")
Back to Journals » Nursing: Research and Reviews » Volume 14
Commentary on the Past, Present, and Future of Nursing Workload Research
Authors MacPhee M, Havaei F , Bookey-Bassett S, Neumann WP , Qureshi SM, Greig MA , Keselman D
Received 30 September 2023
Accepted for publication 17 February 2024
Published 22 February 2024 Volume 2024:14 Pages 59—67
DOI https://doi.org/10.2147/NRR.S442571
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Maura MacPhee,1 Farinaz Havaei,1 Sue Bookey-Bassett,2 W Patrick Neumann,3 Sadeem Munawar Qureshi,3 Michael A Greig,3 David Keselman1
1School of Nursing, University of British Columbia, Vancouver, British Columbia, Canada; 2Daphne Cockwell School of Nursing, Toronto Metropolitan University, Toronto, Ontario, Canada; 3Department of Mechanical and Industrial Engineering, Toronto Metropolitan University, Toronto, Ontario, Canada
Correspondence: Maura MacPhee, School of Nursing, University of British Columbia, T201 2211 Wesbrook Mall, Vancouver, BC, V6T2B5, Canada, Tel +1 778-926-4068, Email [email protected]
Abstract: The aim of this paper is to enhance readers’ understanding of research design strategies, past and present, for studying nursing workloads. Future research directions are also discussed. Nursing workloads are associated with nurse burnout and turnover. During our current global nursing shortage, researchers must identify ways to mitigate nurses’ heavy workloads. Relevant, prior nursing workload research is presented with brief descriptions of designs, methods and findings. To illustrate the current complexity of nurses’ work environments and the myriad factors that influence nurses’ workloads, this paper features the ongoing nursing workload research of two Canadian research teams with different methodological approaches. These two teams are employing current research innovations, such as human factors multi-systems frameworks, design thinking, simulation modeling and integrated knowledge translation. With respect to future research implications, the teams are melding methods and tools to promote a more sophisticated way of understanding the complex linkages between patient needs, systems design and the management of nurses’ workloads.
Keywords: nursing workloads, nurses’ work environments, synergy tool, patient needs assessment, human factors, simulation modeling
Introduction
The aim of this commentary paper is to enhance readers’ understanding of research design strategies for studying nursing workloads. This paper consolidates key learnings from past nursing workload research that most influenced the research direction of the paper’s authors. The current work of two Canadian health services research teams is reported. These teams are currently employing research innovations, such as multi-systems human factors frameworks, design thinking, simulation modeling and integrated knowledge translation. The authors conclude with recommendations for future nursing workload research: research that is vitally important to recruitment and retention of the global nursing workforce.
A Brief Chronological Overview of Nursing Workload Research
Concern about nursing workloads began in the 1990s due to a severe global nursing shortage. Nurse researchers studying factors associated with the nursing shortage found that the quality of the work environment and manageability of workloads were the two primary factors associated with the acute nursing shortage.1 Three decades later, healthcare systems are in the midst of another, severe global nursing shortage.2 Unsurprisingly, the quality of nurses’ work environments and nursing workload management persist as primary factors driving the current nursing shortage.2 Fortunately, ongoing research innovations have enabled researchers to better understand the complexity of factors associated with nurses’ workloads and advanced knowledge translation strategies have provided researchers with the means to foreground evidence of pragmatic use to policymakers and healthcare decision makers. Early foundational nursing research pertaining to nurses’ workloads began with United States (US) and Canadian nurse researchers’ exploration of factors within nurses’ work environments that were positively associated with nurses’ job satisfaction, organizational commitment and intent to stay—requisites for nurse recruitment and retention.3,4 Nurse researchers found that some hospitals had strong recruitment/retention rates during a national nursing shortage in the US, and these hospitals became known as Magnet hospitals due to their magnetic-like attraction for nurses.3,4 In addition to significant, positive associations between Magnet hospital characteristics and better nurse outcomes (eg, increased job satisfaction and intent to stay), US health services researchers demonstrated associations between Magnet hospital characteristics and improved patient outcomes (eg, lower morbidity and mortality rates).5 Lake was one of the first US nurse researchers to develop and validate a practice environment scale-nurse work index (PES-NWI) based on key characteristics of Magnet hospitals.6 There are five major work environment categories included in Lake’s PES-NWI that have been extensively studied for over 2 decades. These five categories are as follows: effective nursing leadership, staff participation in organizational affairs, staffing and resource adequacy, the presence of a nursing model for care delivery (versus medical model), and positive nurse–physician relationships.6
The staffing and resource adequacy category is most closely aligned with nursing workloads.7 Nursing workloads, therefore, are an integral component of nurses’ work environments and one important area of study with respect to nurses’ decisions to stay or leave. The importance of nurses’ workloads was further highlighted by the European Nurses’ Early Exit study that surveyed over 61,000 nurses, reporting that 70% of the sample population identified time pressure from heavy workloads as their main reason for intent to leave their jobs.8 Most recently, the COVID-19 pandemic raised public awareness of nurses’ inability to cope with stressful work environments and unmanageable workloads.9
