")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 15
Chemical versus Mechanical and Chemical Venous Thromboembolism Prophylaxis in Neurocritically Ill Patients: A Cohort Study
Authors Alshaya AI , Alyahya H, Alzoman R, Faden R , Alshaya OA , Al Sulaiman K , Alanazi F, Aldekhyl S
Received 6 September 2022
Accepted for publication 24 December 2022
Published 7 January 2023 Volume 2023:15 Pages 1—8
DOI https://doi.org/10.2147/CPAA.S388950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Abdulrahman I Alshaya,1– 3 Hayaa Alyahya,1 Reema Alzoman,1 Rawa Faden,1 Omar A Alshaya,1– 3 Khalid Al Sulaiman,1– 4 Faisal Alanazi,1– 3 Sara Aldekhyl2,3,5
1College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Saudi Critical Care Pharmacy Research (SCAPE) Platform, Riyadh, Saudi Arabia; 5College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Correspondence: Abdulrahman I Alshaya, Clinical Affairs, College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, P.O. Box 3660, Riyadh, 11481, Saudi Arabia, Tel +966 11-429-9999, Fax +966 11-849-5085, Email [email protected]
Purpose: Patients admitted with neurocritical illness are presumed to be at high risk for venous thromboembolism (VTE). The administration of chemical and/or mechanical VTE prophylaxis is a common practice in critically ill patients. Recent data did not show a significant difference in the incidence of VTE between chemical compared to a combined chemical and mechanical VTE prophylaxis in critically ill patients with limited data in neurocritically ill population. The objective of this study is to investigate the incidence of VTE between chemical alone compared to chemical and mechanical VTE prophylaxis in neurocritically ill patients.
Patients and Methods: This was a retrospective cohort study at a tertiary teaching hospital. Data were obtained from electronic medical records for all patients admitted with neurocritical illness from January 1, 2016, to December 31, 2020. Patients were excluded if they did not receive VTE prophylaxis during admission or were younger than 18 YO. Major outcomes were symptomatic VTE based on clinical and radiological findings, intensive care unit (ICU) length of stay (LOS), and hospital LOS. Minor outcomes included severe or life-threatening bleeding based on GUSTO criteria, and mortality at 28-days.
Results: Two hundred and twelve patients were included in this study. Patients did not have any significant differences in their baseline characteristics. The incidence of VTE was similar in the chemical only group compared to the combined VTE prophylaxis group (19/166 (11.3%) vs 7/46 (15.2%)); P = 0.49. No difference between groups in their ICU LOS 6 [3– 16.2] vs 6.5 [3– 19]; P = 0.52, nor their mortality (18/166 (10.7%) vs 3/46 (6.5%)); P = 0.38, respectively. Less bleeding events were seen in the chemical prophylaxis group compared to the combined VTE prophylaxis group (19/166 (11.3%) vs 12/46 (26.1%); P = 0.01).
Conclusion: Our findings observed no difference between the administration of chemical VTE prophylaxis alone compared to the combined VTE prophylaxis strategy. More data are needed to confirm this finding with more robust methodology.
