")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Causal Association Between Diabetes, Body Mass Index and Lichen Sclerosus: A Bidirectional Two-Sample Mendelian Randomization Analysis
Authors Liu L, Zhang Q, Chang J, Yang K
Received 1 December 2023
Accepted for publication 31 March 2024
Published 26 April 2024 Volume 2024:17 Pages 931—940
DOI https://doi.org/10.2147/CCID.S450399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lin Liu,1,2 Qiuli Zhang,1 Jianmin Chang,1,2 Kun Yang1
1Department of Dermatology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Peking Union Medical College, Chinese Academy of Medical Sciences, Graduate School of Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Kun Yang; Jianmin Chang, Email [email protected]; [email protected]
Background: Previous observational studies have found that lichen sclerosus (LS) is associated with metabolic statuses, such as diabetes mellitus (DM) and body mass index (BMI). However, there are also some studies showing that LS is not related to DM and BMI. The mechanism behind observational results is still unclear. Therefore, the causality of this relationship remains unknown. In this study, a bidirectional two-sample Mendelian randomization (MR) was conducted to investigate the correlation between DM, BMI, and LS.
Methods: The instrumental variables related to DM (including type 1 and type 2 diabetes), and BMI were identified from genome-wide association studies (GWAS) and a GWAS meta-analysis. The GWAS data for LS was from obtained the eighth edition of the FinnGen biological database released in 2022. Inverse variance weighted (IVW), weighted median, and MR-Egger methods were used to conduct a bidirectional two-sample MR analysis. Thereafter, the heterogeneity and horizontal pleiotropy were examined to determine whether the results were affected by a single-nucleotide polymorphism (SNP).
Results: We found a lack of evidence for the causal association of DM, and BMI on LS in inverse variance weighted (type 1 diabetes, OR=0.97, 95% CI=0.91– 1.04, p=0.429; type 2 diabetes, OR=0.91, 95% CI=0.82– 1.00, p=0.0511; BMI, OR=0.92, 95% CI=0.73– 1.15, p=0.4554). In the other direction, the results also showed that LS had no significant causal effect on DM and BMI.
Conclusion: This MR analysis demonstrated no significant causal relationship between DM and BMI with LS in both directions, which contradicts previous observational studies reporting a positive association. Potential confounding factors may contribute to previously observed associations, and further research is necessary.
Keywords: lichen sclerosus, diabetes mellitus, body mass index, Mendelian randomization
Introduction
Lichen sclerosus (LS) is a chronic inflammatory skin disease with a complex etiology that mainly affects the anal and genital regions. It can occur in men and women of any age, but usually affects more women than men, manifesting in a bimodal fashion in pre-pubertal children and middle-aged adults.1,2 LS mainly occurs in the genital region, with a typical clinical manifestation of white atrophic plaques. External genital lichen sclerosus can occur in areas such as the neck, shoulder, upper torso, thigh, and mouth. Genital lichen sclerosus is often accompanied by persistent itching and sexual pain, which can develop into anatomical malformations of the vulva, phimosis, and urinary and sexual dysfunction. The condition seriously affects the quality of life of patients and increases the risk of localized skin malignancies.3–6 Unlike genital lichen sclerosus, extragenital lichen sclerosus usually has no obvious symptoms, progresses slowly, and generally does not undergo malignant transformation.7 Observational studies have shown a correlation between DM, BMI, and LS.8–14 There are also studies indicating that LS is not related to diabetes and BMI.13,15 However, observational research may be limited by reverse causality and confounding factors. Understanding the causal relationship between DM, BMI and LS can help us better understand the pathogenesis of LS. At the same time, it can also guide doctors on whether to conduct relevant disease screening for patients, achieving early diagnosis and intervention of the disease.
MR analysis uses a genetic variation, known as single nucleotide polymorphism (SNP), as a tool variable to assess the causal relationship between risk factors for complex diseases. Due to the random allocation of alleles during gamete formation, MR analysis reduces confounding and enhances exposure-outcome associations with the exponential growth and widespread availability of genotype data. Therefore, MR analysis is considered a “natural” RCT, overcoming the limitations of observational research such as confounding factors and reverse causal relationships.16–18
In view of the uncertain causality of the relationships between DM, BMI, and LS, the present study applied MR to evaluate their correlation using data from the large Genome-Wide Association Study (GWAS).
