")
Back to Journals » Clinical Interventions in Aging » Volume 19
Challenges in Delivering Effective Care for Older Persons with Fragility Fractures
Authors Hurtado Y, Hernández OA , Atencio De Leon DP , Duque G
Received 1 September 2023
Accepted for publication 19 January 2024
Published 24 January 2024 Volume 2024:19 Pages 133—140
DOI https://doi.org/10.2147/CIA.S433999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yesid Hurtado,1 Odismar Andrea Hernández,2 Diana Patricia Atencio De Leon,2 Gustavo Duque3,4
1Division of Endocrinology, Hospital San José, Bogotá, Colombia; 2Division of Geriatric Medicine, La cardio/Fundación Cardioinfantil, Bogotá, Colombia; 3Bone, Muscle & Geroscience Research Group, Research Institute of the McGill University Health Centre, Montreal, Quebec, Canada; 4Dr. Joseph Kaufmann Chair in Geriatric Medicine, Department of Medicine, McGill University, Montreal, Quebec, Canada
Correspondence: Gustavo Duque, FRACP, FGSA, Research Institute of the MUHC - 1001 Decarie Blvd, Room EM1.3226, Montreal, Quebec, H4A 3J1, Canada, Tel +1514-934-1934 x 35165, Email [email protected]
Abstract: Fragility fractures occur because of low-impact trauma or even spontaneously in individuals with osteoporosis. Caring for older persons with fragility fractures can present several challenges due to the unique needs and vulnerabilities of this population. Older individuals commonly have multiple medical conditions, such as osteoporosis, arthritis, cardiovascular diseases, and diabetes. These comorbidities can complicate fracture management and increase the risk of complications. Fracture repair through surgery may be more complex in older patients due to poor bone quality, decreased tissue elasticity, and higher chances of anesthesia complications. In addition, mobility and functional limitations post-fracture are highly prevalent in this population, affecting their independence and increasing their risk of institutionalization. Addressing these challenges requires a multidisciplinary approach involving orthopedic surgeons, geriatricians, physical and rehabilitation physicians, physiotherapists, occupational therapists, dieticians, social workers, and caregivers. Preventive measures, such as fall prevention strategies and osteoporosis management, can also play a vital role in reducing the incidence of fragility fractures in older persons.
Keywords: osteoporosis, fragility fractures, older persons, osteosarcopenia, rehabilitation
Introduction
Fractures associated with osteoporosis are a significant medical occurrence. According to the World Health Organization (WHO), such cases will triple in the next 50 years.1 It is estimated that around one in three women and one in twelve men will suffer a hip fracture throughout their lives.2
Fragility fractures occur due to low-impact trauma and are usually associated with osteoporosis. More than 85% of hip fractures occur in people over 65 years of age;3 this age group suffers a higher incidence of falls at an older age that may be related to increased frailty and functional decline, as well as other frequent alterations in older persons such as decreased visual acuity, neuromuscular coordination, and balance.4,5
Additionally, multimorbidity, functional or cognitive dependence, and frailty syndrome present unique characteristics in this population that translate into the need for special attention to care for their health and functionality. Part of the predisposition to have a fragility fracture derives from the decrease in bone mineral density over the years, delayed bone healing due to the lower expression of type 2 collagen, as well as the lower amount of osteochondral stem cells with proliferation and differentiation potential that are characteristic of bone aging.6–8
Much of the consideration on the quality of life is that after a fragility fracture, between 25 and 75% of people with independent gait may have a severe functional decline and be unable to walk without support after one year.9
The initial management of a fracture in older people can be long and complex. Initial hospital care needs should involve a global assessment of the different aspects of the comprehensive geriatric assessment, with a more significant impact on the control of comorbidities, the presence of complications, and cognitive or functional deterioration. These factors can generate a greater risk of postoperative complications with effects on quality of life and increased costs for the health system.6
In the postoperative period, 6.8% of older patients require prolonged hospitalization for their care. Despite treatment and rehabilitation, over half of these cases fail to recover their functional status.6 It is estimated that mortality from hip fractures ranges between 18 and 33% per year.10 This rate is five to eight times higher among older persons when compared with non-fractured patients. In-hospital mortality is around 2.7%, and after discharge, patients are 3.5 times more likely to die in the next 12 months.6 This risk persists even 10 years after the event.11
For these reasons, there are many challenges when dealing with a patient with a fragility fracture, especially among older persons whose prognosis is even more complex given their specific circumstances. Here, we will develop this topic by addressing its main associated factors and how to approach them in clinical practice.