Keywords: deep vein thrombosis, ICU, neurocritical care, anticoagulation
Introduction
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are two clinical manifestations of venous thromboembolism (VTE), which is common morbidity among patients with critical neurological illness.1,2 The rates of VTEs among different groups of neurological patients are reported to be between 1.2% and 31.6%.3–7 It continues to occur despite the prevalent use of both mechanical and chemical thromboprophylaxis.8 In a study conducted by Reiff et al, in patients with traumatic brain injury (TBI), the risk of DVT had a 3–4-fold increase, even with the use of mechanical and chemical prophylaxis.9 The rates of VTE are estimated to be higher in neurocritically ill patients than those in non-neurocritically ill patients due to prolonged coma and paralysis.2
Prevention of VTEs among hospitalized patients is necessary to reduce morbidity and mortality, which may eventually decrease healthcare cost and improve patients’ functional outcomes.10 Prospective studies reported that the current strategies for prophylaxis significantly reduced the risk of VTE when compared to not undergoing prophylaxis in critically ill patients.2–11 Currently, mechanical, and chemical prophylactic strategies, either combined or not, are considered the standard of care to prevent VTEs among all hospitalized patients.2–11 Guidelines for VTE prophylaxis recommend using chemical prophylaxis over using mechanical prophylaxis strategies. The clinical practice guidelines for neurocritically ill patients generally recommend chemical VTE prophylaxis to be initiated within a range of 1–3 days from admission based on the patient diagnosis, if there are no contraindications. Most guidelines recommend using chemical and mechanical combination strategy compared to using chemical prophylaxis alone to reduce the risk of VTEs.2–14 The foundation of brain trauma in 2016 stated that evidence of level I and II is lacking; however, UFH or LMWH can be prescribed in addition to non-pharmacologic methods to prevent DVT as a level III recommendation. This comes at a cost of expanding intracranial hemorrhage. They also emphasized that only when the brain trauma is stable, pharmacologic prophylaxis can be utilized if the benefit outweighs the risk.15 This study aimed to investigate the incidence of VTEs associated with the use of chemicals alone compared to a combination of chemical and mechanical prophylaxis of VTE in neurocritically ill patientsas a vulnerable population.
Materials and Methods
This is a retrospective cohort study conducted at King Abdulaziz Medical City, National Guard Health Affairs, a tertiary referral teaching hospital with dedicated neurocritical care unit in Riyadh, Saudi Arabia. Data were obtained from electronic medical records (BESTCare) for all patients admitted with neurocritical illness who were prescribed any chemical and/or any mechanical VTE prophylaxis for any of the following indications: ischemic stroke, spontaneous ICH, aSAH, TBI, and others, such as status epilepticus, severe meningitis/encephalitis, brain tumors resections, myasthenia gravis crisis, and severe diabetes insipidus, for at least 24 h from January 1, 2016 to December 31, 2020. King Abdullah International Medical Research Center (KAIMRC) institutional review board (IRB) approved this study with IRB ethical approval number (SP20/446/R), and waived the requirement for the informed consent form based on the retrospective nature of this study design. Patients were excluded if they did not receive any type of VTE prophylaxis during their admission or when they were < 18 years old. Patients who were diagnosed with VTE upon admission, within 24 h of admission, or received full anticoagulation within 24 h of admission were also excluded. After the primary screening, 791 patients were included in the study period. We limited our data collection to only the first 249 patients according to their sequential medical record number from the extracted list by KAIMRC to reduce selection bias and due to logistical issues pertaining data collection.
We screened for patients who were prescribed chemical VTE prophylaxis, including UFH or enoxaparin, during their ICU stay; however, only patients who received UFH or enoxaparin were included in the analysis. Additionally, we screened all patients for using mechanical VTE prophylaxis, including IPC and GCS. Data were stratified based on VTE prophylaxis modality to combined VTE prophylaxis group, defined as using any chemical in addition to concomitant administration of any mechanical VTE prophylaxis strategy and chemical prophylaxis only group. Patients’ demographic data included age, gender, body mass index (BMI), serum creatinine (umol/L) upon ICU admission, creatinine clearance (CrCl) based on the Cockcroft–Gault equation upon ICU admission, history of chronic kidney disease (CKD), and solid/hematological cancer based on laboratory values and chart documentation. The team collected all relevant chemical VTE prophylaxis information, including agent, dose, frequency, time from admission to chemical prophylaxis medication order entry, switch between chemical agents, and interruption of VTE prophylaxis for >5 days. Data for patients who were switched to full anticoagulation and concomitant use of antiplatelet during hospitalization were also collected. Patients were stratified based on the International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) VTE risk score into moderate to high-risk group (score of ≥2) or low-risk group (less than 2 out of 8). Major outcomes included symptomatic VTE based on clinical documentation and radiological findings (ultrasound findings or computed tomography when needed), ICU length of stay (LOS), and hospital LOS. Minor outcomes included severe or life-threatening bleeding based on the GUSTO criteria, and mortality at 28-days from admission date. Sample size calculations were not performed prior to conducting this study. Continuous data were analyzed using Student’s t-test or Mann–Whitney U-test. Chi-square and Fisher’s exact tests were used to compare categorical data as appropriate. Binomial logistic regression was performed using STATA®. Statistical significance was set at p ≤ 0.05. All methods were performed in accordance with the relevant guidelines and regulations at our institution.
