")
Back to Journals » Clinical Interventions in Aging » Volume 19
Bridging Reduced Grip Strength and Altered Executive Function: Specific Brain White Matter Structural Changes in Patients with Alzheimer’s Disease
Authors Liu SW, Ma XT, Yu S , Weng XF, Li M, Zhu J, Liu CF , Hu H
Received 2 October 2023
Accepted for publication 9 January 2024
Published 16 January 2024 Volume 2024:19 Pages 93—107
DOI https://doi.org/10.2147/CIA.S438782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Shan-Wen Liu,1 Xiao-Ting Ma,1 Shuai Yu,2 Xiao-Fen Weng,3 Meng Li,4 Jiangtao Zhu,4 Chun-Feng Liu,1 Hua Hu1
1Department of Neurology, the Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China; 2Department of Neurology, the Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, 215000, People’s Republic of China; 3Department of Geriatric Medicine, the Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, 215000, People’s Republic of China; 4Department of Imaging, the Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China
Correspondence: Hua Hu, Department of Neurology, the Second Affiliated Hospital of Soochow University, 1055 San Xiang Road, Suzhou, Jiangsu Province, 215004, People’s Republic of China, Email [email protected]
Objective: To investigate the correlation between specific fiber tracts and grip strength and cognitive function in patients with Alzheimer’s disease (AD) by fixel-based analysis (FBA).
Methods: AD patients were divided into AD with low grip strength (AD-LGS, n=29) and AD without low grip strength (AD-nLGS, n=25), along with 31 normal controls (NC). General data, neuropsychological tests, grip strength and cranial magnetic resonance imaging (MRI) scans were collected. FBA evaluated white matter (WM) fiber metrics, including fiber density (FD), fiber cross-sectional (FC), and fiber density and cross-sectional area (FDC). The mean fiber indicators of the fiber tracts of interest (TOI) were extracted in cerebral region of significant statistical differences in FBA to further compare the differences between groups and analyze the correlation between fiber properties and neuropsychological test scores.
Results: Compared to AD-nLGS group, AD-LGS group showed significant reductions in FDC in several cerebral regions. In AD patients, FDC values of bilateral uncinate fasciculus and left superior longitudinal fasciculus were positively correlated with Clock Drawing Test scores, while FDC of splenium of corpus callosum, bilateral anterior cingulate tracts, forceps major, and bilateral inferior longitudinal fasciculus were positively correlated with the Executive Factor Score of Memory and Executive Screening scale scores.
Conclusion: Reduced grip strength in AD patients is associated with extensive impairment of WM structural integrity. Changes in FDC of specific WM fiber tracts related to executive function play a significant mediating role in the reduction of grip strength in AD patients.
Keywords: Alzheimer disease, grip strength, white matter, fixel-based analysis, cognition function
Alzheimer’s disease (AD) is the most prevalent type of dementia worldwide, characterized by the progressive cognitive decline as the main clinical symptoms of neurodegenerative disease. Although pharmacological treatment options for AD remain limited, early intervention targeting modifiable risk factors could prevent or delay up to 40–50% of dementia cases.1 Given the long period preceding the onset of AD pathology and early symptoms, identifying and intervening with modifiable risk factors becomes crucial.
Recently, studies have demonstrated that reduced grip strength is a risk factor of early cognitive dysfunction and dementia in older adults.2 Stronger grip strength is correlated with better cognitive processing speed, memory, executive function, as well as less cortical atrophy in brain regions closely related to these cognitive processes, such as the hippocampus, temporal lobe, ventral striatum and thalamus.3 From a neuroimaging perspective, in addition to cortical atrophy, which is a distinctive feature of AD, structural or functional abnormalities in the white matter (WM) fiber tracts, which serve as important network pathways connecting various cerebral regions, are also closely associated with the risk and progression of AD.4 Persistent damage to brain WM fiber pathways not only disrupts functional brain network connectivity and information dissemination but also accelerates abnormal changes in oxidative stress, excitotoxicity, and pathological protein deposition.5 Previous research utilizing animal models for AD suggested that some degree of axonal and myelin damage existed prior to β-amyloid protein (Aβ) deposition and neurofibrillary tangle formation in cortex,6 accentuating that structural changes in the WM may occur before or even at an earlier stage of cognitive decline, which deserves attention and emphasis.7 A cohort study of 190,406 adult patients discovered that each 5kg decrease in grip strength was linked to higher WM hyperintensities (WMH) volume and a greater risk of dementia development in the future,8 suggesting that decreased grip strength and abnormalities in WM structure or function may be one of the early risk markers for the development of AD. To address the question of what role specific structural alterations in WM play in mediating reduced grip strength and altered cognitive function in AD patients is the primary aim of this research.
At present, diffusion-weighted imaging (DWI) based on the diffusion tensor imaging model (DTI) is a popular non-invasive technique for studying the structure of WM fiber tracts. However, the DWI technique has several limitations that can significantly affect a study’s value and reliability, including biased acquisition of data, pre- and post-processing of data, quantitative analysis, and result interpretation.9 Furthermore, its capability in handling complex crossed WM fiber tracts is restricted, and variations in the presence of WM voxels pose challenges in accurately attributing them to specific fiber pathways,10 but WM changes manifest in multiple forms in neurodegenerative diseases, such as fiber atrophy and demyelination. However, a recently proposed diffusion model,11 fixel-based analysis (FBA) can remedy these deficiencies where “fixels” refers to all specific WM fiber tracts within a voxel with different orientations.12 FBA characterizes multiple WM fiber orientations within voxels by analyzing DWI data using constrained spherical inverse fold products,10 detecting structural changes in specific WM fiber tracts. FBA related metrics include fiber density (FD), fiber cross-section (FC) and fiber density and cross-section (FDC).11 FD reflects the microstructure of fiber tracts, FC reflects the macrostructural properties of fiber tracts, and FDC represents the combined impact of these two metrics, reflecting the microscopic and macroscopic variations that co-occur during neurodegeneration.13 A recent study using FBA technology found that patients with early-onset AD exhibited more extensive damage in WM microstructure and poorer cognitive function than patients with late-onset AD, suggesting potential differences in neuropathological mechanisms of WM damage between the two types of AD.14 This highlights the superiority of FBA technique in observing and interpreting structural changes of WM tracts in AD or neurodegenerative diseases.
Applying the latest FBA technique for assessing WM structure, this study attempted to provide a deeper comprehension of how changes in WM fiber tracts influence grip strength and cognitive function in AD patients by examining microscopic and macroscopic alterations in WM structure. We hypothesized that structural changes of some specific WM fiber tracts in AD patients may mediate the reduced grip strength and cognitive function decline through the damage of brain network connections. This provides a theoretical basis for further attention to structural and functional changes in WM, which may help prevent or delay the occurrence and progression of AD.
Materials and Methods
Participants
A total of 54 AD patients diagnosed in the Memory Disorders Clinic of the Department of Neurology of the Second Hospital of Soochow University from January 2021 to December 2022 were recruited after approval by the Ethics Committee of the Second Hospital of Soochow University (JD-LK-2021-049-01), and informed consent was obtained from both the subjects and their caregivers. Additionally, 31 normal controls (NC) with normal cognition and grip strength were included. The inclusion criteria for AD patients include: (1) met the core diagnostic criteria based on the National Institute on Aging and the Alzheimer’s Association (NIA/AA) workgroups in 2011 by the current physician or previously confirmed.15 (2) an age range of 55 to 90 years and right-hand dominance. (3) craniocerebral magnetic resonance imaging (MRI) examination did not show occupying lesions and age-inappropriate periventricular and deep WM lesions.16 (4) Hachinski ischemia score ≤4. (5) no medication with effects on cognitive function and mental status within 1 month prior to enrollment. (6) clinical information was complete and understand the involved scales. The exclusion criteria for AD patients include: (1) other diseases that cause cognitive impairment, such as cerebrovascular disease and brain tumors. (2) serious medical diseases, such as cardiopulmonary, hepatic and renal insufficiency, hypothyroidism, malignancy and other chronic wasting diseases. (3) severe depression, schizophrenia and other psychiatric diseases. (4) those who are unable to perform bioelectrical impedance and MRI examination due to metal placement. (5) those who have motor system disorders or balance dysfunction diseases affecting limb movements, such as lumbar disc herniation, history of fracture, diabetic foot, osteoarthrosis, etc. (6) combined motor system symptoms, such as complaints of subjective fatigue, muscle weakness, muscle atrophy, and signs of cone system and extrapyramidal damage on physical examination. (7) mini nutritional assessment (MNA) score ≤24.17
The inclusion criteria for NC include: (1) an age range of 55 to 90 years and right-hand dominance. (2) Montreal Cognitive Assessment (MoCA) score ≥26 points. (3) normal WM on MRI examination and no central nervous system disease. (4) no medications with effects on cognitive function and mental status within 1 month before enrollment. (5) normal grip strength was ≥28 kg for men and ≥18 kg for women. Exclusion criteria were the same as those for AD patients.