Care Models for Older Persons with Fragility Fractures
In countries like Canada, alternatives have been developed to care for older fractured patients. For example, the “fast track” allows patients presumed to have suffered a fracture to receive priority analgesia, a rapid diagnosis, and timely care.12,13 Another successful example in this medical practice is the “Blue Book” of the United Kingdom, which describes six standards for high quality hip fracture care. The standards include arrival at the orthopedics department within 4 hours, performing surgery within 48 hours, minimizing the risk of pressure ulcers, receiving early management, and continuing with fall prevention after the event.14 This has been considered one of the best strategies for treating older patients with hip fractures, resulting in improved mortality outcomes.15
Based on these experiences, specific scenarios in the approach to these patients, including evidence-based recommendations from global initiatives such as the International Osteoporosis Foundation and the Fragility Fracture Network, will be discussed.
Preoperative
One of the difficulties that has been observed is waiting for patients to be transferred to the operating rooms in time for prompt surgical intervention. This is cause for concern, given that older patients with hip fractures should undergo surgery within the first 24 hours after diagnosis. For those with oral anticoagulation prior to the injury, a maximum of 48 hours could be expected.12,16,17 Surgical correction of the fracture in the first 48 hours after admission has been shown to decrease mortality risk in patients with hip fractures (OR = 0.74, 95% confidence interval [CI] 0.67 to 0.81).15,18
The scenario is complex after a hip fracture, during which variables such as pain, blood loss and immobilization period must be evaluated since these events lead to hypercoagulability, which increases the risk of serious perioperative complications such as thromboembolic disease.19 Preoperative evaluations should include functional status before the fracture, baseline cognitive status, the presence of delirium, hydro electrolytic status, as well as monitoring polypharmacy and immobility.14
From the pain management perspective, pre-surgical regional nerve blocks are an important alternative to avoid or reduce the use of opioids, which have been associated with delirium and a more extended hospital stay.12
Given the complexity of older persons regarding fragility fractures, it is important that they are evaluated by an experienced multidisciplinary group, which is only available in some care centers. This type of preoperative multidisciplinary care allows rapid stabilization and medical optimization, which reduces delays in surgery and provides early treatment for comorbidities, also reducing the risk of delirium and in-hospital mortality.15,20,21 In particular, orthogeriatric co-management care has been associated with a decrease in hospital mortality (RR = 0.60 95% CI 0.43 to 0.84),22 the development of pressure ulcers (OR = 0.3, 95% CI 0.1 to 0.7 p = 0.009), as well as improved pain control and facilitated early mobilization.23,24
Postoperative
It has been determined that the factors associated with the most significant number of postoperative complications are frailty and malignancy.10,25 Other situations also affect prognosis, such as decompensation of heart failure, pulmonary infections, pressure ulcers, and delirium, which could worsen the clinical course of patients.10
On the other hand, delirium is a common and severe complication in older patients, particularly after hip fracture surgery, with an incidence between 20 and 50%.26 It has been associated with falls, impaired functional and cognitive recovery, prolonged hospital stays, and increased mortality.27 One of the evaluation methods for this condition is the Confusion Assessment Method (CAM) scale, which is a simple and quick tool for medical personnel to execute.28
Pressure ulcers are common but preventable complications,29 which are associated with delayed rehabilitation and therefore a worse functional prognosis and higher mortality.30 Among the factors related to these are malnutrition, low weight, diabetes, the presence of neuropathy, poor skin condition and, above all, immobility. The risk of pressure injuries must always be assessed, and different tools can be used, such as the Braden Scale, which has been validated.31
Osteoporosis Treatment
After the first minimal trauma fracture, the risk of a new fracture increases up to 25% in the following 2 years, particularly in women. This risk continues to grow in the following years.32 Because of this, it is vitally important to start pharmacological therapy early for osteoporosis to prevent new fractures both in the short and long term.12 However, the pharmacological initiation does not occur as expected, often due to administrative problems but sometimes due to fear of using this type of medication. This is due to the belief that such therapy could alter the course of osteosynthesis. Currently, there is no evidence that osteoporosis therapy affects the formation of bone callus in operated fractures. On the contrary, the benefit of early initiation of therapy has shown better results, even before hospital discharge, which is very important for the education of the medical team to improve the practice of this recommendation.12
