")
Back to Journals » Journal of Pain Research » Volume 17
Bone Cements Used in Vertebral Augmentation: A State-of-the-art Narrative Review
Authors Williams TD , Adler T, Smokoff L, Kaur A, Rodriguez B, Prakash KJ, Redzematovic E, Baker TS, Rapoport BI, Yoon ES , Beall DP , Dordick JS, De Leacy RA
Received 30 August 2023
Accepted for publication 26 January 2024
Published 13 March 2024 Volume 2024:17 Pages 1029—1040
DOI https://doi.org/10.2147/JPR.S437827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Krishnan Chakravarthy
Tyree D Williams,1– 3 Talia Adler,2,4 Lindsey Smokoff,2,4 Anmoldeep Kaur,2,5 Benjamin Rodriguez,2,3,6 Kavita Jyoti Prakash,6 Edib Redzematovic,2 Turner S Baker,2,3,7 Benjamin I Rapoport,2,3 Edward S Yoon,8 Douglas P Beall,9 Jonathan S Dordick,1 Reade A De Leacy3
1Biomedical Engineering, Rensselaer Polytechnic Institute, Troy, NY, USA; 2Sinai BioDesign, Mount Sinai Medical System, New York, NY, USA; 3Department of Neurosurgery, Mount Sinai Medical System, New York, NY, USA; 4Columbia University School of General Studies, New York, NY, USA; 5Department of Neuroscience, Smith College, Northampton, MA, USA; 6Icahn School of Medicine at Mount Sinai, New York, NY, USA; 7Department of Population Health Science & Policy, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 8Hospital for Special Surgery, New York, NY, USA; 9Spine Fracture Institute, Oklahoma City, OK, USA
Correspondence: Benjamin Rodriguez, Department of Neurosurgery, Mount Sinai Medical System, One Gustave L. Levy Place, Box 1136, New York, NY, USA, Tel +1 615 524-0211, Email [email protected]
Abstract: Vertebral compression fractures (VCFs) are common in osteoporotic patients, with a frequency projected to increase alongside a growing geriatric population. VCFs often result in debilitating back pain and decreased mobility. Cement augmentation, a minimally invasive surgical technique, is widely used to stabilize fractures and restore vertebral height. Acrylic-based cements and calcium phosphate cements are currently the two primary fill materials utilized for these procedures. Despite their effectiveness, acrylic bone cements and calcium phosphate cements have been associated with various intraoperative and postoperative incidents impacting VCF treatment. Over the past decade, discoveries in the field of biomedical engineering and material science have shown advancements toward addressing these limitations. This narrative review aims to assess the potential pitfalls and barriers of the various types of bone cements.
Keywords: osteoporosis, vertebral compression fractures, bone cement, vertebroplasty, kyphoplasty, vertebral augmentation
Introduction
Over one million cases of vertebral compression fractures (VCFs) occur annually in the United States and remain the most common fragility fracture in osteoporotic patients.1 The two most common treatments for VCFs are vertebroplasty, in which injectable bone cement (BC) is administered into the affected vertebrae, and vertebral augmentation with balloon kyphoplasty (BK), where a non-compliant balloon tamp is placed within the affected vertebrae to normalize the vertebral height as much as possible prior to cementing. The primary goals of vertebral augmentation (VA) are vertebral anatomy restoration and optimal fracture stabilization.
Cement leakage is the most prevalent procedural adverse event associated with VA.2 The vast majority of cement extravasations are clinically silent and of no consequence. However, in rare circumstances, it has been associated with serious adverse events. Acrylic bone cements (ABCs) and calcium phosphate cements (CPCs) are sensitive to some extrinsic factors, which influence handling properties resulting in inconsistent mechanical properties following cement setting.3,4 ABCs have been linked with local tissue necrosis during polymerization, and they are typically classified as non-biomimetic.5,6 CPCs provide an opportunity to establish bone regeneration by increasing osteoconductivity and drug or growth factor encapsulation. However, these cements struggle with high rates of cytotoxicity, excessive cost, and poor mechanical properties.4 There is a clear opportunity for further development and improvement of CPCs.
To the authors’ knowledge, the most recent, comprehensive review regarding ABCs was published by Gladius Lewis in 1997.7 In light of advancements in the field, a current extensive review evaluating ABCs and CPCs was thought to be needed. A review of bone cements was last published by Yousefi et al in 2019, but only evaluated a limited number of ABCs and CPCs and did not comprehensively examine novel formulations.7 This paper aims to examine the properties and characteristics associated with both types of bone cements and address them by investigating new alternative formulas that limit the adverse effects most commonly associated with commercially available bone cements used for treating painful VCFs.
Methods
A search was conducted utilizing PubMed, Google Scholar, and ScienceDirect with terms such as “vertebral compression fracture”, “vertebral augmentation”, “kyphoplasty”, “vertebroplasty”, “bone cement (BC)”, “bone cement (BC) complications”, “osteoporosis”, “spinal fracture reduction systems”. Authors identified sources independently. Articles included were published between 2018 and 2023 and were not duplicated between authors. Full-text articles, published in English, or with a published English translation were selected for review. Information used to write this paper is collected from Table 1 outlining our methods.
 |
Table 1 The Search Strategy Summary |
Ideal Characteristics of Bone Cement
Bone cements used for the treatment of VCFs must meet certain clinical and economic requirements and possess the necessary physical properties to be practical as well as safe to use. Bone cements for commercial use must have a bending modulus greater than or equal to 1800 megapascals and a bending strength greater than or equal to 50 megapascals. Additionally, bone cement must have a compressive strength greater than or equal to 70 megapascals to ensure it is capable of high-load bearing and compatible with trabecular bone. Ideal bone cements for VCF treatment should have low exothermic release and relatively fast curing times, with the material being non-toxic to surrounding tissue.4 Optimally, bone cements should be osteoconductive and capable of stimulating new bone formation.8–10 Commercially utilized bone cements typically consist of a powder monomer, polymethyl methacrylate (PMMA), and a liquid monomer, methyl methacrylate (MMA). Bone cements are self-curing and the mixing of the two components initiates the polymerization process. Alterations to the powder-to-liquid ratio of bone cement can alter its mechanical properties and biological characterization.