Methods
Study Design
This study employed a bidirectional two-sample Mendelian randomization (MR) analysis method to study the causal relationship between DM, BMI, and LS. First, single-nucleotide polymorphisms (SNPs) related to DM (including type 1 and type 2 diabetes) and BMI were used to evaluate their causal impact on LS. Then, SNPs related to the LS were used as instrumental variables (IVs) to check for causal relationships in the other direction in order to rule out reverse causal relationships. Sensitivity analysis was conducted to test for heterogeneity and horizontal pleiotropy. In order to screen suitable IVs for dual sample bidirectional MR analysis, the following three key assumptions were adopted. Firstly, IVs used as a tool must be associated with the exposure of interest; secondly, IVs should not be associated with confounding factors; thirdly, genetic variation must not be associated with results independently of the exposure.19 The flowchart is shown in Figure 1.
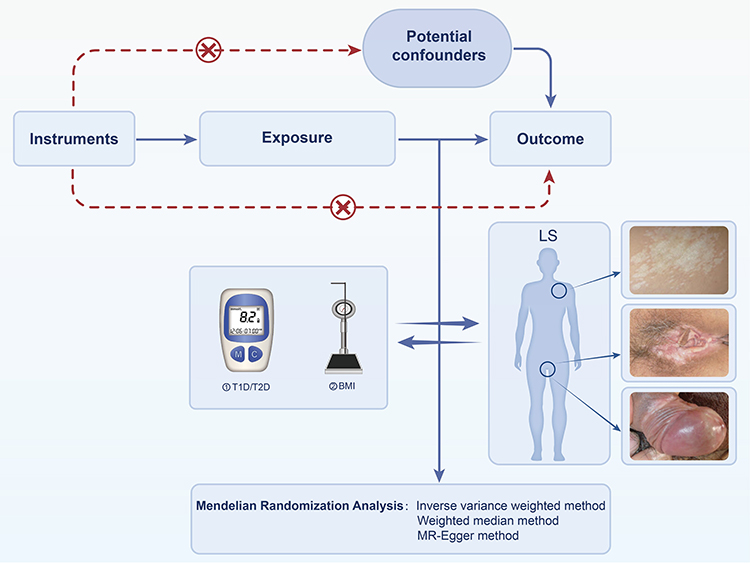 |
Figure 1 Workflow of Mendelian randomization study in this study. |
Data Source
Diabetes
Summary-level data were acquired from a GWAS meta-analysis of type 2 diabetes (T2D), which aimed to identify functional genes and infer the possible mechanism of T2D.20 This study included 62,892 cases of T2D and 596,424 controls, with 5,030,727 SNPs. A meta-analysis of three GWAS datasets of European descent was conducted: DIAbates genetic replication and meta-analysis (DIAGRAM, N=149821), the Genetic Epidemiology of Aging Study (GERA, N=53888), and the British Biological Bank (UKB, N=455607). Summary-level data on type 1 diabetes (GWAS ID: ebi-a-GCST010681) were obtained from a GWAS conducted in 2020, which aimed to identify new rare sites exerting a significant impact on the risk of type 1 diabetes (T1D).21 The study included 9358 cases of T1D and 15,705 controls, covering 12,783,129 SNPs from 12 European cohorts.
BMI
BMI data (GWAS ID: ieu-b-40) were obtained from a GWAS meta-analysis conducted by Yengo et al22 in 2018, in which a meta-analysis of previous GWAS of the Genetic Investigation of ANthropometric Traits (GIANT) consortium studies was performed with new GWAS of height and BMI in ∼450,000 participants of the UK Biobank (UKB), yielding a total sample size of ~700,000. The BMI dataset included 461,460 European male and female descendants with 9,851,867 SNPs, significantly increasing the number of GWAS related to BMI. This provided a larger GWAS sample size, enabling more discoveries.
Lichen sclerosus
The GWAS data for LS was obtained from the eighth edition of the FinnGen biological database released in 2022 (https://storage.googleapis.com/finngen-public-data-r8/summary_stats/finngen_R8_L12_LICHENSCLERATROPH.gz). In total, 1984 cases of LS and 321,903 controls were included, with 20,169,015 SNPs. The patients in this data include both males and females. However, the data does not specify whether the site of the disease is located in the genital area or outside the genital area. The FinnGen research project was launched in 2017, combining genomic information with digital healthcare data from Finnish participants. FinnGen’s research plan used 500,000 unique samples collected from the Finnish National Biobank Network to improve human health through genetic research.23
Since all data used were already in the public domain, no additional ethical approval was required. The genetic background of the study population was derived from people of European descent to avoid bias due to racial-related confounding factors (Table 1).
