")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Comparing the Utility of Landmark-Palpation Guided to Ultrasound-Guided Teaching Methodologies for Subclavian Central Venous Access Using a Formalin-Embalmed Cadaver Model
Authors Lundgreen Mason N , Thomas R, Skidmore C, Loveless B , Muir M, Limov A, Fritsch A, Yancey T, Zapata I, Nigh A
Received 8 September 2023
Accepted for publication 16 November 2023
Published 23 November 2023 Volume 2023:14 Pages 1327—1337
DOI https://doi.org/10.2147/AMEP.S439243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Nena Lundgreen Mason,1 Rebecca Thomas,2 Chad Skidmore,2 Bosten Loveless,2 Maxton Muir,2 Abigail Limov,2 Alexa Fritsch,2 Taylor Yancey,2 Isain Zapata,3 Andrew Nigh2
1Geisel School of Medicine at Dartmouth, Hanover, NH, 03755, USA; 2Rocky Vista University College of Osteopathic Medicine – Southern Utah, Ivins, UT, 84738, USA; 3Rocky Vista University College of Osteopathic Medicine – Colorado, Parker, CO, 80134, USA
Correspondence: Nena Lundgreen Mason, 1 Rope Ferry Road, Hanover, NH, 03755, USA, Email [email protected]
Background: Low-risk and realistic simulation strategies are needed to train clinical learners to perform hands-on invasive procedures. This follow-up study compares the utility of landmark-guided palpation-based to ultrasound-guided teaching techniques for subclavian central venous access using formalin-embalmed cadavers.
Methods: The subclavian veins of 3 cadavers were imaged with ultrasound to evaluate vein patency before palpation-based venous access was attempted. Twenty-three first-year medical students were trained to access the subclavian vein using palpation-based techniques. Training involved ten minutes of didactic orientation and ten minutes of hands-on practical instruction using cadavers. Participant confidence was measured using a 10-point Likert scale on pre- and post-training questionnaires. Objective skills testing for each participant included quantifying the number of skin punctures and recording the time elapsed from first skin puncture to fluid flashback into the syringe. Data was analyzed using a generalized linear model (GLM) approach.
Results: Participant confidence significantly increased following training in both ultrasound and palpation training groups across all questionnaire items (P< 0.001). The ultrasound group had fewer skin punctures (P< 0.001) and fewer failures (1) than the palpation group (6). Participants in the ultrasound group were more confident than those in the palpation group in their ability to locate the vein and select the optimal site for needle access (P< 0.05).
Conclusion: Formalin-embalmed cadavers provide a safe, stress-free, and effective means by which to train students in subclavian vein access using both palpation and ultrasound-based techniques. Repeated practice accessing and aspirating fluid from a cadaveric subclavian vein significantly increases trainee confidence, an essential factor in physician performance that may lead to fewer complications. Introducing this type of low-risk and hands-on practice may be beneficial for trainees before they attempt subclavian vein access on live patients.
Keywords: education, medical, catheterization, central venous, landmark-guided central venous access, ultrasound-guided central venous access, formalin embalmed cadaver
Introduction
Central venous catheterization is used regularly for temporary and permanent venous access. Depending on the clinical scenario, several different access points may be used for this procedure, including the internal jugular, subclavian, and femoral veins.1 The most common access point is the internal jugular vein due to ease of accessibility.2 A review of these various access points has shown few differences in complication rates. Although slightly more difficult to place, subclavian vein central venous catheters have been associated with less risk of central venous catheter-associated bloodstream infection and subsequent sepsis.3,4
Chest X-ray and intracavitary ECG are commonly used clinically to verify or guide correct central venous catheter placement.5–7 Ultrasound (US) is another method that can be used to guide venous access and confirm the correct placement of a central venous catheter.8 Moreover, it is safer, less expensive, and faster than obtaining a chest x-ray.8,9 The Accreditation Council for Graduate Medical Education has established the importance of US guidance and requires a minimum of 20 central venous catheter placements during an emergency medicine residency.10 For most trainee resident physicians, US-guided central venous catheter placement results in fewer complications and faster cannulation than palpation-based techniques.11,12 There is currently no standardized or specific timeline for learning central venous catheter placement in undergraduate medical school curricula.13,14 Trainee residents are typically taught this skill during their first year of residency, although some medical schools have begun training during fourth-year clinical rotations.15 Despite this shift, residents continue to demonstrate a lack of confidence when performing invasive procedures.16 The current pedagogy consists of apprenticeship-style learning on live patients without skills standardization or assessment.17 Consequently, recent medical school graduates report insufficient exposure to invasive procedures such as central venous access.18
Some residency programs have adopted simulation-type training to teach invasive procedures using synthetic models. These models provide a low-risk learning environment for simulated practice but are costly and fall short of representing human tissues and anatomy accurately.19 When evaluating procedures such as intubation, lumbar puncture, central venous catheter placement, and thoracentesis, healthcare professionals who trained on human cadavers performed better to those trained on synthetic models.20 Fresh and soft-embalmed cadavers are highly accurate anatomically and sonographically, however, cost and inaccessibility have proven to be challenging impediments to their widespread utilization.21–23 Formalin-embalmed cadavers, which are widely used for anatomical education, may provide a useful alternative to synthetic models and other types of cadaveric specimens while preserving anatomic, tactile, and sonographic accuracy.24
Although there are many benefits to using formalin-embalmed cadavers in medical education, there exist some obstacles to using them in US-guided procedure training. The desiccated nature of formalin-embalmed tissue often negatively impacts sonographic image quality.24,25 When considering vascular access in a formalin-embalmed cadaver, the embalming process causes fluid to form inside the vessels which is a different consistency than blood in a live patient. This fluid is a mixture of blood and embalming fluid. The embalming process itself can also have highly variable effects on blood vessel size due to variability in clotting.26
This follow-up study presents data that builds upon our prior work that shows that formalin-embalmed cadavers are a useful tool in teaching US-guided subclavian venous access.27 This present study compares the relative utility of palpation-based and US-guided training techniques to teach central venous catheterizations in the subclavian vein. This study aims to determine if formalin-embalmed cadavers are an effective training tool for teaching trainees using both types of central venous access techniques.
