")
Back to Journals » Clinical Interventions in Aging » Volume 18
Clinical and Demographic Characteristics of Centenarians versus Other Age Groups Over 75 Years with Hip Fractures
Authors Bermejo Boixareu C, Ojeda-Thies C, Guijarro Valtueña A, Cedeño Veloz BA , Gonzalo Lázaro M, Navarro Castellanos L, Queipo Matas R, Gómez Campelo P, Royuela Vicente A, González-Montalvo JI, Sáez-López P
Received 17 August 2022
Accepted for publication 19 January 2023
Published 22 March 2023 Volume 2023:18 Pages 441—451
DOI https://doi.org/10.2147/CIA.S386563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Cristina Bermejo Boixareu,1,* Cristina Ojeda-Thies,2,* Ainhoa Guijarro Valtueña,3 Bernardo Abel Cedeño Veloz,4 María Gonzalo Lázaro,4 Laura Navarro Castellanos,5 Rocío Queipo Matas,5,6 Paloma Gómez Campelo,5 Ana Royuela Vicente,7 Juan Ignacio González-Montalvo,5,8 Pilar Sáez-López5,9,10
1Geriatrics Department, Puerta de Hierro Majadahonda University Hospital, Madrid, Spain; 2Orthopaedic Surgery and Traumatology Department, 12 de Octubre University Hospital, Madrid, Spain; 3Orthopaedic Surgery and Traumatology, Puerta de Hierro Majadahonda University Hospital, Madrid, Spain; 4Geriatrics Department, University Hospital of Navarra, Pamplona, Spain; 5La Paz Institute for Health Research - IdiPAZ, Hospital Universitario La Paz - Universidad Autónoma de Madrid, Madrid, Spain; 6European University of Madrid, Madrid, Spain; 7Biostatistics Unit, Puerta de Hierro Majadahonda University Hospital, IDIPHISA, CIBERESP, Madrid, Spain; 8Geriatrics Department, La Paz University Hospital, Madrid, Spain; 9Geriatrics Department, Fundación Alcorcón University Hospital, Madrid, Spain; 10Spanish National Hip Fracture Registry, Madrid, Spain
*These authors contributed equally to this work
Correspondence: Cristina Bermejo Boixareu, Geriatrics Department, Puerta de Hierro University Hospital, Madrid, Spain, Email [email protected]
Objective: The primary objective was to describe the clinical characteristics, management, and outcomes of centenarians with fragility hip fracture and compare them to other age groups. The secondary objective was to determine the variables associated with length of stay, in-hospital mortality and 30-day mortality.
Materials and Methods: This is a secondary analysis of the Spanish National Hip Fracture Registry. We included patients ≥ 75 years admitted for fragility hip fractures in 86 Spanish hospitals between 2017 and 2019, dividing the sample into four age groups. The variables studied were baseline characteristics, type of fracture, management, length of stay, in-hospital mortality and 30-day mortality.
Results: We included 25,938 patients (2888 were 75– 79 years old; 14,762 octogenarians; 8,035 nonagenarians and 253 centenarians). Of the centenarians, 83% were women, 33% had severe dementia, 9% had severe dependency and 36% lived in residential care homes. Six out of ten had intertrochanteric fracture. Length of hospital stay was 8.6 days; in-hospital mortality was 10.3% and 30-day mortality 20.9%. Older age groups had more women, severe functional dependency, severe dementia, intertrochanteric fracture, living in care facilities and being discharged to nursing care. They had less frequent early mobilization, osteoporosis treatment and discharge to rehabilitation units. In-hospital and 30-day mortality were higher with increasing age. In centenarians, time to surgery > 48 hours was independently associated with length of stay (correlation coefficient 3.99 [95% CI: 2.35– 5.64; p< 0.001]) and anaesthetic risk, based on an ASA score of V, was related to 30-day mortality (ASA score II [OR 0.25, 95% CI: 0.09– 0.70; p=0.009] and ASA score III [OR 0.43, 95% CI: 0.19– 0.96; p=0.039]).
Conclusion: Centenarians had different clinical characteristics, management and outcomes. Although centenarians had worse outcomes, nearly 4 out of 5 centenarians were alive one month after surgery.
