in 80–90% of cases. Several authors have focused on this translocation as it consistently results from the fusion of the MYB oncogene with the transcription factor gene NFIB.23 MYB is one of the first identified oncogenes and was discovered nearly 30 years ago. It plays a key role in the control of cell proliferation, survival, differentiation, and angiogenesis. More than 80 genes are recognized as targets of MYB, such as the proliferative genes MYC, CCNA1, CCNB1, CCNE1, c-KIT, the anti-apoptotic BCL-2, HSPA5, HSP70, COX-2 pro-inflammatory and regulatory differentiation genes such as GATA3.24,25
In 2009, Persson et al were the first to describe this fusion transcript.23 The MYB-NFIB fusion transcript results from the loss of the MYB 3’ region, which normally contains target sequences for some microRNAs (miRNAs) (miR-15a, miR-16 and miR150). The MYB gene, deprived of its regulatory sequence, induces a massive transcription of the MYB proto-oncogene, resulting in the overexpression of all its target genes.26
The MYB-NFIB fusion transcript is not found in other salivary gland carcinomas.27,28 It can be detected by reverse transcription, polymerase chain reaction (RT-PCR), fluorescent in situ hybridisation (FISH) or indirect immunohistochemical staining of MYB proteins. Easy to detect, it is a useful diagnostic biomarker when the morphological diagnosis of AdCC is not certain and could also open interesting therapeutic prospects.29,30
Recent studies suggest that Notch 1 plays a key role in cell growth and the presence of distant metastasis. Oncogenic functions of the NOTCH signaling pathway include the inhibition of apoptosis and activation of cell proliferation.31,32 The presence of a mutation in the NOTCH 1 receptor appears to be an adverse prognostic factor in patients with AdCC.33 Targeting this signaling pathway could lead to a potential therapeutic strategy. However, the first published study investigating Notch inhibitors did not provide convincing results (see Table 1).
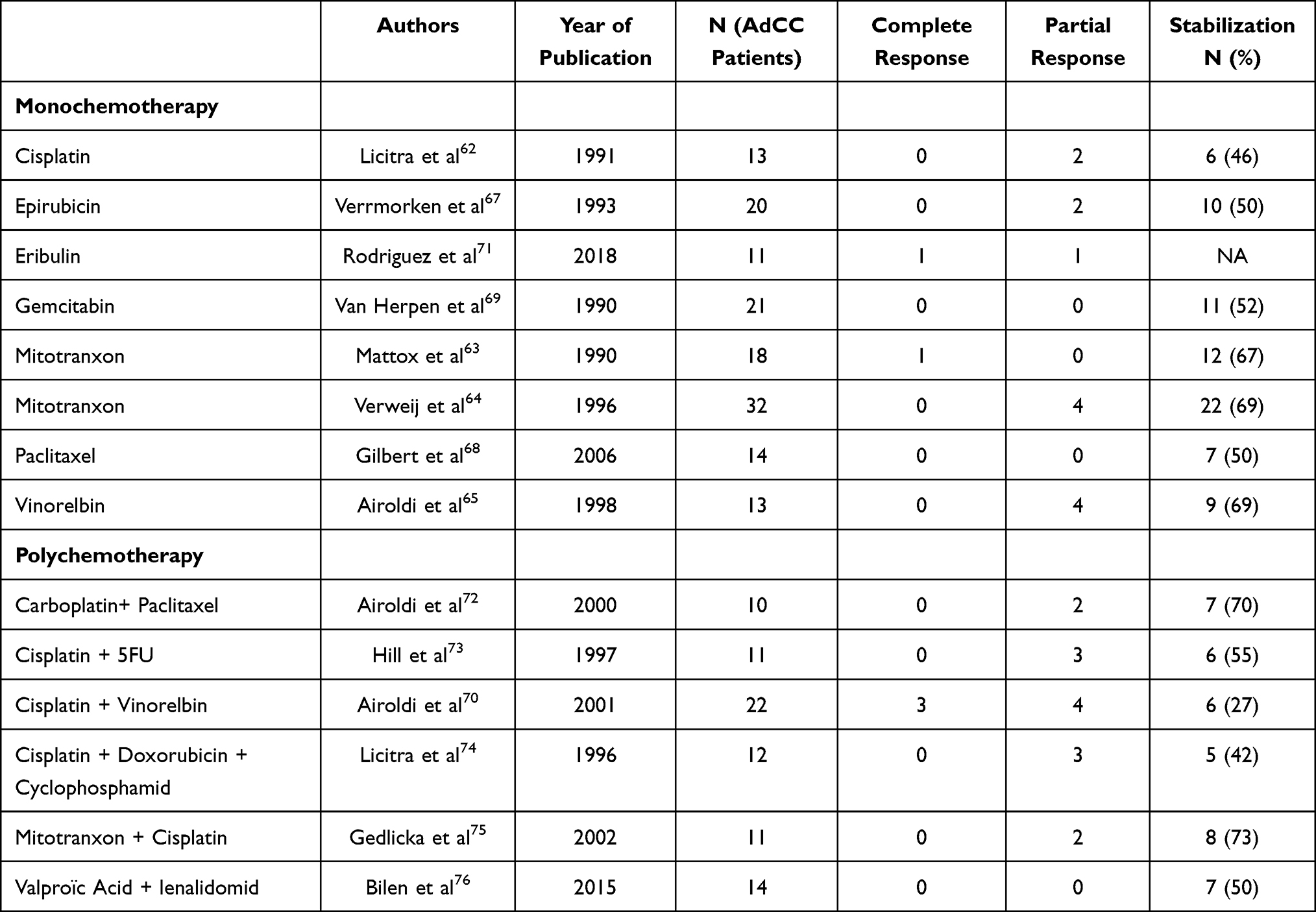 |
Table 1 Chemotherapies Tested in Scientific Literature: Main Results (Non-Exhaustive List) |
Work-Up
Diagnostic imaging should look for lymph nodes and pulmonary metastases, with the standard assessment being computed tomography of neck and chest (CT) with contrast. Local extension of the AdCC should be assessed by MRI with diffusion sequences.34
(18F) fluorodeoxyglucose positron emission tomography (18F-FDG PET) has a well-known predictive value in the initial work-up and follow-up of patients with squamous cell carcinoma of the head and neck.35 However, the value of 18F-FDG PET in patients with AdCC is debated.