Results
After obtaining the data for 249 patients, we included 212 patients in the comparison analysis. Thirty-seven patients were excluded because they did not receive any chemical prophylaxis at any point during admission. No significant differences were observed in our baseline characteristics, as shown in Table 1.
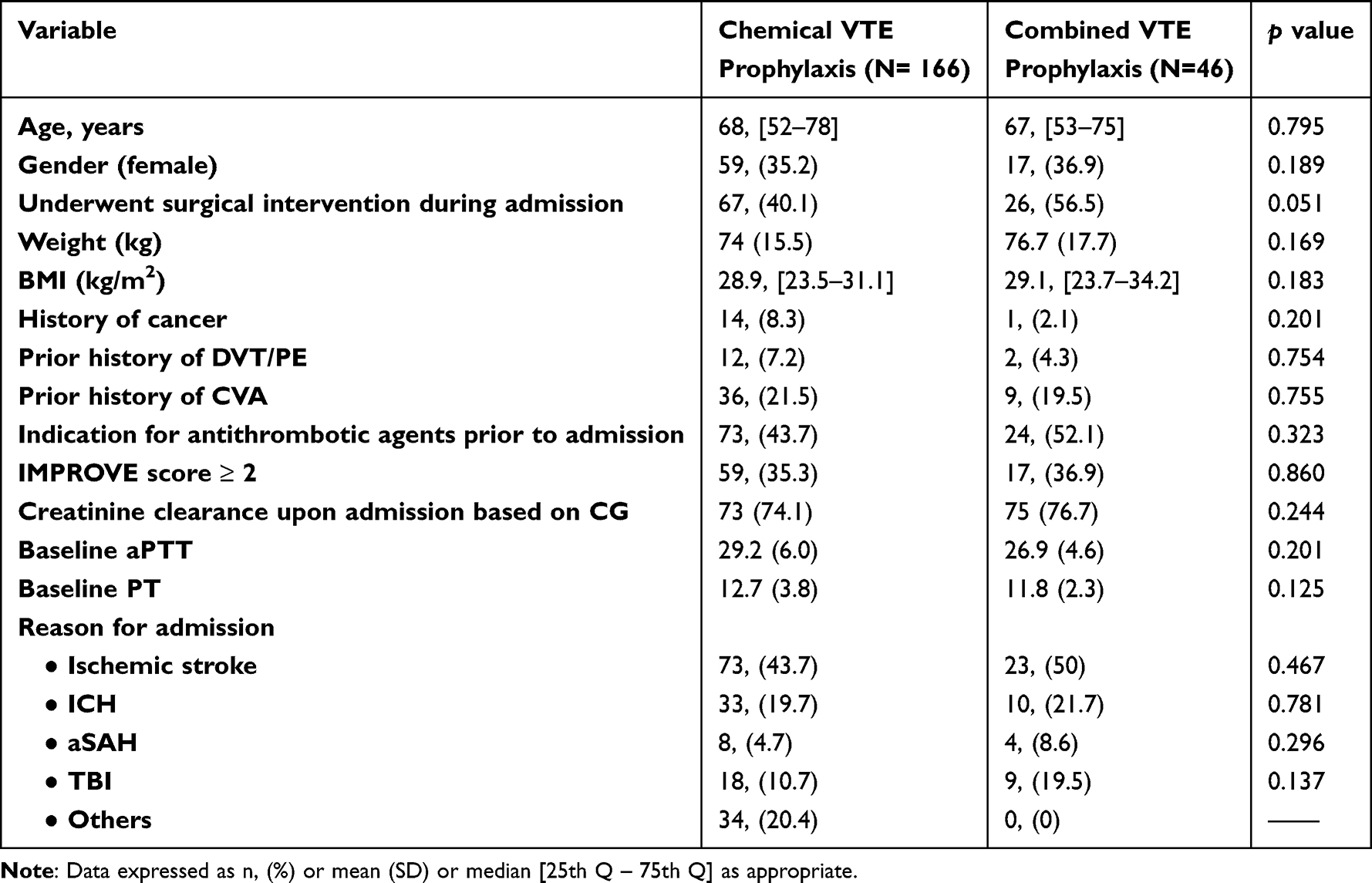 |
Table 1 Baseline Characteristics |
Of the included patients, there was a shorter time to initiate chemical VTE prophylaxis in the chemical VTE prophylaxis compared to the combined VTE prophylaxis, which was statistically significant (1 [1–3] vs 4 [2–5.2]; p < 0.001). We observed a higher percentage of UFH administration as a preferred chemical VTE prophylaxis for both groups as compared to enoxaparin. In-hospital concomitant use of antiplatelets and transition to full anticoagulation were similar between groups, as shown in Table 2. No statistical difference was found in patients who switched between chemical types (from UFH to enoxaparin and vice versa) between groups. Additional data regarding the VTE prophylaxis regimen are shown in Table 2.
 |
Table 2 VTE Prophylaxis Regimen Characteristics |
No major difference was found in our major outcomes between groups, as shown in Table 3. However, more severe or life-threatening bleeding was seen in the combination regimen group 19/166 (11.2%) vs 12/46 (26.1%)); p < 0.013. A binomial regression analysis was used to identify predictors for post-DVT prophylaxis VTE events in the overall cohort. Amongst the examined factors, previous administration of antithrombotic agents (antiplatelet or anticoagulant), DVT prophylaxis interruption and ICU stay for >7 days were found to be strong predictors. All other factors were not statistically significant as shown in Table 4.
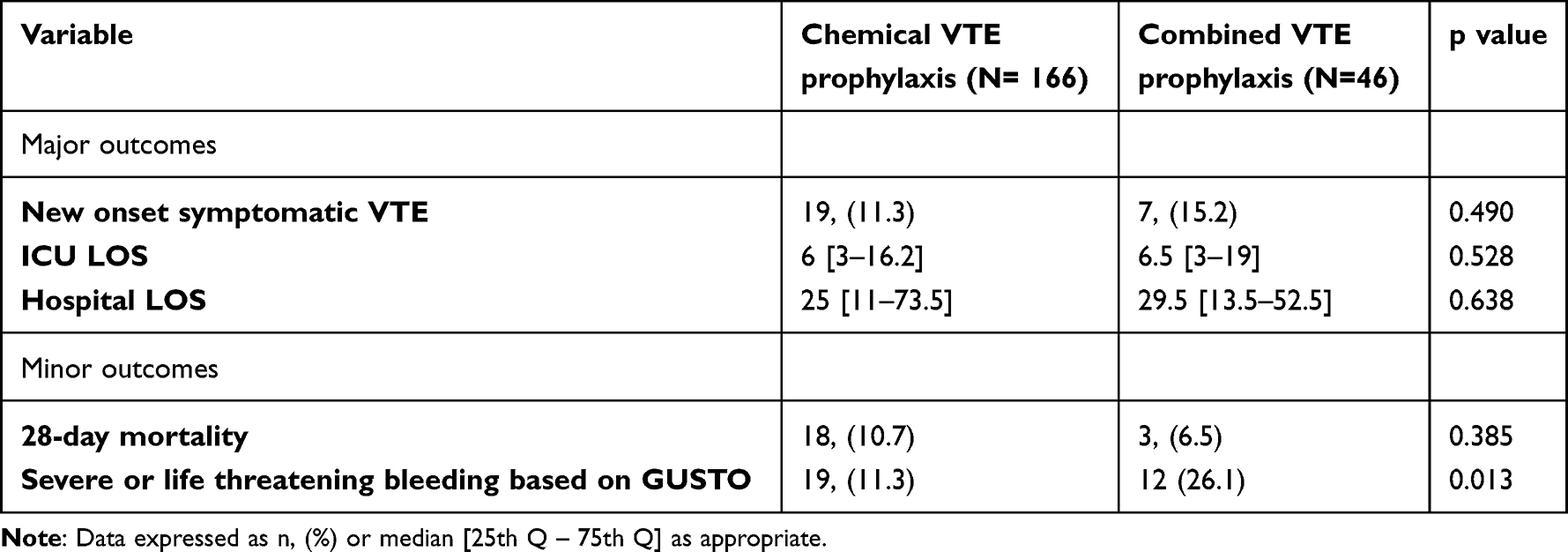 |
Table 3 Study Outcomes |
 |
Table 4 Predictors for VTE After Initiating Prophylaxis VTE Regimens (N = 249) |
Discussion