Materials and Methods
Setting and Population
This single center observational study was conducted at Rocky Vista University College of Osteopathic Medicine (RVUCOM) in Ivins, Utah following study design review and approval by Rocky Vista University’s Institutional Review Board (IRB #2019-0099). Permission to utilize body donor materials for research purposes was obtained by the University of Utah’s Body Donor Program. After IRB approval, 48 first-year medical students volunteered as participants and provided Institutional Review Board-approved written consent. There were 23 first-year medical student participants who had not performed the procedure before in the palpation group. Data from the remaining 25 participants was accessed from a prior study and served as our US group.27 US and palpation-related data were collected and analyzed over one year.
Inclusion and Exclusion Criteria for Study Participants
The only criterion for inclusion in this study was status as a first-year medical student at RVUCOM. First-year students were utilized because they were most likely to be procedure naive. No exclusion criteria were utilized.
Equipment
Subjective questionnaires were distributed to all study participants via Google Forms (Google, LLC, Mountain View, CA). The luminal diameter of each subclavian vein was measured using ImageJ (University of Wisconsin, Madison, WI, and National Institutes of Health, Bethesda, Maryland). Two Z5 Portable Doppler US systems equipped with 12–14 MHz linear transducers were employed during the study (Mindray Medical International Ltd., Shenzhen, China). Each transducer was wrapped in a Tegaderm film (3M Deutschland GmbHm, Neuss, Germany), sealing a layer of transducer gel (McKesson Medical-Surgical, Richmond, VA) against the transducer’s foorprint and protecting it from the cadaver tissue. Placement of the needle into the subclavian vein was executed using 2-inch, 21-gauge BD PrecisionGlide needles with 20 mL disposable syringes (Becton Dickinson and Company, Franklin Lakes, NJ).
Cadaver Imaging and Selection
A total of 6 subclavian veins from 3 formalin-embalmed cadavers were imaged with US to assess the patency of the subclavian veins (Figure 1A and 1B). These 3 cadavers with patient subclavian veins, were utilized to train 23 participants in landmark-guided palpation-based central venous access.
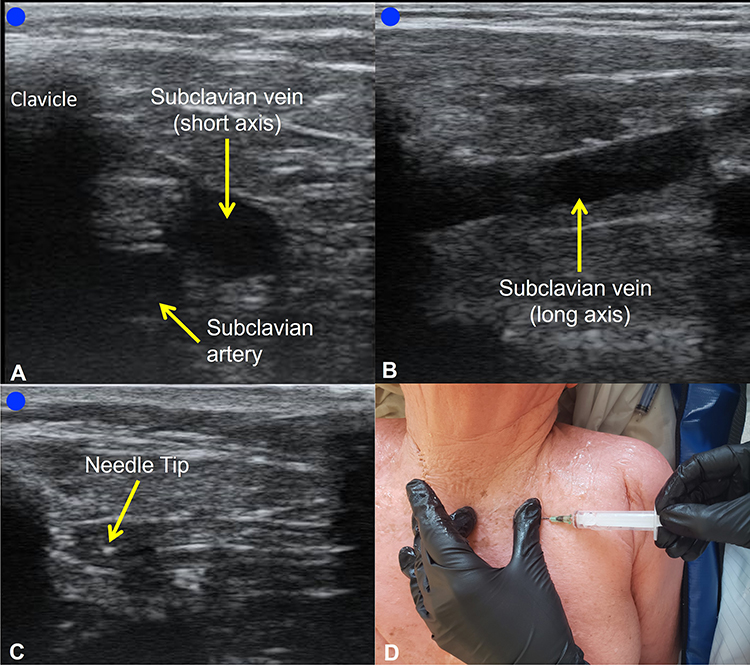 |
Figure 1 Feasibility imaging of the formalin-embalmed subclavian vein. Figure used with permission from the University of Utah’s Body Donor Program. (A–C) Demonstrate the infraclavicular view of a formalin-embalmed cadaver. (A) Depicts a short-axis view of the subclavian artery, vein, and associated structures. (B) Depicts a long-axis view of the isolated subclavian vein. (C) Depicts the short-axis view with a needle tip visible during access to the subclavian vein. (D) Demonstrates introducer needle placement into the subclavian vein using the landmark-guided palpation-based method. |
Didactic Instruction
Each participant watched a 10-minute orientation video outlining the purpose of the study, needle safety, and step-by-step instructions for palpation-based subclavian vein access.