Low 18F-FDG uptake and false negatives have been observed. A weak expression of the glucose transporter GLUT 1 by AdCC is one of the hypotheses explaining this possible decrease in FDG uptake. The normal physiologic absorption of FDG by salivary glands could also be involved in this phenomenon. For tumours located in the skull base, the increased uptake of cerebral FDG (normal brain tissue recognizes glucose as a metabolic substrate) interferes with 18F-FDG PET visualization of these tumours.36
Recent studies suggest an interest of 18F-FDG PET in the initial and follow-up evaluation of patients with AdCC. The study by Jung et al shows that 18F-FDG-PET sensitivity (92.3%) is comparable to that of conventional CT for the detection of primary AdCC. The N and M statuses tend to be modified by the 18F-FDG PET examination, which would in turn alter the tumour staging.37
A high rate of the Standardized Uptake Value (SUVmax) is found to be an adverse prognostic factor. SUVmax was higher in patients with AdCC of higher metastatic potential.38
Currently, some authors consider that 18F-FDG PET is of added value in the evaluation of metastatic salivary gland cancers and has an impact on the therapeutic management of these patients.39
Prostate-specific membrane antigen (PSMA) is a type II transmembrane glycoprotein of the prostate epithelium over-expressed in prostate adenocarcinomas and their metastases.40
Functional imaging using PSMA and radiolabeled ligands (68-Gallium-PSMA-11) coupled with CT imaging (PSMA-PET CT) is currently used for the diagnosis and restaging of certain prostate cancers.41 Recently, PSMA-PET has been assessed in AdCC patients.42
Treatment
The therapeutic strategy used for patients with salivary gland cancer depends on the tumour TNM stage and grade (according to the salivary gland malignancy staging system). The TNM clinical staging of the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) remains the most practical and the most suitable one for electing the appropriate treatment.43 This depends on the site of the primary tumour.
Sorting salivary gland malignancies according to their histologic grade helps to specify their degree of malignancy, on which among other items, the choice of overall therapeutic strategy depends. This proves the need for a simple classification in which tumours with a substantially identical prognosis and comparable treatment are grouped together (high grade/low grade). Such a sorting system makes it possible to apprehend the great majority of clinical situations.44
The 2005 WHO classification introduced an intermediate grade, with a tendency towards more frequent recurrence and/or lymph node metastases in more than 10% of cases. These grades are correlated, regardless of clinical stage, with the potential for regional and distant metastases.
Overall, AdCC is considered as:
According to the “simplified” classification: a high-grade tumour regardless of its type of histologic architecture.
According to the WHO classification: an intermediate-grade tumour for cribriform/tubular types and a high-grade tumour if ≥ 30% solid.
Surgery
Standard care for non-metastatic AdCC, regardless of the primary tumour site, is surgery.45 The main objective should be total surgical resection with free margins.46
The management of lymph node areas in AdCC without nodal metastasis (N0) remains controversial. Although ASCO guidelines recommend elective neck dissection in clinically negative neck in T3-T4 tumours and high-grade malignancies, results from a comparative study of the REFCOR cohort suggest that there is no benefit in terms of event-free survival in cN0 patients having undergone neck dissection.34,47
ASCO guidelines specify the appropriate treatment in the setting of resectable, recurrent locoregional disease and distant metastatic disease, regardless of prior treatment type. In this situation, it may include palliative revision resection and appropriate surgical reconstruction and rehabilitation if the metastatic disease is not rapidly progressive or imminently lethal.34 Surgical treatment of oligometastatic disease may also be considered when complete surgical resection is feasible and when the time to pulmonary relapse after primary tumor treatment is greater than 36 months.48
Post-Operative Radiotherapy (PORT)
Although there is no data available from randomized trials, scientific literature points to better local control in AdCC patients treated with post-operative radiotherapy.49–51 The delineated volumes are specific to this pathology as they must encompass AdCC’s perineural extension often all the way to the nerves’ emergence from the skull base. The proximity to several at-risk organs makes this particular radiotherapy complex. ASCO guidelines recommend that PORT should be offered to all patients with resected AdCC.34
Exclusive Radiotherapy
There are few studies comparing the effectiveness of surgical treatment with exclusive radiotherapy, and these are retrospective and present selection biases.52 The results of these studies should therefore be taken with caution, as the effect of treatment is influenced by the patients’ initial characteristics. This is how Simpson’s paradox is expressed: in this case, small resectable tumours with a better prognosis benefit from surgical treatment, whereas those treated by exclusive radiotherapy are more often incompletely resectable and have a poorer prognosis.53 Exclusive radiotherapy may be considered in the case of surgical contraindications or non-resectable tumours.54
Radiation Treatment Methods
Conventional radiotherapy, involving photons (X-rays) and electrons produced by linear accelerators, is the most frequently employed technique (good accessibility/availability of machines).
