")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Blended Learning with Video Demonstrations Enhances Dental Students’ Achievements in Tooth Carving
Authors Alzer H, Ismail NH, Alsoleihat F
Received 28 August 2023
Accepted for publication 28 November 2023
Published 15 December 2023 Volume 2023:14 Pages 1425—1431
DOI https://doi.org/10.2147/AMEP.S426199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Heba Alzer,1 Noor H Ismail,1 Firas Alsoleihat1,2
1Department of Restorative Dentistry, School of Dentistry, The University of Jordan, Amman, Jordan; 2Department of Restorative Dentistry and Basic Medical Sciences, Faculty of Dentistry, University of Petra, Amman, 11196, Jordan
Correspondence: Heba Alzer, Department of Restorative Dentistry, School of Dentistry, The University of Jordan, Amman, 11942, Jordan, Tel +96265355000-23537, Fax +962 6 5355 52, Email [email protected]
Background: Learning fine motor skill is central to preclinical dental education. Dental students are introduced to anatomical tooth carving to facilitate the development of their fine motor skill and manual dexterity. Various carving technique exists, such as wax build-up, and geometric (block carving technique). Since substantial laboratory Time and instructors’ effort are required to teach students the desired techniques, blended learning approach via pre-recorded demonstration may improve the teaching and learning efficiency of anatomical tooth carving. For years, we used the Geometric method to teach preclinical dental students to carve down tooth sculptures after performing live demonstrations for them. Multiple practical laboratory demonstrations are necessary to deepen the student’s comprehensive understanding of dental anatomical features and teach them correct instrumentation; this is time-consuming and challenging due to limited laboratory hours and limited view field. Accordingly, in 2016 the teaching staff created videos for tooth drawing, carving, and identification, and uploaded them to the students’ university platform. Years later, we decided to perform this retrospective study.
Objective: To assess the enhancement in students’ tooth carving skills after implementing blended learning with video demonstrations.
Methods: The student’s total grades were used for comparative purposes. The students’ total grades between 2010 and 2019 were collected and categorized into two groups: Group 1 (n=858), which learned tooth carving by the Geometric method after live demonstrations, and Group 2 (972), which benefited from blended learning with video demonstrations in learning. The two groups’ mean, median, mode, Percentile 75, and Percentile 90 were compared.
Results: Group 2 showed higher grades than group 1, and the differences between the two groups’ mean and median were statistically significant p< 0.001. Moreover, the mode, P75 and P90 favored group 2.
Conclusion: Results show that blended learning with video demonstrations enhanced the achievements of dental students in tooth carving.
Keywords: dental anatomy, blended learning, video demonstrations, dental morphology, tooth carving, dental education
Introduction
Most dental treatments are complex and require the integration of theoretical knowledge along with fine psychomotor skills. Development of fine psychomotor skills of dental students starts in the preclinical years before the students proceed to carrying out clinical activities on patients in the following clinical years of their study. Establishing and improvement of fine manual and finger dexterity is challenging for dental students, it involves a continuous interaction between cognitive, sensory, and neuromuscular processes.1 Variant tasks are developed to accomplish that, including simulating clinical activities in the laboratory which enhance visual and tactile sensory input systems, combining theoretical and tactile feedback to evaluate the finished tasks which enhance cognitive abilities and repeating the simulated tasks which train the neuromuscular system to master these fine motor movements.2 One of the earliest modules given to the dental students to start training fine manual dexterity is dental anatomy module. The dental anatomy module is given to preclinical dental students early in the curriculum as an introduction to human dentition. Students learn to identify teeth by their anatomy, how teeth are related to the rest of the dentition, and how to restore anatomical features for future dental practices. This module provides the students with one of the basic skills needed to practice clinical dentistry efficiently; for instance, a composite restoration placed on a tooth should mimic the original anatomy to be in harmony with the rest of the dentition.3
In the practical part of the dental anatomy module, the students learn to identify teeth surface details and how to reproduce them either by the Geometric method we utilize at our school, which consists of carving down teeth using blocks of wax bigger than actual teeth, or by the Build-up technique, where teeth are built up in real size on a gypsum model.4 Both methods utilize books, manuals, samples, and models of teeth to illustrate the tooth morphology to students before a practical demonstration is presented to them.4,5 Students are trained to develop appropriate psychomotor skills and tactile sensation. As a result, dental students should be able to apply this knowledge to restore the aesthetics and function of the teeth and the accompanying oral structures in the following clinical study.5
In our school the module duration is fourteen weeks, the students learn to draw and carve the following teeth: the maxillary permanent central incisor, the maxillary permanent canine, the maxillary and mandibular first premolars, the maxillary and mandibular first molars. Moreover, they learn how to identify both permanent and deciduous teeth.