Acrylic Bone Cements
Acrylic bone cements (ABCs) are currently the gold standard due to low cost, ease of use, and durability of the treatment. Physicians have a variety of commercially available products to choose from (Table 2). These cements are associated with monomer toxicity and significant exothermic release intraoperatively, thereby limiting the volume of cement that can be used in a single setting.11 PMMA BCs are the most commonly used BCs for VA and are typically used in medium and high load-bearing applications.11,12 ABCs generally have a compressive strength greater than 100 MPa, which is 30% higher than the ISO standard 5833’s minimum compressive strength requirement for BCs (Table 3).5 A mismatch between mechanical properties of fractured bone and nonfractured bone may be partially reversed by the addition of an adequate amount of BC and may result in less abnormal strain on the adjacent vertebral bodies.13
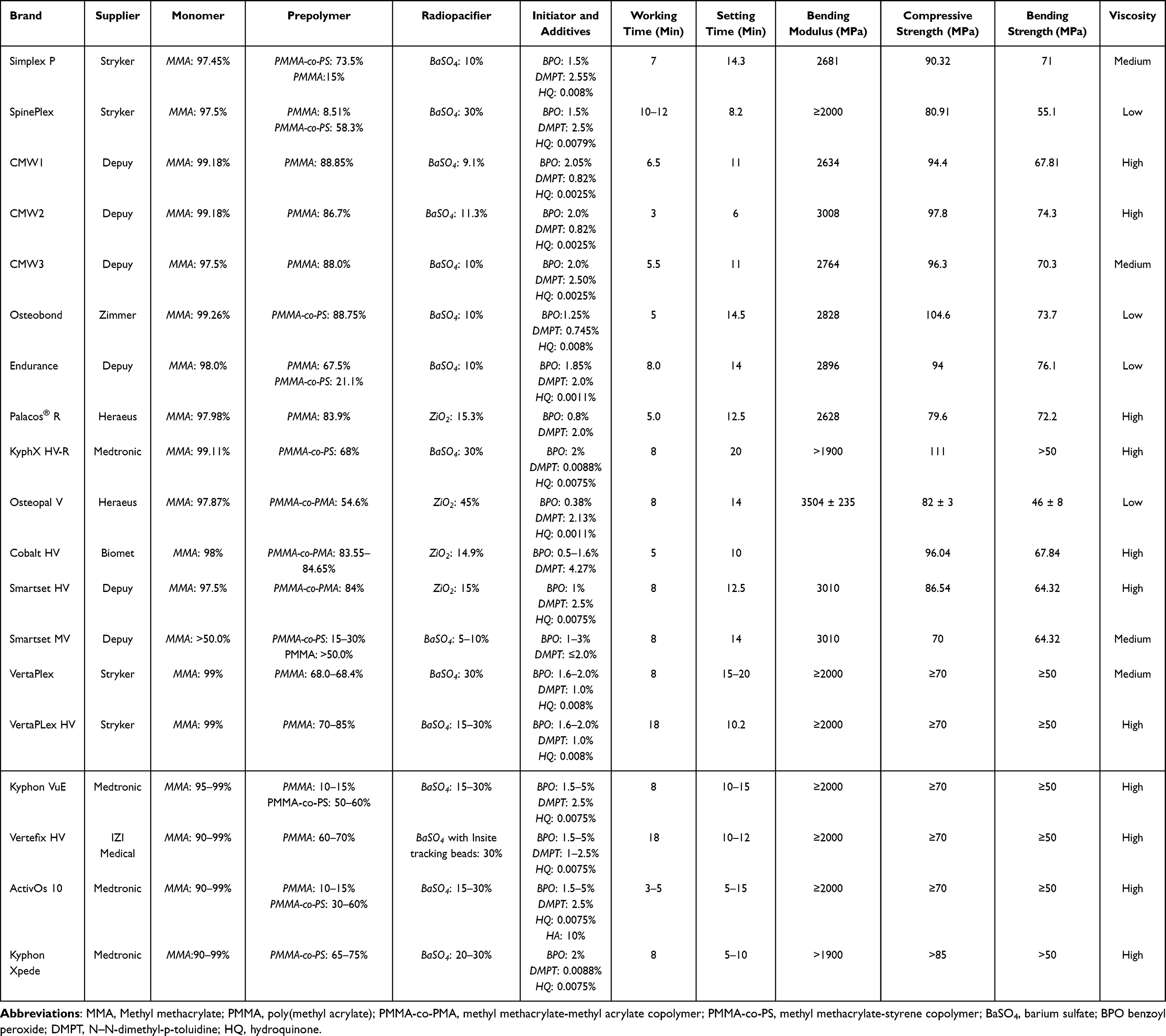 |
Table 2 Commercially Available Acrylic Bone Cements (ABCs) |
 |
Table 3 Mechanical Properties of Commercial Acrylic Bone Cements |
When engineering ABCs, cement viscosity is one of the most important characteristics. The viscosity of the cement affects injectability, leakage, retention in the vertebral body, and the final mechanical properties of the set cement.5 ABCs are prone to high exothermic releases during the polymerization process that can sometimes cause thermal necrosis of bone cells due to the tendency of collagen to denature when exposed to prolonged temperatures above 56 C.5 Increasing the viscosity of cement used in percutaneous vertebroplasty (PVP) decreases leakage and increases cement retention during injection when compared to PVP with low viscosity cement.14,15 While increased cement viscosity can also result in greater strength, it requires greater injection force and potentially earlier curing. The increased force may result in an insufficient volume of injected cement and potentially approach or surpass the physical limit of the human body.14
Two of the most commonly examined ABCs on the market for VCF are Palacos R (Heraeus) and Simplex P (Stryker) (Table 2). Palacos R is a green cement, allowing for better visualization for intraoperative teams to discern between bone and cement in comparison to white bone cements like Simplex P.16 Palacos R is a high viscosity cement with a compressive strength of 79.5 MPa, allowing for more compatibility with surrounding bone. Simplex P is a medium