Keywords: centenarians, fracture, registry, mortality, ASA grade
Introduction
The number of individuals aged 100 years or more is estimated to quadruple by 2033 in Spain. According to the Spanish National Statistics Institute, the number of centenarians will increase from 11,248 in 2018 to 46,366 in 2033. Nevertheless, the literature on centenarian patients is scarce.1
The incidence of hip fractures in centenarians is seven-fold higher than in younger age groups.2 Several studies in Spain and elsewhere have shown that hip fractures are the most common cause of hospital admission in centenarians, ahead of heart failure and pneumonia.3,4
Studies on hip fractures in centenarians are limited in number of patients and show contradictory results.5–24 Differences have been described in relation to the type of fracture,2–8 the relationship between time to surgery and outcomes5 and the risk of complications during hospitalisation.9 Discrepancies have also been published regarding short and long-term outcomes.6–8,11,12 A recent study including more than 4000 centenarians with hip fracture focused exclusively on complications during hospitalization, but did not include outcomes related to mortality or functional status in the first month after the fracture.10
Considering the above, the primary objective of this study was to describe the clinical characteristics, management, and outcomes of centenarians admitted with fragility hip fracture and to compare them with those observed in patients aged 75 to 79, 80 to 89 (octogenarians) and 90 to 99 years old (nonagenarians) using data from the Spanish National Hip Fracture Registry (Registro Nacional de Fracturas de Cadera, RNFC). The secondary objective was to determine the variables associated with length of stay, and both in-hospital and 30-day mortality in older patients including the centenarian group.
Materials and Methods
The RNFC registry is a multicentric, prospective and continuous registry of patients treated for hip fractures in participating hospitals. The RNFC has been approved by the Research Ethics Committees of the participating centres and complies with the Declaration of Helsinki.
The RNFC includes all patients 75 years or older admitted for fragility hip fractures (due to falls from standing height) who have signed an informed consent (signed by the patient or their next of kin) in 86 participating hospitals from Spain between January 2017 and June 2019. Hip fractures occurring as a result of high-energy trauma and fractures in patients with known disseminated cancer are excluded.
The design and organization of the RNFC have been described in greater detail in a previous article.25 Baseline variables were recorded such as age, sex, place of residence, pre-fracture mobility (using Functional Ambulation Categories, FAC), cognitive status (using Pfeiffer’s SPMSQ) and the ASA (American Society of Anaesthesiology) score, as well as whether the patient had received bone protection medication before the fracture. The clinical variables associated with hospital admission were type of fracture, surgical delay, type of surgery performed, type of anaesthesia, use of peripheral nerve blocks, development of pressure ulcers, and whether the patient had been mobilized on the first postoperative day. Variables included at discharge were destination at discharge, length of hospital stay, anti-osteoporotic medication prescribed at discharge and in-hospital mortality. Data at 30 days was collected by contacting the patient or caregivers directly and included readmission, repeat surgery, use of anti-osteoporotic medication, functional status and mortality.
Statistical Analysis
Patients were divided into four age groups: 75–79 years old, 80–89 years old, 90–99 years old and ≥100 years old. These groups were characterized by means of a descriptive analysis for categorical variables using absolute and relative frequencies; numerical variables were characterized using the mean and standard deviation or median and interquartile ranges, according to the normality of the data. The χ2 test was used to compare categorical variables and the Kruskal–Wallis test to compare numerical variables. Linear regression was carried out to study variables related to the length of stay (in days) and logistic regression to assess in-hospital and 30-day mortality. Correlation coefficients and OR with their corresponding 95% confidence intervals are shown, respectively. The differences were considered as statistically significant if the p value was <0.05. The statistical package used was Stata/IC v.15.1. (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Results
Of 25,938 patients included, 253 (1.0%) were centenarians, 2,888 (11.1%) were between 75 and 79 years of age, 14,762 (56.9%) were octogenarians, and 8,035 (31.0%) were nonagenarians.
In the centenarian group, 83.3% were women, 32.8% had severe dementia, 8.8% had severe dependency and 36.0% lived in residential care homes. The most frequent fracture was intertrochanteric (59.6%) and the most common procedure used was cephalomedullary nailing (63.7%). Peripheral nerve blocks were used in 17.1% of patients. Time to surgery ≤48 hours occurred in 52.8% of the centenarians. Six out of ten patients were mobilized the first day after surgery and 12.2% developed pressure ulcers in hospital. The median length of hospital stay was 8.6 days, and in-hospital mortality was 10.3%. At discharge, 14.1% of them received anti-osteoporotic medication, 33.6% calcium and 55.9% vitamin D supplements. Of the patients, 42.3% were transferred to nursing homes and 11.9% to geriatric rehabilitation units. Regarding outcomes at 30 days, 20.9% died, 1.8% were readmitted and 4.9% underwent repeat surgery.
