")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Clinician Awareness of Stickler Syndromes Among Australian Allied Health Care Professionals
Authors Britten-Jones AC , Ayton LN , Graydon K, Boyce JO, Braden R, Dawkins R, Cham KM
Received 11 December 2023
Accepted for publication 8 April 2024
Published 22 April 2024 Volume 2024:17 Pages 1755—1768
DOI https://doi.org/10.2147/JMDH.S454428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alexis Ceecee Britten-Jones,1– 3 Lauren N Ayton,1– 3 Kelley Graydon,4 Jessica O Boyce,4 Ruth Braden,4 Rosie Dawkins,2,3,* Kwang Meng Cham1,* On behalf of The Stickler Syndrome Awareness Study Group
1Department of Optometry and Vision Sciences, University of Melbourne, Melbourne, Victoria, Australia; 2Department of Surgery (Ophthalmology), University of Melbourne, Melbourne, Victoria, Australia; 3Centre for Eye Research Australia, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, Australia; 4Department of Audiology and Speech Pathology, University of Melbourne, Melbourne, Victoria, Australia
*These authors contributed equally to this work
Correspondence: Alexis Ceecee Britten-Jones, Department of Optometry and Vision Sciences, Faculty of Medicine, Dentistry & Health Sciences, the University of Melbourne, Parkville, Victoria, 3010, Australia, Tel +61 3 8344 5980, Email [email protected]
Purpose: Stickler Syndromes are multisystem collagenopathies affecting 1 in 7500– 9000 individuals and are associated with craniofacial, ocular, auditory, and musculoskeletal complications. Prophylactic retinopexy treatment reduces the risk of retinal detachment, emphasising the need for early detection and multidisciplinary referral. This study evaluated knowledge and awareness of Stickler Syndromes among allied health professionals and their perceived needs for targeted education to improve multidisciplinary care.
Methods: A cross-sectional survey was undertaken among audiologists, speech pathologists, optometrists, orthoptists, and physiotherapists in Australia. Survey questions included practitioner demographics, awareness and knowledge of Stickler Syndromes, confidence managing Stickler Syndromes, and perception of multidisciplinary care needs for Stickler Syndromes.
Results: Of 180 healthcare professions who participated (79% female; 78% aged between 25 and 44 years), 55% indicated that they had heard of Stickler Syndrome, and 14% had directly worked with patients known to have Stickler Syndromes. Practitioners who had were either optometrists, orthoptists, or audiologists. The most recognised clinical sign of Stickler Syndromes was retinal detachment (selected by 66% of optometrists and orthoptists and 16% of other professions), but only 41% of optometrists and orthoptists (27% all respondents) selected cryopexy as a potential management strategy. Vitreous anomaly was recognised as a clinical feature by 20% of all respondents. Overall, 69% of allied health professionals did not feel confident managing Stickler Syndromes, and a similar number of practitioners (69%) indicated that they were willing to attend professional development courses for complex conditions such as Stickler Syndromes.
Conclusion: This study provides meaningful insights on awareness and knowledge of Stickler Syndromes among allied healthcare professionals. Targeted clinician education, enhanced communication between healthcare entities, and multidisciplinary care programs can significantly improve the integrated care of Stickler Syndromes leading to better patient outcomes.
Keywords: high myopia, vitreous anomalies, cleft palate, hearing loss, syndromic conditions, clinical education, Stickler Syndrome
Introduction
Stickler Syndrome, also known as hereditary progressive arthro-ophthalmopathy, is a group of multisystem connective tissue disorders affecting 1 in 7500 to 9000 individuals.1 The condition is frequently diagnosed in late childhood to early adolescence, but the onset of symptoms can occur anywhere from birth to over 50 years of age.1
Stickler Syndromes affects collagen proteins that are principally and collectively expressed in the eye and articular and hyaline cartilage, and is associated with a spectrum of ocular, auditory, orofacial and musculoskeletal manifestations, with variable phenotypic expression.1 Key clinical features of Stickler Syndromes are congenital high myopia, retinal detachment, hearing loss (conductive or sensorineural), and premature arthropathy.2,3 Ocular manifestations, which could also include glaucoma and presenile cataracts, are found in about 95% of affected cases.1,2,4 Characteristic craniofacial features of Stickler Syndromes include a flattened facial profile with a depressed nasal bridge, epicanthal folds, cleft palate, and Pierre Robin sequence, which is a triad of micrognathia, glossoptosis, and airway obstruction.1,2,4
Understanding clinical features associated with Stickler Syndromes can assist with diagnosis, but given the phenotypic heterogeneity, genetic testing remains the gold standard.5,6 At least six Stickler Syndrome subgroups have been characterised according to the genetic abnormalities of collagen types affected, including COL2A1 (type 1), COL11A1 (type 2), and COL11A2 (type 3) Stickler Syndrome, associated with autosomal dominant inheritance, and COL9A1 (type 4), COL9A2 (type 5), and COL9A3 (type 6) Stickler Syndrome, associated with autosomal recessive inheritance. COL2A1-related Type 1 Stickler Syndrome is the most common form, accounting for 80–90% of cases,7,8 and frequently presents with membranous vitreous anomaly.9 In contrast, COL11A1-related type 2 Stickler Syndrome accounts for around 20% of cases and is often associated with beaded vitreous abnormaly.10 The non-ocular subtype COL11A2-related Stickler Syndrome and the autosomal recessive forms of Stickler Syndrome (types 4–8) are rarer and less well-characterised.2,11
Early detection of Stickler Syndromes allows for effective clinical management and treatment to address specific symptoms. Orofacial and musculoskeletal abnormalities, which can result in varying degrees of pain and reduced functional ability, may require corrective surgeries, therapy, and/or pharmacological pain management.1,12 Sensorineural hearing loss can be managed through amplification devices, and conductive hearing loss and recurrent otitis media can be managed by ventilation tube insertion or middle ear surgery.7 Some patients may also benefit from individualized speech, feeding, language, physical, and occupational therapy.11 Early detection also enables regular monitoring and prophylactic treatments. Around 40% of individuals with Stickler Syndromes will develop rhegmatogenous retinal detachment,1,13 which, if not detected early, causes severe vision loss. However, Stickler Syndrome diagnosis is often delayed due to a lack of recognition by health care providers, despite 80% of those affected having a positive family history.1,12
Understanding awareness of Stickler Syndromes among primary and allied health care providers can reinforce earlier diagnosis and support multidisciplinary care models.14,15 Only one study has investigated clinician awareness of Stickler Syndrome.16 However, this study presented conflicting data about clinician awareness, reporting that awareness of Stickler Syndrome ranged between 26% and 69% among dental students, and only a single discipline was studied. To date, no studies have investigated knowledge and awareness of Stickler Syndromes among multidisciplinary allied health professionals.