Rehabilitation and Falls Prevention
Rehabilitation after a fracture is essential. It must be carried out early after surgical intervention and involve progressive resistance, weight loads, and balance training, which reduce postoperative complications such as pneumonia, thromboembolic events, urinary tract infections, and pressure ulcers,12 which are related to decreased activities of daily life,33 alterations in the quality of life,34 new falls and hospitalizations.35
The increased morbidity and mortality following a fracture are mainly due to decreased mobility and impaired balance, which can lead to a difficult-to-manage condition called fear of falling.36 This results in only approximately 40% of older people returning to their previous daily activity.9
The delay in rehabilitation has been observed to increase the risk of in-hospital mortality (OR 2.2, 95% CI 1.06–4.42- P= 0.034).17 The duration of the rehabilitation process varies between 9 months for the balance deficit and approximately 1 year to recover walking and its usual speed. Therefore, this practice is not only restricted to the intra-hospital setting but extends to the outpatient setting.12
Considering that falls are an important risk factor for fractures, falls risk assessment and falls prevention interventions should be promptly initiated after rehabilitation. Strategies for assessment and prevention of falls have been recently summarized in the World Guidelines for Falls Prevention.37
Nutrition
Since the cessation of the bone mass peak, it is known that adults over 50 years of age should have an adequate calcium intake of 1200 mg of elemental calcium per day.38 It is necessary to have adequate dietary and/or pharmacological sources for this purpose, improving the prevention of osteoporosis.39,40 Additionally, vitamin D supplementation in doses of at least 700 to 800 IU daily or more is essential for optimal intestinal absorption of calcium and phosphorus. This can also improve balance and muscle strength, thus reducing the risk of falls.41
Nutritional assessment is essential to profile older patients, which can be assessed using the mini-nutritional assessment short form (MNA-SF)42 or the universal malnutrition screening tool (MUST).43 An accurate assessment of muscle mass and body weight is recommended.12
Malnutrition in older persons with hip fractures is relevant since it is associated with higher complications and mortality rates,44 and its prevalence can reach up to 85%.45 Nutritional status before the fracture can contribute to adequate rehabilitation time and subsequent recovery.46
For this reason, early oral nutritional protein supplementation is another fundamental pillar in the comprehensive management of an older person with a fracture, starting with a minimum dose of 0.8 g/kg of body weight up to 1.3–1.5 g/kg in situations of stress, severe frailty, or inflammation. With this practice, time spent in bed was reduced, and a better quality of life at 3 months was observed.47 The choice of the source of these proteins is also essential, as certain precautions must be taken into account with nutritional support, where protein-based supplements of vegetable origin are safer due to their lower bioavailability of phosphate in people with pathologies such as chronic renal failure, which is common in old age.48
Referring to the last two interventions mentioned, the combination of nutritional supplements and rehabilitation has significantly reduced mortality in the postoperative management of patients with hip fractures (RR 0.61, 95% CI 0.39, 0.93; I2=0%).49
Another important item to consider and one of the most observed practices concerning nutritional deficit is prolonged pre-surgical fasting, which can often be extended up to 14 hours or more. Anesthesiologists typically recommend approximately 6 to 8 hours of fasting for solid foods, generating difficulties in metabolic control and hydration.50,51
Thromboprophylaxis
As previously mentioned, thromboembolic complications are frequent, which is why from the moment of admission to care, early initiation of thromboprophylaxis is recommended to avoid these complications among patients that cannot be taken to surgery in the first 12 hours.12
Similarly, pharmacological thromboprophylaxis with low molecular weight heparin or fondaparinux is recommended to prevent thromboembolic episodes for 10 to 35 days after the operation.52 Currently, some meta-analyses demonstrate equivalence for using direct oral anticoagulants compared with the usual pharmacological thromboprophylaxis without difference in effectiveness.53,54
Follow-Up
Patients who experience a hip fracture are also at high risk of a second fracture after discharge. One in three patients who suffer a hip fracture could suffer another in the following 12 months, and more than 50% of patients will suffer another within 5 years,12 so follow-up is essential in these patients.