The group of centenarians was compared to the other age groups, showing that the frequency of women (p<0.001), those living in care facilities (p<0.001), and those with severe dementia (p<0.001), severe functional impairment (p<0.001), and intertrochanteric fracture (p<0.001), increased in the older age groups (Table 1 and Table 2). Non pathological fractures in the surgical pieces were diagnosed in centenarian patients (1.6%, 0.7%, 0.5% and 0%, respectively per age group) and three centenarians had atypical fractures (0.5%, 0.5%, 0.5% and 1.2%; p<0.001).
 |
Table 1 Demographic and Baseline Characteristics of the Patients Included for Analysis |
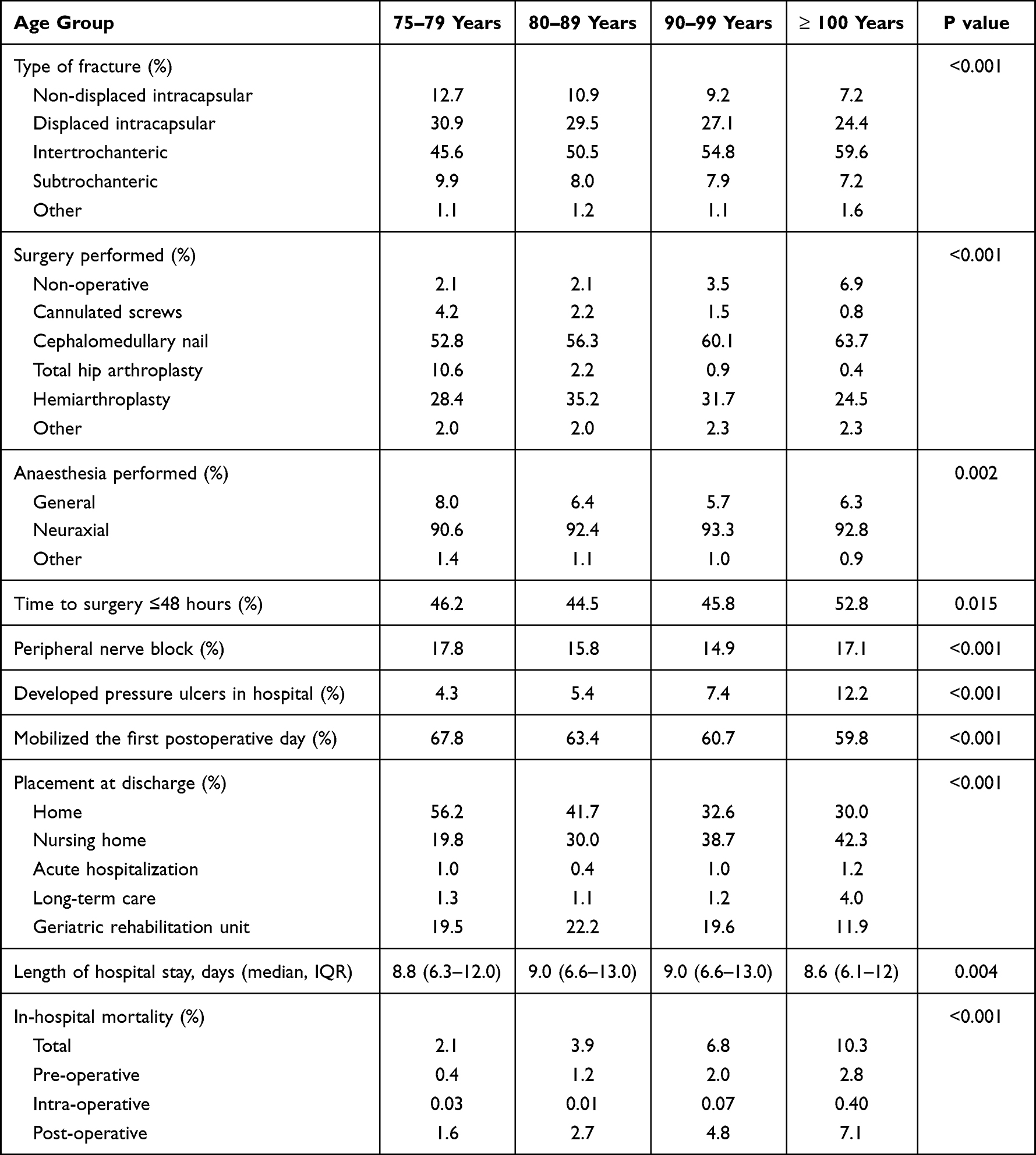 |
Table 2 Fracture and in-Hospital Management Characteristics of the Patients Included for Analysis |
Time to surgery was less than 48 hours in a greater proportion of centenarians than in the younger age groups (p=0.015). The older age groups had lower percentages of mobilization on the first day after surgery (p<0.001) and had higher frequencies of pressure ulcers developed in hospital (p<0.001) (Table 2).