Demographics Data
Gender, age, years of education, hypertension, diabetes, hyperlipidemia, coronary heart disease, history of smoking and alcohol consumption, height, weight were recorded. Body Mass Index (BMI) was calculated as weight (kg)/height (m2). The activity level was assessed based on the amount of weekly walking. Less than 120 minutes of walking per week for females and less than 150 minutes per week for males were considered low physical activity.18 Participants were asked to squeeze the dynamometer (WCS-100, Nantong, China) as hard as possible with each hand. Grip strength was measured for a total of three trials and the maximum value was recorded. The cut-off was defined as <28 kg for men and <18 kg for women.19 Based on whether there was a reduction in grip strength, AD patients were divided into 25 AD patients with low grip strength (AD-LGS) and 29 AD patients without low grip strength (AD-nLGS).
Neuropsychological Assessments
The assessors who had received specialized and consistent training in administering assessment scales conducted neuropsychological tests on the subjects in a quiet room, including evaluations of both cognitive and non-cognitive functions. The cognitive function tests included MoCA, Clock Drawing Test (CDT), Memory and Executive Screening scale (MES), and Digit Symbol Substitution Test (DSST). MoCA assess overall cognitive function. The total score of MES (MES-T) includes the Memory Factor Score (MES-M) to assess situational memory and the Executive Factor Score (MES-E) to assess executive function. The Verbal Fluency Task (VFT) assesses verbal function. Non-cognitive tests include the Activities of Daily Living (ADL) scale, which assesses activities of daily living, and the 17-item Hamilton Depression Scale-17 (HAMD-17), which assesses depression level.
Magnetic Resonance Imaging (MRI) Acquisition and Preprocessing
A total of 65 volumes (DWI 60 gradient direction b=2000s/mm2 and 5 images b=0s/mm2) were acquired by the same 3.0T (Siemens, Germany, Prisma) MRI scanner with the following parameters: repetition time/echo time = 6600/86 ms, 2.2 mm isotropic voxels, phase encoding direction = AP. The DWI acquisition time was 0–9 min. The preprocessing and analysis steps of a state-of-the-art FBA were employed.20 All diffusion MRI data were preprocessed using MRtrix3. The preprocessing steps included denoising, Gibbs ringing correction, correction for eddy current-induced distortions, with subsequent bias field correction applied. Response functions for single-fiber WM as well as gray matter (GM) and cerebrospinal fluid (CSF) were estimated from the data using an unsupervised approach. Next, single-shell 3-tissue constrained spherical deconvolution was employed to obtain WM-like fiber orientation distributions as well as GM and CSF-like compartments across all voxels. The MRtrix3Tissue software (https://3Tissue.github.io), a fork of MRtrix3, was utilized for this step. The obtained WM-like fiber orientation distribution (FOD), GM-like, and CSF-like images were used for multi-tissue informed log-domain intensity normalization. A cubic b-spline interpolation was further employed to upsample the WM fiber orientation distribution images to 1.3 mm isotropic voxels. A study-specific template was subsequently generated using the WM FOD images from 31 NC and all subjects’ FDO images were non-linearly registered to it. Finally, the WM FOD template was utilized to generate a whole-brain probabilistic tractogram that was filtered from 20 million tracts to 2 million tracts to mitigate reconstruction bias.
Fixel-Based Metrics
We employed the FBA framework to calculate FD and FC at the level of a “fixel”,11 which refers to a population of fibers within a voxel. This means that even when multiple fibers are crossing in the same voxel, each fiber still has its own individual measurements of FD and FC. (1) FD, obtained from FOD images because the integration of FOD along a particular direction is proportional to the volume within the axons aligned along that direction. Therefore, FD values are particularly sensitive to changes in the level of microstructure within the voxel. (2) FC, a loss of the axons results in shrinkage of the fiber tract across its cross-section, implying a reduction in the extent of space occupied by that fiber tract, leading to changes in macrostructure.11 Using nonlinear distortion to calculate the spatial normalization of the subject image to the template image, structural differences can be estimated for each FC (in a plane perpendicular to the fixed direction). (3) FDC, the product of the above two metrics and provides information about the combined pathology of microstructural and macrostructural changes, increasing sensitivity to the overall ability of the fiber population to transmit information between connected cerebral regions.
Statistical Analysis
SPSS26.0 software package was used for statistical analysis. Normally distributed continuous variables were presented as means ± standard deviation (SD) and analyzed using Analysis of Variance (ANOVA; F value). Post-hoc tests with Bonferroni corrections for multiple comparisons were conducted when a statistically significant variable was identified in ANOVA. Non-normally distributed continuous variables were reported as medians (interquartile range) and analyzed by the Kruskal–Wallis H-test (H value). Categorical variables were expressed as percentages, and inter-group comparisons were conducted using the χ2 test or Fisher’s exact test (χ2 value). Bonferroni correction was employed to indicate significant group differences. P<0.05 was considered a statistically significant difference.
Whole-Brain Fixel-Based Analysis
To identify regions with altered FD, FC and FDC in the AD-LGS, AD-nLGS and NC groups, we first compared metrics based on whole-brain FBA. A general linear model was used to statistically compare FD, FC, and FDC in the AD-LGS, AD-nLGS, and NC groups. Age and gender were used as covariates to compare differences in fixel levels using the connectivity-based fixel enhancement (CFE). The utilization of smoothing in CFE primarily focuses on applying it along structurally connected fixels. This approach guarantees that fixel-based metrics undergo local smoothing alongside fixels that are part of the same fiber tract. Allocated Family-wise error rate (FWE)-corrected P-values to each fixel using non-parametric permutation testing conducted over 5000 permutations.21
Significant fixels (FWE-corrected P-value<0.05) were visualized using the mrview tool in MRtrix3. To enhance the understanding of the implicated fiber pathways, significant fixels were overlaid on the template-derived tractogram. This approach involved isolating only those fixels that held significance and displaying corresponding streamlines. The visualization utilized color-coded streamlines based on their orientations (anterior-posterior: green, left-right: red, superior-inferior: blue).
Tract of Interest (TOI) Analysis
We performed a further TOI analysis to investigate the potential degeneration of selective fiber pathways in the AD-LGS group. All fixels that demonstrated significant differences in the FDC metric among the three groups upon whole-brain FBA were classified into 21 distinct WM tracts based on JHU brain WM atlas. Mean FDC values for each fiber tract were extracted, including bilateral anterior thalamus radiation (ATR), corticospinal tract (CST), anterior cingulate tract, posterior cingulate tract, uncinate fasciculus (UF), inferior fronto-occipital fasciculus (IFOF), inferior longitudinal fasciculus (ILF), superior longitudinal fasciculus (SLF), genu of corpus callosum (GCC), body of corpus callosum (BCC), splenium of corpus callosum (SCC), forceps major, and forceps minor.
PALM (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/PALM) was used in MATLAB to count the group differences of FDC values in all fiber tracts on the basis of correction for age and gender. Correlation analysis was performed between FDC values of the fiber tracts and neuropsychological scale scores, controlling for age, gender and years of education. The above statistics were calculated by permutation testing to calculate the P-FEW values.
Results
Comparison of General Clinical Characteristics Among the Three Groups
As demonstrated in Table 1, the NC group included 15 males and 16 females, aged (68.45 ± 8.90) years with 11.0 (9.0,16.0) years of education. The AD-nLGS group included 10 males and 19 female patients, aged (67.86 ± 8.63) years with 9.0 (3.0,12.0) years of education. The AD-LGS group included 3 males and 22 female patients, age (76.88 ± 6.79) years with 6.0 (2.0,12.0) years of education. The height, weight, grip strength and MTA scores were statistically significant differences (all P< 0.05). Compared to the NC and AD-nLGS groups, the AD-LGS group had poorer grip strength and higher MTA scores (all P< 0.01).