This retrospective study investigated the role of different VTE prophylaxis modalities on the incidence of symptomatic VTE in neurocritical ill patients and the associated incidence of major bleedings. We observed no difference in the incidence of VTE between the administration of chemical prophylaxis versus the combination of chemical and mechanical prophylaxis. However, the use of chemical only prophylaxis resulted in a significantly lower risk of major bleedings. All other clinical outcomes of interest were not different between VTE prophylaxis strategies, such as ICU LOS, hospital LOS, and 28-day mortality.
There was no difference in baseline characteristics in terms of the type of VTE prophylaxis in admitted patients with ischemic stroke in all groups. Patients admitted with ischemic stroke accounted for the majority of included patients in both groups. Current guidelines recommend using chemical prophylaxis as soon as possible in acute ischemic stroke patients, except in patients with restricted mobility as the use of LMWH plus IPC is more preferred, mainly based on CLOTs 3 trial findings.2,16 These results are inconsistent with the results of the CLOTs 3 trial, which showed a 3.6% reduction in VTE with the use of IPC post-stroke.17 A fewer percentage of patients were admitted with the diagnosis of ICH in the chemical prophylaxis group compared to the combination group in our cohort (19.7% vs 21.7%). Given the delicate bleeding status in this population, mechanical prophylaxis over chemical prophylaxis at the time of admission is recommended, except with stable hematomas where chemical prophylaxis could be administered after 48 hours of admission.2 In a large retrospective study, the utilization of chemical prophylaxis for ICH patients was very low, accounting for less than 20% of the total patients and <10% in the first two days of admission.18 The use of UFH was observed in 71.1% of the patients compared to enoxaparin which was used in 27.5%. This low compliance could have been caused by a lack of knowledge or safety concerns. Similarly, patients with an admission diagnosis of aSAH accounted for 4.7% of the chemical prophylaxis group and 8.6% of the combination group in our cohort. IPC is the recommended VTE