Further Conceptualizations of Nursing Workload
There are many different ways to conceive of nursing workload. One of the first, basic definitions is the time taken to carry out direct and indirect care, including other activities such as unit/ward management.10 More recent workload conceptualizations include systems design thinking, which considers workload as a byproduct of how systems are organized and coordinated to accommodate nursing care delivery. Design thinking is a collaborative process between researchers and stakeholders who have a vested interest in how a system works. Design thinking uses an iterative process of researcher-stakeholder discussions to better understand stakeholder needs and perspectives about the design and management of a particular system, such as a nursing department or care unit.11,12
Within complex systems, such as nurses’ work environments, there are numerous factors associated with nursing workload such as bed occupancy, the duration and frequency of specific nursing interventions, patient acuity and dependency needs, the size and layout of the unit/ward, and nurse experience and competencies.13,14 Nursing workload research designs have grown more sophisticated in recognizing the factors associated with nursing workloads and consequently, nurse, patient, and organizational outcomes.14
One of the best-known research designs for studying nurses’ workloads within the context of their work environments is the global RN4CAST consortium, which currently includes researchers from the US and over 18 European countries. The consortium is constantly expanding, with recent membership from Latin American researchers.15 The RN4CAST research design was developed to address shortcomings with nursing human resource planning models, such as lack of access to accurate and reliable data.16 A multi-level (eg, hospitals, units) cross-sectional design is used by RN4CAST researchers to collect nurse and patient information via validated survey tools. Organizational profile information is obtained from surveys along with administrative data on patient morbidity and mortality rates. In a seminal paper on RN4CAST, the researchers described how the aim of their design and methods was to improve and enhance nursing workforce forecasting methods while addressing “not only volumes, but quality of nursing staff as well as quality of patient care”.16 Quality of nursing staff goes beyond numbers of nurses to consider nurse education and experience, while quality of care is assessed with nurse survey questions that include seven safety culture questions from the Agency for Healthcare Research and Quality (AHRQ).17
The RN4CAST research has made many contributions to researchers’ appreciation of nurses’ work and its impact on patient outcomes, including patient safety and safety culture. In addition to significant associations between nursing workloads and patient morbidity and mortality, RN4CAST researchers found that as nursing workloads increased, nurses’ capacity to problem solve diminished, resulting in increased potential for patient safety breaches.18 In RN4CAST research, a measure of nursing workload is the number of patients per nurse (ie, nurse-to-patient ratios). In one RN4CAST initiative in 12 European countries, data from 33,000 nurses and 11,000 patients in 500 hospitals between 2009 and 2011 found that an increase in nurses’ workloads by one patient increased the likelihood of an inpatient death by 7%.19
From a research design perspective, the RN4CAST research used some innovative strategies for determining nurses’ workloads.16 Given challenges related to accessing nurse staffing data from hospital and regulatory databases, the researchers used a questionnaire format, for example, to determine nurse-to-patient ratios. Nurses were asked questions about the number of patients they cared for on their last workday, as well as the number of nurses and patients present on their unit or shift. This approach to determining nurse-to-patient ratios was validated by the researchers and has demonstrated how nurse responses to questionnaires can provide useful, reliable data when administrative data are not available or reliable.20–23 RN4CAST research also raised researchers’ awareness of patient-centered care approaches, particularly how patients’ acuity and dependency needs significantly influence nurses’ workloads. RN4CAST researchers were some of the first nurse researchers to foreground how nursing care, first and foremost, must be based on patients’ priority care needs.16
In addition to the global RN4CAST consortium, a team led by Dr. Linda Aiken examined workplace stressors and their impact on nurses and physicians working in top-ranked US Magnet hospitals during the COVID-19 pandemic.24 Surveys were administered to almost 16,000 nurses and 5000 physicians within 60 Magnet hospitals. Although Magnet hospitals are considered gold standard work environments for nurses, both nurse and physician groups reported serious concerns with nurses’ heavy workloads and nurse understaffing during the pandemic, particularly with respect to potential patient adverse events and decreased quality of care.24 The pandemic also opened avenues for nursing workload research in other sectors, especially long-term care (LTC). Nursing workload research has been predominantly focused on acute care settings where most nurses are employed. During and after the COVID-19 pandemic, the LTC sector began to garner nursing research attention due to tragic resident outcomes, in many cases due to inadequate nursing resources.25
Current Nursing Workload Research from Two Canadian Research Teams
The authors of this paper represent research teams from the University of British Columbia (UBC)-Vancouver (MacPhee, Havaei, Keselman) and Toronto Metropolitan University (TMU) (Bookey-Bassett, Neumann, Qureshi and Greig). Brief descriptions follow that describe how current research from these teams has built upon previous nursing workload research.