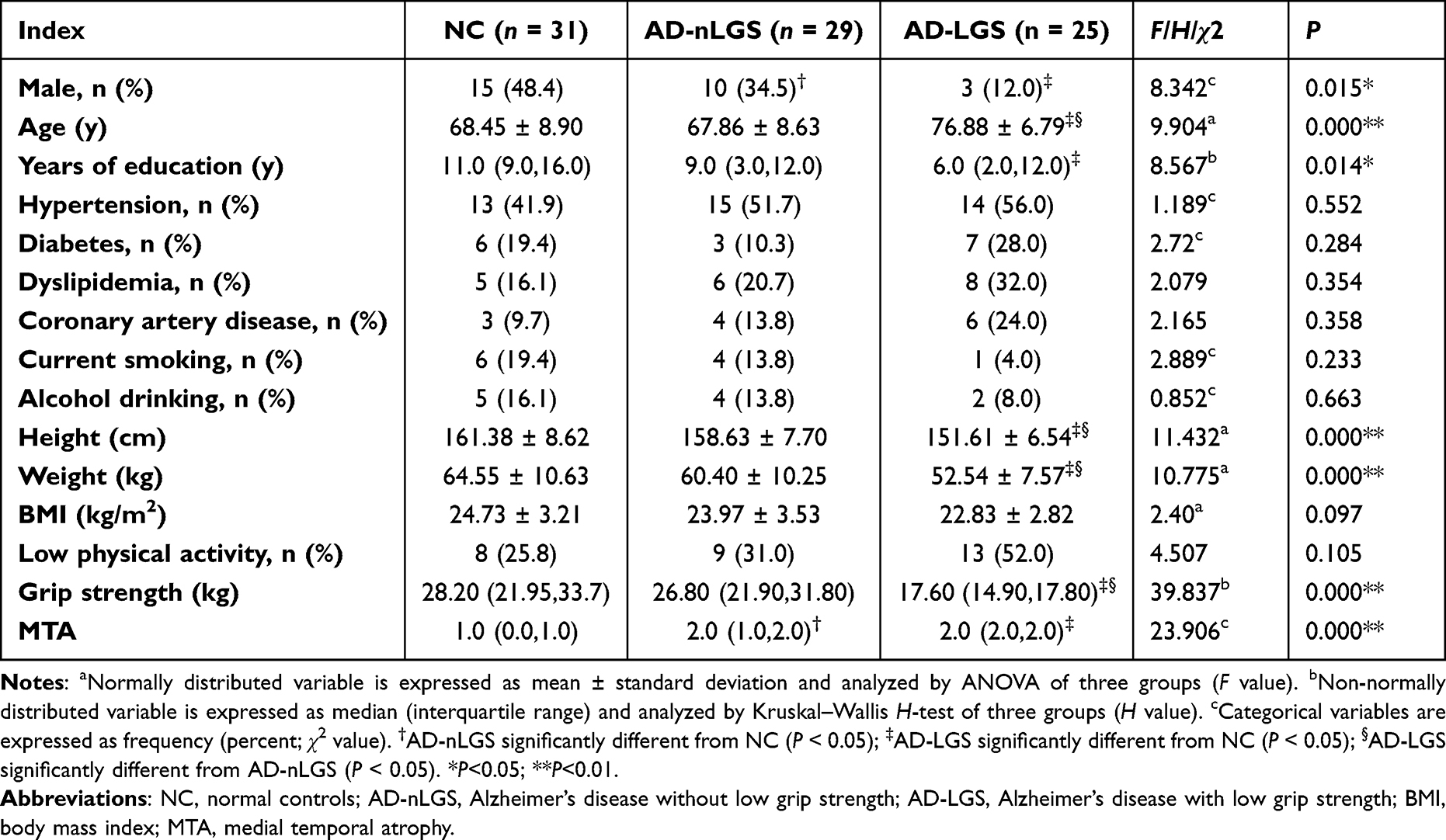 |
Table 1 Comparison of General Clinical Characteristics Among the Three Groups |
Comparison of Neuropsychological Characteristics Among the Three Groups
As demonstrated in Table 2, compared with the NC group, the AD group had lower scores for MoCA, CDT, MES-T, MES-M, MES-E, DSST, FDST, BDST, VFT, and higher scores for ADL and HAMD-17 (all P < 0.05); compared with the AD-nLGS group, the AD-LGS group had lower scores for CDT, MES-E and DSST (P < 0.05).
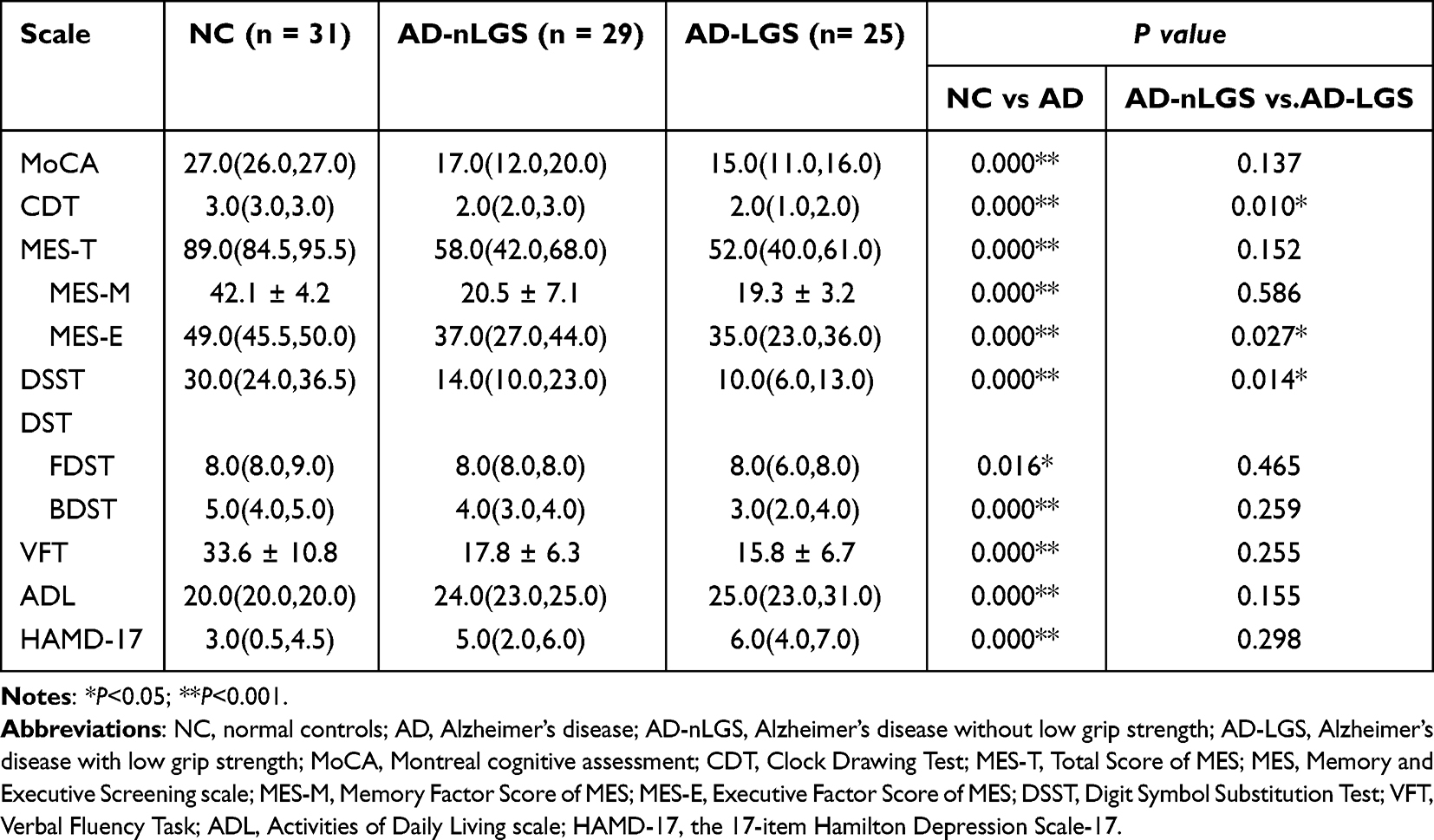 |
Table 2 Comparison of Neuropsychological Characteristics Among the Three Groups |
Comparison of FD, FC and FDC in TOI Among Three Groups
As demonstrated in Figure 1, adjusting for age and gender, streamline segments associated with fixels that had a significant (FWE-corrected P-value < 0.05) decrease between the three groups in FC, FD, and FDC of BCC, GCC, SCC, bilateral ATR, forceps major, forceps minor, bilateral IFOF, bilateral UF, bilateral anterior cingulate tract and bilateral ILF; there were also significant differences among the three groups in FC and FDC of bilateral ILF, bilateral CST and right posterior cingulate tract, and significant differences among the three groups in FDC of the left posterior cingulate tract.
