")
Back to Journals » Infection and Drug Resistance » Volume 17
Clinical Characteristics and Analysis of Associated Risk Factors in Patients with Severe and Non-Severe COVID-19 Infection
Authors Zhou Y, Wang Z, Chen F, Xiong YX, Wang W, Huang JM, Fang W
Received 25 December 2023
Accepted for publication 3 April 2024
Published 18 April 2024 Volume 2024:17 Pages 1539—1544
DOI https://doi.org/10.2147/IDR.S456333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Yong Zhou, Zhen Wang, Fei Chen, Ying-Xia Xiong, Wei Wang, Jun-Min Huang, Wei Fang
Department of Emergency, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Zhen Wang, Department of Emergency, Beijing Shijitan Hospital, Capital Medical University, No. 10 Tieyi Road, Yangfangdian, Haidian District, Beijing, 100038, People’s Republic of China, Tel +86 10 63926250, Fax +86 10 63925651, Email [email protected]
Objective: Our aim was to highlight the clinical characteristics and determine the risk factors associated with severe and non-severe COVID-19 infection.
Study Method: A retrospective review was conducted on clinical data obtained from patients with COVID-19 infection, admitted to the emergency department between November 2022 and January 2023. Total of 1684 participants were categorized into severe (312 cases,18.53%) and non-severe (1,372 cases,81.47%) cohorts. Logistic regression was utilized for multivariate analysis, with a P-value less than 0.05 signifying a significant difference between the groups.
Results: The study consisted of 952 males (56.53%) and 732 females (43.47%) participants. The age distribution ranged from 18 to 93 years in both cohorts. There were statistically significant differences between the clinical symptoms of the severe and non-severe cohorts (P < 0.05). According to the multivariate statistical analysis, patients with more pronounced clinical manifestations had significantly elevated values related to age(P < 0.05), diabetes(P < 0.01), hypertension(P < 0.01), C-reactive protein (CRP) (P < 0.05), and lactate dehydrogenase (LDH) (P < 0.01) as compared to those presenting with milder symptoms.
Conclusion: The primary clinical presentations in both the cohorts were mostly similar. Predominant factors contributing to the severity of COVID-19 infection were age, diabetes, hypertension, elevated CRP levels, and increased LDH.
Keywords: clinical manifestations, COVID-19, risk factors
Introduction
SARS-CoV-2, which is the etiological agent of COVID-19, is a novel acute infectious pathogen that holds a significant threat to human health because of its high rate of infectivity. Its principal modes of transmission are through respiratory droplets, direct contact, and aerosolized particles.1 The most common symptoms of COVID-19 infection include fever and respiratory abnormalities, with a majority of patients manifesting symptoms such as dry cough, dyspnea, fatigue, dizziness, anosmia, and diarrhea.2–4 A percentage of patients exhibit rapid deterioration, resulting in acute respiratory distress syndrome (ARDS), shock, multi-organ failure, and in some instances, mortality within a brief time span.5 At present, the circulating strain has evolved from the initial strain to various subtypes of Omicron. A wave of cases of Omicron infection has been reported across the country as the epidemic prevention and control measures have been relaxed.This investigation was initiated to conduct clinical and epidemiological assessments on 1,684 patients with COVID-19 infection to elucidate disease progression patterns, develop a standard operating protocol for early detection and targeted therapeutic interventions, and establish an early warning index system.
General Information
From a cohort of 1,968 individuals, who presented to the Emergency department of Beijing Shijitan Hospital (affiliated hospital of Capital Medical University) between November 2022 and January 2023, patients with incomplete medical records were excluded from the study. This resulted in a study population of 1,684 patients diagnosed with COVID-19. Most of the patients were vaccinated against COVID-19 a year ago. All patients with confirmed novel coronavirus pneumonia are offered antiviral treatment.
Inclusion criteria: a) The clinical classification and diagnosis of the patients must be in accordance with the Diagnosis and Treatment Protocol for COVID-19 Patients (Tentative 10th Edition). b) Comprehensive general and clinical data must be available for each patient.