viscosity cement with a compressive strength of 90.32 MPa. In comparison to Simplex P, Palacos R has better long-term stability due to a higher molecular weight and non-radiation sterilization.17 A common complication associated with both Palacos R and Simplex P is tissue necrosis due to high exothermic releases.18 The price of one Palacos R high viscosity cement is $60 per 40 g, whereas Simplex P costs $70 per 40 g.19
Calcium Phosphate Cement
Calcium phosphate cements (CPCs) have been researched and in clinical use since the 1980s. They have unique attributes that are capable of self-hardening but are less commonly utilized than ABCs (Tables 4 and 5).16–19 The setting reaction mechanisms of CPCs can be manipulated by changing the solubility of compounds and the entanglement of precipitated crystals causing the hardening.5,20 These cement compounds have been shown to cure within 20 min but do not fully set for 12–48 h (Table 4). CPCs are biodegradable, bioresorbable, osteoconductive, and generate little to no heat during the curing process.21,22 Additionally, they are microporous which allows for transport of nutrients and metabolic waste permitting them to be bioactive.22
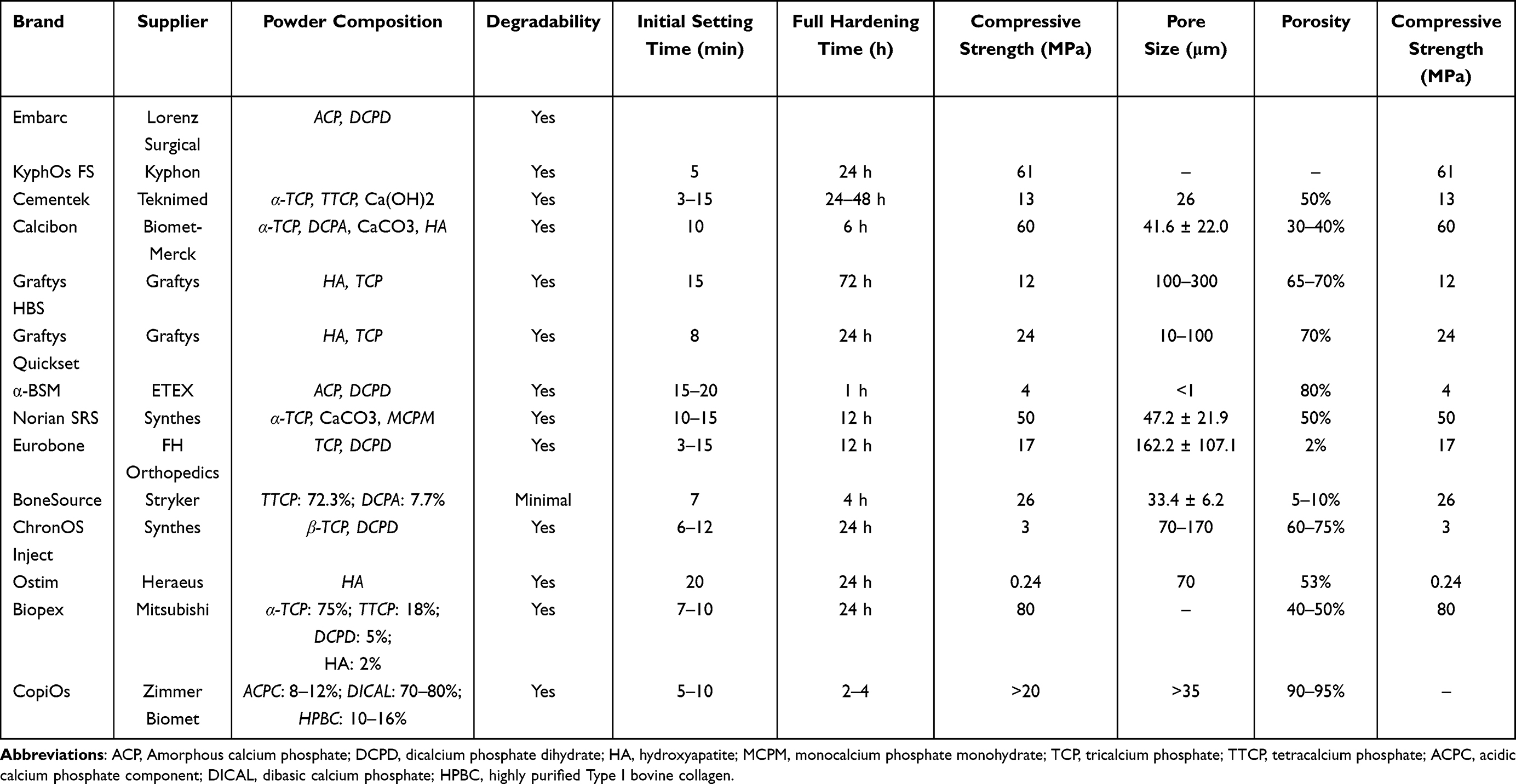 |
Table 4 Commercially Available Calcium Phosphate Bone Cements (CPCs) |
 |
Table 5 Mechanical Properties of Commercial Calcium Phosphate Bone Cements |
Biomechanically, they have low strength and are recommended for use in low load bearing sites, as they have a high predisposition to fracture and are brittle23–25 Compressive strength for CPCs ranges from 0.2 MPa to 184 MPa (Table 5),4,26 far inferior to that of ABCs. They have poor injectability as a result of solid and liquid-phase separation during delivery, which negatively impacts the intraoperative injectability.27 Bone ingrowth and fast resorption are limited by the typical absence of macropores in most CPCs.5,28 The addition of pore-forming additives, namely water-soluble polymers, biodegradable polymers, collagen, glucose, and biphasic calcium phosphate, has been proposed to improve the resorbability of CPCs.5 Additives that improve resorbability also affect the setting time, compressive strength, viscosity, and dispersibility of CPCs. Compared to acrylic PMMA cements, CPCs have a lower stiffness, less compressive strength and require significantly longer duration for complete curing to occur.18,29 All of these factors have resulted in a limited amount of use of CPCs in vertebral augmentation.