Among the newer innovative teaching methods is the use of digital media, programs, and software, which have several characteristics that may enhance the learning of dental anatomy.6,7 These methods can be used anytime and anywhere and can be interactive and intuitive, allowing students to learn at their own pace. They are easier to use, engage three-dimensional models, and help students’ self-assessment. These digital means were used only to give instructions and evaluations digitally to the students.4,8–10
The advantages and disadvantages of teaching tooth carving using the traditional methods are not previously reported in the literature. However, we noticed through years of teaching the Geometric method that it allows the students to imagine the morphological features of a tooth, magnified, and provided a touchable way to reproduce them by hand. On the other hand, this method may dictate an already existing good talent, tactile sensation, and imagination. To overcome this hindrance, the repetition of practical laboratory demonstrations is necessary to deepen the students’ comprehensive understanding of dental anatomical features. We concluded that an adjunct method is to deepen the knowledge of dental anatomical features and how instruments are correctly used to reproduce them. We hypothesized that providing tutorial videos that are available for students anytime, anywhere, repeating the information as much as the student needs, would lead students to reproduce teeth carvings in better quality. Blended learning with video demonstrations was added to the course outline in 2016. Since then, a remarkable difference has been noticed in the quality of the carvings handed in by the students. The present study is a retrospective cohort study that compared the students’ performance in tooth carving before and after blended learning with the video demonstrations included in the course as an adjunct to the Geometric method.
Methods
This study is a retrospective cohort study that was conducted on the student’s results after years of introducing the tutorial videos as an adjunct to the Geometric method, and comparing these results to the earlier years of conventional teaching of dental anatomy by the Geometric method without the tutorial videos. Fortunately, as per our standards, the educational processes, and the evaluation systems, which are reported here in the methods, were and are still standardized which facilitated designing the study.
Creating Video Demonstrations
In 2016, the instructors who taught the dental anatomy practical course, videotaped teeth drawing and carving demonstrations, and uploaded them to the student’s university platform. The videos were approximately twenty minutes long and in English. The videos introduced and explained step-by-step all the anatomical features of the tooth to be carved during carving. The anatomical features of each aspect of the tooth were drawn on the block, and the correct method of handling the carving instruments was shown. The final carved tooth is revised from all aspects to ensure that all anatomical features explained at the beginning of the video and in the theoretical lectures are visible clearly on each aspect.
Carving Training
Each week during the conduction of the dental anatomy practical course, students were given a lecture on the anatomy and morphology of a specific tooth. The following week, the students learn how to carve a model of the same tooth in the laboratory session through a live demonstration. After initial instructions and demonstrations of carving instrument usage and basic carving techniques, they try to mimic the previously carved tooth, done by the instructors. After the blended learning with video demonstrations was introduced to the course, the students were assigned to watch the videos at home on the university platform before each practice session and to try to carve a tooth model on their own and bring all the carved teeth for feedback from the instructors in the laboratory to ensure that they have watched the video. Those lacking proper equipment or internet at home could benefit from the school computer labs as often as needed.
Moreover, the video was broadcasted in the laboratory before the students started carving, to discuss any points the students feel needs to be illuminated or explained. The live demonstrations were canceled, so students could begin carving immediately, preserving the laboratory time. Instructors substituted demonstrations with one-to-one guidance during the lab to the students when needed. The students were allowed to watch the videos during the practice weeks in the laboratory and while practicing tooth carving at home.
In both teaching methods, students were given approximately two weeks to practice carving any assigned tooth. They were recommended the textbook, Wheeler’s Dental Anatomy, Physiology, and Occlusion by Stanley Nelson as a reference.
They learn to carve the maxillary central incisor, the maxillary canine, the first maxillary and mandibular premolars, and the first maxillary and mandibular molars. Throughout the course, they take three carving exams where they should carve one anterior tooth, one premolar, and one first molar. During the exams, the students worked independently in an invigilated environment.