It is recommended that after osteosynthesis of hip fracture, patients have a follow-up within two weeks after discharge. During this time, they may present complications related to their medication and other adverse clinical events.55 This represents a barrier to the proper management of these patients. For example, it is estimated that less than 20% of patients who survive the fracture are evaluated and intervened to prevent falls after a hip fracture.56 The risk factors for falls to be considered in older persons include different aspects evaluated in the comprehensive geriatric assessment, such as cognitive impairment, use of psychoactive medication such as sedatives, poor performance in gait and balance tests, visual or hearing changes, non-use, or incorrect use of support devices.37,57
Strategies for fall prevention in the outpatient setting include avoiding rugs or other obstructions, increasing physical activity with resistance exercises to improve muscle performance, caution with medications that increase the risk of falls, providing mobility aids and hip protectors, assessing fear of falling using scales such as the Falls Efficacy Scale-International (FES-I)58 and ensuring fall prevention education for health care providers and staff,12 the latter in relation to the fact that they must have consistent and clear information to avoid errors.59
As can be seen, there are alterations in follow-up and outpatient care after a fracture which are associated with a lack of an available team, lack of communication with the patient and family, and low levels of knowledge of the care team, which have been associated with the presence of adverse clinical outcomes.6
Regarding the availability of multidisciplinary teams, some authors have considered that variables such as pain, nutrition, pressure ulcers, delirium, constipation, and infection in older patients after a fracture could be identified and managed early in the outpatient setting by the nursing service or home care. This demonstrates that interdisciplinary management among health agents is crucial.6 The availability of human resources that can carry out identification and follow-up tasks at the intra- and extra-hospital level should be emphasized, specifically physiotherapists, occupational therapists, nurses, geriatricians, physical and rehabilitation physicians, and personal support workers, in order to improve clinical results.59 When available, Fracture Liaison Services are vital for the early identification, prevention, and management of osteoporosis-related fractures. By taking a comprehensive and multidisciplinary approach, FLS contributes to improved patient outcomes, reduced healthcare costs, and a positive impact on public health.60
As mentioned, it is important to consider the value of preventing osteoporosis and falls from youth to reduce the impact and improve health outcomes after a fragility fracture. Proper nutrition, achieving and maintaining peak bone and muscle mass, and achieving healthy aging should be a goal for health systems. For this reason, educating the population and medical care groups is essential. Recognizing the importance of identifying people at risk is another crucial pillar in the prevention of fractures during the geriatric assessment: finding warning signs such as neurosensory deprivation, the onset of comorbidities that affect gait or balance, having two or more falls in a year or presenting osteosarcopenia should direct attention to early and comprehensive intervention to prevent fractures.
Once a patient suffers a fracture, the patient, their relatives and the health service need to be aware of the possible functional and psychological consequences that this condition involves in order to plan optimal and prompt management and thus improve the related functional and vital outcomes. Education regarding treatment for primary and specialized care physicians is important to guarantee the education of patients and their families on the requirement of medication for secondary prevention and adherence to it. The availability of resources in the health system to offer treatments can help guarantee patient adherence and reduce the risk of a new fracture. Monitoring patients after the start of management can improve the proper use of medication, thus achieving the desired results.
Table 1 summarizes the barriers that can be found in the identification, investigation, and initiation of treatment for osteoporosis in the event of a fracture, as well as possible solutions.