The aim of this study was to investigate knowledge and awareness of Stickler Syndrome among allied health professionals and their perceived need for targeted education to improve the integrated care of Stickler Syndromes.
Materials and Methods
Ethical approval was obtained from University of Melbourne Human Research Ethics Committee (ID: 2023–26376). This study was performed in accordance with the principles of the Declarations of Helsinki; all participants provided informed consent before commencing the survey.
Eligible participants were clinicians in the fields of audiology, optometry, orthoptics, speech pathology, and physiotherapy, who self-reported to be registered with the relevant Australian professional body and practicing in Australia.
Survey Development
The survey was developed by a multidisciplinary team of Doctor of Optometry, Master of Clinical Audiology, and Master of Speech Pathology students at the University of Melbourne who independently reviewed the literature with a focus on their respective professions and drafted preliminary survey questions. Findings were then presented at interprofessional education meetings, and a set of survey questions were developed based on discussion and consensus.
The draft survey was then reviewed by an interdisciplinary expert panel who provided feedback on the relevance and clarity of the questions. The panel consisted of an ophthalmologist (sub-specialising in retina; RD), two optometrists (with specific research interests in interprofessional education (KC) and inherited retinal diseases (LA)), a physiotherapist (with experience in Stickler Syndromes, JM), an audiologist (with educational and clinical expertise in Stickler Syndrome, KG), and two speech pathologists (with expertise in structural and genetic speech impairments, JB & RB).
The final survey comprised 23 questions divided into four sections (Appendix 1):
- Demographics: age, gender, education, profession, clinical experience, primary practice location, and current scope of patient care (adults/pediatrics/both).
- Awareness and knowledge of Stickler Syndromes: multiple choice questions relating to the causes, signs and symptoms, management, as well as previous experience, and education on Stickler Syndrome.
- Confidence managing Stickler Syndromes: self-rated confidence levels (5-point Likert scale) in managing and communicating with patients with Stickler Syndromes, including communicating with patients, resources, referrals, and collaborating with other healthcare professionals.
- Perception of multidisciplinary care and education on Stickler Syndromes: Experiences with multidisciplinary care for Stickler Syndromes and perception of their effectiveness. The survey also included two open-ended questions on what participants think would increase practitioners’ confidence in working with individuals with Stickler Syndromes and what could be done to increase the awareness of Stickler Syndromes.
The final survey was piloted by the research team. The estimated time to complete the survey was 2 to 10 minutes.
Survey Distribution
Survey responses were collected via Qualtrics, a web-based online survey platform hosted at the University of Melbourne, between 12th May and 2nd July 2023.
Participants were recruited via non-random convenience sampling, through professional organizations, social media, and professional networks of the researchers. Participation was anonymous, responses were non-identifiable, and no incentives or feedback were provided.
Statistical Analysis
Statistical analysis was performed using R for statistical consulting (v4.2.2; R Core Team 2022). A sample size was not chosen to detect a pre-specified effect size between specific outcomes. Participants that had only completed the demographics section and no other questions were excluded. All other responses were included up to their last response.
Descriptive methods were used to summarise participant characteristics, presented as the frequency and percentages of responses for categorical measures. Fisher exact test was used for intergroup comparisons. For comparing responses between disciplines, optometrists, and orthoptists were combined into a single group to represent the eye health profession, and physiotherapists (with six respondents) were excluded from the analysis to mitigate disclosure risk. For comparing whether practitioners were likely to consider Stickler Syndrome in their differential diagnosis, responses that were “sometimes”, “often”, or “always”, were combined to represent “likely to consider”, and “rarely”, “never”, or “unsure” were combined to represent “unlikely to consider”.
Qualitative data from open-set responses were analyzed using inductive thematic analysis.17 Six members of the student optometry team developed a coding framework, independently coded the free-text responses, and then discussed the themes to reach a consensus. Data and final themes were checked by an academic staff (KC) to confirm accuracy. Recommendations for improving clinician knowledge and confidence for managing Stickler Syndromes were formulated by the authorship team based on the themes identified.
Results
Practitioner Demographics
Of 180 respondents who participated, 163 respondents completed the entire survey. Participant demographics are shown in Table 1. Respondents included 69 optometrists, 45 audiologists, 31 speech pathologists, 28 orthoptists, and 6 physiotherapists.
 |
Table 1 Participant Demographics |
Most participants were aged between 25 and 44 years (78%); the majority 79% identified as female, 19% as male, and 2% as other, or preferred not to say. Almost all respondents primarily practiced in metropolitan regions (91%); 9% practiced regionally and none were from rural settings.
There was widespread representation of clinical experience, with 20% having three years’ clinical experience or less, 37% with 4–10 years of experience, 25% with 10–20 years of experience, and 18% with over 20 years’ experience. Between professions, a similar number of respondents had less than 10 years’ experience versus 10 years’ experience or more (p = 0.20). Most participants (156, 87%) had undergraduate or postgraduate professional clinical degrees, and 13% had PhDs. For all disciplines, except for speech pathologists, the majority (over 50%) of respondents provided care to both adults and children. For speech pathologists, 58% provided only paediatric care, and 32% for both adults and children.
Awareness and Knowledge of Stickler Syndromes
Among the 180 respondents, 55% (n = 99) indicated that they had heard of Stickler Syndrome. A relatively higher proportion of optometrists and orthoptists (78% of optometrists/orthoptists) and audiologists (46% of audiologists) had heard of Stickler Syndrome, compared to 7% of speech pathologists. Only 14% of all respondents had direct experience working with individuals with Stickler Syndromes, all of whom were either optometrists or orthoptists (12%) or audiologists (2%).