 |
Table 1 Details of GWAS Used for Exposures and Outcomes. |
Instrumental variable
Criteria for selecting instrumental variables: (1) SNP meets the genome-wide significance criteria (p < 5×10 − 8). However, when LS was exposed to T2D and BMI, no SNP met this standard, so the cut-off p-value was set to 5×10−6); (2) The parameter r2 threshold was set to 0.001 and the kilobase pair (kb) to 10,000 to minimize interference from linkage disequilibrium (LD);24 (3) F-statistic of each SNP was limited to greater than 10 to avoid weak tool bias. (4) We used PhenoScanner V2 to detect and remove genetic variations that exhibit significant associations with different phenotypes, in order to prevent potential horizontal pleiotropy. Finally, effective SNPs significantly related to exposure factors were obtained as IVs (Supplementary Tables 1–7).
Mendelian randomization analysis
The “TwoSampleMR” package in R version 4.1.2 was used for MR analysis. The inverse variance weighting (IVW) method used in this study mainly applies the reciprocal of the variance of each IV as a weight for weighted calculation. This process was conducted under the premise of ensuring that all IVs were valid, in order to evaluate horizontal multiple validity.25 The MR-Egger regression rule used the reciprocal of the outcome variance as the weight to perform a fitting, adding an intercept term.26 WME was defined as the median of a weighted empirical density function of ratio estimates.27
Sensitivity analysis
In this study, Cochran’s Q test was used to assess the heterogeneity between individual genetic variations. Heterogeneity was defined by Cochran’s Q test P<0.05, indicating that the relationship between exposure and outcome was affected by confounding factors. Therefore, the final Mendel randomization results used the IVW random effect model as the gold standard.28 In the Egger intercept method of horizontal pleiotropy, the cutoff value estimates whether genetic variation significantly affects outcomes through pathways other than exposure. In the current study, P<0.05 represented the presence of horizontal pleiotropy, indicating that the selected IV significantly affected outcomes through pathways other than exposure, which violates assumptions 2 and 3.29 The Leave-one-out method is mainly used to determine whether any one of the final SNPs is an outlier by individually eliminating each IV.30 Moreover, the stability of the results was also checked by observing the asymmetry in the funnel diagram. A crossover in the Leave-one-out method would suggest that the positive result was not stable The RadialMR method was employed to identify and remove abnormal SNPs.
Results
Diabetes and Lichen Sclerosus
Causal Effects of Diabetes on Lichen Sclerosus
In total, 29 SNPs related to T1D were used, and the IVW results showed no significant association with LS (OR=0.97, 95% CI=0.91–1.04, p=0.429) (Table 2). The Leave-one-out method result was shown in Supplementary Figure 1A. The scatter plot of MR analysis was shown in Figure 2A. Using 122 T2D-related SNPs, the IVW result was statistically significant (OR=0.88, 95% CI=0.78–0.99, p=0.031), but there was a crossover in the Leave-one-out method result (Supplementary Figure 1B), which indicated that the potential causal effect of T2D on LS was unstable Furthermore, the P value of MR Egger obtained by the Cochran Q test was 2.10×10−5 and the IVW p value was 1.16×10−5, indicating heterogeneity (Supplementary Table 8). The scatter plot of MR analysis was shown in Figure 2B. Subsequently, 10 outliers were identified by the RadialMR method. After removing the 10 outliers (rs10087241, rs10169613, rs1063355, rs11925227, rs16988333, rs1899951, rs2307111, rs2857605, rs576674, and rs753270), MR analysis was reapplied to evaluate the relationship between T2D and LS (Supplementary Figure 2A-D). The IVW results showed no significant correlation between T2D and LS (OR=0.91, 95% CI=0.82–1.00, p=0.0511), as shown in Table 2. In addition, there was no significant evidence of intercept (intercept=0.008; SE=0.008. p=0.113), indicating the absence of directional pleiotropy (Supplementary Table 9). Therefore, no obvious causal relationship was observed between T2D and LS. The funnel plots were shown in Supplementary Figure 3A and 3B.