Regarding hospital outcomes, in-hospital mortality was higher as the age of the groups increased (p<0.001) (Table 2). The median length of stay was also shorter among centenarians (8.8 vs 9.0 vs 9.0 vs 8.6 days, respectively per age group; p=0.004). At discharge, a greater proportion of patients in the older age groups were sent to residential care facilities (19.8%, 30.0%, 38.7% and 42.3%). Centenarians were also less likely to be referred to geriatric recovery units (19.5%, 22.1%, 19.6% and 11.7%). Anti-osteoporotic medication, calcium and vitamin D supplements were much less likely to be prescribed in the older age groups (Figure 1A–C). Figure 2 shows functional status at baseline and 30 days after the fracture using Functional Ambulation Categories.
 |
Figure 1 Bone health prescriptions before the fracture, at discharge and at one-month follow-up, by age group. (A) Anti-osteoporotic medication (antiresorptive treatment and bone-forming agents); (B) Calcium supplements; (C) Vitamin D supplements. |
 |
Figure 2 Functional status at baseline and 30 days after the fracture using Functional Ambulation Categories. |
Table 3 shows characteristics at 30 days after hip fracture by age group. Centenarians had a higher risk of 30-day mortality than the other age groups (p<0.001).
 |
Table 3 Characteristics at One-Month Follow-Up After Hip Fracture, by Age Group |
In-Hospital Mortality
Multivariate analysis found that the following variables were associated with in-hospital mortality: female sex (OR 0.58, 95% CI: 0.48–0.70; p<0.001), time to surgery >48 hours (OR 1.30, 95% CI: 1.08–1.55; p=0.005]), baseline ambulatory capacity with FAC 0 as a reference (FAC 2 [OR: 0.59, 95% CI: 0.37–0.92; p=0.022], FAC 3 [OR: 0.59, 95% CI: 0.37–0.95; p=0.032], FAC 4 [OR: 0.49 [95% CI: 0.36–0.67; p<0.001] and FAC 5 [OR: 0.29, 95% CI: 0.21–0.40; p<0.001]), anaesthetic risk with ASA score I as a reference (ASA score IV [OR 9.29, 95% CI: 1.27–68.1; p=0.028] and ASA score V [OR 15.4 [95% CI: 1.27–187]]; p=0.032)), peripheral nerve block (OR 0.67, 95% CI: 0.51–0.87; p=0.003]), neuraxial anaesthesia (OR 0.66, 95% CI: 0.49–0.90; p=0.008]), and age group, taking <80 years as a reference (80–89 years [OR 1.44, 95% CI: 1.00–2.07; p=0.048]; 90–99 years [OR 2.41 [95% CI: 1.67–3.48; p<0.001]]; ≥100 years [OR 4.55, 95% CI: 2.26–9.13; p<0.001]). In centenarians, multivariate analysis showed no association with in-hospital survival for any of these variables.
Factors Related to Length of Stay
Multivariate analysis found that the variables associated with length of stay were time to surgery >48 hours (coefficient: 3.86, 95% CI: 3.59–4.13; p<0.001), baseline ambulatory capacity, taking FAC 0 as reference (FAC 2 [coefficient: 2.01, 95% CI: 1.18–2.84; p<0.001], FAC 3 [coefficient: 1.75, 95% CI: 0.87–2.63; p<0.001], FAC 4 [coefficient: 1.62, 95% CI: 0.99–2.25; p<0.001] and FAC 5 [coefficient: 1.67, 95% CI: 1.04–2.29; p<0.001]), anaesthetic risk, taking ASA score I as reference (ASA score IV [coefficient 2.11, 95% CI: 0.36–3.85; p<0.001]), and type of fracture, taking as reference non-displaced intracapsular fracture (subtrochanteric fracture [coefficient 0.84, 95% CI: 0.17–1.51; p=0.014] and other fracture [coefficient 1.86, 95% CI: 0.12–3.61; p=0.036]).
In centenarians, only a time to surgery over 48 hours was related to length of stay (coefficient 3.99 [95% CI: 2.35–5.64; p<0.001]).