The UBC Research Team
The UBC research team has been using the RN4CAST research design as a springboard for conceptualization, measurement and interpretation of nursing workload. The UBC team has also been influenced by Kalisch et al,26,27 Ball et al,28,29 and Holden.30 In prior research, Kalisch et al in the US and Ball et al in the UK explored missed care or care left undone as a useful means of assessing nurses’ capacity to manage their workloads. There are 13 essential nursing care interventions that include patient surveillance, pain management, medication delivery and emotional care (eg, comforting and talking with patients).28 Ball et al used nurse staffing levels, as measured by nurse-to-patient ratios, as a proxy for workload. They found that missed nursing care mediated the relationship between nurse staffing (ie, nurses’ workloads) and potential for patient mortality.28 Ball et al concluded that measuring missed care may provide an “early warning” indicator of higher risk for poor patient outcomes28. Consequently, the UBC team has been including missed care questions and RN4CAST survey questions in their nursing workload research.
An additional direction for the UBC team research has been the use of a human factors patient safety framework from Carayon31 with adaptations by Holden.30 The UBC team used Holden’s variant of a human factors conceptual framework to explore nurses’ workloads at unit, job, and task levels. Their 2017 paper32 provides details on how workload was conceptualized and operationalized at each level. Seven workload factors were investigated: Unit-level nurse-to-patient ratios and patient acuity and dependency; job-level nurse perceptions of heavy workloads, compromised professional nursing standards and missed care; and task-level interruptions. Nurse survey questions were used to measure nursing workload outcomes: job satisfaction32 and emotional exhaustion, an indication of burnout.33 The patient workload outcomes were also determined via nurse survey reports of three patient adverse events: medication errors, falls, and hospital-acquired infections.16 In addition to the importance of missed care as a potential mediating mechanism between nurses’ workloads and nurse/patient outcomes, this 2017 study identified compromised nursing standards as another potential mediator. When nurses report that their workloads are compromising their professional standards and code of ethics, there is increased potential for burnout and moral distress.34,35 Based on these research findings, the UBC team recommended that these two mediators, missed care and compromised nursing standards, should serve as a “litmus test” for unmanageable nurses’ workloads.32
In their 2017 study, the UBC team also introduced a new research approach for determining patient acuity and dependency needs.32 An earlier nursing workload study by Upenieks et al influenced their thinking about patient care needs.36 The Upenieks et al study was conducted on similar telemetry units in the same hospital with similar patient populations (eg, age, diagnosis), nurse-to-patient ratios (ie, 1:3), nursing expertise and non-nursing supports. Despite the close matching of factors that influence nurse workloads, there were patient-specific needs that created significant variability in how nurses spent their time delivering patient care. To address how patient needs influence nurses’ workloads, the UBC team used a patient characteristic assessment tool, known as the Synergy tool, to obtain more granular nurse assessments of their patients’ care needs. The Synergy tool is derived from a conceptual model, the Synergy Model™, which postulates that patient needs must be assessed before making nurse assignments to ensure a “fit” between patient needs and nurse competencies.37 Given the understaffing and workload issues associated with the pandemic in LTC, the UBC team recently conducted a nursing workload study in the LTC sector: Resident needs were measured using the Synergy tool, and innovative research visualization strategies were employed to show acuity and dependency needs for individual residents and for different LTC units over time.38 Key findings were that resident needs can vary considerably over a shift—resident needs are not stable. On some resident units, acuity needs were similar to senior care needs on acute care medical-surgical units, signifying the need for more professional nursing staff versus unregulated care assistants. Use of the Synergy tool may also have influenced staff awareness of residents at high risk for falls, as there was a trend for decreased falls over the length of the study.38
The TMU Research Team