Hadron therapy is a form of external radiotherapy that uses an accelerator of neutral or charged “heavy” particles. The heavier particles deliver peak energy at one point delivering little energy to healthy tissue.55 This type of treatment can be particularly valuable for malignant tumours located close to at-risk organs (such as the optic nerve, spinal cord or central nervous system).
Neutrons are high LET particles with no charge. They differ from X-rays by their high Relative Biological Effectiveness (RBE). Neutron therapy was one of the available, standard-care treatments for patients suffering from advanced, unresectable AdCC from 1990 to 2000.56 However, it was abandoned due to high toxicity and high technical cost.57
Carbon ions combine a high LET and an even higher RBE than protons. Thus, they can be an effective treatment option while minimizing the dose delivered to healthy tissue. Several studies suggest that carbon ion radiotherapy does not provide a significant difference in efficacy compared to proton therapy in terms of survival and local control but does show a decrease in grade 3 and 4 toxicities of the treatment.58,59 Cosmic Phase 2 trial investigated Intensity modulated radiotherapy and dose – escalated carbon iodine therapy in salivary gland cancers with incomplete resection or inoperable. A large proportion of AdCC was included. They showed 17% of complete response, 34% of partial response, 11% of stable disease. The local control at 3 years was 75% in inoperable patients. Toxicity level was considered acceptable.60
The radiotherapy procedure for salivary gland cancers must be 3D-conformal radiation therapy with or without intensity modulation. Conformal irradiation with intensity modulation is recommended for teams that possess the full required equipment, whenever photon therapy may be considered.
Hadron therapy may be preferred in case of tumour remnants.60 However, ASCO guidelines specify that although particle therapy including proton, neutron and carbon ion therapy may be used, there are no indication for the use of heavy particles over photon or electron therapy.34
Chemotherapy
There is currently no chemotherapy recognized as effective in the treatment of primary or recurrent tumours in patients with AdCC. Further, chemotherapy concomitantly delivered with radiotherapy is not currently recommended.
Laurie et al showed that palliative chemotherapy may be of interest for a small proportion of patients with advanced AdCC after excluding other palliative therapies (radiotherapy and/or metastasis surgery).61
Administered as monotherapy, cisplatin,62 mitoxantrone63,64 and vinorelbin65 have shown an objective response in prospective clinical trials with tumour stabilization and an acceptable level of toxicity.66 An anthracycline such as epirubicin may be an option.67
If monotherapy is elected, neither paclitaxel nor gemcitabine is recommended due to the lack of proven activity.68,69
If polytherapy is elected, the combination of cisplatin and vinorelbine seems to be the most interesting.70
The observed response rate of AdCC remains very low in all chemotherapy trials (Table 1).
The choice of treatment should be guided by the patient’s co-morbidities, therapeutic history, and the various chemotherapy toxicities.
Laurie et al suggest that inclusion in therapeutic trials should be considered as soon as possible given the low efficacy of all standard chemotherapies.61
Based on the available literature, no standard chemotherapy regimen can be recommended.77
Targeted Therapies
Targeted therapies are promising new molecules for cancer treatment. They target specific pathways that play an important role in the proliferation, angiogenesis and/or apoptosis of cancer cells, with limited toxicity. Several targeted molecular abnormalities have been identified and various drugs such as imatinib, gefitinib, and sorafenib have been tested in patients with metastatic AdCC.78–80
Prolonged stabilization of survival in patients with AdCC is observed with the use of C-Kit, EGFR, VEGF and histone deacetylase (HDAC) inhibitors. However, no complete response is observed, and a small proportion of patients showed partial response to some therapies (Table 2).
 |
Table 2 Targeted Therapies Tested in Scientific Literature: Therapeutic Targets and Main Results (Non-Exhaustive List) |
A Phase I trial testing a NOTCH signaling pathway inhibitor (crenigacestat) showed high toxicity and limited clinical activity (Table 2).
A Phase II trial testing a NOTCH pathway inhibitor (AL 101) is currently ongoing (AL 101, NCT03691207).
Discussion
AdCC of the salivary glands remains a challenging tumour. This review discusses the diagnostic elements of this entity and focuses specifically on the available non-surgical management options.
The histoprognostic classification is still debated: currently, there is no consensus on the use of a two- (presence or absence of solid architecture) or three-grade classification.
The analysis of histological reports of a recent REFCOR series has shown great variability in histological description from one practitioner to another.98
A two-grade classification could therefore be recommended, although an experts’ consensus would be worth seeking on this issue.
The work-up is the same as in other salivary gland malignancies, but the TEP PSMA could open therapeutic prospects.42,99
Surgery remains the gold standard and PORT is now recommended in all AdCC. However, this recommendation relies on intermediate quality evidence: PORT could still be discussed in early stages of the disease after a resection with clear margins.
The SANTAL/ GORTEC 2016–02 trial, which is currently ongoing, will provide some answers to the question of whether chemotherapy can be used to potentiate radiotherapy in patients with cancer of the salivary glands. Its main objective is to assess the impact on progression-free survival of potentiating adjuvant radiotherapy with high-dose cisplatin for salivary gland cancers of every histology (NCT02998385).