30-Day Mortality
Multivariate analysis found that the following variables were associated with 30 day-mortality: female sex (OR 0.47, 95% CI: 0.41–0.54; p<0.001), time to surgery >48 hours (OR 1.24, 95% CI: 1.08–1.42; p=0.002]), baseline ambulatory capacity, taking FAC 0 as a reference (FAC 3 [OR: 0.54, 95% CI: 0.38–0.79; p=0.001], FAC 4 [OR: 0.48 [95% CI: 0.37–0.61; p<0.001] and FAC 5 [OR: 0.31, 95% CI: 0.24–0.40; p<0.001]), baseline cognitive function, taking as a reference no cognitive impairment (moderate dementia [OR: 1.34, 95% CI: 1.11–1.63; p=0.002] and severe dementia [OR: 1.53, 95% CI: 1.27–1.84; p<0.001]), anaesthetic risk, taking ASA score I as reference (ASA score III [OR 8.01, 95% CI: 1.11–58.0; p=0.039], ASA score IV [OR 16.3, 95% CI: 2.24–118; p=0.006] and V [OR 54.5, 95% CI: 5.61–530; p=0.001]), peripheral nerve block (OR 0.77, 95% CI: 0.63–0.93; p=0.007), neuraxial anaesthesia (OR 0.64, 95% CI: 0.51–0.80; p<0.001), and age group, taking <80 years as a reference (80–89 years [OR 1.72, 95% CI: 1.29–2.29; p<0.001]; 90–99 years [OR 3.09, 95% CI: 2.31–4.13; p<0.001]; ≥100 years [OR 6.43, 95% CI: 3.76–11.0; p<0.001]).
In centenarians, after multivariate analysis only the anaesthetic risk, taking ASA score V as reference (ASA score II [OR 0.25, 95% CI: 0.09–0.70; p=0.009] and III [OR 0.43, 95% CI: 0.19–0.96; p=0.039]), remained significantly associated with 30-day mortality.
Discussion
The present study provides three main results. Firstly, centenarians were more frequently women, had a high prevalence of dementia and dependency and nearly four out of ten were institutionalised. The most frequent fracture was intertrochanteric. The length of hospital stay was 8.6 days, in-hospital mortality was 10.3% and 30-day mortality was 20.9%.
Secondly, older age groups had greater percentages of women, severe functional dependency, severe dementia, intertrochanteric fracture, living in care facilities, and being discharged to nursing care. Early mobilisation, treatment for osteoporosis and being discharged to rehabilitation units were less frequent. In-hospital and 30-day mortality were higher with increasing age of groups.
Thirdly, time to surgery was independently associated with length of stay and anaesthetic risk was related to 30-day mortality in the centenarian group.
Our study showed a cohort of centenarians which were commonly women and had a high frequency of functional dependency, cognitive impairment and institutionalisation, in contrast to some previous studies.26 The prevalence of cognitive impairment in patients with hip fractures varies widely among studies, ranging from values similar to those in our group of younger patients (40%) to others more similar to those in our group of centenarians (80%).27
Intertrochanteric fractures were the most frequent in centenarians and also increased with ageing as observed in other studies from Spain and the United States.4–7 In contrast, intracapsular fractures were reported to be more frequent in Denmark.8
One out of two centenarians underwent surgery in less than 48 hours. This frequency was even higher than that of some of the younger age groups. In our study, time to surgery >48 hours was associated with length of hospital stay but not with survival in centenarians. Our finding was consistent with that of other authors,5,28 who concluded that surgery in centenarians in less than 48 hours did not reduce mortality. Some authors showed similar rates of surgery ≤48 hours without shorter length of hospital stay compared to other age groups,9 while others reported longer surgical delay (1.9 vs 3.6 days) and length of stay (14 vs 20 days).28
We would like to highlight the lower percentage of mobilisation on the first day and the higher frequency of pressure ulcer development the older the age group. In the centenarian group, six out of ten were mobilized the first day after surgery and nearly one out of ten developed pressure ulcers during their hospital stay. This may be due to the higher baseline degree of cognitive impairment and dependency or the higher degree of in-hospital complications in this age group.9,11,12
Centenarians received anti-osteoporotic medication (14.1%), calcium (33.6%) and vitamin D supplements (55.9%) at discharge. Bone-protective medication was much less likely to be prescribed in older age groups, despite a seven-fold higher incidence of hip fracture in centenarians than in younger patients2 and despite hip fractures being the most common cause of hospitalization in centenarians.3 In view of the current evidence, the low rate of primary and secondary fracture prevention in centenarians does not seem justified.
The median length of hospital stay was 8.6 days, lower than that of some younger age groups. Length of stay was shorter in centenarians, as observed in other studies.21 As mentioned above, the length of hospital stay was associated with time to surgery >48 hours, baseline ambulatory capacity, anaesthetic risk and type of fracture in our entire sample. Only time to surgery was an independent factor in centenarians.