Data Collection and Criteria
The students’ total grades, which are the sums of three carving tests of three teeth (one anterior, one premolar, and one first molar) performed throughout the course, were used to perform the statistical analysis for comparison purposes. Students’ total grades between 2010 and 2019 were collected and categorized into two groups. The data from 2010 to 2014 represents the students’ grades in the dental anatomy practical course before blended learning with video demonstrations. This group (group 1) has 858 students. Meanwhile, the data from 2016–2019 represent the students’ grades after blended learning with video demonstrations was introduced. This group (group 2) has 972 students. As this is a retrospective cohort study, the data was collected, and then the statistical analysis was performed. The data for 2015 were excluded as the instructors were different, and the teaching method in that year was the Build-up technique instead of the Geometric technique.
Assessment Method and Risk of Bias
The students’ total grades are the sums of three carving tests of three teeth performed throughout the course, one anterior 30%, one premolar 30%, and one first molar 40%. All summed up to be out of 100 points. Students should achieve at least 50 points to pass the course. The grade for each carved tooth is an average of two grades given by two instructors. Grading was anonymous. The criteria for evaluating and grading carved teeth have been set for decades, and they are standard and stable. Three instructors with years of experience teaching dental anatomy created the rubrics (Supplementary Tables 1–6). They included them in the course outline to be distributed to all students at the beginning of each semester. The reference textbook, Wheeler’s Dental Anatomy, Physiology, and Occlusion by Stanley Nelson was chosen as a rubric guideline. Rubrics and instructors were stable during the study timeline except in 2015. The data for 2015 were excluded as the instructors were different, and the teaching method in that year was the Build-up technique instead of the Geometric technique.
Statistical Analysis
An independent two-sample t-test was used to assess the statistical significance of the difference between the means of group 1 and group 2 grades (SPSS, Version 17.0, Inc., Chicago, IL). Levenes’ test was performed to evaluate the distribution of both groups’ data before an independent two-sample t-test was performed, and both showed normal distribution.
Furthermore, the median, mode, standard deviation, P75, and P90 were compared. Moreover, the median test based on the Chi-square analysis was performed to examine the significance of the difference between the medians (SPSS, Version 17.0, Inc., Chicago, IL).
Results
A statistically significant difference was found between the grades mean of group 1, taught by the Geometric method solely (n=858, mean=56.09; SD=11.84), and that of group 2, taught by blended learning with video demonstrations (n=972, mean= 63.21; SD=15.45) (p<0.001, Table 1). In addition, the median, mode, and percentiles 75 and 95 were calculated and compared between the two groups (Table 1 and Figure 1). The median elevated from 57.54 in group 1 to 64.83 in group 2, and the median test showed a significant difference between the two groups (p<0.001, Table 1). The mode showed a leap from 49.00 to 71.00, meaning more students could pass the course and get a grade higher than 50. The percentiles show that only 25% of group 1 achieved a grade higher than 64.38 (P75), while 25% of group 2 students achieved a grade higher than 75.00, and 10% of group 2 were able to achieve a grade higher than 81 (P90) while only 10% of group 1 where able to achieve a grade greater than 69.85.
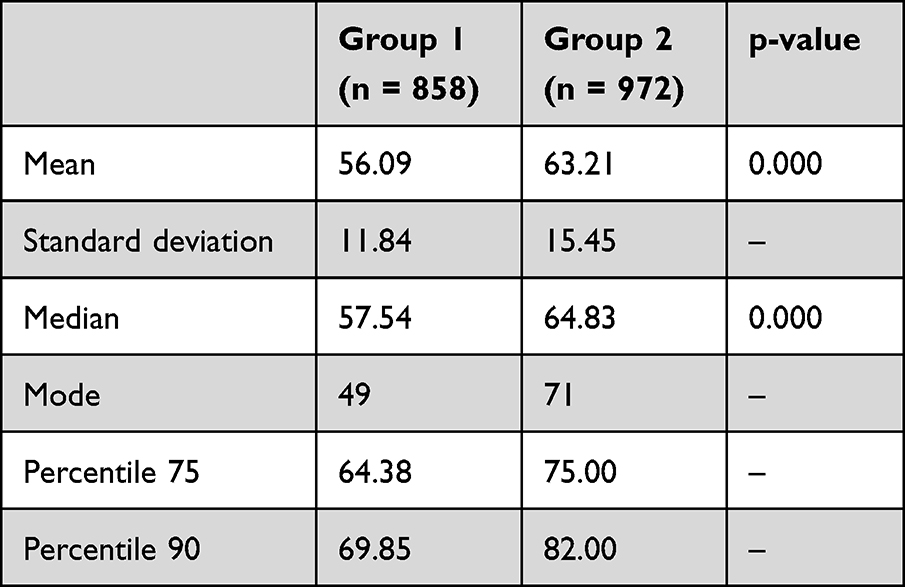 |
Table 1 Grades of Dental Anatomy Practical Course Before (Group 1) and After (Group 2) Blended Learning with Video Demonstrations, Compared by Mean, Median, Mode, Standard Deviation, and Percentiles P75, P90 |