Two widely utilized CPC cements in vertebroplasties and other orthopedic surgeries are Biopex (Mitsubishi) and ChronOS Inject (Synthes) (Table 4). Biopex and ChronOS are both osteoconductive and non-exothermic, and therefore more anatomically suitable.24,30 ChronOs Inject has a relatively low compressive strength of 3 MPa in comparison to Biopex, which has a compressive strength of 80 MPa.
Pedicle Screw Construct
In addition to treating VCFs strictly with injectable bone cement, pedicle screw instrumentation is a common technique used in tandem with vertebroplasty in which the pedicle screw is reinforced through the cement to increase stability of the spine.31 Studies show that minimally invasive pedicle screw fixation (MIPS) combined with PVP is a safe and feasible procedure.31 Risks involved with MIPS can involve nerve injuries as well as fractures in the upper and middle thoracic regions of the spine.31–33 Data suggest that the rate of cement leakage during pedicle screw assisted VP is similar to procedures without screw augmentation.31 Currently, more and better quality data is needed to provide a recommendation for or against the routine use of pedicle screws.30–32,34
Factors Impacting the Intraoperative Effectiveness of Acrylic Bone Cements and Calcium Phosphate Cements
Interventionalists and surgeons should be aware of how the factors that influence the bone cement curing process will affect the cement’s intraoperative performance. Both self-curing ABCs and CPCs are heat sensitive. Any increase or decrease in temperature (either ambient, mixing equipment associated, or produced by the cement components) that deviates from the recommended temperature of 73 °F (23 °C) affects the handling characteristics and setting time of the cement. Variations in humidity affect also handling characteristics and setting time. It is recommended that the unopened cement components are stored at 73 °F (23 °C) for a minimum of 24 h before use.35–37
This sensitivity to ambient temperature greatly impacts the injection-to-set time of the bone cement during procedures. If the ambient environment is too warm during injection, it will cause premature curing of the bone cement. Colder injection environments will slow the cure rate, allowing for a longer injection period at the risk of lower cement viscosity. Refrigeration of bone cement prior to use has been used as a technique to counteract the variability of intraoperative setting time. Despite this utility, pre-chilling of bone cement prior to mixing has been shown to increase the maximum temperature for some cement formulations.38,39
Alterations of temperature in other stages of the cement preparation process, such as the mixing phase, can also affect injection-to-set time. When the acrylic cements were prepared in any vacuum mixing system there was evidence of an increase in the cure temperature. The main factor that contributed to this rise in temperature was an imbalance in the polymer powder to liquid monomer ratio.37,40,41
The variability of the intraoperative environment and bone cement curing process emphasized a need for innovations that minimize the heterogeneity of these factors on the injection-to-set time.
Innovative, Next Generation Bone Cement Formulations
The development of novel bone cement formulations and modifications to commercially available bone cements is imperative to keep improving the effectiveness of VCF treatment and to potentially mitigate some procedural complications. The most common procedural adverse event is cement leakage, which is very common and rarely symptomatic. However, rare instances leading to spinal cord or nerve compression and systemic embolization to the lungs have been reported.42 New formulations that have increased viscosity, a compressive modulus closer to normal bone and a predictable curing process could lead to fewer adverse and serious adverse events (Table 6).
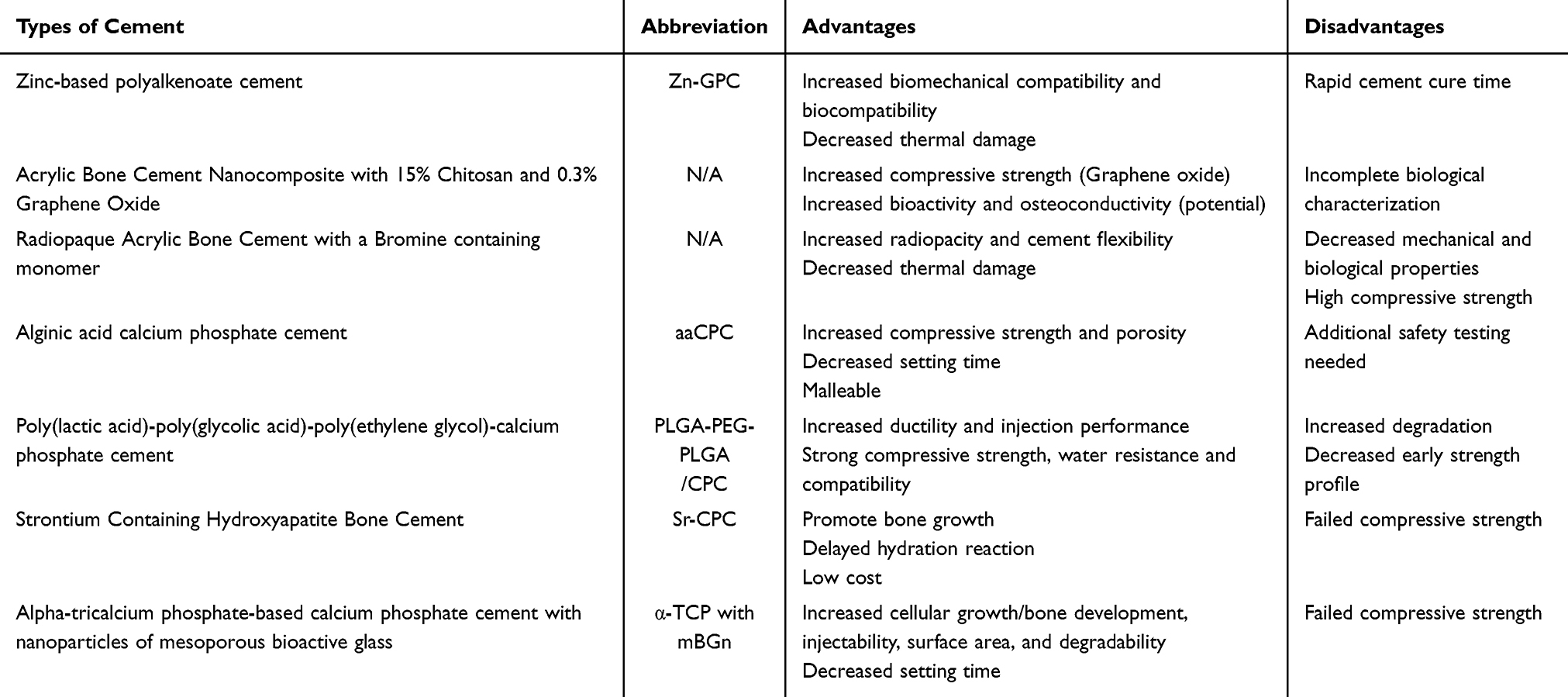 |
Table 6 Next-Generation Formulations of Bone Cement |
Zinc-Based Polyalkenoate Cement
Aluminum-free, zinc-based polyalkenoate cement (Zn-GPC) is considered to be suitable for vertebroplasty and other spinal applications.43,44 Zn-GPC reaches a peak temperature of 33°C thereby decreasing the likelihood of thermal damage to surrounding bone and neural tissue. Zn-GPC’s mechanical properties closely match that of trabecular bone, potentially increasing the biomechanical compatibility with the surrounding osseous tissue.45–47 In addition, Zn-GPC also has favorable biocompatibility.48,49 These data suggest that Zn-GPCs may have the potential to bond directly to living bone tissue after implantation, further improving fracture healing and the stability of the vertebral body.49 In spite of its positive attributes, Zn-GPC is a self-curing free-radical polymerization system and once the components of the experimental Zn-GPC composite are mixed, they have a working set time of 55 seconds.49 This very rapid rate of cement curing is too fast to be clinically applicable. The addition of trisodium citrate to the formulation of Zn-GPCs may improve the working and setting time without affecting its structural integrity, but this possibility is being studied and has yet to be determined.49
Acrylic Bone Cement Nanocomposite with 15% Chitosan and 0.3% Graphene Oxide