Despite only 55% of respondents knowing what Stickler Syndrome is, 66% of respondents (n = 119) correctly identified that the condition is caused by genetic mutation(s). Nonetheless, there was general agreement across all disciplines (with 82% agreeing) that there is currently a lack of awareness of Stickler Syndromes.
Figure 1 shows the frequency of responses from participants from within each discipline who correctly identified signs associated with Stickler Syndromes (Figure 1A) and management options for Stickler Syndromes (Figure 1B).
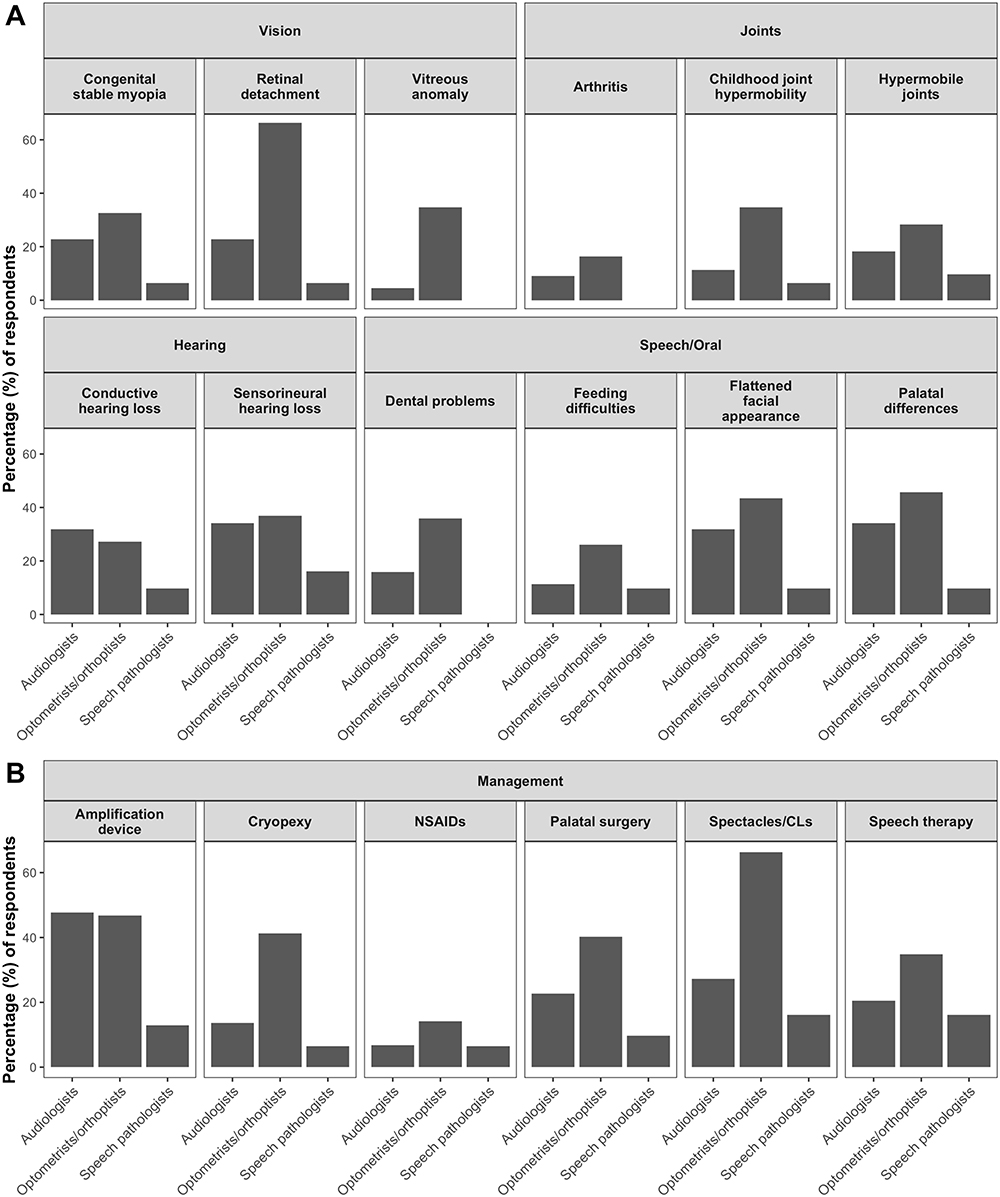 |
Figure 1 Frequency of responses from participants within each discipline who correctly identified (A) signs associated with Stickler Syndromes and (B) management options for Stickler Syndromes. Responses from n=6 physiotherapists were excluded from descriptive summaries. Abbreviations: CLs, contact lenses. |
Among all respondents, 42% indicated that they did not know the clinical signs and symptoms associated with Stickler Syndromes, and 46% did not know the management options for people with Stickler Syndromes. Among clinicians who did, the most well-recognised clinical sign associated with Stickler Syndrome was retinal detachment, selected by 43% of all respondents (66% of optometrists and orthoptists, and 16% of other professions), followed by palatal differences (35% of all respondents), flattened facial appearance (34% of respondents), and sensorineural hearing loss (32% of respondents). The least recognised signs of Stickler Syndrome were arthritis (12% of respondents), feeding difficulties (19% of respondents), and vitreous anomaly (20% of respondents).
Despite retinal detachment being the most well-recognised clinical sign, only 41% of optometrists and orthoptists (27% all respondents) selected cryopexy as a potential management strategy for Stickler Syndromes. Spectacles and contact lenses were indicated as the most common management strategy for Stickler Syndromes (66% of optometrists/orthoptists; 46% across all disciplines), followed by amplification devices (48% of audiologists; 40% across all disciplines).