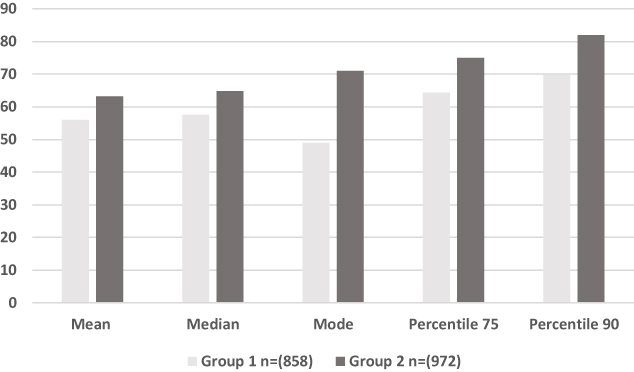 |
Figure 1 Grades of dental anatomy practical course before (group 1) and after (group 2) blended learning with video demonstrations, compared by mean, median, mode, and percentiles P75, P90. |
Discussion
In the dental anatomy practical course, teaching teeth carving by Geometric, or Build-up techniques involves exercises that include creating drawings of teeth, and sculpting them into blocks of wax using carving tools after a live demonstration. The objectives are to provide students with essential cognitive skills related to teeth, and promote psychomotor skills to recreate proper tooth form competently in restorative clinical procedures.11,12 Both methods have some shortcomings, as to mention but not limited to; the demonstrations had to be repeated multiple times due to the limited field of view during a demonstration and the increasing number of students despite the limited time of the laboratory. Furthermore, many students could not understand and repeat the steps after watching a demonstration only once.
New methods are being introduced to facilitate learning tooth morphology; DVDs, programs, and software have shown promising results, introducing interactivity and independence in learning experiences.4,8–10,13,14 Some advantages of these methods include access to information anytime, many times, and anywhere, providing the student with flexible hours for studying independently of the teacher. These digital means of teaching dental anatomy and teeth carving were used as an auxiliary-teaching-methods or as a replacement for the traditional laboratory instructions and demonstrations, showing that they may replace the traditional teaching methods or at least enhance the students understanding, course engagement, and achievements.4,8–10 The studies mentioned above were based on giving instructions and evaluations digitally to the students. Literature showed no previous reports of using tutorial videos of dental anatomy carvings to enhance the student’s results in dental anatomy laboratories. On the other hand, multiple Studies have reported utilizing educational videos to teach or enhance students’ performance in prosthodontics and operative laboratory procedures.15–19
In this study, blended learning with video demonstrations that show a step-by-step reproduction of teeth in the Geometric method was introduced to the students since 2016.
A rubric with specific criteria has been established to help students develop a critical sense of the quality of a dental carving (Supplementary Tables 1–6) and to bypass any bias through the grading procedures, as there were specific criteria to follow. Nevertheless, the grading was anonymous, and the grade was taken as an average of two grades given by two different instructors.
The statistical analysis was performed with the students’ total grades to compare groups 1 and 2, before and after the blended learning with video demonstrations respectively (see materials and methods). Groups 1 and 2 are two independent groups with normal data distribution, as Levenes’ test showed. Accordingly, we choose to utilize the independent two-sample t-test, which determines whether a statistically significant difference exists between the means of two normally distributed unrelated groups. Moreover, the median test based on the Chi-square determines if the medians of two independent samples are equal and if a significant statistical difference exists between them. The statistical analysis showed that all the measured cues were enhanced in group 2 (Table 1 and Figure 1). Percentiles analysis showed that a higher percentage of students could pass the course, and higher grades were achieved in group 2, which elevated the mean, median, and mode. This progress was observable to us as instructors; in previous years, many students handed unfinished teeth carvings in the exams, which is rarely observed now after the introduction of blended learning with video demonstrations.