Exclusion criteria: a) Patients with incomplete or missing data. b) Women who are pregnant. c) Individuals who were asymptomatic but test positive for SARS-CoV-2 antigen or nucleic acid. d) Patients initially diagnosed based on suggestive symptoms but lacked definitive diagnostic confirmation; they may be reconsidered for inclusion upon definitive diagnosis.
Study Methods
Source of Clinical Data
- The patient information management system in the hospital was used to obtain demographic and epidemiological data. This included factors such as gender, age, underlying co-morbidities, or other health conditions. Clinical classifications were determined based on patient presentation prior to and post-admission.
- Data retrieval strategies included comprehensive medical record reviews and telephonic follow-ups to acquire diagnostic and therapeutic details from patients infected with COVID-19.
- Laboratory markers were assessed, including but not limited to C-reactive protein (CRP) and lactate dehydrogenase.
Diagnostic Criteria
The following diagnostic criteria included in the Diagnosis and Treatment Protocol for COVID-19 Patients (Tentative 10th Edition) were utilized: a) Clinical manifestations suggestive of COVID-19 infection. b) At least one of the following pathogenic or serological test results mentioned: i. A positive nucleic acid test result for COVID-19 infection. ii. A positive test result for SARS-CoV-2 antigen. iii. A positive COVID-19 virus isolation and culture. iv. Retrospective diagnosis is indicated after convalescence by a spike in specific IgG antibodies against COVID-19, which is at least four times higher than during the acute phase.
Grouping Strategy
According to the Expert recommendations for management of severe COVID-19, patients with mild to moderate manifestations were allocated to the non-severe group. In comparison, those with severe or critically severe manifestations were categorized in the severe group.6
Statistical Analysis
Data processing and analysis was performed using the SPSS 24.0 software suite. Quantitative data subsets were compared using t-test, and represented as mean ± standard deviation (x±s), while categorical data sets were scrutinized using the chi-squared (χ2) test, and the result expressed in percentages. Logistic regression was used for multivariate analytic methods; a P-value threshold of less than 0.05 was deemed indicative of statistically definitive group variances.
Results
Overview of COVID-19 Cases
In the study cohort of 1684 patients, the average age of patients in the severe group was 52.91±14.44 years, while the non-severe group had an average age of 42.20±14.71 years, representing a statistically significant difference in age distributions (t = 5.823, P < 0.001). Regarding gender, the severe group consisted of 212 males (67.94%) and 100 females (32.06%). In comparison, the non-severe group had 740 males (53.94%) and 632 females (46.06%), with a notable difference in gender distribution (χ2 = 5.078, P=0.024). Among the two groups, 640 patients had pre-existing conditions, of which 288 (45%) were in the severe group and 362 (55%) in the non-severe group. There were 304 cases of hypertension, 192 of diabetes, and 112 with both hypertension and diabetes. In the severe group, 160 patients (12.82%) had a history of hypertension and 128 patients (10.25%) had a history of diabetes. In comparison, in the non-severe group, 144 patients (2.62%) had a history of hypertension and 64 patients (1.17%) had a history of diabetes. The ratio of patients with underlying diseases such as hypertension and diabetes in the severe group was significantly higher than that in the non-severe group (χ2 = 15.332, 18.963, both P < 0.001). (Refer Table 1).