Targeted therapies have not provided convincing results to date (Table 2). They show a small number of partial responses, no complete response, and a variable level of stabilization. It should be noted that disease stabilization is a poor indicator in AdCC, where little or no progression of metastases can be observed for several years even in the absence of treatment.
MYB-NFIB mutation could be a potential therapeutic target, but the drug is not available to date.
Conclusions
The therapeutic strategy for patients with head and neck AdCC remains a challenge. Surgery for the primary site forms the gold standard whenever possible. PORT is recommended, though its modalities remain controversial.
Thanks to a better understanding of AdCC oncogenesis, progress has been made in the field of therapies targeting molecular biomarkers. It is thus useful to discuss the cases in molecular tumor boards.
However, the use of these therapies is currently limited to clinical trials for patients with advanced tumours and their effectiveness is still poor in terms of complete or partial response.
Other research prospects have yet to be examined, such as the study of druggable markers in molecular imaging, developing a therapy targeting the MYB-NFIB fusion transcript, or analyzing immunotherapy potency in patients with AdCC.
Alliances between reference centers specializing in the treatment of rare cancers, such as the French national network on rare head and neck tumours REFCOR or the European reference network on rare cancers EURACAN, could allow the development of more powerful fundamental and clinical studies.
Acknowledgments
The authors thank the Adenoid Cystic Carcinoma Research Foundation (ACCRF), REFCOR and EURACAN for supporting research on AdCC. They also thank Alexis Baujat for editing the manuscript.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Coca-Pelaz A, Rodrigo JP, Bradley PJ, et al. Adenoid cystic carcinoma of the head and neck-An update. Oral Oncol. 2015;51:652–661. doi:10.1016/j.oraloncology.2015.04.005
2. Li N, Xu L, Zhao H, El-Naggar AK, Sturgis EM. A comparison of the demographics, clinical features, and survival of patients with adenoid cystic carcinoma of major and minor salivary glands versus less common sites within the Surveillance, Epidemiology, and End Results registry. Cancer. 2012;118:3945–3953. doi:10.1002/cncr.26740
3. Moskaluk CA. Adenoid cystic carcinoma: clinical and molecular features. Head Neck Pathol. 2013;7:17–22. doi:10.1007/s12105-013-0426-3
4. Gondivkar SM, Gadbail AR, Chole R, Parikh RV. Adenoid cystic carcinoma: a rare clinical entity and literature review. Oral Oncol. 2011;47:231–236. doi:10.1016/j.oraloncology.2011.01.009
5. Bradley PJ. Adenoid cystic carcinoma of the head and neck: a review. Curr Opin Otolaryngol Head Neck Surg. 2004;12:127–132. doi:10.1097/00020840-200404000-00013
6. Dantas AN, de Morais EF, de Macedo RA. Clinicopathological characteristics and perineural invasion in adenoid cystic carcinoma: a systematic review. Braz J Otorhinolaryngol. 2015;81:329–335. doi:10.1016/j.bjorl.2014.07.016
7. Simpson RHW, Skálová A, Di Palma S, Leivo I. Recent advances in the diagnostic pathology of salivary carcinomas. Virchows Arch. 2014;465:371–384. doi:10.1007/s00428-014-1639-x
8. Jaso J, Malhotra R. Adenoid cystic carcinoma. Arch Pathol Lab Med. 2011;135:511–515. doi:10.1043/2009-0527-RS.1
9. Hellquist H, Skalova A. Histopathology of the Salivary Glands, Chapter 8. Adenoid Cystic Carcinoma. Heidelberg: Springer-Verlag; 2014.
10. Szanto PA, Luna MA, Tortoledo ME, White RA. Histologic grading of adenoid cystic carcinoma of the salivary glands. Cancer. 1984;54:1062–1069. doi:10.1002/1097-0142(19840915)54:6<1062::AID-CNCR2820540622>3.0.CO;2-E
11. Badoual C, Baglin A-C, Wassef M, et al. Pathologists and the French network of expertise on rare cancers ENT: the REFCORpath. Ann Pathol. 2014;34:64–69. doi:10.1016/j.annpat.2014.01.006
12. Van Weert S, Van der Waal I, Witte BI, Leemans CR, Bloemena E. Histopathological grading of adenoid cystic carcinoma of the head and neck: analysis of currently used grading systems and proposal for a simplified grading scheme. Oral Oncol. 2015;51:71–76. doi:10.1016/j.oraloncology.2014.10.007
13. Edwards PC, Bhuiya T, Kelsch RD. Assessment of p63 expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and basal cell and canalicular adenomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:613–619. doi:10.1016/S1079210403005742
14. Tasoulas J, Tsourouflis G, Klijanienko J, Theocharis S. Polymorphous adenocarcinoma: an overview of immunohistochemical features and insights on molecular pathology. Histol Histopathol. 2019;34(7):731–744. doi:10.14670/HH-18-089
15. Frierson HF, El-Naggar AK, Welsh JB, et al. Large scale molecular analysis identifies genes with altered expression in salivary adenoid cystic carcinoma. Am J Pathol. 2002;161:1315–1323. doi:10.1016/S0002-9440(10)64408-2
16. Daa T, Kashima K, Kaku N, Suzuki M, Yokoyama S. Mutations in components of the Wnt signaling pathway in adenoid cystic carcinoma. Mod Pathol. 2004;17:1475–1482. doi:10.1038/modpathol.3800209
17. Edwards PC, Bhuiya T, Kelsch RD. C-kit expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and monomorphic adenoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:586–593. doi:10.1067/moe.2003.31
18. Ito FA, Ito K, Coletta RD, Graner E, de Almeida OP, Lopes MA. Salivary gland tumors: immunohistochemical study of EGF, EGFR, ErbB-2, FAS and Ki-67. Anal Quant Cytol Histol. 2009;31:280–287.