Both chitosan and graphene oxide are optimal materials as they possess antibacterial properties and are biocompatible. However, at the time of this writing, biological characterization has not been tested in simulated body fluid. For VCF treatment, the addition of graphene oxide is integral to the chitosan and ABC formula as it increases the compressive strength to above the ISO standard 5833’s minimum compressive strength.50–52 This formula solves some of the major disadvantages associated with ABCs, namely, low bioactivity and osteoconductivity. Further investigation is needed to characterize the influence of this composite on cement curing and setting time.3,52
Radiopaque Acrylic Bone Cement with a Bromine Containing Monomer
ABCs are typically combined with inorganic compounds that allow the cement to be seen radiographically. Inorganic compounds that are utilized to achieve radiopacity are also known to deteriorate the mechanical and biological properties of cement. A bromine-containing monomer has been evaluated as an alternative agent to increase the radiopacity of cement. A novel bromine containing ABC was proposed by Chen et al.53 The modified bone cement significantly enhanced antibacterial function while having a comparable flexural strength to and 3–14% higher flexural modulus than commercial PMMA bone cement.53 Further studies are necessary to elucidate the cement’s interactions with surrounding tissue, exothermic release potentials, impact on radiopacity, fatigue response, and cytotoxicity.53,54
Alginic Acid Calcium Phosphate Cement
A recent study carried out by Shimatani et al investigated the properties of CPCs when mixed with a low viscosity alginic acid. Following the addition of the alginic acid, the setting time decreased from 56 min to 11.5 min. The compressive strength of the mixed cement was 6.4 times higher than that of the control and increased from an average of 7.3 to 46.7 MPa. In animal models, bone replacement was observed as early as 6 weeks with the alginic acid CPC (aaCPC). Scanning electron microscope images confirmed that the aaCPC had higher porosity, theoretically enhancing bone resorption. The aaCPC was observed to be more malleable than the unmodified CPC. Interestingly, the study also reported that a moist environment filled with aaCPC tends to form 3D scaffolds with a complex space suitable for tissue cells to adhere and spread.55 It remains unclear if the cement formulation is safe enough to be used in humans.55 Moreover, studies investigating intraoperative cement control are needed to further validate the formulations’ performance compared to other materials.
Poly(Lactic Acid)-Poly(Glycolic Acid)-Poly(Ethylene Glycol)-Calcium Phosphate Cement
In an attempt to alleviate the previously mentioned disadvantages of CPCs (low compressive strength, poor anti-collapse properties, and poor injection performance), Guo et al synthesized a new biodegradable composite BC system: poly(lactic acid)-poly(glycolic acid)-poly(ethylene glycol)-calcium phosphate cement (PLGA-PEG-PLGA/CPC). This filling material is easily diluted by blood in the cancellous bone and has strong compressive strength, high ductility, good injection performance, and strong water resistance. The new compound had favorable cell compatibility and promoted bone formation. Notably, the degradation rate was faster than typical CPCs with the degradation of the experimental cement being 55% higher than the CPC control.56 One major and consistent drawback of PLGA-PEG-PLGA/CPC was that its early strength profile remained inferior to PMMA, a limitation observed for all CPCs. Their study provides initial insight into the potential capabilities of PLGA-PEG-PLGA/CPC but requires further validation in a large animal or human study.56
Strontium Containing Hydroxyapatite Bone Cement
In a study by Sun et al, a novel Sr-CPC was created using a binary TTCP/Sr-α-TCP combination that created a bone cement with a faster setting time and delayed hydration reaction. This novel system was found to promote new bone growth and have no negative effects on cellular growth. The system is advantageous in that it makes CPCs more clinically usable due to a faster setting time and low cost. Again noted with this novel Sr-CPC was that it failed to develop an adequate compressive strength for bone repair treatments and required further modification in order to be made suitable for VCF treatment.57
Alpha-Tricalcium Phosphate-Based Calcium Phosphate Cement with Nanoparticles of Mesoporous Bioactive Glass (mBGn)
A novel CPC formulated by Ahmed El-Fiqi et al is an α-TCP cement with the incorporation of bioactive nano-component, mesoporous bioactive glass (mBGn). The major advantages of mBGn addition include a high mesoporosity, which makes it an excellent protein/drug delivery system and the release of Si ions that stimulate cellular growth and bone development.58,59 This novel formulation improved the injectability of CPCs, which is a major advantage compared to most CPCs and helps to decrease intraoperative complications associated with cement extravasation. In comparison to other CPCs, this formula had a decreased setting time, higher surface area, and enhanced degradability. Although compressive strength increased as a result of mBGn concentration, the reported values were significantly lower than standards outlined in ISO5833:2002, thereby rendering the cement impractical for clinical use. Further improvements to properties such as porosity and compressive strength are imperative to improve the formula to the point where it could be used in the treatment of VCFs.59 Future evaluation could explore variations in the mGBN concentration to ascertain its effects on the properties of the bone cement.