Practical Instruction – Palpation Group
Using a formalin-embalmed cadaver, participants in the palpation group received ten minutes of individual instruction in locating and accessing the subclavian vein from a board-certified general surgeon. During this instruction period, participants were able to access the subclavian vein as many times as possible during the ten minutes. The instruction of this session was standardized by having the same instructor provide one-on-one training with each participant in the palpation group. For this study, participants only inserted the introducer needle until a flashback of fluid was seen in the syringe and were instructed to stop advancing the needle immediately once flashback was observed to practice the skills needed to minimize the risk of potential pleural injury. None of the participants completed the full Seldinger Technique by placing a J-wire or central venous catheter into the subclavian vein.
Practical Instruction – US Group
Participants in the US group described in previous work27 received ten minutes of individual instruction from an Associate Professor of US using a formalin-embalmed cadaver. Participants were instructed to locate the subclavian vein in a short-axis view (Figure 1A) and use a dynamic approach to access the subclavian vein with the introducer needle (Figure 1C). Again, a rubric was employed to standardize instruction. The instruction steps in the rubric were based on guidelines from the American Institute of Ultrasound in Medicine on the proper use of US-guided vascular access.28
Skills Assessment
Participants of each group were objectively assessed on their ability to utilize either US guidance or palpation to independently achieve fluid flashback into the syringe from a cadaveric subclavian vein. Each attempt was evaluated based on three objective criteria: a flashback of fluid into the syringe, the amount of time from initial needlestick to fluid flashback, and the total number of skin punctures. Participants were allowed an unlimited number of attempts in a five-minute timeframe to achieve flashback, which was considered a successful attempt, and ended the skills assessment.
Subjective Assessment