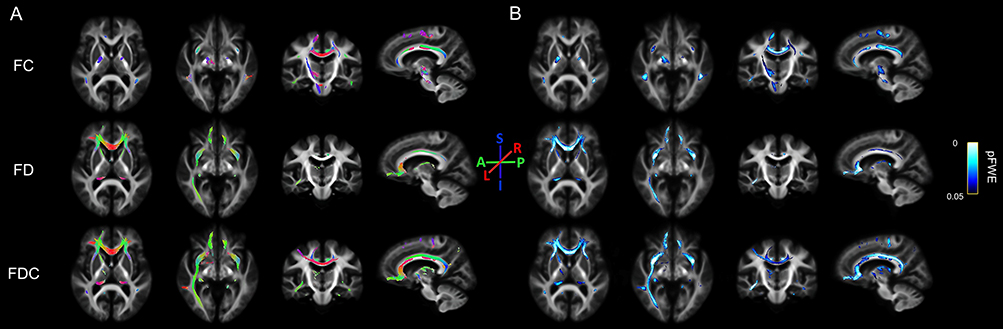 |
Figure 1 Whole-brain FBA results. Fiber tract-specific differences among AD-nLGS, AD-LGS and NC are shown. Streamline segments were cropped from the template tractogram to include only those corresponding to fixels significant at family-wise error-corrected P<0.05. Streamlines were colored by (A) fiber direction (A-P indicates anterior-posterior, green; L-R, left-right, red; and S-I, superior inferior, blue.) and (B) family-wise error-corrected P value for fiber density (FD), fiber cross-section (FC), and combined fiber density and cross-section (FDC). |
Two-by-Two Post Hoc Comparisons of FC, FD, and FDC of the Statistically Different TOI Among the Three Groups
As demonstrated in Figure 2, post hoc test analysis showed that compared to the AD-nLGS group, FDC was significantly lower in the AD-LGS group in CC, SCC, bilateral IFOF, bilateral ILF, bilateral UF, bilateral ATR, right CST, bilateral anterior cingulate tract, left posterior cingulate tract, forceps major and bilateral SLF. FD was significantly lower in CC, SCC, bilateral IFOF, bilateral ILF, bilateral UF, bilateral ATR, bilateral anterior cingulate tract and forceps major. FC was significantly lower in CC, BCC, SCC, bilateral IFOF, bilateral ILF, bilateral UF, left ATR, bilateral anterior cingulate tract and bilateral SLF.
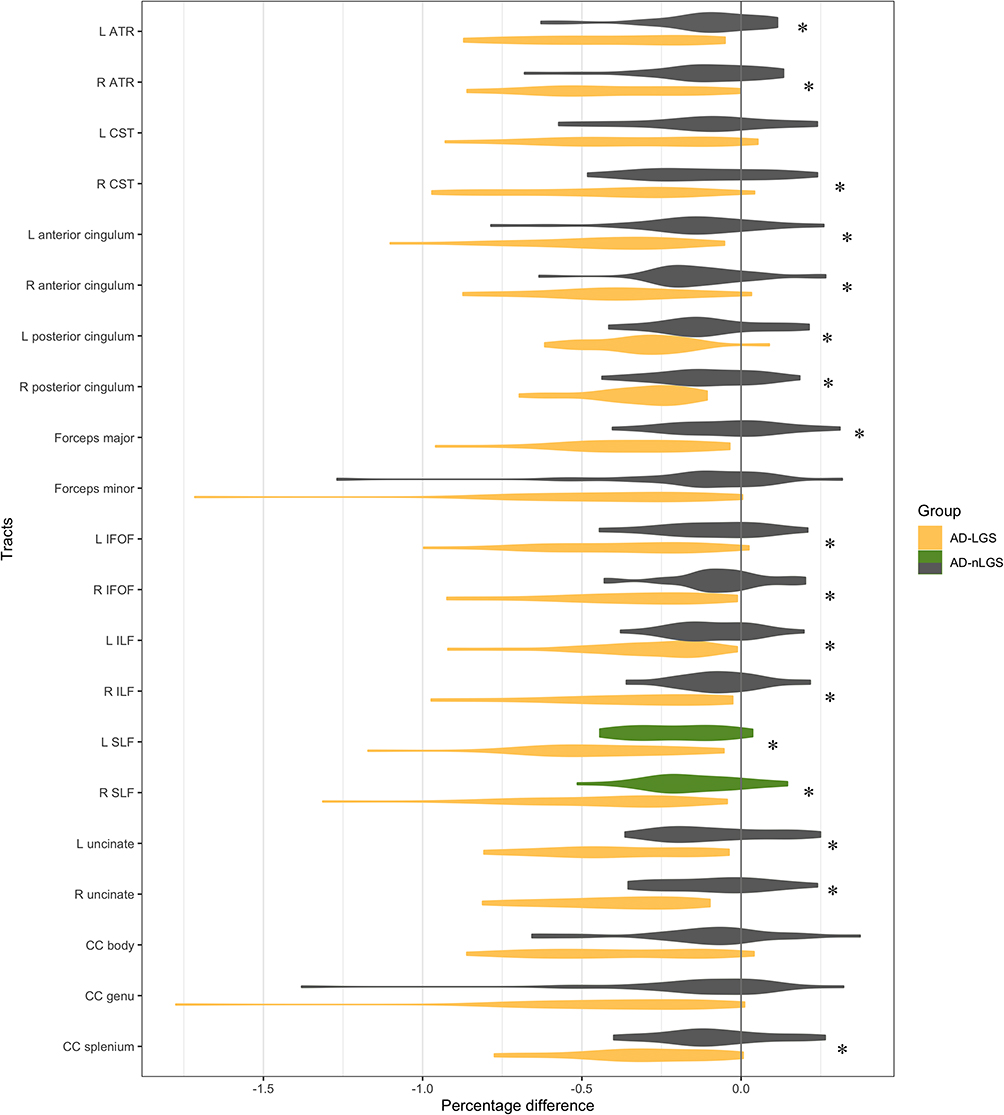 |
Figure 2 Tract-of-interest results. Mean FDC within tracts of interest are displayed for AD-nLGS and AD-LGS, as a percentage difference from the NC mean, adjusted for age and gender. For each AD group vs NC group, significant tracts (P-FWE<0.05) are displayed in color, while non-significant are shown in grey. For AD-nLGS vs AD-LGS, significant tracts are labeled with asterisks (*). Abbreviations: AD-nLGS, AD patients with non-low grip strength; AD-LGS, AD patients with low grip strength; ATR, anterior thalamus radiation; CST, corticospinal tract; IFOF, inferior fronto-occipital fasciculus; ILF, inferior longitudinal fasciculus; SLF, superior longitudinal fasciculus; CC, corpus callosum; L, left; R, right. |
Correlation Between FDC and CDT, DSST, and MES-E Scores of Cerebral TOI with Statistically Differences Between Groups
As demonstrated in Table 3 and Figure 3, correlation analysis showed that after controlling for age, gender, and years of education, the FDC values of AD patients in the left UF (r=0.39, P-FWE=0.016), right UF (r=0.36, P-FWE=0.034), and left SLF (r=0.36, P-FWE=0.033) were positively correlated with CDT scores; the FDC values in the SCC (r= 0.40, P-FWE=0.016), left anterior cingulate tract (r=0.35, P-FWE=0.046), right anterior cingulate tract (r=0.41, P-FWE=0.01), forceps major (r=0.47, P-FWE=0.002), left SLF (r=0.41, P-FWE=0.01), right SLF (r=0.37, P-FWE= 0.03) were positively correlated with MES-E scores (all P<0.05).