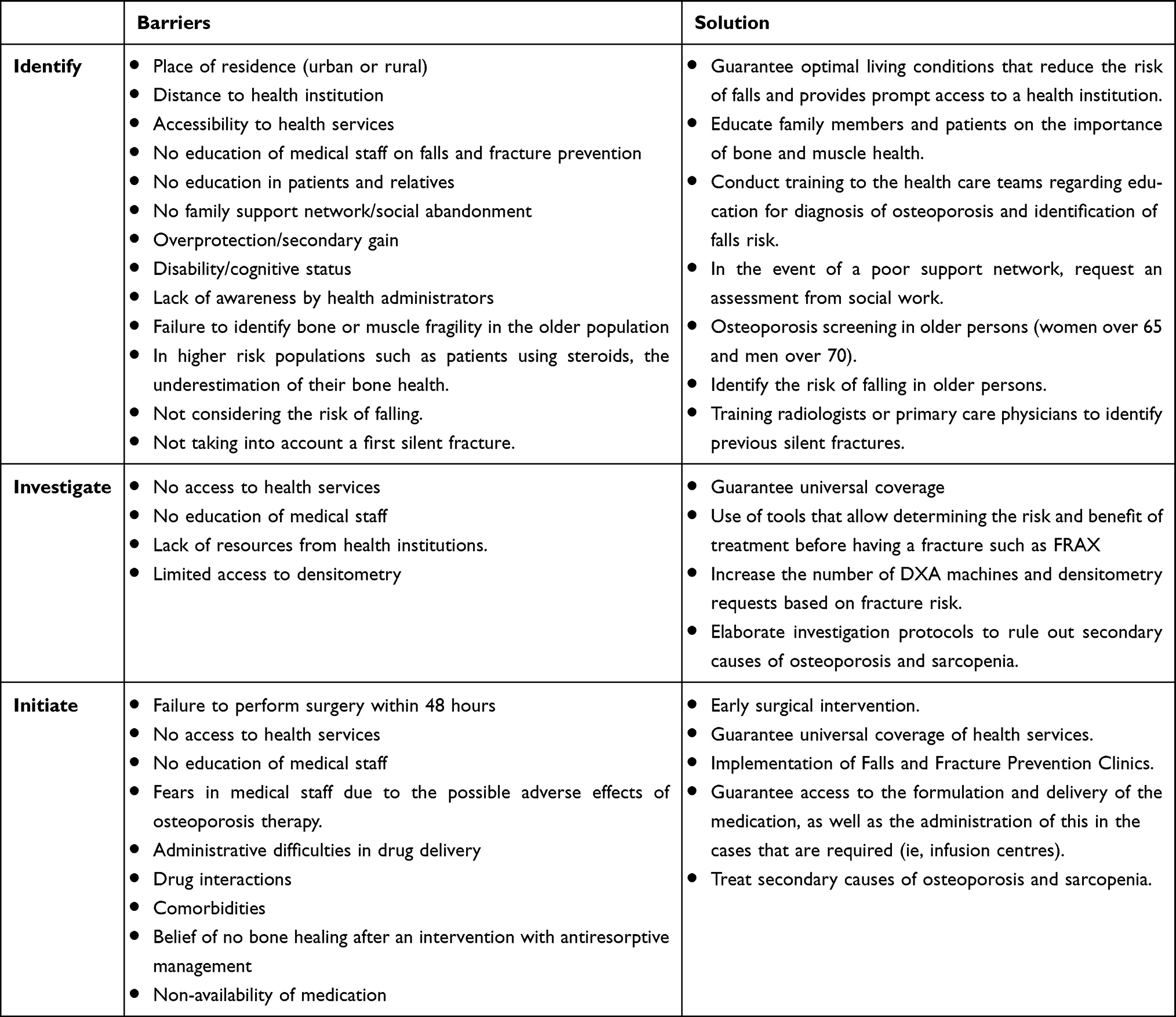 |
Table 1 Barriers in the Identification, Investigation, and Initiation of Treatment for Osteoporosis in the Event of a Fracture, as Well as Possible Solutions |
Conclusions
There are multiple challenges in the care of patients with fragility fractures, especially among older persons, which have a significant impact on complex outcomes such as mortality, functional status and independence. These, once identified, offer multiple opportunities for improvement in care that we could optimize to have better results for our patients. Addressing these challenges requires a multidisciplinary approach, involving orthopedic surgeons, geriatricians, physiotherapists, occupational therapists, dieticians, social workers, and caregivers. Preventive measures, such as fall prevention strategies and osteoporosis management, can also play a vital role in reducing the incidence of fragility fractures in older persons.
Funding
No funding was received.
Disclosure
Gustavo Duque has received honoraria and research grants from TSI Pharmaceuticals and Amgen Australia. The other authors do not have any competing interests to declare.