Figure 2 shows the frequency in which health professionals across different disciplines indicated they would consider Stickler Syndrome in their different diagnosis if an individual presented with an associated symptom. If an individual presented with vitreous abnormalities, 24% of optometrists and orthoptists would consider Stickler Syndrome in their differential diagnosis, compared to 4% from other disciplines (Fisher’s exact test: p = 0.0003). For individuals presenting with a cleft palate, 23% of all respondents indicated that they would consider Stickler Syndrome in their differential diagnosis; none of whom were speech pathologists. There was no difference between audiologists (19%) and other health professionals (22%) in their likelihood to consider Stickler Syndrome as a differential diagnosis if an individual presented with hearing loss (p = 0.83), and 17% of all respondents indicated they would consider Stickler Syndrome if an individual presented with enlarged joints/joint pain.
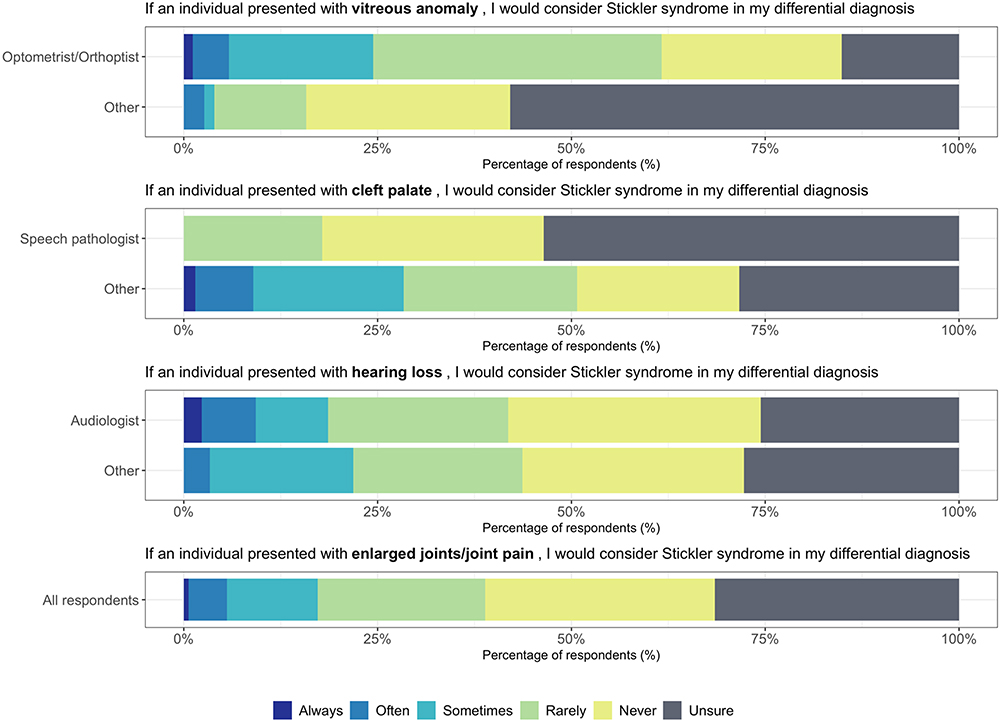 |
Figure 2 Frequency of participant responses on whether they would consider Stickler Syndromes as a differential diagnosis for individuals presenting with associated clinical features (from n=173 respondents). |
Perceptions and Confidence in Managing Stickler Syndrome
Figure 3 shows respondents’ confidence with managing people with Stickler Syndromes. More than half of all respondents (between 51% and 81%) disagreed or strongly disagreed with each statement, indicating a generally low confidence in managing individuals with Stickler Syndromes and participating in multidisciplinary collaboration.
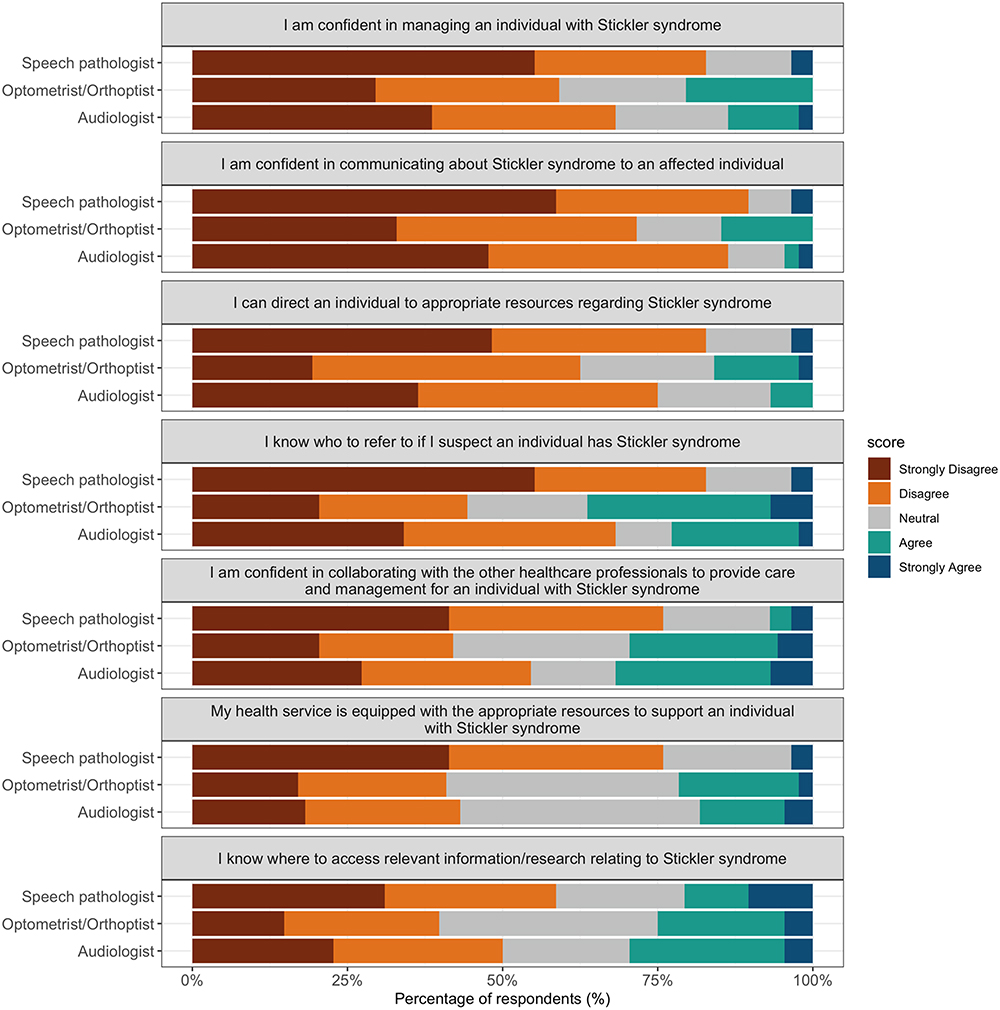 |
Figure 3 Clinicians’ self-reported level of confidence in managing patients with Stickler Syndromes and participating in multidisciplinary care (from n=160 respondents). Responses from n=6 physiotherapists were excluded from the descriptive summaries. |
Across all disciplines, 14% of all respondents agreed or strongly agreed that they felt confident managing individuals with Stickler Syndromes, and 69% disagreed with this statement. Unsurprisingly, practitioners who had experience working with patients with Stickler Syndrome were more likely to indicate that they were confident in managing the condition (60% of practitioners who had experience with Stickler Syndromes agreed and compared to 6% of practitioners who had not or were unsure).