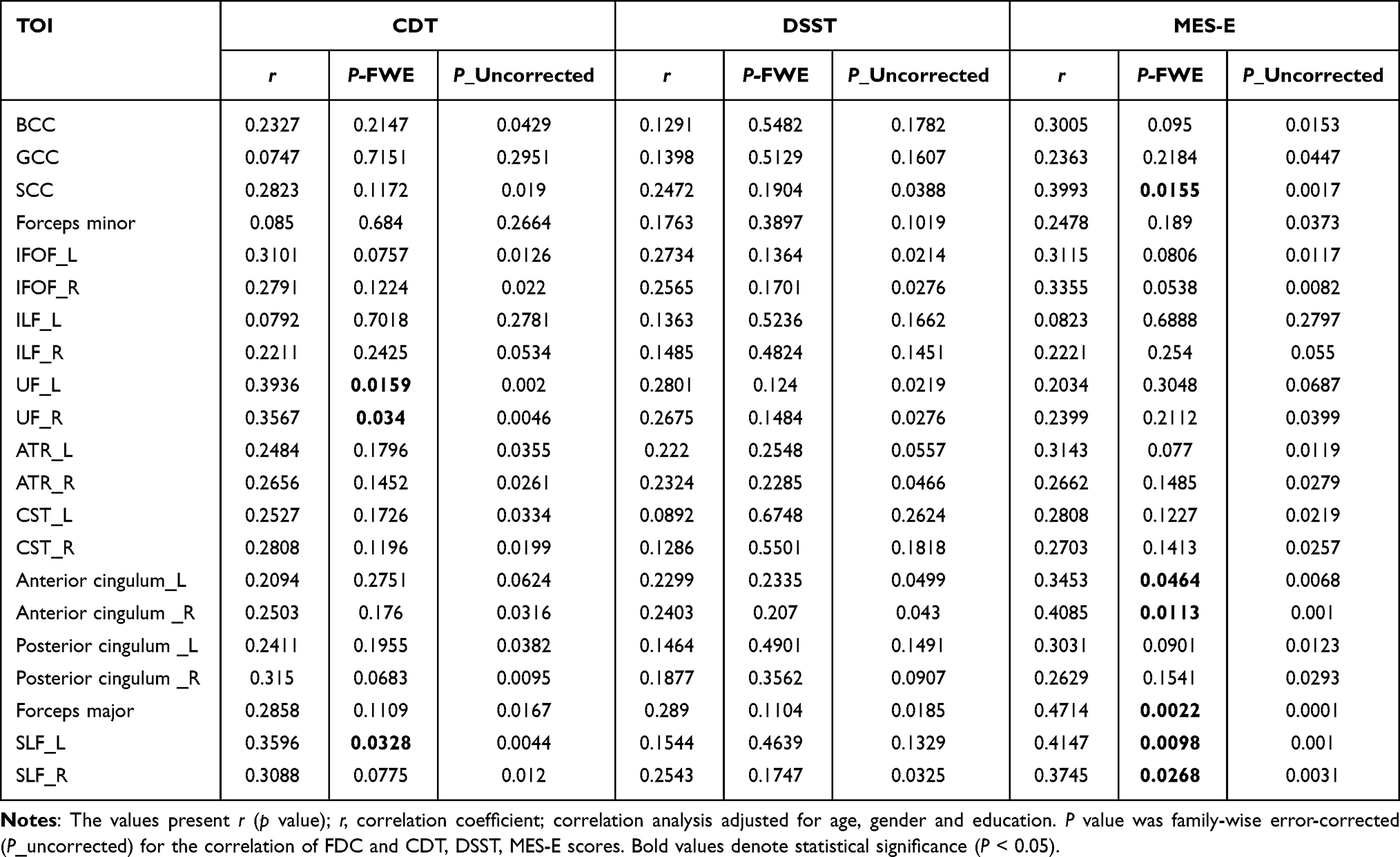 |
Table 3 Correlation Between FDC in Cerebral TOI That Were Statistically Different Between Groups with CDT, DSST and MES-E Scores |
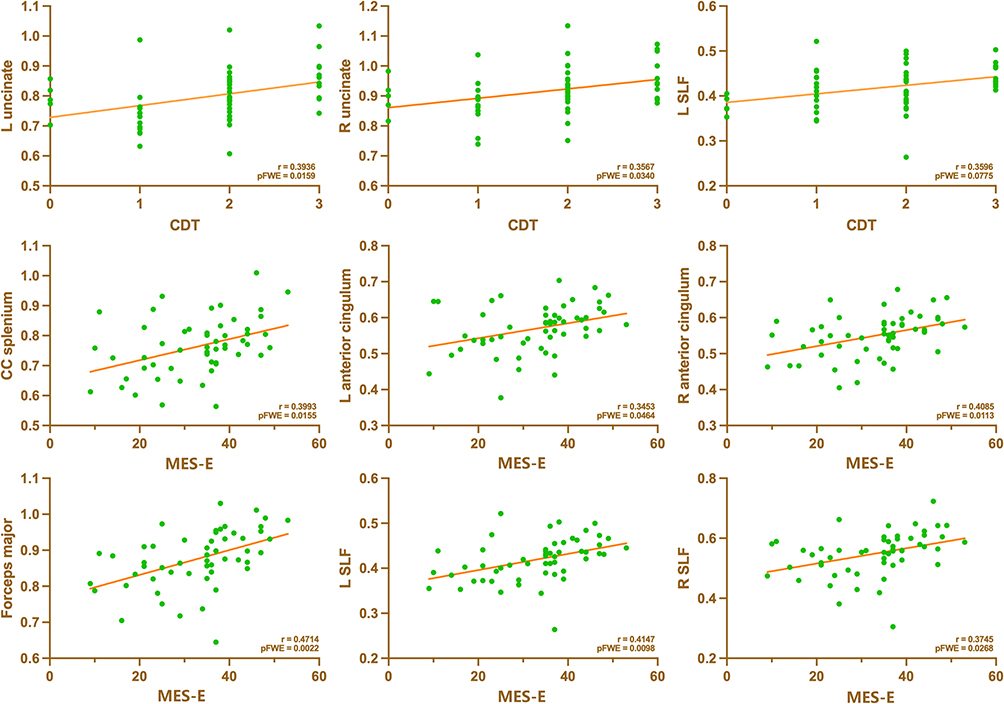 |
Figure 3 Correlations between exacted values of mean FDC of AD patients and scores of CDT and MES-E. |
Discussion
This study showed that compared to the AD-nLGS and NC groups, the damage to the structural WM integrity in the AD-LGS group was more extensive spatially, with more axonal loss in macroscopic and microscopic structures of certain specific WM tracts, such as SCC, BCC, forceps major, bilateral anterior cingulate tracts, bilateral SLF, bilateral UF, bilateral ATR, bilateral IFOF, bilateral ILF, right CST and bilateral posterior cingulate tracts. Compared to the AD-nLGS group, the AD-LGS group had extensive cognitive impairment and scored lower on the CDT, MES-E and DSST, indicating worse executive function, visuospatial ability and information processing speed. Notably, executive function in AD patients was more closely related to SCC, bilateral anterior cingulate tracts, forceps major, bilateral SLF, and bilateral UF, inferring that specific structural alterations of WM fiber tracts associated with executive function may be one of the mechanisms contributing to reduced grip strength in AD patients. These findings highlight the importance of monitoring and maintaining the normal structure and function of WM fiber tracts in AD to prevent or delay the occurrence and progression of the disease.
Current studies on the relationship between grip strength and WM structure mainly rely on WMH and DTI techniques, which have certain limitations. However, WMH results can be influenced by factors such as imaging equipment, image processing methods and evaluator subjectivity, resulting in lack of consistency and specificity, and are unable to accurately assess specific nerve fiber tracts.22,23 Kwak et al24 evaluated nerve fiber tracts using DTI technique and found a significant correlation between decreased grip strength in elderly women and reduced CST volume. Nevertheless, DTI has limitations in identifying diffusion rates of complex intersecting fiber tract structures within up to 90% of WM voxels, reducing the reliability of results.10 Various forms of microstructural and macrostructural changes in WM in neurodegenerative diseases can also make intersecting fibers more complex. If one type of intersecting fiber within a voxel decreases WM integrity while another increases connectivity, these two changes cannot be observed, so DTI is not inherently fiber-specific.25 However, FBA technology can address these deficiencies by showing the direction of multiple WM fiber tracts within a voxel and provide quantitative indicators for macroscopic and microscopic changes in WM fibers.25 The three FBA-related indicators included FD, FC and FDC. Decreased number or individual volume of axons may not affect macroscopic FC, as the extracellular matrix surrounding the axons becomes filled with inflammatory cells or proliferating glial cells. When extracellular matrix or cells surrounding the axons are cleared, fiber tracts may contract and result in decreased FC, suggesting that FD reduction may precede changes in FC.20 FD is more sensitive to neurodegenerative lesions, while decreased FC indicates more severe neurodegeneration and structural atrophy. FDC, reflecting the combined lesion degree of microstructure and macrostructure changes, is noteworthy for its improved sensitivity to the early nerve fiber tract degeneration. This is also why the FDC was mainly utilized for inter-group comparisons and correlation analysis, which is one of the advantages of this study.
Considerable evidence suggests that reduced grip strength is an early risk factor of cognitive decline and dementia incidence in late life.26 A cohort study of 340,212 cognitively normal elderly individuals found that every 5 kg increase in grip strength was associated with a reduced risk for all-cause dementia, AD, and vascular dementia.27 Despite some evidence linking reduced grip strength to cognitive decline and dementia, there still lacks in-depth mechanistic studies. Notably, every 5 kg decrease in grip strength is associated with increased WMH volume and dementia incidence in older adults,8 suggesting that abnormal WM changes may be one of the mechanisms linking cognitive decline and weaker grip strength. This may be due to that WM serves as the primary fiber pathway connecting cortical regions and plays a crucial role in transmitting information and maintaining normal cognitive or motor functions in the cortex. Abnormalities in WM connections can affect cortical function, which is closely related to grip strength. For example, Jiang et al3 included 42,843 normal older adults and found that stronger grip strength was associated with increased hippocampus and temporal cortex volumes. Stronger grip strength in patients with amnestic mild cognitive impairment (MCI) was related to better executive function, possibly due to changes in the hippocampus-prefrontal network integrity.28 This study found that AD-LGS patients had extensive micro- and macrostructural changes in WM fiber tracts, accompanied by extensive cognitive decline, suggesting that changes in specific WM fiber pathways in AD patients may link cognitive decline and reduced grip strength. AD is characterized by large-scale brain network dysfunction associated with Aβ deposition, neurofibrillary tangles, cortical atrophy, and functional disconnection between cortical areas. It exhibits a typical spatio-temporal change pattern13 where WM plays a crucial role in maintaining normal function of cortical regions. Early microstructural WM changes in AD initially manifest in the UF and progressively involve short fiber tracts connecting lateral temporal-parietal lobes as well as long fiber tracts linking to the frontal lobe.29 These WM fiber pathways connect cortical regions susceptible to AD pathology, like the default mode network (DMN), which underlies widespread cognitive decline.30 Anatomically, the cingulate tract is a hub connecting the DMN, including the medial prefrontal cortex, posterior cingulate cortex and medial temporal lobe.31,32 ILF and IFOF also connect to the DMN.33 The UF links the ventral medial prefrontal cortex and hippocampus, while SCC connects the posterior inferior parietal cortex, posterior cingulate gyrus and posterior pressor cortex, all of which are important components of DMN. Therefore, the abnormal structural changes of specific WM fiber tracts in AD patients may mediate the decline of cognitive function and the decrease in grip strength by affecting the normal function of cerebral cortex.