Institutionalization at discharge increased with age, but referral to geriatric rehabilitation units at discharge was lower in centenarians. Functional impairment was greater in centenarians compared to the younger age groups. It has been previously described that centenarians are at higher risk of functional decline and dependency during hospitalization.4 This could be explained in part by the higher prevalence of cognitive impairment, but it would be interesting to study which variables affect this functional decline and to quantify the effect of decreased rehabilitation in this age group, as this is a modifiable factor, since dementia does not appear to be a clear factor in functional deterioration after hip fracture.29 Orthogeriatric interventions have proven to provide the most benefit to the oldest patients and those with functional and cognitive impairment; they have been shown to reduce mortality, complications, length of stay and functional impairment following hip fractures. Centenarians are likely to be among those who would benefit the most from these interventions.27
The in-hospital and one-month mortality were 10.3% and 20.9%, respectively, and was higher as the age of the groups increased. Ogawa T et al showed that age was an independent predictor of in-hospital mortality.10 Thirty-day mortality has been reported to be approximately 8–34% in older patients.6–8,11,12,18,23 Our findings showed that female sex, time to surgery >48 hours, baseline ambulatory capacity and cognitive function, anaesthetic risk, type of anaesthesia and peripheral nerve block, and age group were related to 30-day mortality over the entire sample. However, only the ASA score was associated with 30-day mortality in centenarians. In contrast with previous studies, we did not find an association with type of fracture. Mortality after subtrochanteric fractures has been described to be almost twice as high as after other types of fractures.30,31 Also, while other authors have concluded that arthroplasty reduced the risk of mortality compared to internal fixation,5 we were unable to find differences between different surgical interventions. Regarding anaesthesia, evidence has been conclusive as to the effect of nerve blocks on the reduction of pain and delirium, but their association with functional recovery and mortality was less clear.32
The results of the present work increase the evidence for the effect of age on in-hospital and short-term mortality in elderly patients with hip fracture. Despite this, age per se should not be considered a limiting factor to surgery in very elderly patients. As occurs in younger age groups, surgical treatment of hip fractures has been shown to reduce the risk of mortality in centenarians, compared to those managed non-operatively.24 In the case of centenarians, we have found that their previous medical condition is a prognostic factor and, therefore, the assessment of surgical risk in this age group becomes even more important. The involvement of geriatricians in this decision-making process is crucial in the very elderly, as is taking into consideration the patient’s rights and wishes.33 Furthermore, the multidisciplinary team should work to minimize surgery time, optimize the patient prior to surgery, mobilize the patient early and prevent postoperative complications.
We are aware of several limitations of our study. There are a significant number of variables that are not collected in the registry, for example, geriatric syndromes such as nutritional status34 or delirium35,36 that also contribute to mortality and length of stay and are modifiable factors in older persons. Neither does the registry include perioperative variables such as the need for transfusion or time of surgery, nor postoperative weight-bearing status, likely related with destination and mortality at discharge. The latter has recently been added to the registry’s list of variables. Finally, the number of centenarians in our analysis was lower than the number of patients in other age groups, limiting statistical power and thus increasing the likelihood that associations were not found despite them existing. However, our series is one of the largest published to date, using data collected prospectively from a large number of hospitals in Spain, increasing the external validity of our conclusions. Furthermore, Spain is one of the countries with the highest life expectancy and largest number of centenarians worldwide, with the RNFC providing an ideal framework to study hip fractures in this age group. In contrast to other studies using automated datasets, the RNFC includes follow-up after discharge collected by participating clinicians, providing insight into the functional decline, mortality and institutionalization due to the fracture.
Conclusions
Centenarians were more likely to suffer intertrochanteric fractures and had worse baseline functional status, cognitive status, and short-term outcomes than other age groups. However, nearly 4 out of 5 centenarians were alive in the first month after surgery. One-month survival seemed to be affected more by baseline comorbidity as estimated by anaesthetic risk than by other factors.
Ethics Approval
The RNFC has been approved by the Research Ethics Committees of each of its member hospitals. The same Participant Consent Forms were used across all hospitals.
Acknowledgments
Thank you to F. Javier Martín-Sánchez for his critical review and all the researchers of the 86 hospitals that make up the Spanish National Fracture Registry (RNFC),see Supplementary materials for details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by AMGEN SA, UCB Pharma, Abbott Laboratories and FAES Farma; two research grants awarded by Fundación Mutua Madrileña (grant number AP169672018) and Fundación Mapfre and research grants from the spanish government: Proyecto de investigaci’ón en Salud del ISC III (AS2020) PI 20/00158. The sponsors were not involved in any aspect of the project or in the preparation of the manuscript.
Disclosure
Dr Cristina Ojeda-Thies reports grants, travel assistance for scientific meetings from UCB Iberica, grants, personal fees, honoraria for presentations, travel assistance for scientific meetings from AMGEN, travel assistance for scientific meetings from STADA, personal fees, honoraria for presentations travel assistance for scientific meetings from Grunenthal Pharma, during the conduct of the study; personal fees, honoraria for presentations travel assistance for scientific meetings from MBA Surgical Empowerment, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Instituto Nacional de Estadística. Proyecciones de Población 2018. Instituto Nacional de Estadística; 2018:20.