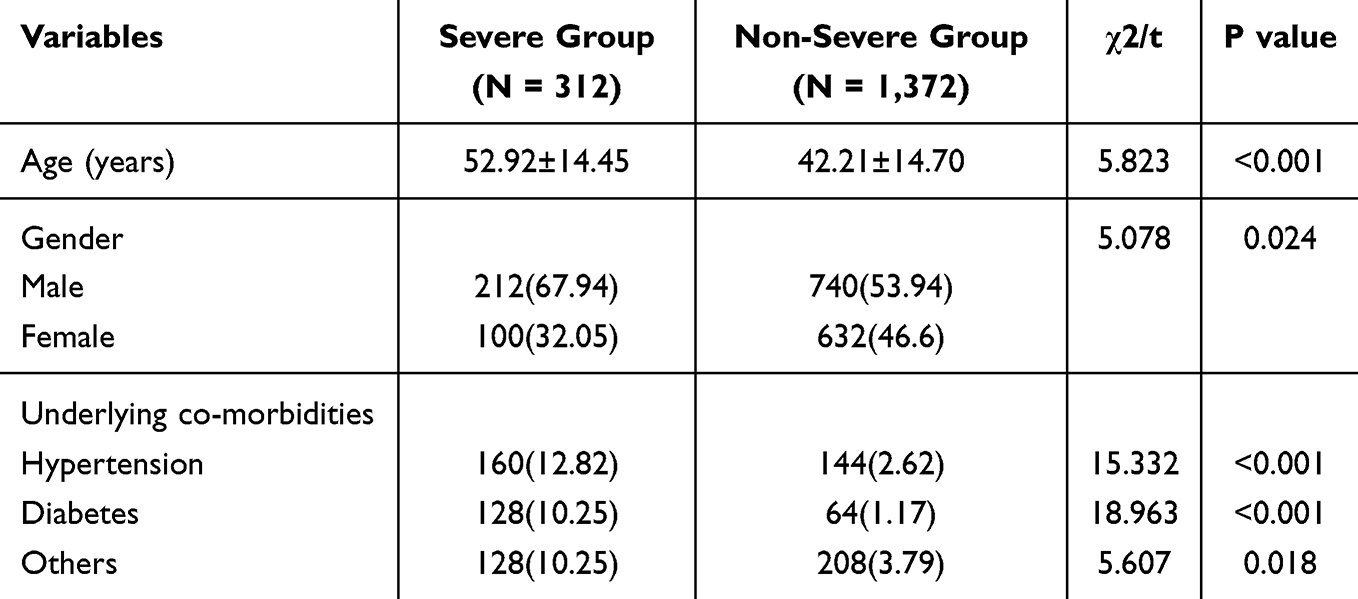 |
Table 1 Comparison of Male to Female Ratio, Age, and Underlying Diseases Between the Two Groups of Patients with COVID-19 Infection |
Comparison of Clinical Manifestations Between the Groups
The severe group exhibited an increased frequency of initial symptoms like fever, cough, fatigue, and dyspnea compared to the non-severe group. Among these, 128 patients (41.02%) in the severe group had temperatures exceeding 38.5 °C, whereas 312 patients (22.74%) in the non-severe group registered below this threshold, marking a significant difference (χ2 = 11.008, P < 0.001)). The prevalence of severe cough with expectoration was seen in 44 patients (14.10%) in the severe group, in comparison with 84 patients (6.12%) in the non-severe group (χ2 = 5.762, P = 0.016). Fatigue was reported by 64 patients (20.51%) in the severe group and 140 patients (10.20%) in the non-severe group (χ2 = 6.343, P = 0.012). Dyspnea was observed in 48 patients (15.38%) in the severe group and 48 patients (3.49%) in the non-severe group, with the difference being statistically significant (χ2 = 3.994, P = 0.046) (Refer Table 2).