Conclusions and Perspectives
There are over 25,000 vertebral augmentation procedures performed annually in the US, and the cost of VCF management and treatment is upwards of $13 billion with the total economic burden predicted to increase as the aging population rises. The CPCs and ABCs currently available are effective but can be further optimized for VCF treatment as they have certain limitations that can make them difficult to use intra-operatively and can be modified to reduce potential complications. It is imperative to explore next-generation formulations that enhance the cement–bone interface, decrease the injection-to-set time, limit the impact of extrinsic factors, and provide biomimetic properties. Additional testing of next-generation formulations is necessary to determine clinical applicability and safety. Additionally, given that the typical individual suffering from an osteoporotic VCF is an elderly patient with multiple comorbidities, it is crucial to limit the surgical time and the complications that may come from the vertebral augmentation treatment. Improving the effectiveness of these procedures with new bone cement formulations would ultimately provide patients with a safe, durable, and cost-effective treatment.
Disclosure
Dr Douglas Beall reports grants from Medtronic, Medical Metrics, Avanos, Relievant, Boston Scientific, Stryker, Sollis Pharmaceuticals, Simplify Medical, Lenoss Medical, Spine BioPharma, Eliem Therapeutics, Smart Soft, Tissue Tech, Vivex, Stratus Medical, Restorative Therapies, Kolon TissueGene, Companion Spine, DiscGenics, SI Bone, and Choice Spine, during the conduct of the study. Dr Reade De Leacy reports personal fees from Stryker IVS, grants from Hyprevention, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Kushchayev SV, Wiener PC, Teytelboym OM, Arrington JA, Khan M, Preul MC. Percutaneous vertebroplasty: a history of procedure, technology, culture, specialty, and economics. Neuroimaging Clin N Am. 2019;29(4):481–494. doi:10.1016/j.nic.2019.07.011
2. Beall DP, Phillips TR. Vertebral augmentation: an overview. Skeletal Radiol. 2022;52(10):1911–1920. doi:10.1007/s00256-022-04092-8
3. Robu A, Ciocoiu R, Antoniac A, et al. Bone cements used for hip prosthesis fixation: the influence of the handling procedures on functional properties observed during in vitro study. Materials. 2022;15(9):2967. doi:10.3390/ma15092967
4. Jang J-H, Shin S, Kim H-J, et al. Improvement of physical properties of calcium phosphate cement by elastin-like polypeptide supplementation. Sci Rep. 2018;8(1):5216. doi:10.1038/s41598-018-23577-y
5. Yousefi AM. A review of calcium phosphate cements and acrylic bone cements as injectable materials for bone repair and implant fixation. J Appl Biomater Funct Mater. 2019;17(4):2280800019872594. doi:10.1177/2280800019872594
6. Zapata MEV, Tovar CDG, Hernandez JHM. The role of chitosan and graphene oxide in bioactive and antibacterial properties of acrylic bone cements. Biomolecules. 2020;10(12). doi:10.3390/biom10121616
7. Lewis G. Properties of acrylic bone cement: state of the art review. J Biomed Mater Res. 1997;38(2):155–182. doi:10.1002/(SICI)1097-4636(199722)38:2<155::AID-JBM10>3.0.CO;2-C
8. Pahlevanzadeh F, Bakhsheshi-Rad HR, Hamzah E. In-vitro biocompatibility, bioactivity, and mechanical strength of PMMA-PCL polymer containing fluorapatite and graphene oxide bone cements. J Mech Behav Biomed Mater. 2018;82:257–267. doi:10.1016/j.jmbbm.2018.03.016
9. Meng D, Dong L, Yuan Y, Jiang Q. In vitro and in vivo analysis of the biocompatibility of two novel and injectable calcium phosphate cements. Regen Biomater. 2019;6(1):13–19. doi:10.1093/rb/rby027
10. Raut HK, Das R, Liu Z, Liu X, Ramakrishna S. Biocompatibility of biomaterials for tissue regeneration or replacement. Biotechnol J. 2020;15(12):e2000160. doi:10.1002/biot.202000160
11. Soleymani Eil Bakhtiari S, Bakhsheshi-Rad HR, Karbasi S, et al. Poly(methyl methacrylate) bone cement, its rise, growth, downfall and future. Polym Int. 2021;70(9):1182–1201. doi:10.1002/pi.6136
12. Kumar A, Ghosh R. Fracture toughness of acrylic PMMA bone cement: a mini-review. Indian J Orthop. 2021;55(5):1208–1214. doi:10.1007/s43465-021-00495-2
13. Chen XS, Jiang JM, Sun PD, Zhang ZF, Ren HL. How the clinical dosage of bone cement biomechanically affects adjacent vertebrae. J Orthop Surg Res. 2020;15(1):370. doi:10.1186/s13018-020-01906-0
14. Aebi M, Maas C, Di Pauli von Treuheim T, Friedrich H, Wilke HJ. Comparative biomechanical study of a new transpedicular vertebral device and vertebroplasty for the treatment or prevention of vertebral compression fractures. Clin Biomech. 2018;56:40–45. doi:10.1016/j.clinbiomech.2018.05.001
15. Liao JC, Chen MJW, Lin TY, Chen WP. Biomechanical comparison of vertebroplasty, kyphoplasty, vertebrae stent for osteoporotic vertebral compression fractures—a finite element analysis. NATO Adv Sci Inst Ser E Appl Sci. 2021;11(13):5764.