This is the first study to report utilizing blended learning by video demonstrations created by the academic staff to enhance students’ achievement in dental carvings. It was challenging to create high-quality videos to detect the fine details of dental carvings, as a high-quality camera is expensive and requires professional videotaping personnel. This study suggests that blended learning with video demonstrations showing clear and comprehensive information would replace traditional laboratory live demonstrations to teach dental carvings.
Blended learning has been introduced to dental students previously in the dental anatomy theoretical course, it enhanced students’ accessibility, self-assessment, and level of engagement.20 In one report, utilizing flipped classroom which consisted of a self-study period before each class session and in-class activities and discussion where students were asked to review a dental anatomy lecture video, study the required dental anatomy textbook and take a brief quiz prior to each of the five classes has been reported to enhance students’ scores in dental waxing.21 Moreover, augmented reality, virtual reality and other digital means are introduced recently for health sciences teaching and they still under investigations.22–25 For instance, some efforts to develop the students’ skills in replicating dental morphology implemented augmented reality, by providing virtual teeth models that is displayed in the real world by Microsoft Hololens, suggest that augmented reality can be helpful in dental anatomy education, but now they are still not suitable replacements for physical 3D models.26
In the future we seek to upgrade our efforts to include developing the dental student’s self-assessment skills of their dental carvings; it was reported that a statistically significant correlation exists between self-assessment ability and waxing performance in dental students.27 Accordingly, we are establishing a website where students can upload photos of their carvings and use a special software designed by us to assess and compare their carvings to the correct anatomical sculptures desired from them (unpublished work).
Conclusions
Competence in dental anatomy and good practice are fundamental to achieving excellent dental sculptures and perfect restoration in the future. Thus, theoretical and practical support for dental carving students should be improved. The results of this study suggested investing the new technological horizons as blended learning with video demonstrations. This approach attracts students because it allows for more independent learning anytime, anywhere, and at the student’s preferred pace.
Consent and Ethical Approval
Not applicable as the study was conducted retrospectively and anonymously on the student’s grades. This type of study is exempted from approval by the ethics committee at the University of Jordan.
Research Data and Material Availability
The data and material required to produce the above findings are available upon request from the corresponding author.
Acknowledgment
This study was conducted in the School of Dentistry at the University of Jordan.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
Funding
No funding was received for conducting this study.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Mulder T. Motor control and learning: implications for neorogogical rehabilitation. In: Greenwood I, editors. Handbook of Neurological Rehabilitation. Psychology press; 2003.
2. El-Kishawi M, Khalaf K, Winning T. How to improve fine motor skill learning in dentistry. Berger SB, ed. Int J Dent. 2021; 2021: 6674213. doi: 10.1155/2021/6674213
3. Nelson SJ. Wheeler’s Dental Anatomy. Physiology Occlusion. Elsevier Health Sciences; 2015.
4. de Azevedo Rde A, da Rosa WL, da Silva AF, Correa MB, Torriani MA, Lund RG. Comparative effectiveness of dental anatomy carving pedagogy: a systematic review. J Dent Educ. 2015;79(8):914–921. doi:10.1002/j.0022-0337.2015.79.8.tb05981.x
5. Nayak MT, Sahni P, Singhvi A, Singh A. The perceived relevance of tooth carving in dental education: views of practicing dentists and faculty in West India. Educ Health. 2014;27(3):238–242. doi:10.4103/1357-6283.152177
6. de Azevedo RA, Correa MB, Torriani MA, Lund RG. Optimizing quality of dental carving by preclinical dental students through anatomy theory reinforcement. Anat Sci Educ. 2018;11(4):377–384. doi:10.1002/ase.1752
7. Kilistoff AJ, Mackenzie L, D’Eon M, Trinder K. Efficacy of a step-by-step carving technique for dental students. J Dent Educ. 2013;77(1):63–67. doi:10.1002/j.0022-0337.2013.77.1.tb05444.x
8. Nance ET, Lanning SK, Gunsolley JC. Dental anatomy carving computer-assisted instruction program: an assessment of student performance and perceptions. J Dent Educ. 2009;73(8):972–979. doi:10.1002/j.0022-0337.2009.73.8.tb04786.x
9. Mitov G, Dillschneider T, Abed MR, Hohenberg G, Introducing PP. and evaluating morphodent, a web-based learning program in dental morphology. J Dent Educ. 2010;74(10):1133–1139. doi:10.1002/j.0022-0337.2010.74.10.tb04968.x
10. Bogacki RE, Best A, Abbey LM. Equivalence study of a dental anatomy computer-assisted learning program. J Dent Educ. 2004;68(8):867–871. doi:10.1002/j.0022-0337.2004.68.8.tb03836.x
11. Obrez A, Briggs C, Buckman J, Goldstein L, Lamb C, Knight WG. Teaching clinically relevant dental anatomy in the dental curriculum: description and assessment of an innovative module. J Dent Educ. 2011;75(6):797–804. doi:10.1002/j.0022-0337.2011.75.6.tb05108.x
12. Curriculum guidelines for occlusion. Section on dental anatomy and occlusion of the American association of dental schools. J Dent Educ. 1993;57(5):384–387. doi:10.1002/j.0022-0337.1993.57.5.tb02763.x
13. Lee LM, Nagel RW, Gould DJ. The educational value of online mastery quizzes in a human anatomy course for first-year dental students. J Dent Educ. 2012;76(9):1195–1199. doi:10.1002/j.0022-0337.2012.76.9.tb05374.x
14. Howerton WB, Enrique PR, Ludlow JB, Tyndall DA. Interactive computer-assisted instruction vs. lecture format in dental education. J Dent Hyg. 2004;78(4):10.