2. Alvarez-Nebreda ML, Jiménez AB, Rodríguez P, Serra JA. Epidemiology of Hip fracture in the elderly in Spain. Bone. 2008;42(2):278–285. doi:10.1016/j.bone.2007.10.001
3. Sáez-Nieto C, Ly-Yang F, Pérez-Rodríguez P, Alarcón T, López-Arrieta J, González-Montalvo JI. Impact of hospital admission on centenarians admitted due to an acute illness. A description of a series of 165 cases and comparison with the literature. Rev Esp Geriatr Gerontol. 2019;54(6):315–320. doi:10.1016/j.regg.2019.04.005
4. Rodríguez-Molinero A, Yuste A, Banegas JR. High incidence of Hip fracture in Spanish centenarians. J Am Geriatr Soc. 2010;58(2):403–405. doi:10.1111/j.1532-5415.2009.02706.x
5. Manoli A, Driesman A, Marwin RA, Konda S, Leucht P, Egol KA. Short-term outcomes following hip fractures in patients at least 100 years old. J Bone Joint Surg Am. 2017;99(13):e68. doi:10.2106/JBJS.16.00697
6. Tanner DA, Kloseck M, Crilly RG, Chesworth B, Gilliland J. Hip fracture types in men and women change differently with age. BMC Geriatr. 2010;10:12. doi:10.1186/1471-2318-10-12
7. López-Torres II, Sanz-Ruiz P, Montero-Fernández N, et al. Surgical treatment of Hip fracture in centenarians: complications and independent risk factors of death. Injury. 2020;51(Suppl 1):S25–S29. doi:10.1016/j.injury.2020.03.053
8. Mosfeldt M, Madsen CM, Lauritzen JB, Jørgensen HL. Centenarian Hip fracture patients: a nationwide population-based cohort study of 507 patients. Acta Orthop. 2019;90(4):342–347. doi:10.1080/17453674.2019.1602386
9. Barceló M, Francia E, Romero C, Ruiz D, Casademont J, Torres OH. Hip fractures in the oldest old. Comparative study of centenarians and nonagenarians and mortality risk factors. Injury. 2018;49(12):2198–2202. doi:10.1016/j.injury.2018.09.043
10. Ogawa T, Schermann H, Kobayashi H, Fushimi K, Okawa A, Jinno T. Age and clinical outcomes after Hip fracture surgery: do octogenarian, nonagenarian and centenarian classifications matter? Age Ageing. 2021;50(6):1952–1960. doi:10.1093/ageing/afab137
11. Dick AG, Davenport D, Bansal M, Burch TS, Edwards MR. Hip fractures in centenarians: has care improved in the national Hip fracture database era? Geriatr Orthop Surg Rehabil. 2017;8(3):161–165. doi:10.1177/2151458517722104
12. Morice A, Reina N, Gracia G, et al. Proximal femoral fractures in centenarians. A retrospective analysis of 39 patients. Orthop Traumatol Surg Res. 2017;103(1):9–13. doi:10.1016/j.otsr.2016.09.025
13. Warner MA, Saletel RA, Schroeder DR, Warner DO, Offord KP, Gray DT. Outcomes of anesthesia and surgery in people 100 years of age and older. J Am Geriatr Soc. 1998;46(8):988–993. doi:10.1111/j.1532-5415.1998.tb02754.x
14. Tarity TD, Smith EB, Dolan K, Rasouli MR, Maltenfort MG. Mortality in centenarians with Hip fractures. Orthopedics. 2013;36(3):e282–e287. doi:10.3928/01477447-20130222-15
15. Forster MC, Calthorpe D. Mortality following surgery for proximal femoral fractures in centenarians. Injury. 2000;31(7):537–539. doi:10.1016/s0020-1383(00)00049-8
16. Oliver CW, Burke C. Hip fractures in centenarians. Injury. 2004;35(10):1025–1030. doi:10.1016/j.injury.2003.10.004
17. Holt G, Smith R, Duncan K, Hutchison JD, Gregori A. Outcome after surgery for the treatment of Hip fracture in the extremely elderly. J Bone Joint Surg Am. 2008;90(9):1899–1905. doi:10.2106/JBJS.G.00883
18. Cheung MY, Ho AW, Wong SH. Operative outcome of Hong Kong centenarians with Hip fracture. Hong Kong Med J. 2017;23(1):63–66. doi:10.12809/hkmj164823
19. Mazzola P, Perego S, Picone D, et al. Hip fracture in centenarians: retrospective analysis of an orthogeriatric unit reveals the limitations of the current research. Glob Anesth Perioper Med. 2015;1(3). doi:10.15761/GAPM.1000118
20. Barrett-Lee J, Barbur S, Johns J, Pearce J, Elliot RR. Hip fractures in centenarians: a multicentre review of outcomes. Ann R Coll Surg Engl. 2021;103(1):59–63. doi:10.1308/rcsann.2020.0203
21. Sarasa-Roca M, Torres-Campos A, Redondo-Trasobares B, Angulo-Castaño MC, Gómez-Vallejo J, Albareda-Albareda J. Hip fracture in centenarians, what can we expect? Rev Esp Cir Ortop Traumatol. 2021. doi:10.1016/j.recot.2021.04.004
22. Hogan PCP, Ferris H, Brent L, McElwaine P, Coughlan T. Characteristics of centenarians in the Irish Hip fracture database. Ir Med J. 2021;114(7):401.