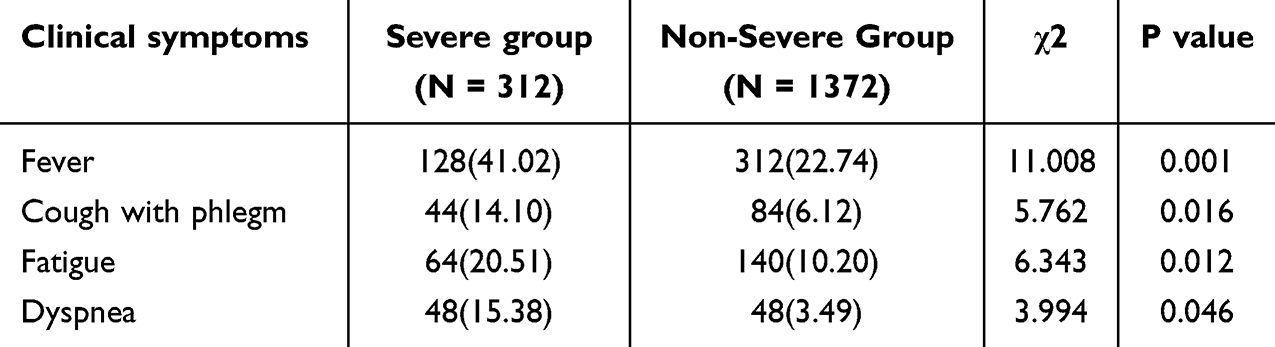 |
Table 2 Comparison of Clinical Symptoms Between the Severe and Non-Severe Groups |
Logistic Regression Analysis of Factors Influencing Severe COVID-19 Disease Progression
Age, hypertension, diabetes, CRP, and LDH levels were included as continuous variables in the logistic regression model with the progression to severe disease as the dependent variable(0 = no, 1 = yes), (Refer Table 3). A suitable model was developed after these categorical variables were assigned values and the stepwise regression method was used to eliminate unnecessary variables (P < 0.05). The conclusive multivariate regression analysis identified the factors for increased severity in patients with COVID-19 infection as: age (odds ratio = 1.05), history of type 2 diabetes (odds ratio = 7.52), antecedent hypertension (odds ratio = 1.31), LDH (odds ratio = 1.01), and CRP (odds ratio = 1.03) (P < 0.05) (Refer Table 4).
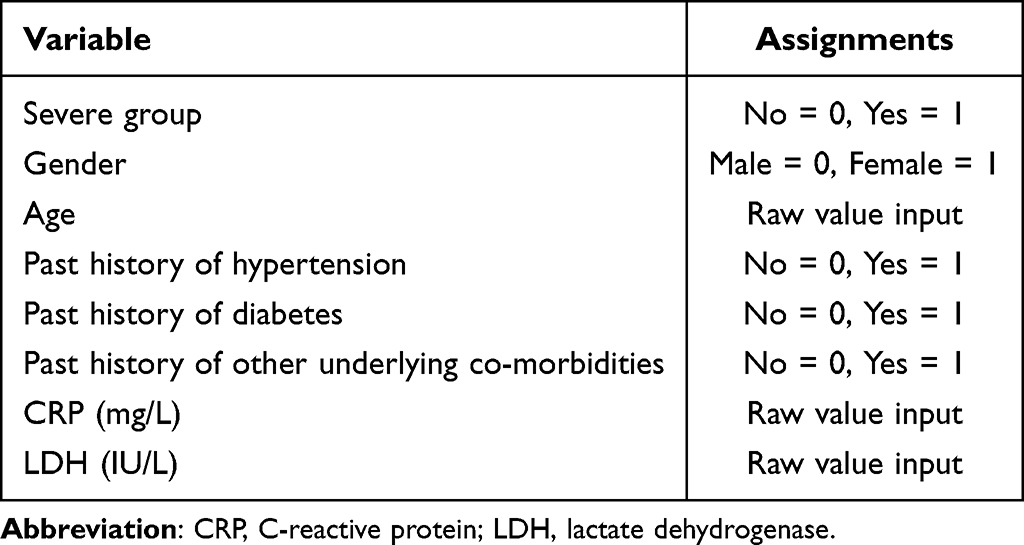 |
Table 3 Assignment Table |
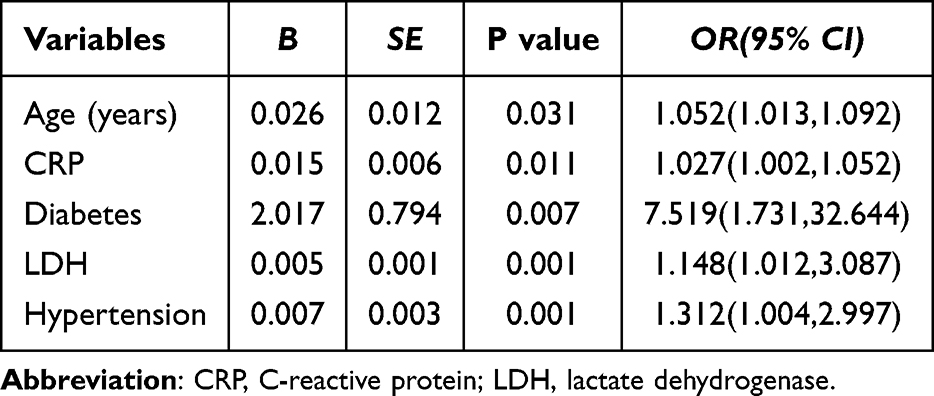 |
Table 4 Multivariate Logistic Regression Analysis of Risk Factors for Patients with Severe COVID-19 Infection |
Discussion
COVID-19 infection exhibits clinical manifestations that are often non-specific, making early detection a challenge. As the disease progresses, patient mortality tends to rise sharply. Consequently, identifying disease characteristics and significant risk factors for adverse outcomes becomes crucial in improving the accuracy of therapeutic approaches, thus mitigating complications and minimizing mortality rate.