15. Cheng L, Kalvandi M, McKinstry S, et al. Application of denteach in remote dentistry teaching and learning during the COVID-19 pandemic: a Case Study. Front Robot AI. 2021;7: doi:10.3389/frobt.2020.611424
16. Fayaz A, Mazahery A, Hosseinzadeh M, Yazdanpanah S. Video-based learning versus traditional method for preclinical course of complete denture fabrication. J Dent. 2015;16(1 Suppl):21–28.
17. Iqbal A, Ganji KK, Khattak O, et al. Enhancement of skill competencies in operative dentistry using procedure-specific educational videos (e-learning tools) post-covid-19 era—a randomized controlled trial. Int J Environ Res Public Health. 2022;19(7):4135. doi:10.3390/ijerph19074135
18. Gadbury-Amyot CC, Purk JH, Williams BJ, Van Ness CJ. Using tablet technology and instructional videos to enhance preclinical Dental laboratory learning. J Dent Educ. 2014;78(2):250–258. doi:10.1002/j.0022-0337.2014.78.2.tb05675.x
19. Aragon CE, Zibrowski EM. Does exposure to a procedural video enhance preclinical dental student performance in fixed prosthodontics? J Dent Educ. 2008;72(1):67–71. doi:10.1002/j.0022-0337.2008.72.1.tb04454.x
20. Ullah R, Siddiqui F, Adnan S, Afzal AS, Sohail Zafar M. Assessment of blended learning for teaching dental anatomy to dentistry students. J Dent Educ. 2021;85(7):1301–1308. doi:10.1002/jdd.12606
21. Chutinan S, Riedy CA, Park SE. Student performance in a flipped classroom dental anatomy course. Eur J Dent Educ. 2018;22(3):e343–e349. doi:10.1111/eje.12300
22. Susilawati E, Johari A, Marzal J, Anggereini E. Effects of multimedia e-books and augmented reality on knowledge and skills of health sciences students: a systematic review. J Client-Centered Nurs Care. 2022;8(2):99–110. doi:10.32598/JCCNC.8.2.380.2
23. Dolega-Dolegowski D, Proniewska K, Dolega-Dolegowska M, et al. Application of holography and augmented reality based technology to visualize the internal structure of the dental root – a proof of concept. Head Face Med. 2022;18(1). doi:10.1186/s13005-022-00307-4
24. Blanchard J, Koshal S, Morley S, McGurk M. The use of mixed reality in dentistry. Br Dent J. 2022;233(4):261–265. doi:10.1038/s41415-022-4451-z
25. Dzyuba N, Jandu J, Yates J, Kushnerev E. Virtual and augmented reality in dental education: the good, the bad and the better. Eur J Dent Educ. 2022; doi:10.1111/eje.12871
26. Grad P, Przeklasa-Bierowiec AM, Malinowski KP, Witowski J, Proniewska K, Tatoń G. Application of HoloLens based augmented reality and three-dimensional printed anatomical tooth reference models in dental education. Anat Sci Educ. 2023;16(4):743–755. doi:10.1002/ase.2241
27. Cevallos M, Pardo A, Kakadia R, Jiang T, Chutinan S. Can self-assessment ability predict student performance in a dental anatomy course? Eur J Dent Educ. 2023. doi:10.1111/eje.12916
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.