23. Moore J, Carmody O, Carey B, Harty JA, Reidy D. The cost and mortality of Hip fractures in centenarians. Ir J Med Sci. 2017;186(4):961–964. doi:10.1007/s11845-017-report1589-9
24. Ng WX, Kwek EB. Too old for surgery? Outcomes of Hip fracture surgery in centenarians. Ann Acad Med Singap. 2017;46(3):115–117. doi:10.47102/annals-acadmedsg.V46N3p115
25. Sáez-López P, González-Montalvo JI, Ojeda-Thies C, et al. Spanish National Hip Fracture Registry (SNHFR): a description of its objectives, methodology and implementation. Rev Esp Geriatr Gerontol. 2018;53(4):188–195. doi:10.1016/j.regg.2017.12.001
26. Blanco JF, da Casa C, Sánchez de Vega R, Hierro-Estévez MA, González-Ramírez A, Pablos-Hernández C. Oldest old Hip fracture patients: centenarians as the lowest complexity patients. Aging Clin Exp Res. 2020;32(12):2501–2506. doi:10.1007/s40520-020-01476-5
27. Tarazona-Santabalbina FJ, Ojeda-Thies C, Figueroa Rodríguez J, Cassinello-Ogea C, Caeiro JR. Orthogeriatric management: improvements in outcomes during hospital admission due to Hip fracture. Int J Environ Res Public Health. 2021;18(6):3049. doi:10.3390/ijerph18063049
28. Verma R, Rigby AS, Shaw CJ, Mohsen A. Acute care of Hip fractures in centenarians--do we need more resources? Injury. 2009;40(4):368–370. doi:10.1016/j.injury.2008.09.008
29. Delgado A, Cordero G-G E, Marcos S, Cordero-Ampuero J. Influence of cognitive impairment on mortality, complications and functional outcome after Hip fracture: dementia as a risk factor for sepsis and urinary infection. Injury. 2020;51(Suppl 1):S19–S24. doi:10.1016/j.injury.2020.02.009
30. Panteli M, Giannoudi MP, Lodge CJ, West RM, Pountos I, Giannoudis PV. Mortality and medical complications of subtrochanteric fracture fixation. J Clin Med. 2021;10(3):540. doi:10.3390/jcm10030540
31. Mattisson L, Bojan A, Enocson A. Epidemiology, treatment and mortality of trochanteric and subtrochanteric Hip fractures: data from the Swedish fracture register. BMC Musculoskelet Disord. 2018;19(1):369. doi:10.1186/s12891-018-2276-3
32. Guay J, Kopp S. Peripheral nerve blocks for Hip fractures in adults. Cochrane Database Syst Rev. 2020;11:CD001159. doi:10.1002/14651858.CD001159.pub3
33. Herrera-Pérez M, González-Martín D, Sanz EJ, Pais-Brito JL. Ethical dilemmas with regard to elderly patients with Hip fracture: the problem of nonagenarians and centenarians. J Clin Med. 2022;11(7):1851. doi:10.3390/jcm11071851
34. Malafarina V, Reginster JY, Cabrerizo S, et al. Nutritional status and nutritional treatment are related to outcomes and mortality in older adults with Hip fracture. Nutrients. 2018;10(5):555. doi:10.3390/nu10050555
35. Zerah L, Cohen-Bittan J, Raux M, et al. Association between cognitive status before surgery and outcomes in elderly patients with Hip fracture in a dedicated orthogeriatric care pathway. J Alzheimers Dis. 2017;56(1):145–156. doi:10.3233/JAD-160655
36. Lee PJ, Shorten GD. Delirium after Hip fracture surgery. J Clin Anesth. 2019;58:119–120. doi:10.1016/j.jclinane.2019.06.034
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.