Before didactic or practical instruction, all study participants completed an online questionnaire that inquired about participants’ previous experience operating US machines, performing US-guided or landmark-based procedures, and personal experience with central venous catheter placement. Depending on their assigned group, participants were also asked to indicate their self-confidence to perform specific technique-dependent tasks related to subclavian access (Table 1). This portion of the questionnaire used a sliding 10-point Likert scale (0 = strongly disagree to 10 = strongly agree) to evaluate participants’ self-confidence in each of these areas. The same questionnaire, with the additional option to submit free response participant feedback, was administered again after the didactic and practical instruction sessions. Questionnaire items 1–3 in the US and palpation group questionnaires were designed to be matched during analysis to allow comparison of any confidence differences between the groups (Table 1 and Table 2). Items 4 and 5 were unique to the US group questionnaire and assessed participant confidence in US transducer-specific skills (Table 1).
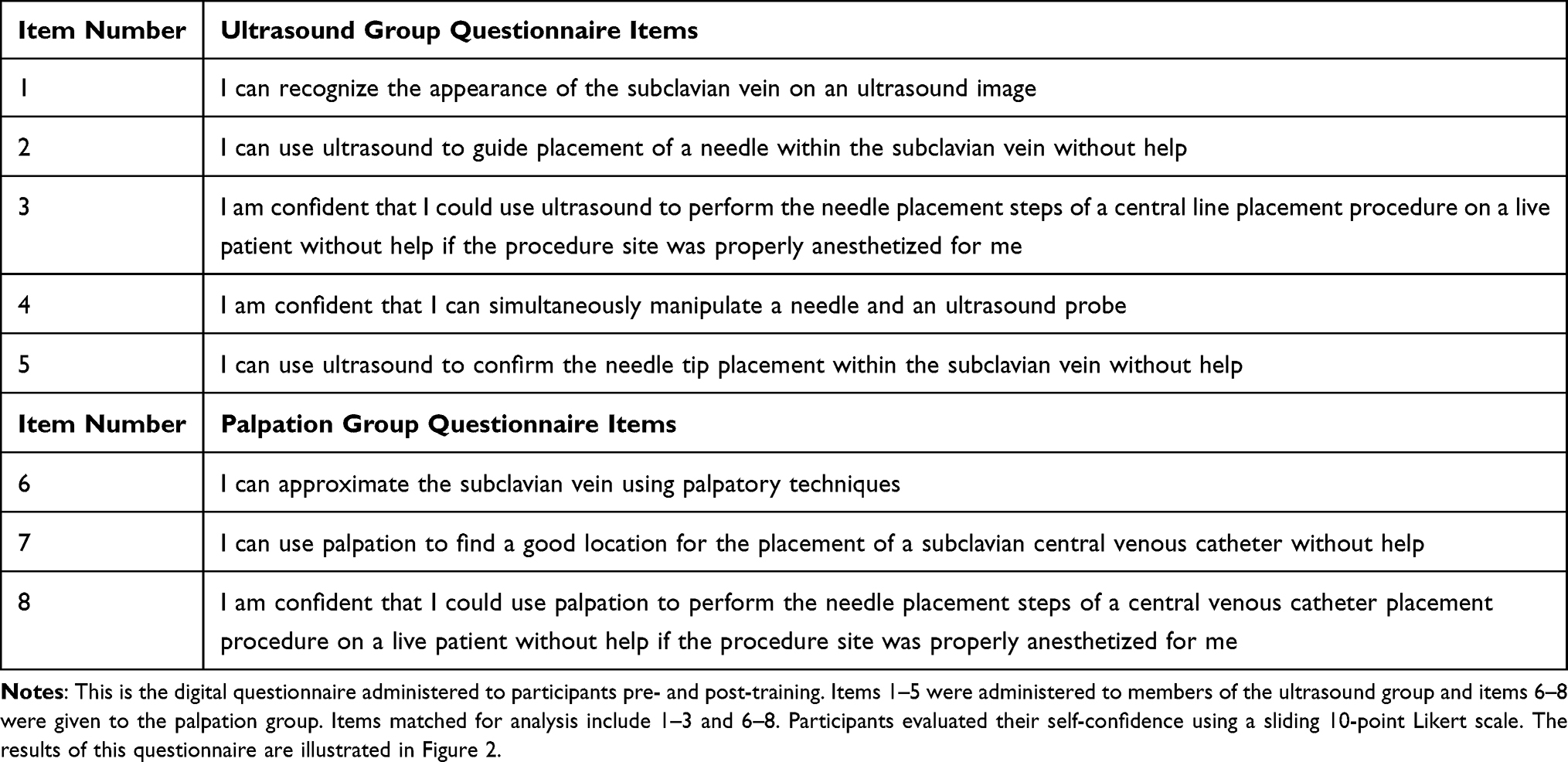 |
Table 1 Subjective Questionnaire Items |
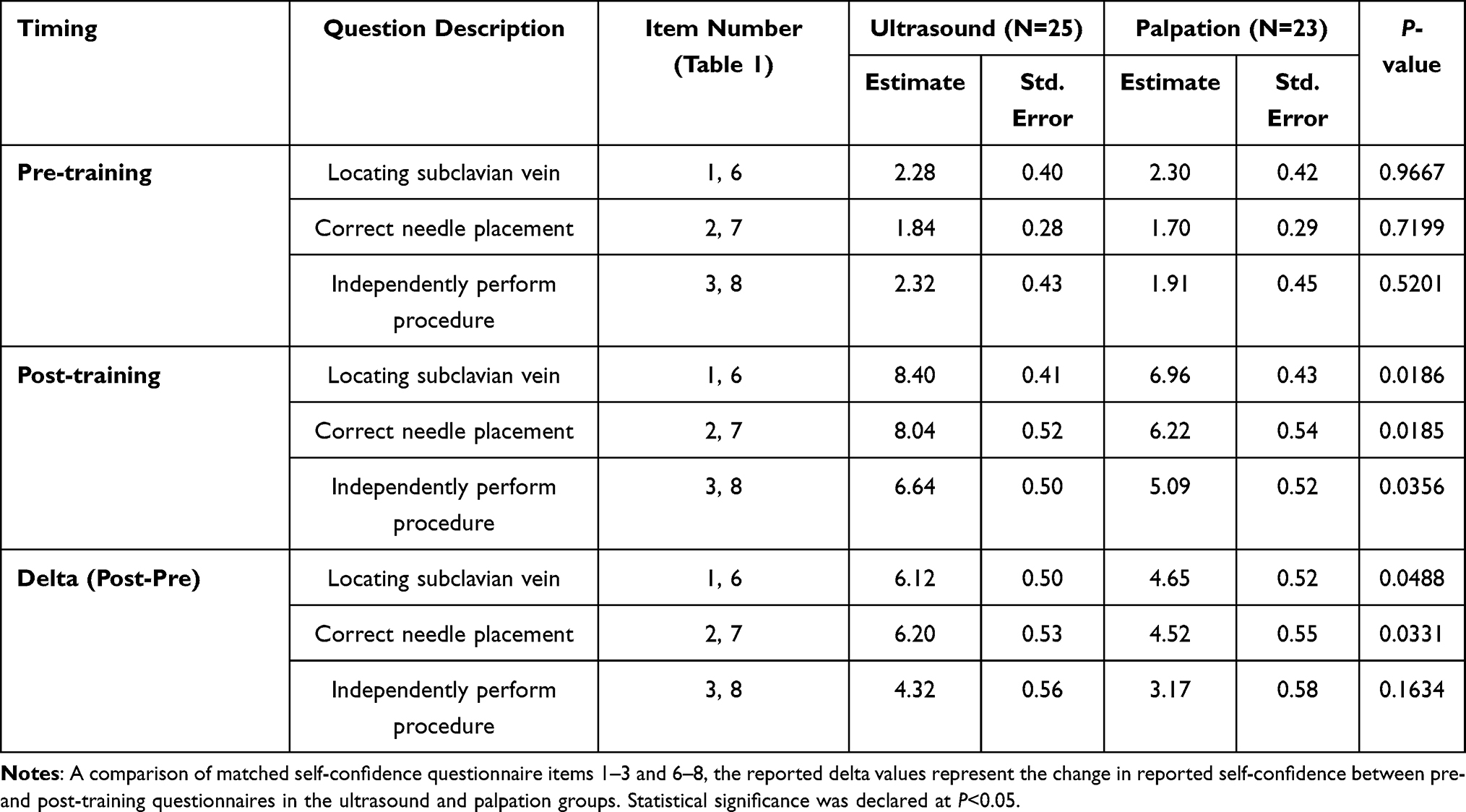 |
Table 2 Matched Questionnaire Items Comparing the Ultrasound and Palpation Groups |
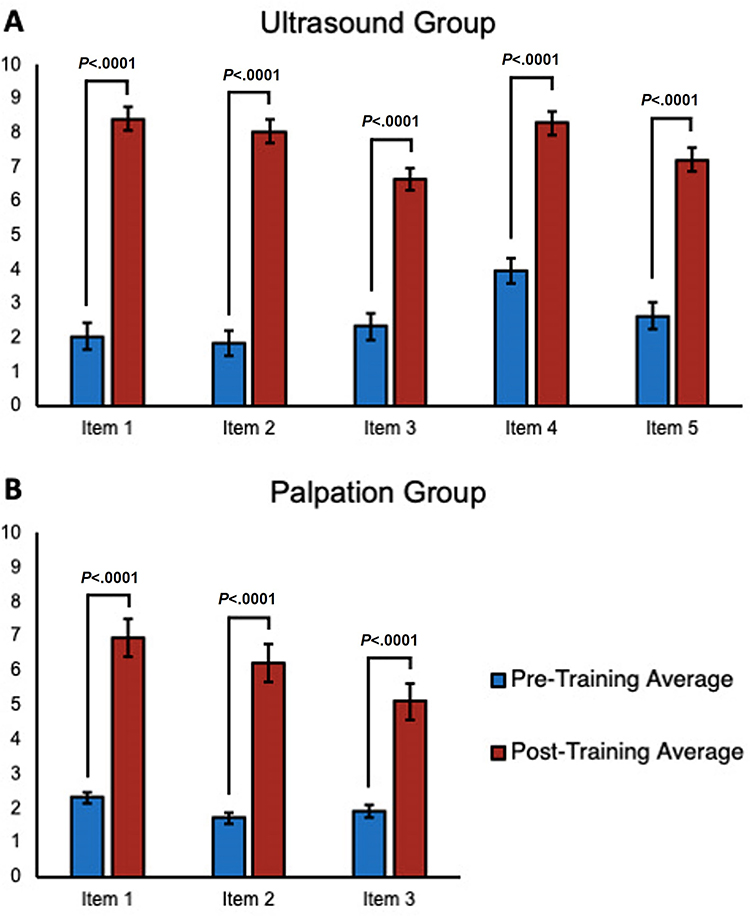 |
Figure 2 Self-confidence questionnaire results by training group. (A and B) Show the change in confidence scores from pre- to post-training reported by participants in the ultrasound (n=25) and palpation (n=23) groups respectively. Specific questionnaire item numbers can be viewed in Table 1. Statistical significance was declared at P<0.05. |
The pre- and post-training questionnaire items used in this study were previously validated by use in a previous project which explored using formalin-embalmed cadavers to teach medical students to perform US-guided knee arthrocentesis.24 The language of the questionnaire was modified to assess study participant self-confidence in independently performing subclavian central venous access rather than knee arthrocentesis.
Statistical Analysis
Data was analyzed using a generalized linear model (GLM) approach where the responses in the pre- and post-training questionnaire assessments were defined as dependent variables while the assigned group was defined as the independent variable.29–31 An examination of the delta (Δ, post-pre) values are presented in Table 2 to evaluate the magnitude of the change from pre- to post-test. The goal was to detect associations in the questionnaire scores attributable to the specific training group to which a participant was assigned. The aptness of our models was evaluated for normality based on their residual