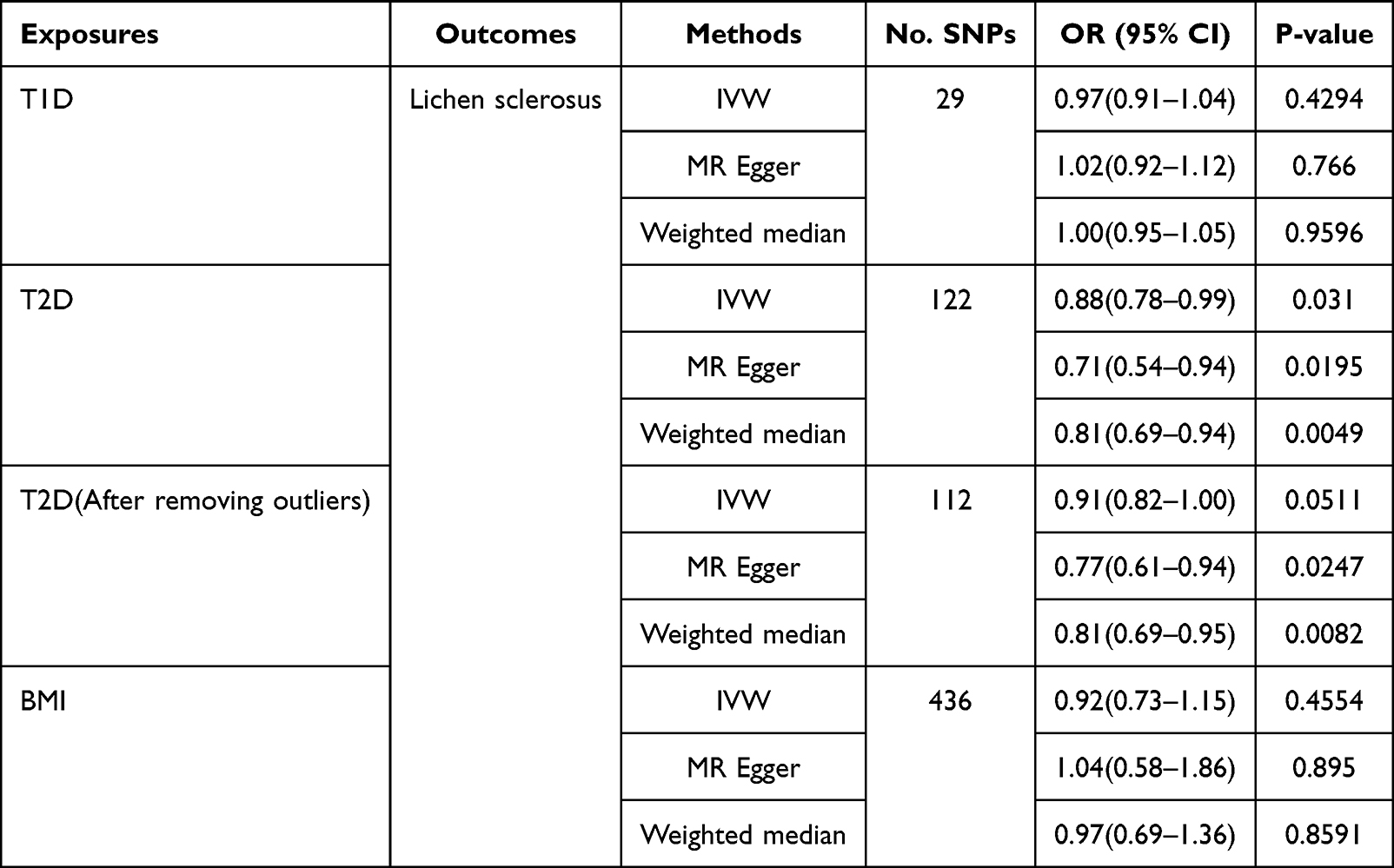 |
Table 2 The Causal Effect of (A) T1D, (B) T2D, and (C) BMI on Lichen Sclerosus. |
 |
Figure 2 Scatter plots visualizing the Mendelian randomization (MR) estimates of the different exposures ((A): Type 1 diabetes; (B): Type 2 diabetes; (C): Body mass index) with the outcome (lichen sclerosus). Inverse-variance weighted (IVW), MR-Egger, and weighted median methods were the main estimators of the analysis. |
Causal Effects of Lichen Sclerosus on Diabetes
Four SNPs were significantly related to LS and were used as IVs; the IVW results showed no significant association between LS and T1D (OR=0.74, 95% CI=0.27–2.05, p=0.5639) (Table 3). The scatter plot of MR analysis was shown in Figure 3A. Thereafter, 8 T2D-related SNPs (p<5×10−6) were used, and the IVW results showed no causal relationship between LS and T2D (OR=0.97, 95% CI=0.92–1.03, p=0.3979) (Table 3). The scatter plot of MR analysis was shown in Figure 3B. The Cochran Q test yielded an MR Egger P value of 0.005, while the IVW p value was 0.005 (Supplementary Table 10). However, the presence of heterogeneity did not affect the results as IVW can accept heterogenicity. The p-value obtained from the pleiotropic test was 0.45, indicating that IVs did not significantly affect outcomes through pathways other than exposure (Supplementary Table 11). The funnel plots were shown in Supplementary Figure 4A and 4B.