The TMU team is anchored in the Human Factors Engineering (HFE) Lab at TMU with members spanning the disciplines of industrial engineering, nursing, design science, and human factors. The discipline (and science) of human factors aims to apply knowledge about humans to the design of systems in order to improve both system performance and human wellbeing.39 The HFE Lab conducts research on how to design work systems, such as healthcare systems, in ways that provide high quality work environments where employees can be productive and deliver quality in their work in a sustainable way. The HFE lab work environment definition includes all aspects of the design and management of the workplace that affects employee workloads and wellbeing.40 This definition includes attention to the perceptual, cognitive, physical, and psychosocial (emotional) demands of the work. If these demands exceed a given nurse’s capabilities, there will be negative effects on the individual’s wellbeing (including fatigue, discomfort, injury, and burnout) and subsequent work performance compromise—in this case the quality and quantity of care delivered to patients. The “Better Work, Better Care” conceptual framework, as illustrated in Figure 1, depicts these relationships.40 The key drivers of nursing workload are based on the design of the care system (eg, patient care unit) including the physical system layouts, location of supplies, care routines and policies, patient bed assignments and patient acuity and dependency needs. This conceptual approach to nursing workload also considers task performance times and the perceptual, cognitive, physical, and emotional demands placed on nurses while performing these tasks (ie, the “amplitude dimension” of workload in human factors terms). The challenge faced by healthcare system designers and managers is that there are few quantitative measures of nursing workload, as defined by human factors engineers, which are sensitive to the specific design and operational conditions of the healthcare unit in question.
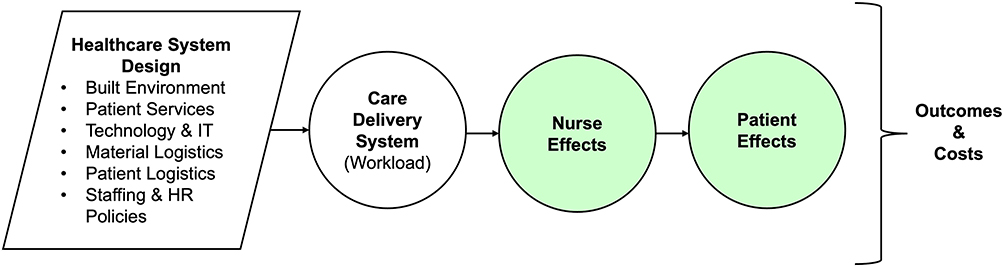 |
Figure 1 Conceptual model illustrating the design stage determinants of nursing workload with consequent effects for nurses, patients and organizations. |
The TMU team has been using simulation modeling tools, such as system dynamics modeling and discrete event simulation (DES), to help isolate the specific job design drivers of nursing workload at different systems levels. These tools allow for the integration of available evidence and information about a specific unit in question, and they also generate scientific evidence regarding the effects these demands have on nurse and patient outcomes. Healthcare unit models can be used to isolate and quantify the impacts of specific design features or elements, providing decision makers with insights on sources of problems and potential effects of changes in the system. Farid et al, for example, used system dynamics modeling to examine the effects of changes in staffing policies on fatigue-driven burnout and error-making rates.41 This study showed that both longer work hours and longer work weeks increased nurse burnout rates by 600%, absenteeism by 500%, and medical errors by 150%. The novelty of this approach is that evidence can be tuned and applied to conditions for a specific site context. In other words, general scientific knowledge can be contextualized to apply to a given decision-maker’s system design to give case-specific quantification of workload and related outcomes. These kinds of simulation tools have been used as decision supports that allow for testing and comparing policy alternatives.42 While these system dynamics models provide high-level policy analysis tools, they are not as good at examining specific operational design choices. Discrete event simulation allows for more granular, task-by-task analysis.43
Discrete event simulation is a common and commercially available tool in industrial engineering. The TMU team is using DES to create models of nursing work that are based on the actual unit conditions to understand the relationship between system design, workload, and effects on simulant nurses and patients. The current approach to DES uses measures corresponding to 1) physical layout of the care unit including geographic patient assignments, 2) a distribution of care task frequencies according to patient acuity and dependency needs, 3) a distribution of individual task times obtained either from institutional standards or time and motion studies, and 4) nurse caregiving logics including the travel path for carrying out tasks and task priorities (ie, how the simulant nurse will choose which task to do next). With these inputs, the DES tool can map simulant nurses’ task-by-task activity patterns for entire shifts based on a specific scenario. The DES approach can also provide specific time utilization information with respect to shift-long nursing workloads/assignments.43–45 Outputs from the model include factors such as nurse walking distance, time spent in each type of care task, number of tasks completed, the time it takes for a task to be completed (ie, task waiting time), the number of tasks waiting “in queue” that the nurse must keep in mind, and the number of tasks that remain to be done at the end of the programmed shift (ie, missed care). This modeling approach was validated in an acute care setting comparing model walking distances to actual measured distances under different patient assignment scenarios.45
The TMU-DES model above was extended and validated to examine pandemic impacts and associated infection control routines on nurse workload from COVID-19.46 It was observed that simulant nurses in a medical-surgical unit with five COVID-19 positive patients had to don and doff personal protective equipment (PPEs) over 100 times or the equivalent to about six hours in a 12-hour shift. The donning and doffing of PPE caused delays in care delivery and missed care increased by up to 140 tasks per 12-hour shift. This delay also increased nurses’ mental/cognitive workloads.46