In our cohort of 1,684 patients with COVID-19 infection, the male-to-female ratio stood at 1.28:1. A striking observation was that males constituted 67.9% of the severe category, while females represented only 32.1%. This gender disparity is consistent with earlier studies indicating that men are at a heightened risk for contracting COVID-19 and develop severe disease.7 Mechanistic studies provide some insights into this discrepancy; the ACE receptor found on the cellular membranes plays a key role in facilitating the entry of SARS-COV-2 in to the cells. Existing literature suggests that ACE expression may vary depending on the gender. Notably, estrogen has been shown to downregulate ACE expression in vitro,8 a finding that is supported by research in murine models.9 The gender disparity in the severity of SARS-COV-2 infection that have been discovered may be explained by these variations in ACE expression.
According to previous studies, it has been highlighted that children have a reduced predisposition for severe COVID-19 outcomes. This has been attributed to diminished ACE expression in their respiratory tract.10 Age emerges as a pivotal factor in the susceptibility, severity, and fatality associated with SARS-CoV-2 infections.11,12 Consistent with these findings, our data revealed a prevalence of COVID-19 infection in patients aged between 40 to 69 years. More specifically, patients with severe symptoms had an average age of 52.91±14.44 years, which is higher than their non-severe counterparts, with an average age of 42.20±14.71 years. This enhanced vulnerability of the elderly to severe COVID-19 outcomes is highlighted by this discrepancy. As a result, it is suggested that this group should be managed with extra caution. It is essential to take preventive steps, such as prohibiting them from attending large gatherings, and institute strict visitation rules in institutions catering to the elderly such as housing for senior citizens.
Our clinical observations suggest a complex correlation between the severity of COVID-19 and existing co-morbidities. Specifically, patients with multiple chronic ailments, particularly hypertension and diabetes, exhibited worse clinical prognosis compared to those without such underlying conditions. In this cohort of 640 patients with pre-existing conditions, 204 patients were diagnosed with hypertension, 192 patients with diabetes, and 112 had a dual diagnosis of both hypertension and diabetes. Several potential mechanisms have been explained in literature. It is postulated that SARS-CoV-2 may exacerbate insulin resistance,13 through its interaction with the ACE2 receptor.14 Interestingly, the profile of ACE2 expression is altered in diabetics.15 Patients with diabetes are more likely to experience more severe COVID-19 symptoms due to increased ACE2 expression, which also increases the mortality risk.15 Captopril is one common antihypertensive drug, that may possibly increase the expression of ACE2 protein in patients with hypertension. This potentially facilitates greater viral uptake, resulting in a more aggressive disease trajectory.16 Considering these insights, it is significant for healthcare professionals to meticulously assess medical histories of patients upon presentation, taking in to account any underlying medical conditions, Vaccination history, medications, allergies, surgical interventions, and more. Furthermore, those with chronic ailments like hypertension and diabetes should strictly adhere to COVID-19 preventive measures.
Subsequently, we utilized logistic regression to analyze how various factors impacted the severity of COVID-19. Our findings highlighted the profound influence of variables such as age, history of diabetes and hypertension, LDH, and CRP levels on the clinical severity of COVID-19. Recognizing and monitoring these parameters during hospital admissions and preliminary investigations can offer a strategic advantage, facilitating the early detection of potential severe COVID-19 cases and permitting for timely targeted interventions, and ultimately improving patient outcomes.