 |
Table 3 The Causal Effect of LS on (A) T1D, (B) T2D, and (C) BMI. |
 |
Figure 3 Scatter plots visualizing the Mendelian randomization (MR) estimates of the exposure (lichen sclerosus) with different outcomes ((A): Type 1 diabetes; (B): Type 2 diabetes; (C): Body mass index). |
BMI and Lichen Sclerosus
Causal Effects of BMI on Lichen Sclerosus
In total, 436 SNPs related to BMI were identified, and the IVW, MR Egger, and weighted median methods used to estimate the causal relationship between BMI and LS did not show a significant correlation (IVW, OR=0.92, 95% CI=0.73–1.15, p=0.4554; MR Egger, OR=1.04, 95% CI=0.58–1.86, p=0.8950; weighted median, OR=0.97, 95% CI=0.69–1.36, p=0.8584) (Table 2). The scatter plot of MR analysis was shown in Figure 2C. The Leave-one-out method result was shown in Supplementary Figure 1C. The P value of MR Egger obtained by the Cochran Q test was 0.017, while the IVW p value was 0.018 (Supplementary Table 8). The presence of heterogeneity did not affect the results. The funnel plot was shown in Supplementary Figure 3C.
Causal Effects of Lichen Sclerosus on BMI
In this study, 6 LS-related SNPs were identified to estimate the causal relationship between LS and BMI. IVW, MR Egger, and weighted media methods did not show a significant correlation (IVW, β=−0.01, SE=0.014, p=0.314; MR Egger, β=0.1, SE=0.080, p=0.282; weighted median, β=0.01, SE=0.007, p=0.444) (Table 3). The scatter plot of MR analysis was shown in Figure 3C. The P value of MR Egger obtained by the Cochran Q test was 9.00×10−7, with an IVW p value of 8.41×10−10 (Supplementary Table 10). The result was heterogeneous, therefore, IVW was used as the gold standard in the final result of the MR. The funnel plot was shown in Supplementary Figure 4C.
Discussion
The pathogenesis of LS involves genetic factors, immune factors, hormone levels, microbial infections, and other aspects.31 Sherman et al32 conducted a basic genetic study on family members of LS patients. The study found that 12% of family members of LS patients also had this disease, indicating the potential role of genetic components. Some studies have found that specific HLA types, especially DQ7, DQ8, and DQ9, are more common in LS patients.33–35 Studies also have found that the expression of estrogen receptors is increased in the external genitalia of LS patients.31 In this study, a bidirectional two-sample MR analysis was performed to determine the correlation between metabolic factors, including DM, BMI, and LS, revealing no correlation between them.