16. PALACOS Bone Cement; 2023. Available from: https://www.heraeus.com/us/hme/usa_products_heraeus_medical/us_palacos_bone_cements/palacos_plain_bone_cement/palacos_bone_cement_plain.html.
17. Ziegler T, Jaeger R. Fracture toughness and crack resistance curves of acrylic bone cements. J Biomed Mater Res B Appl Biomater. 2020;108(5):1961–1971. doi:10.1002/jbm.b.34537
18. Stoops K, Brown JM, Santoni B, Groundland J. Thermal properties of polymethyl methacrylate vary depending on brand and type. J Orthop Res. 2023;41(3):614–618. doi:10.1002/jor.25389
19. WestCMR; 2023. Available from: https://www.westcmr.com/.
20. Quan Q, Gongping X, Ruisi N, Shiwen L. New research progress of modified bone cement applied to vertebroplasty. World Neurosurg. 2023;176:10–18. doi:10.1016/j.wneu.2023.04.048
21. Schützenberger S, Schwarz SM, Greiner L, et al. Is vertebral body stenting in combination with CaP cement superior to kyphoplasty? Eur Spine J. 2018;27(10):2602–2608. doi:10.1007/s00586-018-5717-7
22. Lu Q, Liu C, Wang D, Liu H, Yang H, Yang L. Biomechanical evaluation of calcium phosphate-based nanocomposite versus polymethylmethacrylate cement for percutaneous kyphoplasty. Spine J. 2019;19(11):1871–1884. doi:10.1016/j.spinee.2019.06.007
23. Priyadarshi S, Singhal V, Gupta S. Percutaneous transpedicular vertebroplasty using calcium phosphate cement for osteoporotic vertebral fractures: a Prospective Study of Functional Outcomes. J Orthop Dis Traumatol. 2023;6(2):157. doi:10.4103/jodp.jodp_99_22
24. Schröter L, Kaiser F, Stein S, Gbureck U, Ignatius A. Biological and mechanical performance and degradation characteristics of calcium phosphate cements in large animals and humans. Acta Biomater. 2020;117:1–20. doi:10.1016/j.actbio.2020.09.031
25. Purcell P, Tyndyk M, McEvoy F, Tiernan S, Sweeney D, Morris S. A multiscale finite element analysis of balloon kyphoplasty to investigate the risk of bone-cement separation in vivo. Int J Spine Surg. 2021;15(2):302–314. doi:10.14444/8040
26. Lu J, Yu H, Chen C. Biological properties of calcium phosphate biomaterials for bone repair: a review. RSC Adv. 2018;8(4):2015–2033. doi:10.1039/C7RA11278E
27. Jeong J, Kim JH, Shim JH, Hwang NS, Heo CY. Bioactive calcium phosphate materials and applications in bone regeneration. Biomater Res. 2019;23:4. doi:10.1186/s40824-018-0149-3
28. Lodoso-Torrecilla I, van den Beucken JJJP, Jansen JA. Calcium phosphate cements: optimization toward biodegradability. Acta Biomater. 2021;119:1–12. doi:10.1016/j.actbio.2020.10.013
29. Dorozhkin SV. Synthetic amorphous calcium phosphates (ACPs): preparation, structure, properties, and biomedical applications. Biomater Sci. 2021;9(23):7748–7798. doi:10.1039/d1bm01239h
30. Brueckner T, Heilig P, Jordan MC, et al. Biomechanical evaluation of promising different bone substitutes in a clinically relevant test set-up. Materials. 2019;12(9):1364. doi:10.3390/ma12091364
31. Xu HH, Wang P, Wang L, et al. Calcium phosphate cements for bone engineering and their biological properties. Bone Res. 2017;5(1):17056. doi:10.1038/boneres.2017.56
32. Demir-Oğuz Ö, Boccaccini AR, Loca D. Injectable bone cements: what benefits the combination of calcium phosphates and bioactive glasses could bring? Bioact Mater. 2023;19:217–236. doi:10.1016/j.bioactmat.2022.04.007
33. Rustom LE, Poellmann MJ, Wagoner Johnson AJ. Mineralization in micropores of calcium phosphate scaffolds. Acta Biomater. 2019;83:435–455. doi:10.1016/j.actbio.2018.11.003
34. Peng Y, Du X, Huang L, et al. Optimizing bone cement stiffness for vertebroplasty through biomechanical effects analysis based on patient-specific three-dimensional finite element modeling. Med Biol Eng Comput. 2018;56(11):2137–2150. doi:10.1007/s11517-018-1844-x
35. Boucas P, Mamdouhi T, Rizzo SE, Megas A. Cement augmentation of pedicle screw instrumentation: a literature review. Asian Spine J. 2023;17(5):939–948. doi:10.31616/asj.2022.0216
36. Pusceddu C, Marsico S, Derudas D, et al. Percutaneous CT-guided Microwave Ablation Combined with Pedicle Screw Fixation Followed by Vertebroplasty (MASFVA): initial experience of a minimally invasive treatment of vertebral metastases with extension to the vertebral pedicle. Curr Oncol. 2023;30(2):1663–1672. doi:10.3390/curroncol30020127
37. Li Z, Wang Y, Xu Y, Xu W, Zhu X, Chen C. Efficacy analysis of percutaneous pedicle screw fixation combined with percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fractures with kyphosis. J Orthop Surg Res. 2020;15(1):53. doi:10.1186/s13018-020-1583-1
38. Lou C, Yu W, Chen Z, Gao J, Liu F, He D. Short-term outcomes of percutaneous pedicle screw fixation combined with vertebroplasty: a minimally invasive treatment for Kümmell’s disease with intravertebral instability. Acta Orthop Traumatol Turc. 2020;54(6):627–633. doi:10.5152/j.aott.2020.19245
39. Wen Z, Mo X, Zhao S, et al. Comparison of percutaneous kyphoplasty and pedicle screw fixation for treatment of thoracolumbar severe osteoporotic vertebral compression fracture with kyphosis. World Neurosurg. 2021;152:e589–e596. doi:10.1016/j.wneu.2021.06.030
40. Artilia I, Zakaria MN, Cahyanto A. Setting time, handling property and mechanical strength evaluation of SCPC50 and apatite cement mixture in various combinations. In: Asian BioCeramics. Trans Tech Publications Ltd; 2020:40–45.