The patients included in this study are located in Beijing, where the population vaccination rate is high, and most of the patients included in the study have a history of vaccination. Most of the patients had a vaccination history of more than one year at the time of visit, so the vaccination history was not included in the factor analysis in this study. All hospitalized patients are offered antiviral treatment after being diagnosed with COVID-19. The study period was at the end of the epidemic, and the infectious agent was Omicron subtype, so the study had certain geographical and time limitations. It needs attention.
Conclusion
Our study outlines key factors like age, a history of diabetes and hypertension, CRP, and LDH levels that are correlated with the severity of SARS-CoV-2 infection. Prioritizing these factors during patient admissions and initial evaluations will help identify patients with severe COVID-19 infections quickly and enable early management.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study is a retrospective study, where researchers only conduct retrospective analysis on the condition and treatment, without inquiring about patient names. Strict confidentiality is maintained for other personal information of the patients. Therefore, the Ethics Committee of Beijing Shijitan Hospital does not require patient consent for reviewing their medical records in such retrospective studies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wu F, Zhao S, Yu B. et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265–269. doi:10.1038/s41586-020-2008-3
2. Danzi GB, Loffi M, Galeazzi G, Gherbesi E. Acute pulmonary embolism and COVID-19 pneumonia: a random association? Eur Heart J. 2020;41(19):1858. doi:10.1093/eurheartj/ehaa254
3. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
4. Mao L, Jin H, Wang M, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683–690. doi:10.1001/jamaneurol.2020.1127
5. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574. doi:10.1016/S0140-6736(20)30251-8
6. Jiang L, Pan C, Sang L et al. Chinese society of critical care medicine.expert recommendations for management of severe COVID-19. Chinese. J Cri Care Inten Care Med. 2020;6(01):1–11.
7. Alwani M, Yassin A, Al-Zoubi RM, et al. Sex-based differences in severity and mortality in COVID-19. Rev Med Virol. 2021;31(6):e2223. doi:10.1002/rmv.2223
8. Stelzig KE, Canepa-Escaro F, Schiliro M, Berdnikovs S, Prakash YS, Chiarella SE. Estrogen regulates the expression of SARS-CoV-2 receptor ACE2 in differentiated airway epithelial cells. Am J Physiol Lung Cell Mol Physiol. 2020;318(6):L1280–L1281. doi:10.1152/ajplung.00153.2020
9. Liu J, Ji H, Zheng W, et al. Sex differences in renal angiotensin converting enzyme 2 (ACE2) activity are 17β-oestradiol-dependent and sex chromosome-independent. Biol Sex Differ. 2010;1(1):6. doi:10.1186/2042-6410-1-6
10. Abrehart T, Suryadinata R, McCafferty C, et al. Age-related differences in SARS-CoV-2 binding factors: an explanation for reduced susceptibility to severe COVID-19 among children? Paediatr Respir Rev. 2022;44:61–69. doi:10.1016/j.prrv.2022.01.008
11. Chen Y, Li C, Liu F, et al. Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model. Emerg Microbes Infect. 2022;11(1):368–383. doi:10.1080/22221751.2022.2026741
12. Fialkowski A, Gernez Y, Arya P, Weinacht KG, Kinane TB, Yonker LM. Insight into the pediatric and adult dichotomy of COVID-19: age-related differences in the immune response to SARS-CoV-2 infection. Pediatr Pulmonol. 2020;55(10):2556–2564. doi:10.1002/ppul.24981
13. Yang JK, Lin SS, Ji XJ, Guo LM. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol. 2010;47(3):193–199. doi:10.1007/s00592-009-0109-4
14. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–280.e8. doi:10.1016/j.cell.2020.02.052
15. Peric S, Stulnig TM. Diabetes and COVID-19: disease-management-people. Wien Klin Wochenschr. 2020;132(13–14):356–361. doi:10.1007/s00508-020-01672-3
16. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020;8(4):e21. doi:10.1016/S2213-2600(20)30116-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.