As early as 1988, Garcfa Bravo et al36 first published a report on the correlation between LS and diabetes. Subsequently, many studies have reported the correlation between LS and metabolic factors, such as DM and BMI. A retrospective cohort study found that women with LS were associated with an increased risk of metabolic syndrome. That study observed a 1.49-fold increase in the risk of LS with T2DM compared to normal individuals. Another retrospective study also found that an increase in BMI and vulvar LS were associated.14
Hofer et al10 performed a case-control study and found an association between male LS and increased BMI and diabetes. The study aimed to identify potential comorbidity factors that may promote its development and persistence. Considering the correlation between obesity and diabetes, they believed that the etiology or development of LS may have metabolic or lifestyle components. Therefore, the authors hypothesized that LS may be caused by systemic changes that affect blood perfusion in terminal organs, and that LS may not be solely a skin disease. Metabolic and lifestyle factors may play a role in the development of LS. Edmonds et al37 have also found that both adult and child patients with LS exhibited reduced regulation of cellular metabolism, and decreased physiological processes related to cellular metabolism. Moreover, Virgili’s et al8 research results also indicated a higher incidence of overweight and obesity in patients with vulvar LS than in the general population. These findings suggest that metabolic factors and possibly a sedentary lifestyle may play a role in the pathogenesis of GLS in genetically susceptible patients. Despite some differences in the onset of symptoms, the risk profile is similar for men and women. Therefore, metabolic factors were hypothesized to be involved in the pathogenesis of LS. The article also mentioned that their observations only assumed causal relationships. Nevertheless, no histological confirmation of LS patients was performed in the study, and the study cohort included only caucasian patients, so the findings may not be generalized to other races.8
All previous observational studies were susceptible to confusing risk factors. In contrast, the present study applied MR methods to maximize the disclosure of causal relationships despite potential bias. The results revealed that diabetes was not a risk factor for LS, and LS was not a predisposing factor for diabetes. On the one hand, we believe that a large part of the high-risk population comprises menopausal women and middle-aged men, which also coincides with the onset age of T2D, potentially leading to a false combination of the two diseases.1 On the other hand, the current diagnostic standard of LS states that pathology can not be necessary in cases with typical clinical manifestations, which makes the diagnosis of the disease subjective. In addition, patients with diabetes are prone to skin itching and eczema.1,38–42 Therefore, there is a possibility of misdiagnosis of vulval LS in clinical practice. Due to LS occurring mostly in the genital area, it can cause discomfort in the external genitalia, leading to behavioral changes such as a decrease in overall activity levels. This may lead to a relatively high BMI in LS patients. The present study applied MR analysis and found no correlation between diabetes (including T1D and T2D), BMI, and LS. However, these findings do not elucidate whether controlling the metabolic factors of individuals already suffering from LS would reduce its progress. Therefore, managing these factors is still important to minimize their inherent negative health effects.
This research has several significant advantages. To our knowledge, this is the first study to explore the two-way causal relationship between DM, BMI, and LS through bidirectional two-sample MR analysis. Compared to observational studies, this analysis method is less susceptible to potential confounding, reverse causality, and non-differential measurement exposure errors. Secondly, the current results have been confirmed in various sensitivity analyses, and there was no sign of horizontal pleiotropy. Nevertheless, Mendelian randomized studies also have some limitations. First, the incidence of LS in men and women and its relationship to metabolic factors could not be determined as the FinnGen biological database did not include information on the gender of LS. Then, further stratification of the included population is not possible owing to the nature of GWAS summary statistics. Moreover, all GWAS data were collected from the European population, and whether the current findings can be extended to other populations remains to be investigated. Prospective studies with a larger sample size are also needed for further exploration.
Conclusions
In conclusion, our study suggests the lack of causal relationship between diabetes, BMI, and lichen sclerosus. Potential confounding factors may contribute to previously observed associations, and further research is necessary.
Abbreviations
LS, Lichen sclerosus; GLS, Genitalia lichen sclerosus; DM, Diabetes mellitus; T1D, Type 1 diabetes; T2D, Type 2 diabetes; BMI, Body mass index; MR, Mendelian randomization; GWAS, Genome-wide association studies; IVW, Inverse variance weighted; IV, Instrumental variable; SNP, Single-nucleotide polymorphism.
Data Sharing Statement
All analyses were conducted using publicly available data. The GWAS summary data for type 1 diabetes and BMI are available in GWAS catalog, at https://gwas.mrcieu.ac.uk/. The summary-level data of type 2 diabetes were acquired from a GWAS meta-analysis. The GWAS summary data for lichen sclerosus are available in FinnGen, at https://www.finngen.fi/en.
Ethics Approval and Consent to Participate
According to Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Beings adopted by the National Science and Technology Ethics Committee of the People’s Republic of China, ethical review can be exempted because the data used in this study do not cause any harm to human beings, do not involve any sensitive personal information or commercial interests, and the databases selected are open and legal. Therefore, approval from a new ethics review committee is not required.
Acknowledgments
We want to acknowledge the participants and investigators of the FinnGen study. We thank all the participants and investigators who provided valuable genetic summary statistics for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82203919).
Disclosure
The authors declare they have no conflicts of interest.