The systems design and simulation modeling approaches to nursing workload hold promise as ways to reduce missed care while optimizing nurses’ effectiveness and efficiency during direct and indirect care delivery.47 In one TMU team simulation study on missed care, as nurse-to-patient ratios increased, there was a linear increase in missed care by shift’s end. In some scenarios, over 115 tasks were uncompleted by the end-of-shift.47 Similarly, geographical patient bed assignments were shown to affect missed care rates—with more distal and more distributed assignments having higher missed care rates.48 There were also increases in missed care based on patient acuity.48 This body of research complements research findings from the UBC team: Missed nursing care may be a proxy for excess workload due to inadequate systems design and workload management decisions.47,48
Collaborations
Recently, a collaboration between the TMU-UBC teams resulted in competitive planning grant funding to talk with healthcare stakeholders about nursing workload management. The teams’ nursing workload research findings were shared with key Canadian decision makers in healthcare administration, non-profit organizations, and government agencies. The teams’ aim was to discuss uptake and application of their research findings with stakeholders at different systems levels. These conversations revealed a significant lack of current workload management guidelines and protocols to guide nursing resource allocation and system design decision-making. Managers and decision makers within the Canadian healthcare system described “flying blind” due to a lack of clearly established quantitative workload indicators.
To address identified gaps in nursing workload management, the TMU-UBC team is currently collaborating with cross-jurisdictional stakeholders to combine Synergy tool use with simulation modeling; a research innovation that will address data-driven nursing workload in ways that are sensitive to person-centered, holistic patient needs. In this collaboration, direct care nurses will be using the Synergy tool to assess their patients’ acuity and dependency needs, and their Synergy scores will become a key input for nursing workload simulation modeling. Use of nurse Synergy scores will help decrease research resources used in past simulation work to derive input data on patient care needs from administrative databases using diagnostic-related groups.
The TMU-UBC research team collaborations have included another important research innovation—the voice of stakeholders (also known as knowledge users in the knowledge translation literature). Participatory action research and design thinking are both stakeholder-inclusive methods these teams have used in their research programs. A new knowledge translation strategy, integrated knowledge translation or iKT, is currently being employed by the teams to ensure stakeholder engagement in every phase of research design, implementation, evaluation, knowledge translation to policy and practice and further research innovation.49–51 Just as research methods evolve to better understand complex systems, researchers must also be comfortable engaging with new strategies to engage individuals and groups with lived experience.49 Integrated knowledge translation ensures that stakeholders with lived experience are actively involved in every phase of the research process—from the co-development of research questions to interpretation and application of research findings.50 The iKT approach increases utilization of research findings and researchers and stakeholders report enhanced awareness of each other’s knowledge and skills. Researchers also acquire a better appreciation of facilitators and barriers associated with policy and practice in healthcare settings, while stakeholders acquire data that increases their capacity to make more objective design and management determinations that improve nurse, patient and organizational outcomes.49–51
Future Directions
Current research designs discussed above (eg, system design thinking, simulation modeling, iKT) promote exploration of factors that most influence nursing workload within a system and at more granular levels (eg, unit/ward)—producing evidence to inform care delivery improvement. These approaches require the collaboration of stakeholders at different system levels, including decision makers, managers, direct care nurses and patients and their families. As always, model veracity is bounded by the “garbage in – garbage out” rule of simulation modeling: Accurate data inputs matter. Current models are deficient, for example, in capturing nurse perspectives of patient acuity and dependency needs. In most instances, patient needs are crudely captured by administrative data on diagnostic categories. Collaborations between research teams using the Synergy tool and simulation modeling will hopefully shed light on future research directions. Immediate future directions for the TMU-UBC research teams will also involve research-practice-policy collaborations to determine how information about nurses’ workloads should be taken up across the Canadian healthcare system: This will include unit-level operations, institutional quality improvement and data management processes and governance-level decisions about system designs.