19. Gibbons MD, Manne U, Carroll WR, Peters GE, Weiss HL, Grizzle WE. Molecular differences in mucoepidermoid carcinoma and adenoid cystic carcinoma of the major salivary glands. Laryngoscope. 2001;111(8):1373–1378. doi:10.1097/00005537-200108000-00011
20. Ho AS, Kannan K, Roy DM, et al. The mutational landscape of adenoid cystic carcinoma. Nat Genet. 2013;45:791–798. doi:10.1038/ng.2643
21. Stephens PJ, Davies HR, Mitani Y, et al. Whole exome sequencing of adenoid cystic carcinoma. J Clin Invest. 2013;123:2965–2968. doi:10.1172/JCI67201
22. Bradley PJ. Adenoid cystic carcinoma evaluation and management: progress with optimism Curr Opin Otolaryngol Head Neck Surg. 2017;25:147–153. doi:10.1097/MOO.0000000000000347
23. Persson M, Andrén Y, Mark J, Horlings HM, Persson F, Stenman G. Recurrent fusion of MYB and NFIB transcription factor genes in carcinomas of the breast and head and neck. Proc Natl Acad Sci USA. 2009;106:18740–18744. doi:10.1073/pnas.0909114106
24. Ramsay RG, Gonda TJ. MYB function in normal and cancer cells. Nat Rev Cancer. 2008;8:523–534. doi:10.1038/nrc2439
25. Drabsch Y, Robert RG, Gonda TJ. MYB suppresses differentiation and apoptosis of human breast cancer cells. Breast Cancer Res. 2010;12:R55. doi:10.1186/bcr2614
26. Persson M, Andrén Y, Moskaluk CA, et al. Clinically significant copy number alterations and complex rearrangements of MYB and NFIB in head and neck adenoid cystic carcinoma. Genes Chromosomes Cancer. 2012;51:805–817. doi:10.1002/gcc.21965
27. Seethala RR, Stenman G. Update from the 4th Edition of the World Health Organization classification of head and neck tumours: tumors of the salivary gland. Head Neck Pathol. 2017;11:55–67. doi:10.1007/s12105-017-0795-0
28. Stenman G. Fusion oncogenes in salivary gland tumors: molecular and clinical consequences. Head Neck Pathol. 2013;7:12–19. doi:10.1007/s12105-013-0462-z
29. Andersson MK, Afshari MK, Andrén Y, Wick MJ, Stenman G. Targeting the oncogenic transcriptional regulator MYB in adenoid cystic carcinoma by inhibition of IGF1R/AKT signaling. J Natl Cancer Inst. 2017;109. doi: 10.1093/jnci/djx017.
30. Subramaniam T, Lennon P, O’Neill JP. Ongoing challenges in the treatment of adenoid cystic carcinoma of the head and neck. Ir J Med Sci. 2015;184:583–590. doi:10.1007/s11845-015-1298-1
31. Bell D, Hanna EY. Head and neck adenoid cystic carcinoma: what is new in biological markers and treatment? Curr Opin Otolaryngol Head Neck Surg. 2013;21:124–129. doi:10.1097/MOO.0b013e32835c05fd
32. Xie M, Wei S, Wu X, Li X, You Y, He C. Alterations of Notch pathway in patients with adenoid cystic carcinoma of the trachea and its impact on survival. Lung Cancer. 2018;121:41–47. doi:10.1016/j.lungcan.2018.04.020
33. Ferrarotto R, Mitani Y, Diao L, et al. Activating NOTCH1 mutations define a distinct subgroup of patients with adenoid cystic carcinoma who have poor prognosis, propensity to bone and liver metastasis, and potential responsiveness to notch1 inhibitors. J Clin Oncol. 2017;35:352–360. doi:10.1200/JCO.2016.67.5264
34. Geiger JL, Ismaila N, Beadle B, et al. Management of salivary gland malignancy: ASCO guideline. J Clin Oncol. 2021;39:1909–1941. doi:10.1200/JCO.21.00449
35. Lonneux M, Hamoir M, Reychler H, et al. Positron emission tomography with [18F]fluorodeoxyglucose improves staging and patient management in patients with head and neck squamous cell carcinoma: a multicenter prospective study. J Clin Oncol. 2010;28:1190–1195. doi:10.1200/JCO.2009.24.6298
36. Tomura N, Mizuno Y, Saginoya T. PET/CT findings for tumors in the base of the skull: comparison of 18 F-FDG with 11 C-methionine. Acta Radiol. 2016;57:325–332. doi:10.1177/0284185115575342
37. Jung JH, Lee SW, Son SH, et al. Clinical impact of18F-FDG positron emission tomography/CT on adenoid cystic carcinoma of the head and neck. Head Neck. 2017;39:447–455. doi:10.1002/hed.24605
38. Kim D, Kim W, Lee J, et al. Pretreatment maximum standardized uptake value of (18) F-fluorodeoxyglucose positron emission tomography as a predictor of distant metastasis in adenoid cystic carcinoma of the head and neck. Head Neck. 2016;38:755–761. doi:10.1002/hed.23953
39. Freling N, Crippa F, Maroldi R. Staging and follow-up of high-grade malignant salivary gland tumours: the role of traditional versus functional imaging approaches - A review. Oral Oncol. 2016;60:157–166. doi:10.1016/j.oraloncology.2016.04.016
40. Wright GL, Haley C, Beckett ML, Schellhammer PF. Expression of prostate-specific membrane antigen in normal, benign, and malignant prostate tissues. Urol Oncol. 1995;1:18–28. doi:10.1016/1078-1439(95)00002-Y
41. Afshar-Oromieh A, Hetzheim H, Kratochwil C, et al. The theranostic PSMA ligand PSMA-617 in the diagnosis of prostate cancer by PET/CT: biodistribution in humans, radiation dosimetry, and first evaluation of tumor lesions. J Nucl Med. 2015;56:1697–1705. doi:10.2967/jnumed.115.161299
42. Klein Nulent TJW, van Es RJJ, Krijger GC, de Bree R, Willems SM, de Keizer B. Prostate-specific membrane antigen PET imaging and immunohistochemistry in adenoid cystic carcinoma-A preliminary analysis. Eur J Nucl Med Mol Imaging. 2017;44:1614–1621. doi:10.1007/s00259-017-3737-x