References
1. Amarilla-Donoso FJ, Lopez-Espuela F, Roncero-Martin R., et al. Quality of life in elderly people after a hip fracture: a prospective study. Health Qual Life Outcomes. 2020;18(1):71. doi:10.1186/s12955-020-01314-2
2. Chami G, Jeys L, Freudmann M, Connor L, Siddiqi M. Are osteoporotic fractures being adequately investigated? A questionnaire of GP & orthopaedic surgeons. BMC Fam Pract. 2006;7(1):7. doi:10.1186/1471-2296-7-7
3. Moon A, Gray A, Deehan D. Neck of femur fractures in patient’s aged more than 85 years-are they a unique subset? Geriatr Orthop Surg Rehabil. 2011;2(4):123–127. doi:10.1177/2151458511414562
4. Lord SR, Menz HB, Tiedemann A. A physiological profile approach to falls risk assessment and prevention. Phys Ther. 2003;83(3):237–252. doi:10.1093/ptj/83.3.237
5. Carty CP, Cronin NJ, Nicholson D, et al. Reactive stepping behaviour in response to forward loss of balance predicts future falls in community-dwelling older adults. Age Ageing. 2015;44(1):109–115. doi:10.1093/ageing/afu054
6. Fitzgerald A, Verrall C, Henderson J, Willis E. Factors influencing missed nursing care for older people following fragility hip fracture. Collegian. 2020;27(4):450–458. doi:10.1016/j.colegn.2019.12.003
7. Clark D, Nakamura M, Miclau T, Marcucio R. Effects of aging on fracture healing. Curr Osteoporos Rep. 2017;15(6):601–608. doi:10.1007/s11914-017-0413-9
8. Lu C, Miclau T, Hu D, et al. Cellular basis for age-related changes in fracture repair. J Orthop Res. 2005;23(6):1300–1307. doi:10.1016/j.orthres.2005.04.003.1100230610
9. Tang VL, Sudore R, Cenzer IS, et al. Rates of recovery to pre-fracture function in older persons with hip fracture: an observational study. J Gen Intern Med. 2017;32(2):153–158. doi:10.1007/s11606-016-3848-2
10. Roche JJ, Wenn RT, Sahota O, Moran CG. Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study. BMJ. 2005;331(7529):1374. doi:10.1136/bmj.38643.663843.55
11. Haentjens P. Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(Suppl 6):380–390. doi:10.1059/0003-4819-152-6-201003160-00008
12. Khan AA, AbuAlrob H, Al-Alwani H, et al. Post Hip fracture orthogeriatric care-a Canadian position paper addressing challenges in care and strategies to meet quality indicators. Osteoporos Int. 2023;34(6):1011–1035. doi:10.1007/s00198-022-06640-3
13. Larsson G, Holgers KM. Fast-track care for patients with suspected hip fracture. Injury. 2011;42(11):1257–1261. doi:10.1016/j.injury.2011.01.001
14. Blue Book on fragility fracture care. The care of patients with fragility fracture; 2007.
15. Zhang J, Yang M, Zhang X, et al. The effectiveness of a co-management care model on older hip fracture patients in China - A multicentre non-randomised controlled study. Lancet Reg Health West Pac. 2022;19:100348. doi:10.1016/j.lanwpc.2021.100348
16. Schermann H, Gurel R, Gold A, et al. Safety of urgent hip fracture surgery protocol under influence of direct oral anticoagulation medications. Injury. 2019;50(2):398–402. doi:10.1016/j.injury.2018.10.033
17. Frenkel Rutenberg T, Vitenberg M, Haviv B, Velkes S. Timing of physiotherapy following fragility hip fracture: delays cost lives. Arch Orthop Trauma Surg. 2018;138(11):1519–1524. doi:10.1007/s00402-018-3010-1
18. Moja L, Piatti A, Pecoraro V, et al. Timing matters in hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175. doi:10.1371/journal.pone.0046175
19. You D, Skeith L, Korley R, et al. Identification of hypercoagulability with thrombelastography in patients with hip fracture receiving thromboprophylaxis. Can J Surg. 2021;64(3):E324–E329. doi:10.1503/cjs.021019