distributions. Verification was necessary due to the vulnerability of the Likert scale to normality issues when responses are clustered to one extreme of the scale. However, no normality concerns were detected, thus indicating the suitability of the GLM approach. All estimates are presented with their respective standard errors. All statistical analyses were performed using SAS/STAT v.9.4. (SAS Institute Inc. Cary, NC). Statistical significance was declared at p≤0.05.
Results
Cadaver Imaging and Selection
US images of the infraclavicular region in the formalin-embalmed cadaver are shown in Figure 1. This images demonstrate the patency of the formalin-embalmed subclavian veins used to teach subclavian central venous access by landmark-guided palpation-based technique.
Subjective Assessment
Study participants did not have prior hands-on experience with central venous catheter placement or US-guided procedures. However, ten participants (six in the palpation group and four in the US group) reported having previously observed central venous catheter placement in a clinical setting. Statistical analysis via the GLM approach revealed no significant effects in the subjective or objective evaluations of these ten participants when compared to others without prior central venous catheter-related experience. Following training, participant confidence increased significantly across all questionnaire items (Figure 2).
Table 2 compares the self-confidence scores of the US group to the palpation group on matched questionnaire items 1–3 and 6–8 (seen in Table 1). The pre-training subjective questionnaire demonstrated that there was no significant difference in reported confidence levels between the palpation and US groups. Post-training, participants in the US group felt significantly more confident than the participants in the palpation group across all matched questionnaire items.
The change in participant self-confidence between the US and palpation groups (Δ, post-pre) is shown in the bottom row of Table 2. When asked to report their confidence in locating the subclavian vein and selecting the optimal location for needle access using their respective assigned training technique, participants in the US group were significantly more confident than those in the palpation group. However, the reported confidence in their ability to access the subclavian vein independently on a live patient if the procedure site was properly anesthetized for them, showed no significant difference between groups (P=0.163).