43. Brierley JD, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours. John Wiley & Sons; 2017.
44. Simpson RH. Classification of tumours of the salivary glands. Histopathology. 1994;24:187–191. doi:10.1111/j.1365-2559.1994.tb01303.x
45. Meyers M, Granger B, Herman P, et al. Head and neck adenoid cystic carcinoma: a prospective multicenter REFCOR study of 95 cases. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:13–17. doi:10.1016/j.anorl.2015.09.009
46. Amit M, Na’ara S, Trejo-Leider L, et al. Defining the surgical margins of adenoid cystic carcinoma and their impact on outcome: an international collaborative study. Head Neck. 2017;39(5):1008–1014. doi:10.1002/hed.24740
47. Atallah S, Moya-Plana A, Malard O, et al. Should a neck dissection be performed on patients with cN0 adenoid cystic carcinoma? A REFCOR propensity score matching study. Eur J Cancer. 2020;130:250–258. doi:10.1016/j.ejca.2019.12.026
48. Girelli L, Locati L, Galeone C, et al. Lung metastasectomy in adenoid cystic cancer: is it worth it? Oral Oncol. 2017;65:114–118. doi:10.1016/j.oraloncology.2016.10.018
49. Dubergé T, Bénézery K, Resbeut M, et al. Adenoid cystic carcinoma of the head and neck: a retrospective series of 169 cases. Cancer Radiother. 2012;16:247–256. doi:10.1016/j.canrad.2012.02.003
50. Balamucki CJ, Amdur RJ, Werning JW, et al. Adenoid cystic carcinoma of the head and neck. Am J Otolaryngol. 2012;33:510–518. doi:10.1016/j.amjoto.2011.11.006
51. Chen AM, Bucci MK, Weinberg V, et al. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: prognostic features of recurrence. Int J Radiat Oncol Biol Phys. 2006;66:152–159. doi:10.1016/j.ijrobp.2006.04.014
52. Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Hinerman RW, Villaret DB. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck. 2004;26(2):154–162. doi:10.1002/hed.10380
53. Hernán MA, Clayton D, Keiding N. The Simpson’s paradox unraveled. Int J Epidemiol. 2011;40:780–785. doi:10.1093/ije/dyr041
54. Iseli TA, Karnell LH, Graham SM, et al. Role of radiotherapy in adenoid cystic carcinoma of the head and neck. J Laryngol Otol. 2009;123:1137–1144. doi:10.1017/S0022215109990338
55. Fokas E, Kraft G, An H, Engenhart-Cabillic R. Ion beam radiobiology and cancer: time to update ourselves. Biochim Biophys Acta. 2009;1796:216–229. doi:10.1016/j.bbcan.2009.07.005
56. Huber PE, Debus J, Latz D, et al. Radiotherapy for advanced adenoid cystic carcinoma: neutrons, photons or mixed beam? Radiother Oncol. 2001;59:161–167. doi:10.1016/S0167-8140(00)00273-5
57. Laramore GE, Krall JM, Griffin TW, et al. Neutron versus photon irradiation for unresectable salivary gland tumors: final report of an RTOG-MRC randomized clinical trial. Radiation Therapy Oncology Group. Medical Research Council. Int J Radiat Oncol Biol Phys. 1993;27:235–240. doi:10.1016/0360-3016(93)90233-l
58. Takagi M, Demizu Y, Hashimoto N, et al. Treatment outcomes of particle radiotherapy using protons or carbon ions as a single-modality therapy for adenoid cystic carcinoma of the head and neck. Radiother Oncol. 2014;113:364–370. doi:10.1016/j.radonc.2014.11.031
59. Mizoe JE, Hasegawa A, Jingu K, et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother Oncol. 2012;103:32–37. doi:10.1016/j.radonc.2011.12.013
60. Jensen AD, Nikoghosyan AV, Lossner K, et al. COSMIC: a regimen of IMRT plus dose escalated rasted scanned carbon ion boost for malignant salivary gland tumors: results of the prospective Phase II Trial. Int J Radiat Oncol Biol Phys. 2015;93(1):37–46. doi:10.1016/j.ijrobp.2015.05.013
61. Laurie SA, Ho AL, Fury MG, Sherman E, Pfister DG. Systemic therapy in the management of metastatic or locally recurrent adenoid cystic carcinoma of the salivary glands: a systematic review. Lancet Oncol. 2011;12:815–824. doi:10.1016/S1470-2045(10)70245-X
62. Licitra L, Marchini S, Spinazzè S, et al. Cisplatin in advanced salivary gland carcinoma. A phase II study of 25 patients. Cancer. 1991;68:1874–1877. doi:10.1002/1097-0142(19911101)68:9<1874::aid-cncr2820680904>3.0.co;2-s
63. Mattox DE, Von Hoff DD, Balcerzak SP. Southwest Oncology Group study of mitoxantrone for treatment of patients with advanced adenoid cystic carcinoma of the head and neck. Invest New Drugs. 1990;8:105–107. doi:10.1007/BF00216934
64. Verweij J, de Mulder PH, de Graeff A, et al. Phase II study on mitoxantrone in adenoid cystic carcinomas of the head and neck EORTC Head and Neck Cancer Cooperative Group. Ann Oncol. 1996;7:867–869. doi:10.1093/oxfordjournals.annonc.a010770
65. Airoldi M, Bumma C, Bertetto O, Gabriele P, Succo G, Pedani F. Vinorelbine treatment of recurrent salivary gland carcinomas. Bull Cancer. 1998;85:892–894.