41. Fathi M, Kholtei A, EL Youbi S, Chafik El Idrissi B. Setting properties of calcium phosphate bone cement. Mater Today; 2019;13:876–881.
42. Gelli R, Mati L, Ridi F, Baglioni P. Tuning the properties of magnesium phosphate-based bone cements: effect of powder to liquid ratio and aqueous solution concentration. Mater Sci Eng C Mater Biol Appl. 2019;95:248–255. doi:10.1016/j.msec.2018.10.083
43. Cyphert EL, Learn GD, Marques DW, Lu CY, von Recum HA. Antibiotic refilling, antimicrobial activity, and mechanical strength of PMMA bone cement composites critically depend on the processing technique. ACS Biomater Sci Eng. 2020;6(7):4024–4035. doi:10.1021/acsbiomaterials.0c00305
44. Elliott R, Regazzola G, Bruce WJM. Ambient theatre temperature and cement setting time in total knee arthroplasty. ANZ J Surg. 2019;89(11):1424–1427. doi:10.1111/ans.15463
45. Li C, Hao W, Wu C, et al. Injectable and bioactive bone cement with moderate setting time and temperature using borosilicate bio-glass-incorporated magnesium phosphate. Biomed Mater. 2020;15(4):045015. doi:10.1088/1748-605X/ab633f
46. Kubota M, Yokoi T, Ogawa T, et al. In-vitro heat-generating and apatite-forming abilities of PMMA bone cement containing TiO2 and Fe3O4. Ceram Int. 2021;47(9):12292–12299. doi:10.1016/j.ceramint.2021.01.080
47. Zhang K, She J, Zhu Y, Wang W, Li E, Ma D. Risk factors of postoperative bone cement leakage on osteoporotic vertebral compression fracture: a retrospective study. J Orthop Surg Res. 2021;16(1):183. doi:10.1186/s13018-021-02337-1
48. Wen X, Wang J, Pei X, Zhang X. Zinc-based biomaterials for bone repair and regeneration: mechanism and applications. J Mater Chem B Mater Biol Med. 2023;11(48):11405–11425. doi:10.1039/D3TB01874A
49. Toledano M, Osorio R, Vallecillo-Rivas M, et al. Zn-doping of silicate and hydroxyapatite-based cements: dentin mechanobiology and bioactivity. J Mech Behav Biomed Mater. 2021;114:104232. doi:10.1016/j.jmbbm.2020.104232
50. Khader BA, Rodriguez O, Towler MR. The effect of Mg2+ incorporation into the glass phase of zinc-based glass polyalkenoate cements. J Non-Cryst Solids. 2018;483:106–117. doi:10.1016/j.jnoncrysol.2018.01.007
51. Mokhtari S, Krull EA, Sanders LM, et al. Investigating the effect of germanium on the structure of SiO2-ZnO-CaO-SrO-P2O5 glasses and the subsequent influence on glass polyalkenoate cement formation, solubility and bioactivity. Mater Sci Eng C Mater Biol Appl. 2019;103:109843. doi:10.1016/j.msec.2019.109843
52. Moheet IA, Luddin N, Rahman IA, Kannan TP, Abd Ghani NR N, Masudi SM. Modifications of glass ionomer cement powder by addition of recently fabricated nano-fillers and their effect on the properties: a review. Eur J Dent. 2019;13(3):470–477. doi:10.1055/s-0039-1693524
53. Marx D, Phull S, Papini M, Towler M. Tissue response to a novel bone adhesive implanted subcutaneously in rats: a histological and gene expression analysis. Nano Sel. 2023;4(6):408–418. doi:10.1002/nano.202300015
54. Kargozar S, Montazerian M, Fiume E, Baino F. Multiple and promising applications of Strontium (Sr)-containing bioactive glasses in bone tissue engineering. Front Bioeng Biotechnol. 2019;7:161. doi:10.3389/fbioe.2019.00161
55. Tan QC, Jiang XS, Chen L, et al. Bioactive graphene oxide-functionalized self-expandable hydrophilic and osteogenic nanocomposite for orthopaedic applications. Mater Today Bio. 2023;18:100500. doi:10.1016/j.mtbio.2022.100500
56. Zapata MEV, Ruiz Rojas LM, Mina Hernández JH, Delgado-Ospina J, Tovar CDG. Acrylic bone cements modified with graphene oxide: mechanical, physical, and antibacterial properties. Polymers. 2020;12(8):. doi:10.3390/polym12081773
57. Valencia Zapata ME, Mina Hernandez JH, Grande Tovar CD, et al. Novel bioactive and antibacterial acrylic bone cement nanocomposites modified with graphene oxide and chitosan. Int J Mol Sci. 2019;20(12):2938. doi:10.3390/ijms20122938
58. Chen Y, Caneli G, Almousa R, Xie D. A novel antibacterial zirconia-containing PMMA bone cement. J Mech Behav Biomed Mater. 2022;129:105135. doi:10.1016/j.jmbbm.2022.105135
59. Tang C, Dang Z, Lu T, Ye J. A novel anti-washout curing solution of calcium phosphate cement prepared via irradiation polymerization. J Mater Chem B Mater Biol Med. 2023;11(31):7410–7423. doi:10.1039/D3TB00544E
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.