Skills Assessment
For each group, the number of participants who failed the skills assessment (Panel A), the average time to successful flashback (Panel B), and the average number of skin punctures (Panel C), are depicted in Figure 3. Six participants in the palpation group failed the assessment by not achieving a flashback of fluid into the syringe within the time limit. In contrast, only one participant in the US group failed the assessment. The time to successful flashback between participants who passed the assessment in the US and palpation groups was not found to be significant P=0.307. The difference between the number of skin punctures in the palpation and US groups (Panel C) was determined to be significant (P<0.001). The number of skin punctures completed by the unsuccessful participants in achieving flashback is included in the average number of skin punctures performed by each group illustrated in Figure 3C.
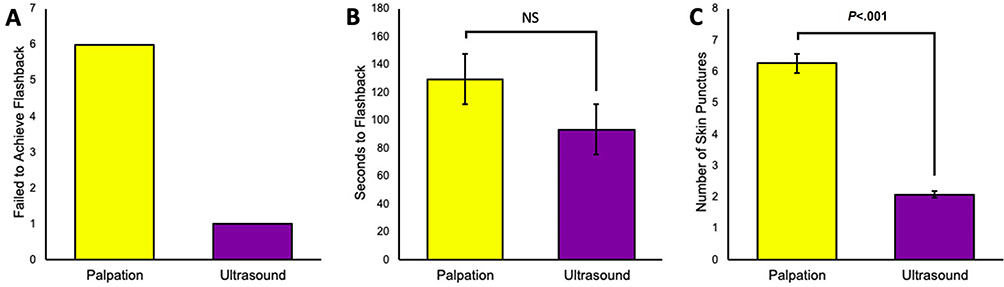 |
Figure 3 Skills assessment performance. (A) Depicts the number of participants who were unable to independently achieve flashback into the syringe within the time limit. (B) Depicts the average time taken to achieve a flashback. Participants who did not achieve flashback within 5 minutes were excluded from the data set depicted (B), as they never achieved fluid flashback into the syringe. NS indicates a non-significant relationship (P=0.307) between the average times to successful flashback in each group. (C) Depicts the average number of skin punctures by all members of each group during the skills assessment. Statistical significance was declared at P<0.05. |
Discussion
Cadaver Imaging
Formalin-embalmed cadavers have not been utilized to teach subclavian central venous access until our prior publication27 due to perceived barriers to their use in training programs related to tissue desiccation and blood coagulation during the embalming process.24,25 The sonographic clarity of these images (Figure 1) and the patent status of these veins illustrate the utility of formalin-embalmed cadavers in subclavian vein access training using either US-guided or palpation-based techniques.
Subjective Assessments
Participant confidence in all matched assessment items significantly improved after only 20 minutes of didactic and practical training for both groups. The comparison of assessment items between groups revealed participants in the US group were significantly more confident in locating the subclavian vein and correctly placing the needle than those in the palpation group (Table 2), reflective of findings previously reported in the literature.11,12 As expected, US guidance provides trainees an opportunity to visualize their target rather than relying on the palpation of superficial landmarks to approximate its most likely location. However, when asked if they would be comfortable performing the procedure independently, there was no significant difference between the group’s responses (Table 2). This suggests that training in either US-guided or palpation-based methods of subclavian vein access using a formalin-embalmed cadaver improves trainee confidence, which may likewise improve their confidence in performing this procedure in a clinical setting. This finding is supported by other studies that show that simulation-based training in central venous catheterization increases patient safety as well as tactile skill and confidence in trainees.32,33
Skills Assessments
First-year medical students performed subclavian central venous access at a slightly slower rate (US: 93 seconds, Palpation: 129 seconds) when compared to residents (US: 60 seconds) performing US-guided access to the internal jugular vein.34 Medical students failed palpation-based access more frequently than US-guided access (Figure 3A). This data supports the findings of prior studies that US guidance improves the performance of novice clinicians.11,12 However, some studies have reported that landmark-guidance fist-pass success rates are higher than US-guided in patients with easy anatomical access, but this could be due to increased operator experience level.35
A recent meta-analysis of studies that compares the clinical use of US and landmark guidance for subclavian vein cannulation reports that US-guided vein cannulation is a safer and more efficient option when compared to landmark guided techniques in a clinical setting.36 Data in this study complements these findings by showing that novice medical trainees learning to access the subclavian perform the procedure more quickly and with less skin punctures than those using landmark guided venous access techniques. It’s worth noting that while the US group demonstrated statistically significantly fewer skin punctures when performing the procedure than the palpation group, the palpation-based technique can require by its nature a high number of skin punctures, which does not necessarily reflect a decreased skill level in the palpation group.12 However, an increased number of skin punctures during procedures may translate to increased procedure time and patient discomfort.12
Limitations and Future Directions
A limitation of this study is that it only addresses the initial step of subclavian vein access with an introducer needle and does not include placing a J-wire or catheter. We were unable to perform central venous catheterization in its entirety due to embalming-related clotting affecting the patency of the cadaveric venous system distally. Additional limitations of this study include power analysis and skills retention. Power analysis of the sample size was not performed because the sample size was not sufficient. Any follow-up studies should include a mathematical justification of the sample size and a longitudinal design to examinate retention of procedure skills. Further investigation is required to compare the efficacy of synthetic models, live patients, and cadavers preserved with alternative embalming techniques in central venous access training activities.