Conclusion
The contemporary landscape of healthcare delivery stands at a pivotal juncture characterized by a worldwide shortage of nurses. The severity of this human resource scarcity necessitates a meticulous examination of factors contributing to the shortage. Historically, health services researchers, exemplified by the RN4CAST consortium,15 have studied nurses’ work environments extensively, with nursing workloads being a focal element. Heavy nursing workloads and another important focus of study, missed nursing care, are associated with adverse outcomes, such as nurse burnout and turnover.1,2,28,29 Collaborative innovations, such as those orchestrated by the TMU-UBC research teams, have effectively built upon prior research evidence while offering potential research directions for unraveling the complexity of nursing workloads. As exemplified by iKT, research-generated knowledge must include stakeholders’ collaboration during the development, dissemination and uptake of new, evidence-informed practices and policies across all levels of healthcare systems.
Abbreviations
AHRQ, Agency for Healthcare Research and Quality; DES, discrete event simulation; HFE, Human Factors Engineering; iKT, integrated knowledge translation; LTC, long-term care; PES-NWI, practice environment scale-nurse work index; PPE, personal protective equipment; TMU, Toronto Metropolitan University; UBC, University of British Columbia; UK, United Kingdom; US, United States.
Disclosure
Dr Michael Greig reports grants from Natural Sciences and Engineering Research Council of Canada, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Duffield C, O’Brien-Pallas L. The causes and consequences of nursing shortages: a helicopter view of the research. Aust Health Rev Publ Aust Hosp Assoc. 2003;26(1):186–193. doi:10.1071/ah030186
2. Drennan VM, Ross F. Global nurse shortages-The facts, the impact and action for change. Br Med Bull. 2019;130(1):25–37. doi:10.1093/bmb/ldz014
3. Aiken LH, Sochalski J, Lake ET. Studying outcomes of organizational change in health services. Med Care. 1997;35(11):NS6–NS18.
4. Laschinger HKS, Shamian J, Thomson D. Impact of magnet hospital characteristics on nurses’ perceptions of trust, burnout, quality of care, and work satisfaction. Nurs Econ. 2001;19(5):209–219.
5. Aiken LH, Smith HL, Lake ET. Lower medicare mortality among a set of hospitals known for good nursing care. Med Care. 1994;32(8):771–787.
6. Lake ET. Development of the practice environment scale of the nursing work index. Res Nurs Health. 2002;25(3):176–188. doi:10.1002/nur.10032
7. Griffiths P, Saville C, Ball J, Jones J, Pattison N, Monks T. Nursing workload, nurse staffing methodologies and tools: a systematic scoping review and discussion. Int J Nurs Stud. 2020;103:103487. doi:10.1016/j.ijnurstu.2019.103487
8. Estryn-Behar M, van der Heijden BIJM, Fry C, Hasselhorn HM. Longitudinal analysis of personal and work-related factors associated with turnover among nurses. Nurs Res. 2010;59(3):166. doi:10.1097/NNR.0b013e3181dbb29f
9. Havaei F, Ma A, Staempfli S, MacPhee M. Nurses’ workplace conditions impacting their mental health during COVID-19: a Cross-Sectional Survey Study. Healthcare. 2021;9(1):84. doi:10.3390/healthcare9010084
10. Needham J. Accuracy in workload measurement: a fact or fallacy? J Nurs Manag. 1997;5(2):83–87. doi:10.1046/j.1365-2834.1997.00250.x
11. Neumann WP, Kolus A, Wells RW. Human factors in production system design and quality performance – a systematic review. IFAC Pap. 2016;49(12):1721–1724. doi:10.1016/j.ifacol.2016.07.830
12. Siirala E, Tuominen O, Salanterä S. Using design thinking in nursing management and leadership. In: Pakarinen A, Lemström T, Rainio E, Siirala E, editors. Design Thinking in Healthcare: From Problem to Innovative Solutions. Springer International Publishing; 2023:79–90. doi:10.1007/978-3-031-24510-7_6
13. Alghamdi MG. Nursing workload: a concept analysis. J Nurs Manag. 2016;24(4):449–457. doi:10.1111/jonm.12354
14. Saville CE, Griffiths P, Ball JE, Monks T. How many nurses do we need? A review and discussion of operational research techniques applied to nurse staffing. Int J Nurs Stud. 2019;97:7–13. doi:10.1016/j.ijnurstu.2019.04.015
15. UPenn Nursing Center for Health Outcomes and Policy Research. RN4CAST international studies. Center for Health Outcomes and Policy Research, University of Pennsylvania Nursing; 2023. Available from: https://www.nursing.upenn.edu/chopr/rn4cast/.