While 9% of respondents felt confident in communicating about Stickler Syndromes to an affected individual, most (81%) did not. Even though 23% of all participants agreed that they know where to access relevant information and research relating to Stickler Syndromes, only 10% indicated that they could direct patients to appropriate resources about Stickler Syndromes.
Regarding multidisciplinary care models, 24% of all respondents agreed that they know who to refer to if they suspect an individual that has Stickler Syndrome, and similar proportion of respondents (23%) felt confident in collaborating with other healthcare professionals to co-manage individuals with Stickler Syndromes. However, most respondents (53%) did not think that their health service is equipped with the appropriate resources to support an individual with Stickler Syndrome.
Multidisciplinary Management and Integrated Care
As shown in Figure 4, respondents identified audiologists, ophthalmologists, and optometrists to be the key professions involved in the primary management of Stickler Syndromes (each selected by over 50% of respondents). Speech pathologists received comparatively less recognition as the seventh most identified profession and was only selected by 23% of participating speech pathologists.
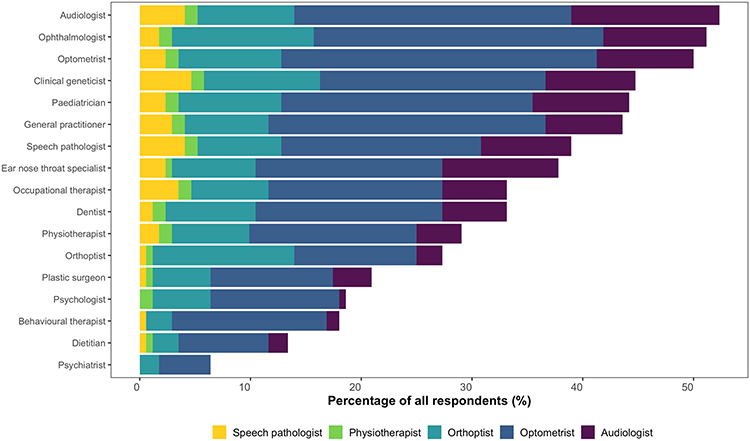 |
Figure 4 Frequency of participant responses on health professionals who would be involved in the primary management of Stickler Syndromes (from n=172 respondents). |
Regarding practitioners’ perception on whether multidisciplinary teams for individuals with Stickler Syndrome work effectively, 66% of all respondents indicated that they have not seen this in practice. Of those who did (34%), half found them to be effective, and the other half were unsure.
Across the cohort, there was consensus from 67% of allied health professionals that their professional training did not prepare them for working with an individual with Stickler Syndrome. No orthoptists, physiotherapists, or speech pathologists felt they had received adequate education on Stickler Syndromes. A similar number of respondents indicated that additional education about complex conditions such as Stickler Syndromes would assist their clinical practice (70%) and expressed willingness to attend additional professional development or educational courses for managing these conditions (69%).
Most respondents (89%) who completed the survey provided open-text responses regarding strategies that could improve individual practitioners’ confidence in working with someone diagnosed with Stickler Syndrome and to increase awareness of the condition. From 145 respondents who provided a response, four educational strategies were identified: 1) Continuing professional development with a focus on multidisciplinary care; 2) Improving accessible clinical resources; 3) Promoting advocacy and public awareness; 4) Integrating into tertiary education, including enhancing clinical exposure and patient experience.
At least one in every four health professionals highlighted continuing professional development and accessible resources as two key areas for prompting confidence and awareness. Based on suggestions by clinicians, Table 2 shows a list of strategies that could be used to promote the integrated care of Stickler Syndromes and other rare multi-system diseases.