Conclusions
The purpose of this study is to compare the utility of the formalin-embalmed cadaver as a training tool for teaching novice trainees to use palpation-landmark guided techniques to access the subclavian vein and provide a comparison to US-guided training methods reported in our prior study.27 The palpation group took longer to successfully canulate (approximately 36 seconds more), with more failures and more needlesticks required for success than the US group which may translate to increased patient discomfort and increased infection rates in live patients. Another significant advantage the US group had was that they were able to visualize the needle while advancing, a practice which decreases the risk of pleural injury, which is a common complication of this procedure.36,37 Of the two approaches, the data presented in this study suggests that US-guidance is the more optimal method for new learners. However, this study also shows that medical students practicing both US-guided and palpation-based techniques on formalin-embalmed cadavers can gain significantly increased confidence in their ability to independently perform subclavian central venous access, and that formalin embalmed cadavers are a viable and effective training tool for teaching both methods. Formalin-embalmed cadavers provide a safe, effective, and comfortable environment that could be useful for any clinician or medical trainee to learn subclavian central venous access using resources readily available to most medical education institutions. Medical trainees can repeatedly practice procedural dexterity using a tool that accurately simulates the tactile sensation and anatomical variability of living patients without risking patient safety or discomfort. Introducing hands-on training to students early in their medical education may allow them to develop the skills and confidence needed to be more successful in performing subclavian vein catheterization accurately during clinical rotations or residency.
Abbreviations
US, Ultrasound.
Data Sharing Statement
Additional data and information related to this work are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the IRB of Rocky Vista University #2019-0099. All participants volunteered to participate and signed a written consent form indicating as such.
Consent for Publication
The authors grant consent to publication of this work to Advances in Medical Education and Practice
Acknowledgments
The authors want to thank Rocky Vista University for the facility, equipment, and cadavers that were used in this study. We also want to thank those who donate their bodies to the medical sciences.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tse A, Schick MA. Central line placement. In: StatPearls. StatPearls Publishing; 2023. Available from: http://www.ncbi.nlm.nih.gov/books/NBK470286/.
2. Androes M, Heffner A. Placement of jugular venous catheters. In: UpToDate. Wolters Kluwer; 2023. Available from: https://www.uptodate.com/contents/placement-of-jugular-venous-catheters.
3. Maizel J, Guyomarc’h L, Henon P, et al. Residents learning ultrasound-guided catheterization are not sufficiently skilled to use landmarks. Crit Care. 2014;18(1):P127. doi:10.1186/cc13317
4. Parienti JJ, Mongardon N, Mégarbane B, et al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med. 2015;373(13):1220–1229. doi:10.1056/NEJMoa1500964
5. Graham AS, Ozment C, Tegtmeyer K, Lai S, Braner DAV. Videos in clinical medicine. Central venous catheterization. N Engl J Med. 2007;356(21):e21. doi:10.1056/nejmvcm055053
6. Gebhard RE, Szmuk P, Pivalizza EG, Melnikov V, Vogt C, Warters RD. The accuracy of electrocardiogram-controlled central line placement. Anesth Analg. 2007;104(1):65. doi:10.1213/01.ane.0000250224.02440.fe
7. Liu G, Hou W, Zhou C, et al. Meta-analysis of intracavitary electrocardiogram guidance for peripherally inserted central catheter placement. J Vasc Access. 2019;20(6):577–582. doi:10.1177/1129729819826028
8. Zanobetti M, Coppa A, Bulletti F, et al. Verification of correct central venous catheter placement in the emergency department: comparison between ultrasonography and chest radiography. Intern Emerg Med. 2013;8(2):173–180. doi:10.1007/s11739-012-0885-7
9. Pittiruti M, La Greca A, Scoppettuolo G. The electrocardiographic method for positioning the tip of central venous catheters. J Vasc Access. 2011;12(4):280–291. doi:10.5301/JVA.2011.8381
10. Accreditation Council for Graduate Medical Education. Emergency medicine defined key index procedure minimums; 2017. Available from: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.acgme.org/globalassets/pfassets/programresources/em_key_index_procedure_minimums_103117.pdf.