A recent study found a positive correlation between stronger grip strength and higher CDT scores in older adults, particularly in men.34 Weaker grip strength in patients with subjective cognitive decline and MCI was associated with worse baseline information processing speed and executive function but no longitudinal association was observed.35 However, previous studies lack a mechanistic explanation for the correlation between grip strength and executive function. Similarly, this study also revealed that AD-LGS patients had lower CDT, DSST and MES-E scores compared to AD-nLGS patients, indicating poorer executive and visuospatial functions. Further analysis showed that CDT scores were correlated with FDC of bilateral UF and left SLF; MES-E scores were correlated with SCC, bilateral SLF, forceps major and bilateral anterior cingulate tracts. This suggests that structural alterations in specific WM fiber tracts associated with executive function are closely related to grip strength reduction in AD patients.
Among the above brain regions, the CC is particularly noteworthy as its atrophy is linked to cognitive impairment in MCI and AD patients, even before the onset of AD.36,37 Composed of over 20 billion fibers,38 the CC serves as the largest WM fiber tract responsible for transmitting and integrating information between cerebral hemispheres, affecting executive function, visual-motion integration, spatial attention and complex motor control.39 It has four parts: the rostrum and genu form the front portion, BCC makes up the central portion and SCC is the posterior part. Few studies explored the relationship between the CC and grip strength in AD patients, with most research focusing on manual dexterity and coordination. Notably, the SCC connects both hemispheres’ primary motor cortex, associated with hand movements and coordination,40 and also links the bilateral parietal lobes and posterior cingulate cortex, which are closely related to grip strength41 and form a network structure associated with executive function.42 This study also found that AD-LGS patients had a smaller FDC in the SCC, which was associated with executive function. Garnier-Crussard et al43 propose that WMH of SCC is the core feature of AD, present in the early stage and associated with poor overall cognitive performance and executive function, independent of cortical Aβ deposition, cortical and hippocampal atrophy. SCC is more involved in AD and located near cortical regions more vulnerable to AD pathological proteins (eg, posterior cingulate cortex and posterior hippocampus),44 while GCC is more susceptible to cerebrovascular injury factors. Consequently, SCC may be a specific WM fiber tracts affecting grip strength and executive function decline in AD patients. It also sends out a large fiber tract as forceps major to the occipital lobe, forming a CC swelling in the medial wall of the atrial and occipital angle.45 Forceps major’s microstructure integrity is correlated with executive function, visual space and working memory,46 and abnormalities in the activity of the attached occipital visual cortex have also been strongly associated with decreased information processing speed.47 The combination of WM integrity in forceps major with perceptual speed and hippocampal volume (AUC = 0.911) was found to be the most predictive model for AD,48 indicating forceps major as another specific site of WM degeneration in AD.
AD-LGS patients also show significant axonal loss in the microstructure and macrostructure of the anterior cingulate fasciculus, associated with executive function. This crucial cingulate fasciculus connects the limbic system, cingulate gyrus and DMN,49 including short fiber tracts connecting to the cingulate gyrus and long fiber tracts to the prefrontal, parietal and temporal cortices, controlling cognitive functions like executive function and memory.50 While few studies explored the relationship between the anterior cingulate tract and grip strength, some have shown cortical regions connected by this tract are related to hand motor performance and coordination.51 Cordani et al52 found that hand motor performance decline in multiple sclerosis patients was associated with the left anterior cingulate gyrus atrophy and the right CST structural abnormalities, possibly because the anterior cingulate gyrus is instrumental in attention and modulating supplementary motor cortical areas during movement tasks. Stronger non-dominant side grip strength in AD patients was associated with larger hippocampal volume, while stronger dominant side grip strength was correlated with larger frontal cortical volume.53 Therefore, we speculate that structural alterations in the anterior cingulate tract in AD patients affect its connectivity to cortical regions related to executive function (eg, frontal lobe, anterior cingulate gyrus), mediating the relationship between the reduced grip strength and diminished executive function. Proliferating studies have also demonstrated that the anterior cingulate gyrus exhibits anatomical and functional abnormalities in amnestic MCI and AD, predicting the progression from amnestic MCI to AD. Normal connectivity of the anterior cingulate gyrus relies on the integrity of the anterior cingulate tract,54 so structural alterations in this tract may be a characteristic WM fiber tract involved in executive function decline and grip strength reduction in AD patients.
In addition, this study revealed that the higher the FDC of the left SLF and bilateral UF in AD-LGS group, the higher the CDT score, suggesting that SLF and UF are related to visuospatial and executive functions. Disruption of the SLF in AD patients can cause hypofunction of the DMN, sensorimotor and frontoparietal cortices, accompanied by decreased motor and executive abilities,55 as the SLF connects the frontal, parietal, temporal and occipital lobes that are vital for language, visuospatial function and metacognitive function.56,57 For example, in clinical pre-AD patients with a family history of dementia or carrying APOE e4, damage to the WM integrity of SLF, UF, CC and cingulum serve as an important predictor of poorer visual-motor integration ability,58 which can impact grip strength performance.59 MCI patients have more Aβ and tau protein deposition60 and microstructural WM damage in UF is also related to memory and executive function in AD and amnestic MCI patients.61 It connects with some limbic systems (eg, the hippocampus and amygdala) and the orbitofrontal cortex,62 which are vulnerable to Aβ and tau protein accumulation,63 and related to grip strength.64 Therefore, we should also consider the specific role of SLF and UF in the grip strength and executive functions of AD patients.
Conclusion
This study found that AD-LGS patients had more extensive structural alterations in WM macroscopically and microscopically, and a broad cognitive function decline compared to NC and AD-nLGS patients. Compared to AD-nLGS patients, AD-LGS patients performed worse in executive and visuospatial functions. Notably, specific structural alterations in WM fiber tracts associated with executive functions may mediate reduced grip strength in AD patients, such as SCC, bilateral anterior cingulate tracts, forceps major, left SLF and bilateral UF tracts. Grip strength may indicate micro- or macrostructural alterations in WM and executive function impairment in AD patients. These findings broaden our comprehension of the structural changes in WM fiber tracts – executive function alterations – grip strength reduction pathway. Targeted interventions for WM structural or functional changes may contribute to delaying AD progression and have some clinical implications for effective screening and treatment.
This study still has shortcomings: 1. It is a cross-sectional study, and future longitudinal studies are required to confirm the causal relationship between WM fiber tracts, grip strength and cognitive function. 2. The sample size is relatively small (especially for men), and more AD and MCI patients are needed for a stratified analysis by gender and age. Compared with the NC and AD-nLGS groups, the proportion of females and age in the AD-LGS group were significantly higher. The explanation was not only due to the small sample size but also that older age and female were the characteristics and major influencing factors for grip strength weakening in AD patients. Similarly, Jian et al65 included 2623 older Americans and found that weak grip strength was associated with female, older age and lower educational levels. To minimize potential confounding effects of age and gender, we made adjustments in imaging management accordingly. Therefore, the results can still provide some theoretical basis for the mechanism of grip strength decline and cognitive function impairment in AD patients. 3. Subjects were all right-handed, making the left CST more dominant than the right CST for grip strength.66 This may explain why the FDC of CST differ only on the right side among groups. Maximum grip strength of both hands should be collected for a stratified analysis. 4. Given that some studies have confirmed the effects of vitamin D levels, dipeptidyl peptidase-4 inhibitors, and renin-angiotensin-aldosterone system blockers on muscle strength,67–69 it is necessary to collect these indicators in future research. 5. Multi-shell data and higher b-value data allow for a more accurate assessment of fiber orientation, but data with a single b-value can also produce relatively robust results.10 Future research methods can be further refined using multi-shell MRI.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was performed in accordance with the guidelines of the 1964 Declaration of Helsinki and was approved by the ethics committee of the Second Affiliated Hospital of Soochow University (JD-LK-2021-049-01). All patients provided written informed consent prior to the study.