16. Sermeus W, Aiken LH, Van den Heede K, et al. Nurse forecasting in Europe (RN4CAST): rationale, design and methodology. BMC Nurs. 2011;10(1):6. doi:10.1186/1472-6955-10-6
17. AHRQ. Hospital survey on patient safety culture. AHRQ Agency for Healthcare Research and Quality; 2013. Available from: https://www.ahrq.gov/patient-safety/resources/index.html.
18. Sermeus W. Understanding the role of nurses in patient safety: from evidence to policy with RN4CAST. BMC Nurs. 2016;15:1.
19. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W; RN4CAST Consortium. Nurses’ reports of working conditions and hospital quality of care in 12 countries in Europe. Int J Nurs Stud. 2013;50(2):143–153. doi:10.1016/j.ijnurstu.2012.11.009
20. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987–1993. doi:10.1001/jama.288.16.1987
21. Aiken LH, Clarke SP, Cheung RB, Sloane DM, Silber JH. Educational levels of hospital nurses and surgical patient mortality. JAMA. 2003;290(12):1617–1623. doi:10.1001/jama.290.12.1617
22. Kutney-Lee A, McHugh MD, Sloane DM, et al. Nursing: a key to patient satisfaction. Health Aff. 2009;28(Supplement 3):w669–w677. doi:10.1377/hlthaff.28.4.w669
23. Rafferty AM, Clarke SP, Coles J, et al. Outcomes of variation in hospital nurse staffing in English hospitals: cross-sectional analysis of survey data and discharge records. Int J Nurs Stud. 2007;44(2):175–182. doi:10.1016/j.ijnurstu.2006.08.003
24. Aiken LH, Lasater KB, Sloane DM, et al. Physician and nurse well-being and preferred interventions to address burnout in hospital practice: factors associated with turnover, outcomes, and patient safety. JAMA Health Forum. 2023;4(7):e231809. doi:10.1001/jamahealthforum.2023.1809
25. Hoedl M, Thonhofer N, Schoberer D. COVID-19 pandemic: burdens on and consequences for nursing home staff. J Adv Nurs. 2022;78(8):2495–2506. doi:10.1111/jan.15193
26. Kalisch BJ, Landstrom GL, Hinshaw AS. Missed nursing care: a concept analysis. J Adv Nurs. 2009;65(7):1509–1517. doi:10.1111/j.1365-2648.2009.05027.x
27. Kalisch BJ, Xie B, Dabney BW. Patient-reported missed nursing care correlated with adverse events. Am J Med Qual. 2014;29(5):415–422. doi:10.1177/1062860613501715
28. Ball JE, Murrells T, Rafferty AM, Morrow E, Griffiths P. “Care left undone” during nursing shifts: associations with workload and perceived quality of care. BMJ Qual Saf. 2014;23(2):116–125. doi:10.1136/bmjqs-2012-001767
29. Ball JE, Bruyneel L, Aiken LH, et al. Post-operative mortality, missed care and nurse staffing in nine countries: a cross-sectional study. Int J Nurs Stud. 2018;78:10–15. doi:10.1016/j.ijnurstu.2017.08.004
30. Holden RJ, Scanlon MC, Patel NR, et al. A human factors framework and study of the effect of nursing workload on patient safety and employee quality of working life. BMJ Qual Saf. 2011;20(1):15–24. doi:10.1136/bmjqs.2008.028381
31. Carayon P, Hundt AS, Karsh BT, et al. Work system design for patient safety: the SEIPS model. BMJ Qual Saf. 2006;15(suppl 1):i50–i58. doi:10.1136/qshc.2005.015842
32. MacPhee M, Dahinten VS, Havaei F. The impact of heavy perceived nurse workloads on patient and nurse outcomes. Adm Sci. 2017;7(1):7. doi:10.3390/admsci7010007
33. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag. 2009;17(3):331–339. doi:10.1111/j.1365-2834.2009.01004.x
34. Atashzadeh-Shoorideh F, Tayyar-Iravanlou F, Chashmi ZA, Abdi F, Cisic RS. Factors affecting moral distress in nurses working in intensive care units: a systematic review. Clin Ethics. 2021;16(1):25–36. doi:10.1177/1477750920927174
35. Lamiani G, Borghi L, Argentero P. When healthcare professionals cannot do the right thing: a systematic review of moral distress and its correlates. J Health Psychol. 2017;22(1):51–67. doi:10.1177/1359105315595120
36. Upenieks VV, Kotlerman J, Akhavan J, Esser J, Ngo MJ. Assessing nursing staffing ratios: variability in workload intensity. Policy Polit Nurs Pract. 2007;8(1):7–19. doi:10.1177/1527154407300999
37. Curley MAQ. Synergy: The Unique Relationship Between Nurses and Patients, the AACN Synergy Model for Patient Care. Sigma Theta Tau International; 2007.