strategy in this population and should be started immediately upon admission.2 UFH should also be initiated, except for cases of unsecured ruptured aneurysms that require surgery.19 This may be extrapolated for patients undergoing endovascular treatment; however, data on this matter remain unelucidated. In postoperative patients, UFH should be started within 24 h, as per guidelines recommendations. In a retrospective study investigating the timing of DVT in aSAH, the incidence of DVT peaked between day 5–9 of admission with a lower incidence of DVT in the group receiving heparin prophylaxis.19
In patients with hemorrhagic stroke, early anticoagulation is associated with a significant reduction in PE, a non-significant reduction in DVT or death, and a non-significant increase in hematoma size.20 Moreover, patients with TBI represented 10.7% of the chemical prophylaxis group compared to 19.5% of the combination group of the included patients. In this patient population, the use of IPC within 24 h of presentation or 24 h post craniotomy is recommended by the neurocritical society, reserving chemical prophylaxis for patients with TBI and ICH to be used within 24–48 h, or 24 h post craniotomy.2 In contrast, the American College of Chest Physicians (CHEST) guidelines recommend LMWH for major trauma patients unless contraindicated.21 The most recent guideline of the Brain Trauma Foundation does not provide any strong recommendation for the agent choice in terms of VTE prophylaxis, dosing or timing of administration.15 In addition, the recent clinical consensus from the American Association for the Surgery of Trauma (AAST) Critical Care Committee recommends initiating VTE prophylaxis within 24–72 h, depending on the stability of the intracranial and extracranial hemorrhages.22 These recommendations may explain the higher percentage of our patients in the combination therapy as they may have been started on mechanical prophylaxis initially then combined with chemical prophylaxis later. Previous guidelines also emphasized on the superiority of LMWH over UFH with low quality evidence.