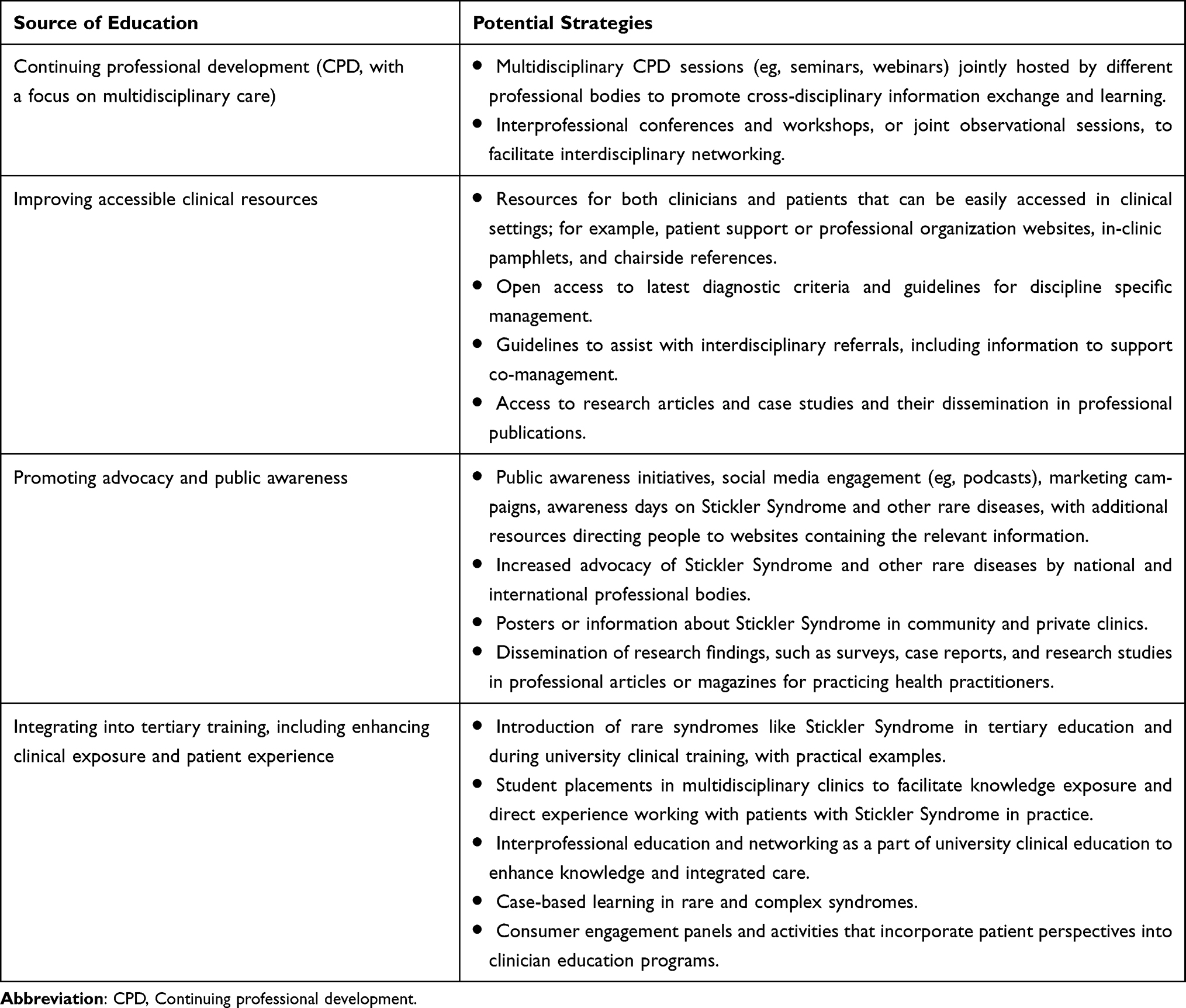 |
Table 2 Suggestions for Improving the Multidisciplinary Management of Stickler Syndrome Based on Open Text Responses |
Discussion
This study investigated knowledge and awareness of Stickler Syndromes among allied health professionals in Australia. We identified low levels of awareness towards recognizing clinical features of Sticker Syndromes and their management, highlighting knowledge needed to improve diagnostic access. To our knowledge, this is the first study to evaluate perspectives of multidisciplinary health professionals towards Sticker Syndromes. Current findings provide insights into areas for targeted professional education and opportunities for enhancing multidisciplinary care.
This study found that while half of the participating health professionals had heard of Stickler Syndrome (55%), only 14% have directly worked with patients with Stickler Syndromes. The awareness of Stickler Syndromes in the current study appears to be lower than that among dental students at an Indian university, where up to 69% had heard of Stickler Syndromes.16 However, the data on awareness from the dental students survey was conflicting, as the authors later stated that 44% of undergraduate and 26% of postgraduate dental students were aware of what Stickler Syndrome was. Moreover, this previous study lacked details on survey design and data collection methods, which limits the interpretation of its findings.
The present study provides novel insights on experiences and perceptions with Stickler Syndromes among multidisciplinary health care providers. Compared to eyecare professionals and audiologists, fewer speech pathologists had heard of Stickler Syndrome, although none of the participating speech pathologists had directly worked with patients with Stickler Syndrome. Patients with Stickler Syndromes are frequently referred to cleft specialist speech pathologists with access to diagnostic methods and equipment that may not be available in all primary care settings.18 Hence, practitioners from other settings may have had fewer opportunities to interact with patients with rarer syndromic conditions associated with cleft palate.
Clinician awareness of Stickler Syndromes (55%) was lower than that of Usher Syndrome (96%) reported in a recent survey of Australian optometrists, orthoptists, and audiologists,19 despite the two conditions having a similar prevalence. Usher syndrome, characterized by dual sensory hearing and vision loss, also requires multidisciplinary care. Notably, the Usher Syndrome study recruited clinicians from within university teaching clinics, whereas the present study aimed to capture a general practicing population. Another reason for this difference could be attributed to their presentations; Usher Syndrome is the most common syndromic condition associated with retinitis pigmentosa and accounts for approximately 50% of deafness-blind cases.20 In contrast, high myopia and cleft palate are more common conditions among the general population, affecting 2–6% of Australian adults,21 and around 1 in 2000 children,22 respectively, but the prevalence of Stickler Syndromes is much lower (around 1 in 7500) and, therefore, could be missed as a differential diagnosis. This finding emphasizes the need to consider syndromic associations and aetiologies, rather than individual phenotypic features in isolation when managing patients.