66. Cherifi F, Rambeau A, Johnson A, et al. Systemic treatments of metastatic or locally recurrent adenoid cystic carcinoma of the head and neck, a systematic review. Bull Cancer. 2019;106:923–938. doi:10.1016/j.bulcan.2019.05.003
67. Vermorken JB, Verweij J, de Mulder PH, et al. Epirubicin in patients with advanced or recurrent adenoid cystic carcinoma of the head and neck: a phase II study of the EORTC Head and Neck Cancer Cooperative Group. Ann Oncol. 1993;4:785–788. doi:10.1093/oxfordjournals.annonc.a058665
68. Gilbert J, Li Y, Pinto HA, et al. Phase II trial of taxol in salivary gland malignancies (E1394): a trial of the Eastern Cooperative Oncology Group. Head Neck. 2006;28:197–204. doi:10.1002/hed.20327
69. van Herpen CML, Locati LD, Buter J, et al. Phase II study on gemcitabine in recurrent and/or metastatic adenoid cystic carcinoma of the head and neck (EORTC 24982). Eur J Cancer (Oxf Engl. 1990;2008(44):2542–2545.
70. Airoldi M, Pedani F, Succo G, et al. Phase II randomized trial comparing vinorelbine versus vinorelbine plus cisplatin in patients with recurrent salivary gland malignancies. Cancer. 2001;91:541–547. doi:10.1002/1097-0142(20010201)91:3<541::AID-CNCR1032>3.0.CO;2-Y
71. Rodriguez CP, Martins RG, Baik C, et al. Phase II trial of eribulin mesylate in recurrent or metastatic salivary gland malignancies. Head Neck. 2018;40:584–589. doi:10.1002/hed.25020
72. Airoldi M, Fornari G, Pedani F, et al. Paclitaxel and carboplatin for recurrent salivary gland malignancies. Anticancer Res. 2000;20:3781–3783.
73. Hill ME, Constenla DO, A’Hern RP, et al. Cisplatin and 5-fluorouracil for symptom control in advanced salivary adenoid cystic carcinoma. Oral Oncol. 1997;33:275–278. doi:10.1016/S0964-1955(97)00026-2
74. Licitra L, Cavina R, Grandi C, et al. Cisplatin, doxorubicin and cyclophosphamide in advanced salivary gland carcinoma. A phase II trial of 22 patients. Ann Oncol. 1996;7:640–642. doi:10.1093/oxfordjournals.annonc.a010684
75. Gedlicka C, Schüll B, Formanek M, et al. Mitoxantrone and cisplatin in recurrent and/or metastatic salivary gland malignancies. Anticancer Drugs. 2002;13:491–495. doi:10.1097/00001813-200206000-00007
76. Bilen MA, Fu S, Falchook GS, et al. Phase I trial of valproic acid and lenalidomide in patients with advanced cancer. Cancer Chemother Pharmacol. 2015;75:869–874. doi:10.1007/s00280-015-2695-x
77. Papaspyrou G, Hoch S, Rinaldo A, et al. Chemotherapy and targeted therapy in adenoid cystic carcinoma of the head and neck: a review. Head Neck. 2011;33:905–911. doi:10.1002/hed.21458
78. Pfeffer MR, Talmi Y, Catane R, Symon Z, Yosepovitch A, Levitt M. A phase II study of Imatinib for advanced adenoid cystic carcinoma of head and neck salivary glands. Oral Oncol. 2007;43:33–36. doi:10.1016/j.oraloncology.2005.12.026
79. Jakob JA, Kies MS, Glisson BS, et al. Phase II study of gefitinib in patients with advanced salivary gland cancers. Head Neck. 2015;37:644–649. doi:10.1002/hed.23647
80. Locati LD, Perrone F, Cortelazzi B, et al. A phase II study of sorafenib in recurrent and/or metastatic salivary gland carcinomas: translational analyses and clinical impact. Eur J Cancer. 2016;69:158–165. doi:10.1016/j.ejca.2016.09.022
81. Ho AL, Dunn L, Sherman EJ, et al. A phase II study of axitinib (AG-013736) in patients with incurable adenoid cystic carcinoma. Ann Oncol. 2016;27:1902–1908. doi:10.1093/annonc/mdw287
82. Argiris A, Ghebremichael M, Burtness B, Axelrod RS, Deconti RC, Forastiere AA. A phase 2 trial of bortezomib followed by the addition of doxorubicin at progression in patients with recurrent or metastatic adenoid cystic carcinoma of the head and neck: a trial of the Eastern Cooperative Oncology Group (E1303). Cancer. 2011;117:3374–3382. doi:10.1002/cncr.25852
83. Locati LD, Bossi P, Perrone F, et al. Cetuximab in recurrent and/or metastatic salivary gland carcinomas: a phase II study. Oral Oncol. 2009;45:574–578. doi:10.1016/j.oraloncology.2008.07.010