In a retrospective cohort study conducted by Sauro et al in Canada, the adherence of current practice guidelines and the effect on clinical outcomes were evaluated in patients admitted to 10 different neurological, medical, and surgical ICUs. Among the neurocritically ill patients, chemical prophylaxis, mechanical prophylaxis, and no prophylaxis was provided to 60.9%, 46.9%, and 12.2%, respectively. Only 56% of the days spent in ICU were adherent to the practice guidelines. In particular, concordance to the guidelines when prescribing pharmacologic prophylaxis was reported in 26.6% of ICU days, whereas it was up to 80% of ICU days in patients eligible for mechanical prophylaxis. The results of this study demonstrate the variations and uncertainty regarding the optimal practices for the prevention of VTE in neurocritically ill patients.23
In this study, we observed an increase in the utilization of UFH compared to enoxaparin despite having normal baseline renal function. This observation is mainly attributed to the pharmacokinetic advantages of UFH over LMWH, especially in patients who underwent neurosurgical interventions during their ICU admission. UFH is a more reasonable option when acute interruption of anticoagulation is needed for emergent surgery or an active bleeding event. Moreover, an anticoagulation reversal can be better controlled with UFH than with enoxaparin.24,25 The incidence of symptomatic VTE post-acute stroke was reported to be 2%–10%, while we observed slightly an increased incidence in our population despite having 65% being categorized as low thrombotic risk based on their IMPROVE scores of <2.2,19 This minimal increase may be a result of the late re-initiation of anticoagulation in patients who had an indication. Our observed data for an increased risk in the combined VTE prophylaxis is puzzling. Possible explanations may include that approximately 50% of our included patients had an indication for an antithrombotic agent prior to admission; however, only 15% were transitioned to full anticoagulation in both groups. Additionally, the concomitant use of antiplatelets was lower than expected in the combined VTE modality group, given the difference in the likelihood of these patients carrying a higher risk of bleeding upon admission. This may be due to the higher numerical percentage of having surgical interventions during ICU admission (40% vs 56%; p = 0.051).
This study has some limitations. First, we randomly selected neurocritically ill patients who were admitted to our institution during the study period. Therefore, we may have missed some patients in our data collection. Second, we have combined all neurocritical injuries in our cohort, which may have limited the application of our findings to a specific neurocritical injury due to heterogeneity. Further studies with a specific focus on one injury may better reflect the impact of different VTE prophylaxis modalities. Third, we did not collect data on thrombolytic use in acute ischemic stroke patients. However, we have very limited patients who present to our institution for the administration of such therapy within the appropriate study period.25 Availability of such data may better explain the increased incidence of bleeding in a group. Fourth, UFH was used more than LMWH in our cohort, which may have contributed to the similar efficacy between the two groups. In the PREVAIL trial, the use of LMWH was associated with a reduction in VTE risk by 43% compared to UFH, showing clear superiority in acute ischemic stroke patients.26 Fifth, we did not adjust for baseline differences during data analysis which may have impacted our results. Finally, we could not differentiate patients with a high or low risk of bleeding, as this would have only been achieved if a better documentation by a clinician existed. However, to the best of our knowledge, there is no proven tool to predict or estimate the risk of bleeding in neurocritically ill patients. More data are needed to validate our findings.