In addition to clinician awareness, we found that only about half of participating healthcare professionals recognised at least one clinical sign and/or symptom associated with Stickler Syndromes, regardless of their profession. For example, vitreous anomaly in Stickler Syndrome, a predominant ocular feature, was only selected by 34% of optometrists and orthoptists. Given that Stickler Syndrome is a rare disorder, lower levels of knowledge regarding specific clinical features associated with the syndrome is not surprising. However, even though retinal detachment was the most well-recognized feature of Stickler Syndromes (identified by 65% of eye health professionals and 43% of all respondents), few knew that cryopexy is a potential management strategy. Approximately 40% of individuals with Stickler Syndromes are estimated to develop retinal detachments.1,13,23 Prophylactic cryotherapy has been shown to reduce the risk of retinal detachments to around 8%.13,24 LASER retinopexy is another prophylactic treatment for preventing retinal detachment in Stickler Syndromes and preferred by some groups.25 The efficacy of cryotherapy versus LASER retinopexy for preventing retinal detachment in Stickler Syndromes has not been directly compared. Nevertheless, targeted education for eye health professionals on the significance of prophylactic treatment is warranted as it would facilitate timely referrals and significantly improve clinical outcomes, especially for type 1 Sticker Syndrome patients with a higher retinal detachment risk.10
Being a complex multisystem condition, Stickler Syndromes can affect vision, hearing, joints, speech, and oral health; thus, ongoing management requires input from multidisciplinary teams. A challenge lies in the timely detection of Stickler Syndromes and ensuring comprehensive monitoring of all associated symptoms, given its complexity. As highlighted in the present study, there is a need to provide targeted clinician education on the spectrum of signs associated with Stickler Syndromes, and avenues to facilitate interdisciplinary communications and referrals. Furthermore, clinicians who are well-informed about Stickler Syndromes can provide valuable guidance towards genetic testing and counselling for affected individuals and their families, which has a major impact on ongoing clinical management and family planning decisions.26
Australia has a fragmented healthcare system, where affected individuals and families often receive care from healthcare professionals across different settings depending on presentation. A fragmented healthcare system, where different healthcare sectors operate independently, limits opportunities for collaboration and posits a barrier to coordinated care delivery. Addressing these challenges requires a coordinated effort between government and professional bodies, healthcare providers, tertiary and training institutions, and communities. Significant commitment and dedication are required to establish effective collaboration between healthcare entities to implement innovative educational and training programs. A potential solution to address these barriers is establishing multidisciplinary care clinics to improve outcomes for patients with both chronic and complex disorders. An example is the Stickler Highly Specialised Service (implemented by the National Health Service), which has seen over 750 families with Stickler Syndromes since 2011 with over 90% continuing under annual review.3 This has allowed a powerful database to be built for evaluating the long term outcomes of this disorder, which has significant implications for the healthcare system.
We have identified several avenues for targeted clinician education (Table 2), including multidisciplinary professional development, accessible practice guidelines, and advocacy to improve the recognition and diagnosis of Stickler Syndromes and other rarer and complex conditions. Improving clinician knowledge and confidence can help practitioners recognize the spectrum of features associated with Stickler Syndromes, facilitating timely and accurate diagnosis. Interdisciplinary education can enhance clinicians’ confidence in collaborating with other healthcare disciplines enhancing integrated care.27
This study is the first to provide data on allied health practitioners’ perspectives of Stickler Syndromes. A key strength is the inclusion of multidisciplinary allied health professions from different settings who are involved in the diagnosis and management of ocular, orofacial, auditory, and musculoskeletal manifestations of Stickler Syndromes. We deliberately targeted Australian allied primary care health professionals involved in managing symptoms associated with Stickler Syndromes and did not include tertiary medical care providers. Nonetheless, we acknowledge the variability in the roles of primary care professions across different countries, and professionals surveyed in this study may not possess an equivalent scope of practice elsewhere. There was lower representation from speech pathologists and physiotherapists in our dataset. To reduce participation bias, we excluded responses from physiotherapists in cross-disciplinary comparisons. Recruitment was conducted via non-randomized convenience sampling, which may have limited the equitable participation of individuals within the intended population, thus potentially affecting the generalizability of the findings. We aimed to capture a general practicing population and did not limit recruitment based on practice setting; however, respondents working in specialized environments, such as tertiary clinics, are likely to have higher levels of awareness of Stickler Syndromes compared to other settings. Additionally, the voluntary nature of survey participation could have led to self-selection bias, as individuals with prior knowledge of Stickler Syndromes and those with an interest in genetic syndromes may have been more inclined to respond due to their interest or familiarity with the subject, potentially overestimating the level of Stickler Syndrome awareness.
Potential avenues for future research are to investigate awareness and perceptions of Stickler Syndromes among other healthcare professions, such as general practitioners and tertiary care providers. To gain a more in-depth understanding of practices, barriers, and opportunities for improving the multidisciplinary care of Stickler Syndromes, focus group discussions or semi-structured interviews would be beneficial.
Conclusion
This study provides valuable insights on awareness and knowledge of Stickler Syndromes among primary allied healthcare professionals. Across all allied health professions, there was generally under recognition of symptoms associated with Stickler Syndromes and their management, with fewer than 50% of respondents recognizing any of the signs and symptoms associated with Stickler Syndromes. Enhanced awareness of Stickler Syndromes among different allied health care providers could lead to earlier detection, more coordinated multidisciplinary care, and timely referrals to appropriate tertiary medical services; for example, prophylactic retinopexy treatment to prevent retinal detachment. Key knowledge gaps include poor awareness on vitreous abnormalities as an identifying feature of Stickler Syndromes, limited recognition of cryopexy as a prophylactic management strategy to prevent retinal detachments, and minimal exposure of inter-disciplinary referral pathways to provide coordinated care. Targeted education, enhanced efforts to establish collaboration between different healthcare entities, and implementation of innovative multidisciplinary care programs can significantly improve the integrated care of Stickler Syndromes and patient outcomes.
The Stickler Syndrome Study Group
Kar Yee Foh
Jasmine Jade Gregory
Smilla Elizabeth Maccora
Hoi Ching Lydia Ng
Jessica Hanh Nguyen
Leonie Pham
Reina Ann Punnoose
Habiba Qassim
Maya Salinger
Jonathan Brook Simpson
Pranav Sood
Rachele Stin
Kaise Tang
Vindhya Yadlapalli
Veronica Chi Ching Yan
Acknowledgments
We thank Professor Jennifer McGinley for her assistance in piloting the survey and the following professional organisations for their help in distributing of the survey: Optometry Australia, Australian College of Optometry, Centre for Eye Research Australia, Melbourne Teaching Health Clinics, Orthoptics Australia.