84. Dillon PM, Petroni GR, Horton BJ, et al. A Phase II study of dovitinib in patients with recurrent or metastatic adenoid cystic carcinoma. Clin Cancer Res. 2017;23:4138–4145. doi:10.1158/1078-0432.CCR-16-2942
85. Keam B, Kim SB, Shin SH, et al. Phase 2 study of dovitinib in patients with metastatic or unresectable adenoid cystic carcinoma. Cancer. 2015;121:2612–2617. doi:10.1002/cncr.29401
86. Kim DW, Oh DY, Shin SH, et al. A multicenter phase II study of everolimus in patients with progressive unresectable adenoid cystic carcinoma. BMC Cancer. 2014;14:795. doi:10.1186/1471-2407-14-795
87. Hotte SJ, Winquist EW, Lamont E, et al. Imatinib mesylate in patients with adenoid cystic cancers of the salivary glands expressing c-kit: a Princess Margaret Hospital phase II consortium study. J Clin Oncol. 2005;23:585–590. doi:10.1200/JCO.2005.06.125
88. Lin CH, Yen RF, Jeng YM, Tzen CY, Hsu C, Hong RL. Unexpected rapid progression of metastatic adenoid cystic carcinoma during treatment with imatinib mesylate. Head Neck. 2005;27:1022–1027. doi:10.1002/hed.20274
89. Ochel HJ, Gademann G, Röcken C, Wördehoff H. Effects of imatinib mesylate on adenoid cystic carcinomas. Anticancer Res. 2005;25:3659–3664.
90. Agulnik M, Cohen EWE, Cohen RB, et al. Phase II study of lapatinib in recurrent or metastatic epidermal growth factor receptor and/or erbB2 expressing adenoid cystic carcinoma and non adenoid cystic carcinoma malignant tumors of the salivary glands. J Clin Oncol. 2007;25:3978–3984. doi:10.1200/JCO.2007.11.8612
91. Ganesan P, Piha-Paul S, Naing A, et al. Phase I clinical trial of lenalidomide in combination with sorafenib in patients with advanced cancer. Invest New Drugs. 2014;32:279–286. doi:10.1007/s10637-013-9966-3
92. Chau NG, Hotte SJ, Chen EX, et al. A phase II study of sunitinib in recurrent and/or metastatic adenoid cystic carcinoma (ACC) of the salivary glands: current progress and challenges in evaluating molecularly targeted agents in ACC. Ann Oncol. 2012;23:1562–1570. doi:10.1093/annonc/mdr522
93. Ramalingam SS, Parise RA, Ramananthan RK, et al. Phase I and pharmacokinetic study of vorinostat, a histone deacetylase inhibitor, in combination with carboplatin and paclitaxel for advanced solid malignancies. Clin Cancer Res. 2007;13:3605–3610. doi:10.1158/1078-0432.CCR-07-0162
94. Goncalves PH, Heilbrun LK, Barrett MT, et al. A phase 2 study of vorinostat in locally advanced, recurrent, or metastatic adenoid cystic carcinoma. Oncotarget. 2017;8:32918–32929. doi:10.18632/oncotarget.16464
95. Even C, Lassen U, Merchan J, et al. Safety and clinical activity of the Notch inhibitor, crenigacestat (LY3039478), in an open-label phase I trial expansion cohort of advanced or metastatic adenoid cystic carcinoma. Invest New Drugs. 2020;38:402–409. doi:10.1007/s10637-019-00739-x
96. Tchekmedyian V, Sherman EJ, Dunn L, et al. Phase II study of lenvatinib in patients with progressive recurrent or metastatic adenoid cystic carcinoma. J Clin Oncol. 2019;37:1529–1537. doi:10.1200/JCO.18.01859
97. Locati LD, Galbiati D, Calareso G, et al. Patients with adenoid cystic carcinomas of the salivary glands treated with lenvatinib: activity and quality of life. Cancer. 2020;126:1888–1894. doi:10.1002/cncr.32754
98. Atallah S, Casiraghi O, Fakhry N, et al. A prospective multicentre REFCOR study of 470 cases of head and neck Adenoid cystic carcinoma: epidemiology and prognostic factors. European Journal of Cancer. 2020;130:241–249. doi:10.1016/j.ejca.2020.01.023
99. Fendler WP, Reinhardt S, Ilhan H, et al. Preliminary experience with dosimetry, response and patient reported outcome after 177Lu-PSMA-617 therapy for metastatic castration-resistant prostate cancer. Oncotarget. 2017;8:3581–3590. doi:10.18632/oncotarget.12240
100. Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10):e1–e34. doi:10.1016/j.jclinepi.2009.06.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.