Acknowledgments
We would like to thank all the participants and their relatives, and the staff of the Second Affiliated Hospital of Soochow University for their cooperation and assistance. Shan-wen Liu and Xiao-ting Ma contributed equally to this work and shared the first authorship.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Application of Clinical Technology in Elderly Health Research Project in Jiangsu Province (LD2021031); Suzhou Science and Technology Plan Medical and Health Care Science and Technology Innovation Applied Basic Research (SKY2022161); Research Project of Neurological Diseases in the Second Affiliated Hospital of Suzhou University, Research Center (ND2023A01); Jiangsu Provincial Medical Key Discipline for the 14th Five-Year Plan (ZDXK202217). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no competing interests relevant to the content of this work.
References
1. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396:413–446. doi:10.1016/S0140-6736(20)30367-6
2. Dercon Q, Nicholas JM, James SN, Schott JM, Richards M. Grip strength from midlife as an indicator of later-life brain health and cognition: evidence from a British birth cohort. BMC Geriatr. 2021;21:475. doi:10.1186/s12877-021-02411-7
3. Jiang R, Westwater ML, Noble S, et al. Associations between grip strength, brain structure, and mental health in > 40,000 participants from the UK Biobank. BMC Med. 2022;20:286. doi:10.1186/s12916-022-02490-2
4. Pietroboni AM, Colombi A, Carandini T, Scarpini E, Galimberti D, Bozzali M. The Role of Amyloid-beta in White Matter Damage: possible Common Pathogenetic Mechanisms in Neurodegenerative and Demyelinating Diseases. J Alzheimers Dis. 2020;78:13–22. doi:10.3233/JAD-200868
5. Nasrabady SE, Rizvi B, Goldman JE, Brickman AM. White matter changes in Alzheimer’s disease: a focus on myelin and oligodendrocytes. Acta Neuropathol Commun. 2018;6:22. doi:10.1186/s40478-018-0515-3
6. Chu TH, Cummins K, Sparling JS, et al. Axonal and myelinic pathology in 5xFAD Alzheimer’s mouse spinal cord. PLoS One. 2017;12:e0188218. doi:10.1371/journal.pone.0188218
7. Chang YL, Chen TF, Shih YC, Chiu MJ, Yan SH, Tseng WY. Regional cingulum disruption, not gray matter atrophy, detects cognitive changes in amnestic mild cognitive impairment subtypes. J Alzheimers Dis. 2015;44:125–138. doi:10.3233/JAD-141839
8. Duchowny KA, Ackley SF, Brenowitz WD, et al. Associations Between Handgrip Strength and Dementia Risk, Cognition, and Neuroimaging Outcomes in the UK Biobank Cohort Study. JAMA Network Open. 2022;5:e2218314. doi:10.1001/jamanetworkopen.2022.18314
9. Jones DK, Knosche TR, Turner R. White matter integrity, fiber count, and other fallacies: the do’s and don’ts of diffusion MRI. Neuroimage. 2013;73:239–254. doi:10.1016/j.neuroimage.2012.06.081
10. Jeurissen B, Leemans A, Tournier JD, Jones DK, Sijbers J. Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum Brain Mapp. 2013;34:2747–2766. doi:10.1002/hbm.22099
11. Raffelt DA, Tournier JD, Smith RE, et al. Investigating white matter fibre density and morphology using fixel-based analysis. Neuroimage. 2017;144:58–73. doi:10.1016/j.neuroimage.2016.09.029
12. Raffelt DA, Smith RE, Ridgway GR, et al. Connectivity-based fixel enhancement: whole-brain statistical analysis of diffusion MRI measures in the presence of crossing fibres. Neuroimage. 2015;117:40–55. doi:10.1016/j.neuroimage.2015.05.039
13. Mito R, Raffelt D, Dhollander T, et al. Fibre-specific white matter reductions in Alzheimer’s disease and mild cognitive impairment. Brain. 2018;141:888–902. doi:10.1093/brain/awx355
14. Luo X, Wang S, Jiaerken Y, et al. Distinct fiber-specific white matter reductions pattern in early- and late-onset Alzheimer’s disease. Aging. 2021;13:12410–12430. doi:10.18632/aging.202702
15. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:263–269. doi:10.1016/j.jalz.2011.03.005
16. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol. 1987;149:351–356. doi:10.2214/ajr.149.2.351
17. Liu H, Jiao J, Zhu M, et al. Nutritional Status According to the Short-Form Mini Nutritional Assessment (MNA-SF) and Clinical Characteristics as Predictors of Length of Stay, Mortality, and Readmissions Among Older Inpatients in China: a National Study. Front Nutr. 2022;9:815578. doi:10.3389/fnut.2022.815578
18. Jia RX, Liang JH, Xu Y, Wang YQ. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: a meta-analysis. BMC Geriatr. 2019;19:181. doi:10.1186/s12877-019-1175-2
19. Chen LK, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc. 2020;21:300–307 e302. doi:10.1016/j.jamda.2019.12.012
20. Dhollander T, Clemente A, Singh M, et al. Fixel-based Analysis of Diffusion MRI: methods, Applications, Challenges and Opportunities. Neuroimage. 2021;241:118417. doi:10.1016/j.neuroimage.2021.118417
21. Nichols TE, Holmes AP. Nonparametric permutation tests for functional neuroimaging: a primer with examples. Hum Brain Mapp. 2002;15:1–25. doi:10.1002/hbm.1058
22. Qiao S, Li H, Guo F, Cai G, Zhang Y. Research progress on cognitive impairment and the expression of serum inflammatory markers in patients with white matter hyperintensities: a narrative review. Ann Transl Med. 2022;10:421. doi:10.21037/atm-22-1016
23. Melazzini L, Vitali P, Olivieri E, et al. White Matter Hyperintensities Quantification in Healthy Adults: a Systematic Review and Meta-Analysis. J Magn Reson Imaging. 2021;53:1732–1743. doi:10.1002/jmri.27479
24. Kwak SY, Kwak SG, Yoon TS, Kong EJ, Chang MC. Deterioration of Brain Neural Tracts in Elderly Women with Sarcopenia. Am J Geriatr Psychiatry. 2019;27:774–782. doi:10.1016/j.jagp.2019.02.018
25. Li Y, Guo T, Guan X, et al. Fixel-based analysis reveals fiber-specific alterations during the progression of Parkinson’s disease. Neuroimage Clin. 2020;27:102355. doi:10.1016/j.nicl.2020.102355
26. Esteban-Cornejo I, Ho FK, Petermann-Rocha F, et al. Handgrip strength and all-cause dementia incidence and mortality: findings from the UK Biobank prospective cohort study. J Cachexia, Sarcopenia Muscle. 2022;13:1514–1525. doi:10.1002/jcsm.12857
27. Kuo K, Zhang YR, Chen SD, et al. Associations of grip strength, walking pace, and the risk of incident dementia: a prospective cohort study of 340212 participants. Alzheimers Dement. 2023;19:1415–1427. doi:10.1002/alz.12793
28. Herold F, Labott BK, Grassler B, et al. A Link between Handgrip Strength and Executive Functioning: a Cross-Sectional Study in Older Adults with Mild Cognitive Impairment and Healthy Controls. Healthcare. 2022;10. doi:10.3390/healthcare10020230
29. Teipel S, Grothe MJ, Zhou J, et al. Measuring Cortical Connectivity in Alzheimer’s Disease as a Brain Neural Network Pathology: toward Clinical Applications. J Int Neuropsychol Soc. 2016;22:138–163. doi:10.1017/S1355617715000995
30. Yang Z, Chen Y, Hou X, Xu Y, Bai F. Topologically convergent and divergent large scale complex networks among Alzheimer’s disease spectrum patients: a systematic review. Heliyon. 2023;9:e15389. doi:10.1016/j.heliyon.2023.e15389
31. Tsolaki E, Sheth SA, Pouratian N. Variability of white matter anatomy in the subcallosal cingulate area. Hum Brain Mapp. 2021;42:2005–2017. doi:10.1002/hbm.25341
32. Vlegels N, Ossenkoppele R, van der Flier WM, et al. Alzheimer’s Disease Neuroimaging I. Does Loss of Integrity of the Cingulum Bundle Link Amyloid-beta Accumulation and Neurodegeneration in Alzheimer’s Disease? J Alzheimers Dis. 2022;89:39–49. doi:10.3233/JAD-220024
33. Hau J, Sarubbo S, Perchey G, et al. Cortical Terminations of the Inferior Fronto-Occipital and Uncinate Fasciculi: anatomical Stem-Based Virtual Dissection. Front Neuroanat. 2016;10:58. doi:10.3389/fnana.2016.00058
34. El Said SMS, Adly NN, Abdul-Rahman SA. Executive Function and Physical Function Among Community-Dwelling Egyptian Older Adults. J Alzheimers Dis. 2021;80:1583–1589. doi:10.3233/JAD-201423