Funding
Perth Eye Foundation Grant (RD). University of Melbourne Postdoctoral Research Fellowship (ACBJ). National Health and Medical Research Council Investigator grant (GNT#1195713) and University of Melbourne Driving Research Momentum Fellowship (LNA). The Centre for Eye Research Australia receives operational infrastructure support from the Victorian State government.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stickler GB, Hughes W, Houchin P. Clinical features of hereditary progressive arthro-ophthalmopathy (Stickler syndrome): a survey. Genet Med. 2001;3(3):192–196. doi:10.1097/00125817-200105000-00008
2. Snead MP, McNinch AM, Poulson AV, et al. Stickler syndrome, ocular-only variants and a key diagnostic role for the ophthalmologist. Eye (Lond). 2011;25(11):1389–1400. doi:10.1038/eye.2011.201
3. Snead MP, Richards AJ, McNinch AM, et al. Stickler syndrome - lessons from a national cohort. Eye (Lond). 2022;36(10):1966–1972. doi:10.1038/s41433-021-01776-8
4. O’Brien DA, Phillips AJ. Stickler syndrome. Clin Exp Optom. 2000;83(6):330–332. doi:10.1111/j.1444-0938.2000.tb04921.x
5. Snead MP, JRW Y. Clinical and molecular genetics of Stickler syndrome. J Med Genet. 1999;36(5):353–359. doi:10.1136/jmg.36.5.353
6. Khan AO, AlAbdi L, Patel N, et al. Genetic testing results of children suspected to have Stickler syndrome type collagenopathy after ocular examination. Mol Genet Genomic Med. 2021;9(5):e1628. doi:10.1002/mgg3.1628
7. Acke FRE, Dhooge IJM, Malfait F, De Leenheer EMR. Hearing impairment in Stickler syndrome: a systematic review. Orphanet J Rare Dis. 2012;7(1):84. doi:10.1186/1750-1172-7-84
8. Hoornaert KP, Vereecke I, Dewinter C, et al. Stickler syndrome caused by COL2A1 mutations: genotype–phenotype correlation in a series of 100 patients. Eur J Hum Genet. 2010;18(8):872–880. doi:10.1038/ejhg.2010.23
9. Richards AJ, Laidlaw M, Whittaker J, et al. High efficiency of mutation detection in type 1 stickler syndrome using a two-stage approach: vitreoretinal assessment coupled with exon sequencing for screening COL2A1. Hum Mutat. 2006;27(7):696–704. doi:10.1002/humu.20347
10. Richards AJ, McNinch A, Martin H, et al. Stickler syndrome and the vitreous phenotype: mutations in COL2A1 and COL11A1. Hum Mutat. 2010;31(6):E1461–E1471. doi:10.1002/humu.21257
11. Snead M, Martin H, Bale P, et al. Therapeutic and diagnostic advances in Stickler syndrome. Ther Adv Rare Dis. 2020;1:2633004020978661. doi:10.1177/2633004020978661
12. Webb AC, Markus AF. The diagnosis and consequences of Stickler syndrome. Br J Oral Maxillofac Surg. 2002;40(1):49–51. doi:10.1054/bjom.2001.0747
13. Fincham GS, Pasea L, Carroll C, et al. Prevention of retinal detachment in Stickler syndrome: the Cambridge prophylactic cryotherapy protocol. Ophthalmology. 2014;121(8):1588–1597. doi:10.1016/j.ophtha.2014.02.022
14. Davison N, Payne K, Eden M, et al. Exploring the feasibility of delivering standardized genomic care using ophthalmology as an example. Genet Med. 2017;19(9):1032–1039. doi:10.1038/gim.2017.9
15. Feero WG, Green ED. Genomics education for health care professionals in the 21st century. JAMA. 2011;306(9):989–990. doi:10.1001/jama.2011.1245
16. Yazhini P, Chokkattu JJ, Ramanathan V, G D. Awareness Of Stickler Syndrome Among Dental Students. J Positive School Psych. 2022;6(3):706–717.
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. Karnell MP, Bailey P, Johnson L, Dragan A, Canady JW. Facilitating communication among speech pathologists treating children with cleft palate. Cleft Palate Craniofac J. 2005;42(6):585–588. doi:10.1597/04-130r1.1
19. Ayton LN, Galvin KL, Johansen L, O’Hare F, Shepard ER. Awareness of Usher Syndrome and the Need for Multidisciplinary Care: a Cross-Occupational Survey of Allied Health Clinicians. J Multidiscip Healthc. 2023;16:1927–1936. doi:10.2147/JMDH.S411306
20. Stephenson KAJ, Whelan L, Zhu J, et al. Usher Syndrome on the Island of Ireland: a Genotype-Phenotype Review. Invest Ophthalmol Vis Sci. 2023;64(10):23. doi:10.1167/iovs.64.10.23
21. Mackey DA, Lingham G, Lee SS, et al. Change in the prevalence of myopia in Australian middle-aged adults across 20 years. Clin Exp Ophthalmol. 2021;49(9):1039–1047. doi:10.1111/ceo.13980
22. Vallino-Napoli LD, Riley MM, Halliday J. An epidemiologic study of isolated cleft lip, palate, or both in Victoria, Australia from 1983 to 2000. Cleft Palate Craniofac J. 2004;41(2):185–194. doi:10.1597/02-076
23. Ang A, Poulson AV, Goodburn SF, Richards AJ, Scott JD, Snead MP. Retinal detachment and prophylaxis in type 1 Stickler syndrome. Ophthalmology. 2008;115(1):164–168. doi:10.1016/j.ophtha.2007.03.059
24. Linton E, Jalil A, Sergouniotis P, et al. LASER PROPHYLAXIS IN STICKLER SYNDROME: the Manchester Protocol. Retina. 2023;43(1):88–93. doi:10.1097/IAE.0000000000003634
25. Alexander P, Snead MP. Prevention of Blindness in Stickler Syndrome. Genes (Basel). 2022;13(7):1150. doi:10.3390/genes13071150
26. Britten-Jones AC, Mack HG, Vincent AL, Hill LJ, Edwards TL, Ayton LN. Genetic testing and gene therapy in retinal diseases: knowledge and perceptions of optometrists in Australia and New Zealand. Clin Genet. 2023;105(1):34–43. doi:10.1111/cge.14415
27. van Diggele C, Roberts C, Burgess A, Mellis C. Interprofessional education: tips for design and implementation. BMC Medical Education. 2020;20(2):455. doi:10.1186/s12909-020-02286-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.