References
1. Tran DA, Tan X, Macri CJ, Goldstein AT, Fu SW. Lichen Sclerosus: an autoimmunopathogenic and genomic enigma with emerging genetic and immune targets. Int J Biol Sci. 2019;15(7):1429–1439. doi:10.7150/ijbs.34613
2. De Luca DA, Papara C, Vorobyev A, et al. Lichen sclerosus: the 2023 update. Front Med. 2023;10:1106318.
3. Wallace HJ. Lichen sclerosus et atrophicus. Trans St Johns Hosp Dermatol Soc. 1971;57(1):9–30.
4. Kirtschig G, Cooper S, Aberer W, et al. Evidence-based (S3) guideline on (anogenital) lichen sclerosus. J Eur Acad Dermatol Venereol. 2017;31(2):e81–e83. doi:10.1111/jdv.13740
5. Halonen P, Jakobsson M, Heikinheimo O, Riska A, Gissler M, Pukkala E. Lichen sclerosus and risk of cancer. Int J Cancer. 2017;140(9):1998–2002. doi:10.1002/ijc.30621
6. Micheletti L, Preti M, Radici G, et al. Vulvar lichen sclerosus and neoplastic transformation: a retrospective study of 976 cases. J Low Genit Tract Dis. 2016;20(2):180–183. doi:10.1097/LGT.0000000000000186
7. Arif T, Fatima R, Sami M. Extragenital lichen sclerosus: a comprehensive review. Australas J Dermatol. 2022;63(4):452–462. doi:10.1111/ajd.13890
8. Virgili A, Borghi A, Cazzaniga S, et al. New insights into potential risk factors and associations in genital lichen sclerosus: data from a multicentre Italian study on 729 consecutive cases. J Eur Acad Dermatol Venereol. 2017;31(4):699–704. doi:10.1111/jdv.13867
9. Erickson BA, Elliott SP, Myers JB, et al. Understanding the relationship between chronic systemic disease and lichen sclerosus urethral strictures. J Urol. 2016;195(2):363–368. doi:10.1016/j.juro.2015.08.096
10. Hofer MD, Meeks JJ, Mehdiratta N, Granieri MA, Cashy J, Gonzalez CM. Lichen sclerosus in men is associated with elevated body mass index, diabetes mellitus, coronary artery disease and smoking. World J Urol. 2014;32(1):105–108. doi:10.1007/s00345-013-1090-7
11. Fekete GL, Schwarzkopf-Kolb D, Brihan I, Boda D, Fekete L. Balanitis xerotica obliterans: an observational, descriptive and retrospective clinical study. Exp Ther Med. 2022;23(5):361. doi:10.3892/etm.2022.11288
12. Magro CM, Kalomeris TA, Mo JH, Rice M, Nuovo G. Lichen sclerosus: a C5B-9 mediated chronic microvascular injury syndrome potentially reflective of common adult comorbidities. Ann Diagn Pathol. 2023;63:152098. doi:10.1016/j.anndiagpath.2022.152098
13. Ranum A, Freese R, Ramesh V, Pearson DR. Lichen sclerosus in female patients is associated with an increased risk of metabolic syndrome and cardiovascular comorbidities: a retrospective cohort review. Br J Dermatol. 2022;187(6):1030–1032. doi:10.1111/bjd.21811
14. Luu Y, Cheng AL, Reisz C. Elevated body mass index, statin use, and cholecystectomy are associated with vulvar lichen sclerosus: a retrospective, case-control study. J Am Acad Dermatol. 2023;88(6):1376–1378. doi:10.1016/j.jaad.2023.01.023
15. Sideri M, Parazzini F, Rognoni MT, et al. Risk factors for vulvar lichen sclerosus. Am J Obstet Gynecol. 1989;161(1):38–42. doi:10.1016/0002-9378(89)90228-7
16. Sekula P, Del Greco MF, Pattaro C, Köttgen A. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1681/ASN.2016010098
17. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
18. Hemani G, Bowden J, Davey Smith G. Evaluating the potential role of pleiotropy in Mendelian randomization studies. Hum Mol Genet. 2018;27(R2):R195–R208. doi:10.1093/hmg/ddy163
19. Boef AG, Dekkers OM, le Cessie S. Mendelian randomization studies: a review of the approaches used and the quality of reporting. Int J Epidemiol. 2015;44(2):496–511. doi:10.1093/ije/dyv071
20. Xue A, Wu Y, Zhu Z, et al. Genome-wide association analyses identify 143 risk variants and putative regulatory mechanisms for type 2 diabetes. Nat Commun. 2018;9(1):2941. doi:10.1038/s41467-018-04951-w
21. Forgetta V, Manousaki D, Istomine R, et al. Rare genetic variants of large effect influence risk of type 1 diabetes. Diabetes. 2020;69(4):784–795. doi:10.2337/db19-0831
22. Yengo L, Sidorenko J, Kemper KE, et al. Meta-analysis of genome-wide association studies for height and body mass index in ∼700000 individuals of European ancestry. Hum Mol Genet. 2018;27(20):3641–3649. doi:10.1093/hmg/ddy271
23. Kurki MI, Karjalainen J, Palta P, et al. Author correction: finngen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;615(7952):E19.
24. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7. 10.7554/eLife.34408
25. Burgess S, Bowden J, Fall T, Ingelsson E, Thompson SG. Sensitivity analyses for robust causal inference from Mendelian randomization analyses with multiple genetic variants. Epidemiology. 2017;28(1):30–42. doi:10.1097/EDE.0000000000000559
26. Slob EAW, Groenen PJF, Thurik AR, Rietveld CA. A note on the use of egger regression in Mendelian randomization studies. Int J Epidemiol. 2017;46(6):2094–2097. doi:10.1093/ije/dyx191
27. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
28. Bowden J, Spiller W, Del Greco MF, et al. Improving the visualization, interpretation and analysis of two-sample summary data Mendelian randomization via the radial plot and radial regression. Int J Epidemiol. 2018;47(6):2100. doi:10.1093/ije/dyy265
29. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
30. Gronau QF, Wagenmakers EJ. Limitations of bayesian leave-one-out cross-validation for model selection. Comput Brain Behav. 2019;2(1):1–11. doi:10.1007/s42113-018-0011-7
31. Taylor AH, Guzail M, Al-Azzawi F. Differential expression of oestrogen receptor isoforms and androgen receptor in the normal vulva and vagina compared with vulval lichen sclerosus and chronic vaginitis. Br J Dermatol. 2008;158(2):319–328. doi:10.1111/j.1365-2133.2007.08371.x
32. Sherman V, McPherson T, Baldo M, Salim A, Gao XH, Wojnarowska F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. 2010;24(9):1031–1034. doi:10.1111/j.1468-3083.2010.03572.x
33. Azurdia RM, Luzzi GA, Byren I, et al. Lichen sclerosus in adult men: a study of HLA associations and susceptibility to autoimmune disease. Br J Dermatol. 1999;140(1):79–83. doi:10.1046/j.1365-2133.1999.02611.x
34. Marren P, Yell J, Charnock FM, Bunce M, Welsh K, Wojnarowska F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. 1995;132(2):197–203. doi:10.1111/j.1365-2133.1995.tb05013.x
35. Powell J, Wojnarowska F, Winsey S, Marren P, Welsh K. Lichen sclerosus premenarche: autoimmunity and immunogenetics. Br J Dermatol. 2000;142(3):481–484. doi:10.1046/j.1365-2133.2000.03360.x
36. García-Bravo B, Sánchez-Pedreño P, Rodríguez-Pichardo A, Camacho F. Lichen sclerosus et atrophicus. A study of 76 cases and their relation to diabetes. J Am Acad Dermatol. 1988;19(3):482–485. doi:10.1016/S0190-9622(88)70201-7
37. Edmonds E, Barton G, Buisson S, et al. Gene expression profiling in male genital lichen sclerosus. Int J Exp Pathol. 2011;92(5):320–325. doi:10.1111/j.1365-2613.2011.00779.x
38. Kirtschi G. Lichen sclerosus-presentation diagnosis and management. Dtsch Arztebl Int. 2016;113(19):337–343. doi:10.3238/arztebl.2016.0337
39. de Lusignan S, Alexander H, Broderick C, et al. Atopic dermatitis and risk of autoimmune conditions: population-based cohort study. J Allergy Clin Immunol. 2022;150(3):709–713. doi:10.1016/j.jaci.2022.03.030
40. Xu X, Zhang H, Li L, et al. Study of the involvement of the P2Y12 receptor in chronic itching in type 2 diabetes mellitus. Mol Neurobiol. 2022;59(3):1604–1618. doi:10.1007/s12035-021-02676-4
41. Roh YS, Choi J, Sutaria N, Kwatra SG. Itch: epidemiology, clinical presentation, and diagnostic workup. J Am Acad Dermatol. 2022;86(1):1–14. doi:10.1016/j.jaad.2021.07.076
42. Stawiski MA, Voorhees JJ. Cutaneous signs of diabetes mellitus. Cutis. 1976;18(3):415–421.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.