Conclusion
The incidence of VTE was similar among neurocritical ill patients who received chemical and a combination of chemical and mechanical VTE prophylaxis. Less bleeding events were seen in the chemical prophylaxis group compared to the combined VTE prophylaxis group which can be related to a possible increased baseline risk in the combined VTE prophylaxis group. Further studies with a more robust design and targeted investigation of specific neurological injury are warranted to confirm the safety and efficacy of different VTE prophylaxis modalities in neurocritically ill patients as vulnerable population.
Abbreviations
DVT, Deep vein thrombosis; PE, Pulmonary embolism; TE, Venous thromboembolism; TBI, traumatic brain injury; UFH, Unfractionated heparin; LMWH, Low molecular weight heparin; GCS, Gradual compression stockings; IPC, Intermittent pneumatic compression; ICH, Intracranial hemorrhage; SAH, subarachnoid hemorrhage; RCT, randomized clinical trial; CrCl, Creatinine clearance; CKD, Chronic kidney diseases; BMI, Body mass index; IMPROVE score, The International Medical Prevention Registry on Venous Thromboembolism score; ICU, Intensive care unit; LOS, length of stay.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
IRB approval for this study was granted by IRB of KAIMRC with study number (SP20/446/R). The study was conducted in accordance with the World Medical Association Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects (adopted 1964; updated 2013), national ethical regulations, and local institutional guidance of study centers. The IRB committee waived informed consent from the study patients due to the retrospective observational nature of the study.
Acknowledgments
The authors sincerely thank Dr. Muneerah Aliessa for her work on the data analysis and critique of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is unfunded.
Disclosure
The authors declare that they have no competing interest.
References
1. Betthauser K, Pope H, Gowan M, Human T. Practice patterns of venous thromboembolism prophylaxis in underweight, critically ill patients with neurologic injury. Neurocrit Care. 2017;27(1):96–102. doi:10.1007/s12028-016-0373-4
2. Nyquist P, Bautista C, Jichici D, et al. Prophylaxis of venous thrombosis in neurocritical care patients, an evidence-based guideline, a statement for healthcare professionals from the neurocritical care society. Neurocrit Care. 2016;24(1):47–60. doi:10.1007/s12028-015-0221-y
3. Deitelzweig SB, Johnson BH, Lin J, Schulman KL. Prevalence of clinical venous thromboembolism in the USA, current trends and future projections. Am J Hematol. 2011;86(2):217–220. doi:10.1002/ajh.21917
4. Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98(4):756–764. doi:10.1160/TH07-03-0212
5. Douds GL, Hellkamp AS, Olson DM, et al. Venous thromboembolism in the get with the guidelines-stroke acute ischemic stroke population, incidence and patterns of prophylaxis. J Stroke Cerebrovasc Dis. 2014;23(1):123–129. doi:10.1016/j.jstrokecerebrovasdis.2012.10.018
6. Skaf E, Stein PD, Beemath A, Sanchez J, Bustamante MA, Olson RE. Venous thromboembolism in patients with ischemic and hemorrhagic stroke. Am J Cardiol. 2005;96(12):1731–1733. doi:10.1016/j.amjcard.2005.07.097
7. Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism following acute intracerebral hemorrhage. Neurocrit Care. 2009;10(1):28–34. doi:10.1007/s12028-008-9134-3
8. Minet C, Potton L, Bonadona A, et al. Venous thromboembolism in the ICU, main characteristics, diagnosis and thromboprophylaxis. Crit Care. 2015;19(1):287. doi:10.1186/s13054-015-1003-9
9. Reiff DA, Haricharan RN, Bullington NM, Griffin RL, McGwin G, Rue LW. Traumatic brain injury is associated with the development of deep vein thrombosis independent of pharmacological prophylaxis. J Trauma. 2009;66(5):1436–1440. doi:10.1097/TA.0b013e31817fdf1c
10. Amin A, Hussein M, Battleman D, Lin J, Stemkowski S, Merli GJ. Appropriate VTE prophylaxis is associated with lower direct medical costs. Hosp Pract. 2010;38(4):130–137. doi:10.3810/hp.2010.11.350
11. Kahn SR, Lim W, Dunn AS, et al. Prevention of VTE in nonsurgical patients, antithrombotic therapy and prevention of thrombosis, 9th ed, American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2Suppl):e195S–e226S. doi:10.1378/chest.11-2296
12. Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med. 1982;10(7):448–450. doi:10.1097/00003246-198207000-00006
13. Fraisse F, Holzapfel L, Couland JM, et al. Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD. The association of non-university affiliated intensive care specialist physicians of France. Am J Respir Crit Care Med. 2000;161(4 Pt 1):1109–1114. doi:10.1164/ajrccm.161.4.9807025
14. Dennis M, Sandercock P, Graham C, Forbes J. CLOTS (clots in legs or stockings after stroke) trials collaboration, smith j. the clots in legs or stockings after stroke (CLOTS) 3 trial, a randomised controlled trial to determine whether or not intermittent pneumatic compression reduces the risk of post-stroke deep vein thrombosis and to estimate its cost-effectiveness. Health Technol Assess. 2015;19(76):1–90.
15. Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury. Neurosurgery. 2017;80(1):6–15. doi:10.1227/NEU.0000000000001432
16. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke, 2019 update to the 2018 guidelines for the early management of acute ischemic stroke, a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
17. Dennis M, Sandercock P; CLOTS (Clots in Legs Or sTockings after Stroke) Trials Collaboration. Effectiveness of intermittent pneumatic compression in reduction of risk of deep vein thrombosis in patients who have had a stroke (CLOTS 3), a multicentre randomised controlled trial. Lancet. 2013;382(9891):516–524.
18. Prabhakaran S, Herbers P, Khoury J, et al. Is prophylactic anticoagulation for deep venous thrombosis common practice after intracerebral hemorrhage? Stroke. 2015;46(2):369–375. doi:10.1161/STROKEAHA.114.008006
19. Liang CW, Su K, Liu JJ, Dogan A, Hinson HE. Timing of deep vein thrombosis formation after aneurysmal subarachnoid hemorrhage. J Neurosurg. 2015;123(4):891–896. doi:10.3171/2014.12.JNS141288
20. Paciaroni M, Agnelli G, Venti M, Alberti A, Acciarresi M, Caso V. Efficacy and safety of anticoagulants in the prevention of venous thromboembolism in patients with acute cerebral hemorrhage, a meta-analysis of controlled studies. J Thromb Haemost. 2011;9(5):893–898. doi:10.1111/j.1538-7836.2011.04241.x
21. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease, CHEST guideline and expert panel report. Chest. 2016;149(2):315–352. doi:10.1016/j.chest.2015.11.026
22. Rappold JF, Sheppard FR, Carmichael ISP, et al. Venous thromboembolism prophylaxis in the trauma intensive care unit, an American Association for the surgery of trauma critical care committee clinical consensus document. Trauma Surg Acute Care Open. 2021;6(1):e000643. doi:10.1136/tsaco-2020-000643
23. Sauro KM, Soo A, Kramer A, et al. Venous thromboembolism prophylaxis in neurocritical care patients, are current practices, best practices? Neurocrit Care. 2019;30(2):355–363. doi:10.1007/s12028-018-0614-9
24. Liss DB, Mullins ME. Antithrombotic and antiplatelet drug toxicity. Crit Care Clin. 2021;37(3):591–604. doi:10.1016/j.ccc.2021.03.012
25. Al Khathaami AM, Al Bdah B, Tarawneh M, et al. Utilization of intravenous tissue plasminogen activator and reasons for nonuse in acute ischemic stroke in Saudi Arabia. J Stroke Cerebrovasc Dis. 2020;29(5):104761. doi:10.1016/j.jstrokecerebrovasdis.2020.104761
26. Sherman DG, Albers GW, Bladin C, et al. The efficacy and safety of enoxaparin versus unfractionated heparin for the prevention of venous thromboembolism after acute ischaemic stroke (PREVAIL Study), an open-label randomised comparison. Lancet. 2007;369(9570):1347–1355. doi:10.1016/S0140-6736(07)60633-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.