38. Havaei F, Kobekyaa F, Ma A, et al. A mixed methods study to implement the synergy tool and evaluate its impact on long-term care residents. Healthcare. 2023;11(15):2187. doi:10.3390/healthcare11152187
39. IEA Council. Definition and Domains of Ergonomics. International Ergonomics Association; 2021. Available from: https://iea.cc/about/what-is-ergonomics/.
40. Neumann WP, Purdy N. The better work, better care framework: 7 strategies for sustainable healthcare system process improvement. Health Syst. 2023;1–17. doi:10.1080/20476965.2023.2198580
41. Farid M, Purdy N, Neumann WP. Using system dynamics modelling to show the effect of nurse workload on nurses’ health and quality of care. Ergonomics. 2020;63(8):952–964. doi:10.1080/00140139.2019.1690674
42. Rouse WB, Naylor MD, Yu Z, et al. Policy flight simulators: accelerating decisions to adopt evidence-based health interventions. J Healthc Manag Am Coll Healthc Exec. 2019;64(4):231–241. doi:10.1097/JHM-D-18-00114
43. Qureshi SM, Purdy N, Mohani A, Neumann WP. Predicting the effect of nurse–patient ratio on nurse workload and care quality using discrete event simulation. J Nurs Manag. 2019;27(5):971–980. doi:10.1111/jonm.12757
44. Qureshi SM, Purdy N, Neumann WP. Development of a methodology for healthcare system simulations to quantify nurse workload and quality of care. IISE Trans Occup Ergon Hum Factors. 2020;8(1):27–41. doi:10.1080/24725838.2020.1736692
45. Qureshi SM, Purdy N, Neumann WP. Developing a modelling approach to quantify quality of care and nurse workload — field validation study. Oper Res Health Care. 2021;29:100301. doi:10.1016/j.orhc.2021.100301
46. Qureshi SM, Bookey-Bassett S, Purdy N, Greig MA, Kelly H, Neumann WP. Modelling the impacts of COVID-19 on nurse workload and quality of care using process simulation. PLoS One. 2022;17(10):e0275890. doi:10.1371/journal.pone.0275890
47. Neumann WP, Qureshi SM, Bookey-Bassett S. Computer models in healthcare shed light on the roots of missed care in system design: nurse workload. J Adv Nurs. 2023. doi:10.1111/jan.15870
48. Qureshi SM, Purdy N, Neumann WP. A computerized model quantifying the impact of geographical patient-bed assignment on nurse workload and quality care. Nurs Econ. 2021;39(1):23.
49. Gagliardi AR, Berta W, Kothari A, Boyko J, Urquhart R. Integrated knowledge translation (IKT) in health care: a scoping review. Implement Sci. 2016;11(1):38. doi:10.1186/s13012-0155
50. Jull J, Giles A, Graham ID. Community-based participatory research and integrated knowledge translation: advancing the co-creation of knowledge. Implement Sci IS. 2017;12:150. doi:10.1186/s13012-017-0696-3
51. Dunn SI, Bhati DK, Reszel J, Kothari A, McCutcheon C, Graham ID. Understanding how and under what circumstances integrated knowledge translation works for people engaged in collaborative research: metasynthesis of IKTRN casebooks. JBI Evid Implement. 2023;21(3):277. doi:10.1097/XEB.00000000000003676-0399-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.