20. Forni S, Pieralli F, Sergi A, Lorini C, Bonaccorsi G, Vannucci A. Mortality after hip fracture in the elderly: the role of a multidisciplinary approach and time to surgery in a retrospective observational study on 23,973 patients. Arch Gerontol Geriatr. 2016;66:13–17. doi:10.1016/j.archger.2016.04.014
21. Flikweert ER, Izaks GJ, Knobben BAS, Stevens M, Wendt K. The development of a comprehensive multidisciplinary care pathway for patients with a hip fracture: design and results of a clinical trial. BMC Musculoskelet Disord. 2014;15(188). doi:10.1186/1471-2474-15-188
22. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma. 2014;28(3):e49–55. doi:10.1097/BOT.0b013e3182a5a045
23. Nyholm AM, Gromov K, Palm H, Brix M, Kallemose T, Troelsen A. Time to surgery is associated with thirty-day and ninety-day mortality after proximal femoral fracture: a retrospective observational study on prospectively collected data from the Danish fracture database collaborators. J Bone Joint Surg Am. 2015;97(16):1333–1339. doi:10.2106/JBJS.O.00029
24. Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ. 2010;182(15):1609–1616. doi:10.1503/cmaj.092220
25. Kua J, Ramason R, Rajamoney G, Chong MS. Which frailty measure is a good predictor of early post-operative complications in elderly hip fracture patients? Arch Orthop Trauma Surg. 2016;136(5):639–647. doi:10.1007/s00402-016-2435-7
26. Mosk CA, Mus M, Vroemen JP, et al. Dementia and delirium, the outcomes in elderly hip fracture patients. Clin Interv Aging. 2017;12:421–430. doi:10.2147/CIA.S115945
27. Kat MG, de Jonghe JF, Vreeswijk R, et al. Mortality associated with delirium after hip-surgery: a 2-year follow-up study. Age Ageing. 2011;40(3):312–318. doi:10.1093/ageing/afr014
28. Waszynski CM. The Confusion Assessment Method (CAM). Geriatr Nurs. 2007; 12:1.
29. Baumgarten M, Margolis DJ, O DL. Pressure ulcers in elderly hip fracture patients across the continuum of care. J Am Geriatr Soc. 2009;57(5):863–870. doi:10.1111/j.1532-5415.2009.02245.x
30. Barrois B, Labalette C, Rousseau P. A national prevalence study of pressure ulcers in French hospital inpatients. J Wound Care. 2008; 16(17): 378–379.
31. Huang C, Ma Y, Wang C, et al. Predictive validity of the Braden scale for pressure injury risk assessment in adults: a systematic review and meta-analysis. Nurs Open. 2021;8(5):2194–2207. doi:10.1002/nop2.792
32. Balasubramanian A, Zhang J, Chen L, et al. Risk of subsequent fracture after prior fracture among older women. Osteoporos Int. 2019;30(1):79–92. doi:10.1007/s00198-018-4732-1
33. Alarcon T, Gonzalez-Montalvo JI, Gotor P, Madero R, Otero A. Activities of daily living after hip fracture: profile and rate of recovery during 2 years of follow-up. Osteoporos Int. 2011;22(5):1609–1613. doi:10.1007/s00198-010-1314-2
34. Peeters CM, Visser E, Van de Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after hip fracture in the elderly: a systematic literature review. Injury. 2016;47(7):1369–1382. doi:10.1016/j.injury.2016.04.018
35. Pollock FH, Bethea A, Samanta D, Modak A, Maurer JP, Chumbe JT. Readmission within 30 days of discharge after hip fracture care. Orthopedics. 2015;38(1):e7–13. doi:10.3928/01477447-20150105-53
36. Johnell O, Kanis JA, Oden A, et al. Mortality after osteoporotic fractures. Osteoporos Int. 2004;15(1):38–42. doi:10.1007/s00198-003-1490-4
37. Montero-Odasso M, van der Velde N, Martin FC, et al. Task force on global guidelines for falls in older adults. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. 2022;51(9):afac205.
38. Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–58. doi:10.1210/jc.2010-2704
39. Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the women’s health Initiative limited access dataset and meta-analysis. BMJ. 2011;342:d2040. doi:10.1136/bmj.d2040
40. Jackson RD, L AZ, Gass M. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354(7):669–683. doi:10.1056/NEJMoa055218
41. Bischof-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T, Dawson-Hughes B. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. JAMA. 2005;293(18):2257–2264. doi:10.1001/jama.293.18.2257
42. Murphy MC, Brooks CN, New SA, Lumbers ML. The use of the Mini-Nutritional Assessment (MNA) tool in elderly orthopaedic patients. Eur J Clin Nutr. 2000;54(7):555–562. doi:10.1038/sj.ejcn.1601055
43. Stratton RJ, King CL, Stroud MA, Jackson AA, Elia M. ‘Malnutrition universal screening tool’ predicts mortality and length of hospital stay in acutely ill elderly. Br J Nutr. 2006;95(2):325–330. doi:10.1079/bjn20051622
44. Lim SL, Ong KC, Chan YH, Loke WC, Ferguson M, Daniels L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin Nutr. 2012;31(3):345–350. doi:10.1016/j.clnu.2011.11.001
45. Koren-Hakim T, Weiss A, Hershkovitz A, et al. Comparing the adequacy of the MNA-SF, NRS-2002 and MUST nutritional tools in assessing malnutrition in hip fracture operated elderly patients. Clin Nutr. 2016;35(5):1053–1058. doi:10.1016/j.clnu.2015.07.014
46. Wong AM, Xu BY, Low LL, Allen JC Jr, Low SG. Impact of malnutrition in surgically repaired hip fracture patients admitted for rehabilitation in a community hospital: a cohort prospective study. Clin Nutr ESPEN. 2021;44:188–193. doi:10.1016/j.clnesp.2021.06.024
47. Shi H, Lu JH, Wang SN, Na Q, Xu LF, Hong JA. Effect of early enteral nutrition in elderly patients with hip fracture during the perioperative period. J Back Musculoskelet Rehabil. 2020;33(1):109–117. doi:10.3233/BMR-181191
48. Scialla JJ, Appel LJ, Wolf M, et al. Plant protein intake is associated with fibroblast growth factor 23 and serum bicarbonate levels in patients with chronic kidney disease: the chronic renal insufficiency cohort study. J Ren Nutr. 2012;22(4):379–388 e1. doi:10.1053/j.jrn.2012.01.026
49. Takahashi K, Momosaki R, Yasufuku Y, Nakamura N, Maeda K. Nutritional therapy in older patients with hip fractures undergoing rehabilitation: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21(9):1364–1364 e6. doi:10.1016/j.jamda.2020.07.005
50. Smith I, Kranke P, Murat I, et al. Perioperative fasting in adults and children: guidelines from the European society of anaesthesiology. Eur J Anaesthesiol. 2011;28(8):556–569. doi:10.1097/EJA.0b013e3283495ba1
51. Force AT. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American society of anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. 2017; 126(3):376–393. doi:10.1097/ALN.0000000000001452
52. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e278S–e325S. doi:10.1378/chest.11-2404
53. Waever D, Lewis D, Sakso H, Borris LC, Tarrant S, Thorninger R. The effectiveness and safety of direct oral anticoagulants following lower limb fracture surgery: a systematic review and meta-analysis. J Orthop Trauma. 2021;35(4):217–224. doi:10.1097/BOT.0000000000001962
54. Nederpelt CJ, Bijman Q, Krijnen P, Schipper IB. Equivalence of DOACS and LMWH for thromboprophylaxis after Hip fracture surgery: systematic review and meta-analysis. Injury. 2022;53(3):1169–1176. doi:10.1016/j.injury.2021.11.052
55. Services AH optimizing the post-acute continuum of care following a hip fracture; 2019.
56. Kanis JA, Svedbom A, Harvey N, McCloskey EV. The osteoporosis treatment gap. J Bone Miner Res. 2014;29(9):1926–1928. doi:10.1002/jbmr.2301
57. Li Y, Hou L, Zhao H, Xie R, Yi Y, Ding X. Risk factors for falls among community-dwelling older adults: a systematic review and meta-analysis. Front Med Lausanne. 2022;9:1019094. doi:10.3389/fmed.2022.1019094
58. Dewan N, MacDermid JC. Fall Efficacy Scale-International (FES-I). J Physiother. 2014;60(1):60. doi:10.1016/j.jphys.2013.12.014
59. Cadel L, Kuluski K, Everall AC, Guilcher SJT. Recommendations made by patients, caregivers, providers, and decision-makers to improve transitions in care for older adults with hip fracture: a qualitative study in Ontario, Canada. BMC Geriatr. 2022;22(1):291. doi:10.1186/s12877-022-02943-6
60. Paccou J, Philippoteaux C, Cortet B, Fardellone P. Effectiveness of fracture liaison services in osteoporosis. Joint Bone Spine. 2023;90(5):105574. doi:10.1016/j.jbspin.2023.105574
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.