35. Hooghiemstra AM, Ramakers I, Sistermans N, et al. Gait Speed and Grip Strength Reflect Cognitive Impairment and Are Modestly Related to Incident Cognitive Decline in Memory Clinic Patients With Subjective Cognitive Decline and Mild Cognitive Impairment: findings From the 4C Study. J Gerontol a Biol Sci Med Sci. 2017;72:846–854. doi:10.1093/gerona/glx003
36. Wang XD, Ren M, Zhu MW, et al. Corpus callosum atrophy associated with the degree of cognitive decline in patients with Alzheimer’s dementia or mild cognitive impairment: a meta-analysis of the region of interest structural imaging studies. J Psychiatr Res. 2015;63:10–19. doi:10.1016/j.jpsychires.2015.02.005
37. Van Schependom J, Niemantsverdriet E, Smeets D, Engelborghs S. Callosal circularity as an early marker for Alzheimer’s disease. Neuroimage Clin. 2018;19:516–526. doi:10.1016/j.nicl.2018.05.018
38. Liu Y, Hsu CH, Huang CC, et al. Connectivity-Based Topographical Changes of the Corpus Callosum During Aging. Front Aging Neurosci. 2021;13:753236. doi:10.3389/fnagi.2021.753236
39. Innocenti GM, Schmidt K, Milleret C, et al. The functional characterization of callosal connections. Prog Neurobiol. 2022;208:102186. doi:10.1016/j.pneurobio.2021.102186
40. Wahl M, Lauterbach-Soon B, Hattingen E, Hubers A, Ziemann U. Callosal anatomical and effective connectivity between primary motor cortices predicts visually cued bimanual temporal coordination performance. Brain Struct Funct. 2016;221:3427–3443. doi:10.1007/s00429-015-1110-z
41. Weitnauer L, Frisch S, Melie-Garcia L, et al. Mapping grip force to motor networks. Neuroimage. 2021;229:117735. doi:10.1016/j.neuroimage.2021.117735
42. Luna FG, Lupianez J, Martin-Arevalo E. Microstructural white matter connectivity underlying the attentional networks system. Behav Brain Res. 2021;401:113079. doi:10.1016/j.bbr.2020.113079
43. Garnier-Crussard A, Bougacha S, Wirth M, et al. White matter hyperintensity topography in Alzheimer’s disease and links to cognition. Alzheimers Dement. 2022;18:422–433. doi:10.1002/alz.12410
44. Gaubert M, Lange C, Garnier-Crussard A, et al. Topographic patterns of white matter hyperintensities are associated with multimodal neuroimaging biomarkers of Alzheimer’s disease. Alzheimers Res Ther. 2021;13:29. doi:10.1186/s13195-020-00759-3
45. Sihvonen AJ, Virtala P, Thiede A, Laasonen M, Kujala T. Structural white matter connectometry of reading and dyslexia. Neuroimage. 2021;241:118411. doi:10.1016/j.neuroimage.2021.118411
46. Krogsrud SK, Fjell AM, Tamnes CK, et al. Development of white matter microstructure in relation to verbal and visuospatial working memory-A longitudinal study. PLoS One. 2018;13:e0195540. doi:10.1371/journal.pone.0195540
47. Wang S, Jiaerken Y, Yu X, et al. Understanding the association between psychomotor processing speed and white matter hyperintensity: a comprehensive multi-modality MR imaging study. Hum Brain Mapp. 2020;41:605–616. doi:10.1002/hbm.24826
48. Muller T, Payton NM, Kalpouzos G, et al. Cognitive, Genetic, Brain Volume, and Diffusion Tensor Imaging Markers as Early Indicators of Dementia. J Alzheimers Dis. 2020;77:1443–1453. doi:10.3233/JAD-200445
49. Lin YC, Shih YC, Tseng WY, et al. Cingulum correlates of cognitive functions in patients with mild cognitive impairment and early Alzheimer’s disease: a diffusion spectrum imaging study. Brain Topogr. 2014;27:393–402. doi:10.1007/s10548-013-0346-2
50. Bubb EJ, Metzler-Baddeley C, Aggleton JP. The cingulum bundle: anatomy, function, and dysfunction. Neurosci Biobehav Rev. 2018;92:104–127. doi:10.1016/j.neubiorev.2018.05.008
51. Zhai F, Liu J, Su N, et al. Disrupted white matter integrity and network connectivity are related to poor motor performance. Sci Rep. 2020;10:18369. doi:10.1038/s41598-020-75617-1
52. Cordani C, Meani A, Esposito F, et al. Imaging correlates of hand motor performance in multiple sclerosis: a multiparametric structural and functional MRI study. Mult Scler. 2020;26:233–244. doi:10.1177/1352458518822145
53. Meysami S, Raji CA, Glatt RM, et al. Handgrip Strength Is Related to Hippocampal and Lobar Brain Volumes in a Cohort of Cognitively Impaired Older Adults with Confirmed Amyloid Burden. J Alzheimers Dis. 2023;91:999–1006. doi:10.3233/JAD-220886
54. Liang Y, Chen Y, Li H, et al. Disrupted functional connectivity related to differential degeneration of the cingulum bundle in mild cognitive impairment patients. Curr Alzheimer Res. 2015;12:255–265. doi:10.2174/1567205012666150302155336
55. Yang FPG, Bal SS, Lee JF, Chen CC. White Matter Differences in Networks in Elders with Mild Cognitive Impairment and Alzheimer’s Disease. Brain Connect. 2021;11:180–188. doi:10.1089/brain.2020.0767
56. Zheng Y, Wang D, Ye Q, Zou F, Li Y, Kwok SC. Diffusion property and functional connectivity of superior longitudinal fasciculus underpin human metacognition. Neuropsychologia. 2021;156:107847. doi:10.1016/j.neuropsychologia.2021.107847
57. Nakajima R, Kinoshita M, Shinohara H, Nakada M. The superior longitudinal fascicle: reconsidering the fronto-parietal neural network based on anatomy and function. Brain Imaging Behav. 2020;14:2817–2830. doi:10.1007/s11682-019-00187-4
58. Rogojin A, Gorbet DJ, Hawkins KM, Sergio LE. Differences in structural MRI and diffusion tensor imaging underlie visuomotor performance declines in older adults with an increased risk for Alzheimer’s disease. Front Aging Neurosci. 2022;14:1054516. doi:10.3389/fnagi.2022.1054516
59. Richardson JK, Ellmers TJ. The relationship between clinical measures of cognitive function and grip strength in healthy older adults. BMC Geriatr. 2022;22:907. doi:10.1186/s12877-022-03629-9
60. Pichet Binette A, Theaud G, Rheault F, et al. Bundle-specific associations between white matter microstructure and Abeta and tau pathology in preclinical Alzheimer’s disease. Elife. 2021:10. doi:10.7554/eLife.62929
61. Serra L, Cercignani M, Basile B, et al. White matter damage along the uncinate fasciculus contributes to cognitive decline in AD and DLB. Curr Alzheimer Res. 2012;9:326–333. doi:10.2174/156720512800107555
62. Granger SJ, Leal SL, Larson MS, et al. Integrity of the uncinate fasciculus is associated with emotional pattern separation-related fMRI signals in the hippocampal dentate and CA3. Neurobiol Learn Mem. 2021;177:107359. doi:10.1016/j.nlm.2020.107359
63. van der Kant R, Goldstein LSB, Ossenkoppele R. Amyloid-beta-independent regulators of tau pathology in Alzheimer disease. Nat Rev Neurosci. 2020;21:21–35. doi:10.1038/s41583-019-0240-3
64. Firth JA, Smith L, Sarris J, et al. Handgrip Strength Is Associated With Hippocampal Volume and White Matter Hyperintensities in Major Depression and Healthy Controls: a UK Biobank Study. Psychosom Med. 2020;82:39–46. doi:10.1097/PSY.0000000000000753
65. Huang J, Wang X, Zhu H, et al. Association between grip strength and cognitive impairment in older American adults. Front Mol Neurosci. 2022;15:973700. doi:10.3389/fnmol.2022.973700
66. Jang SH, Jang WH. Change of the Corticospinal Tract in the Unaffected Hemisphere by Change of the Dominant Hand Following Stroke: a Cohort Study. Medicine (Baltimore). 2016;95:e2620. doi:10.1097/MD.0000000000002620
67. Agoncillo M, Yu J, Gunton JE. The Role of Vitamin D in Skeletal Muscle Repair and Regeneration in Animal Models and Humans: a Systematic Review. Nutrients. 2023;15. doi:10.3390/nu15204377
68. Bouchi R, Fukuda T, Takeuchi T, et al. Dipeptidyl peptidase 4 inhibitors attenuates the decline of skeletal muscle mass in patients with type 2 diabetes. Diabetes Metab Res Rev. 2018;34. doi:10.1002/dmrr.2957
69. Ekiz T, Kara M, Ata AM, et al. Rewinding sarcopenia: a narrative review on the renin-angiotensin system. Aging Clin Exp Res. 2021;33:2379–2392. doi:10.1007/s40520-020-01761-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.