11. Woo MY, Frank J, Lee AC, et al. Effectiveness of a novel training program for emergency medicine residents in ultrasound-guided insertion of central venous catheters. Can J Emergency Med. 2009;11(4):343–348. doi:10.1017/S1481803500011398
12. Froehlich CD, Rigby MR, Rosenberg ES, et al. Ultrasound-guided central venous catheter placement decreases complications and decreases placement attempts compared with the landmark technique in patients in a pediatric intensive care unit*. Crit Care Med. 2009;37(3):1090. doi:10.1097/CCM.0b013e31819b570e
13. Dodge KL, Lynch CA, Moore CL, Biroscak BJ, Evans LV. Use of ultrasound guidance improves central venous catheter insertion success rates among junior residents. J Ultrasound Med. 2012;31(10):1519–1526. doi:10.7863/jum.2012.31.10.1519
14. Moureau N, Lamperti M, Kelly LJ, et al. Evidence-based consensus on the insertion of central venous access devices: definition of minimal requirements for training. Br J Anaesth. 2013;110(3):347–356. doi:10.1093/bja/aes499
15. Huang GC, Newman LR, Schwartzstein RM, et al. Procedural competence in internal medicine residents: validity of a central venous catheter insertion assessment instrument. Acad Med. 2009;84(8):1127. doi:10.1097/ACM.0b013e3181acf491
16. Chao A, Lai CH, Chan KC, et al. Performance of central venous catheterization by medical students: a retrospective study of students’ logbooks. BMC Med Educ. 2014;14(1):168. doi:10.1186/1472-6920-14-168
17. Evans LV, Dodge KL, Shah TD, et al. Simulation training in central venous catheter insertion: improved performance in clinical practice. Acad Med. 2010;85(9):1462. doi:10.1097/ACM.0b013e3181eac9a3
18. Promes SB, Chudgar SM, Grochowski CO, et al. Gaps in procedural experience and competency in medical school graduates. Acad Emerg Med. 2009;16(s2):S58–S62. doi:10.1111/j.1553-2712.2009.00600.x
19. Berman JR, Ben-Artzi A, Fisher MC, Bass AR, Pillinger MH. A comparison of arthrocentesis teaching tools: cadavers, synthetic joint models, and the relative utility of different educational modalities in improving trainees’ comfort with procedures. J Clinic Rheumatol. 2012;18(4):175. doi:10.1097/RHU.0b013e318258259e
20. Michels NR, Vanhomwegen E. An educational study to investigate the efficacy of three training methods for infiltration techniques on self-efficacy and skills of trainees in general practice. BMC Fam Pract. 2019;20(1):133. doi:10.1186/s12875-019-1023-7
21. Boaz NT, Anderhuber F. The uses of soft embalming for cadaver-based dissection, instruction in gross anatomy, and training of physicians. FASEB J. 2009;23(S1):
22. Kondrashova T, Canaan R, Gunn B, Pazdernik V, Houser JJ. Development of competency in needle-guided procedures through the use of soft-embalmed cadavers. Mo Med. 2020;117(5):461–468.
23. Varga S, Smith J, Minneti M, et al. Central venous catheterization using a perfused human cadaveric model: application to surgical education. J Surg Educ. 2015;72(1):28–32. doi:10.1016/j.jsurg.2014.07.005
24. Clason J, Liederbach M, Balkman N, Davis E, Zapata I, Mason NL. The feasibility of ultrasound-guided knee arthrocentesis training using formalin-embalmed cadavers. JBJS Open Access. 2021;6(3):
25. Benkhadra M, Faust A, Ladoire S, et al. Comparison of fresh and thiel’s embalmed cadavers according to the suitability for ultrasound-guided regional anesthesia of the cervical region. Surg Radiol Anat. 2009;31(7):531–535. doi:10.1007/s00276-009-0477-z
26. Klaubert W, Schönbauer R, Gilg T, et al. The role of coagulation, fibrinogenolysis and fibrinolysis in the development of fluid and clotted cadaver plasma. Thromb Res. 1988;50(1):53–63. doi:10.1016/0049-3848(88)90174-0
27. Loveless BA, Muir MW, Limov AL, et al. Advancing point-of-care ultrasound training in medical schools: ultrasound-guided subclavian vein access training using formalin-embalmed cadavers. Crit Care Explor. 2022;4(4):e0680. doi:10.1097/CCE.0000000000000680
28. Moore C, Kollpainter R, Andrews L, et al. AIUM practice parameter for the use of ultrasound to guide vascular access procedures. J Ultrasound Med. 2019;38(3):E4–E18. doi:10.1002/jum.14954
29. Peterson NB, Friedman RH, Ash AS, Franco S, Carr PL. Faculty self-reported experience with racial and ethnic discrimination in academic medicine. J Gen Intern Med. 2004;19(3):259–265. doi:10.1111/j.1525-1497.2004.20409.x
30. Mokhles S, Nuyttens JJME, de Mol M, et al. Treatment selection of early stage non-small cell lung cancer: the role of the patient in clinical decision making. BMC Cancer. 2018;18(1):79. doi:10.1186/s12885-018-3986-5
31. Keeney AJ, Hohman M, Bergman E. Interprofessional education: a poverty simulation with elementary teachers and social work students. J Teach Soc Work. 2019;39(2):148–162. doi:10.1080/08841233.2019.1586808
32. Spencer TR, Bardin-Spencer AJ. Pre- and post-review of a standardized ultrasound-guided central venous catheterization curriculum evaluating procedural skills acquisition and clinician confidence. J Vasc Access. 2020;21(4):440–448. doi:10.1177/1129729819882602
33. Jagneaux T, Caffery TS, Musso MW, et al. Simulation-based education enhances patient safety behaviors during central venous catheter placement. J Patient Saf. 2021;17(6):425. doi:10.1097/PTS.0000000000000425
34. Nguyen B-V, Prat G, Vincent J-L, et al. Determination of the learning curve for ultrasound-guided jugular central venous catheter placement. Intensive Care Med. 2014;40(1):66–73. doi:10.1007/s00134-013-3069-7
35. Gottlieb M, O’Brien JR, Schraft EK. What is the role of ultrasound guidance versus the landmark-based technique for peripheral intravenous cannulation? Ann Emergency Med. 2023;82(3):366–368. doi:10.1016/j.annemergmed.2023.02.018
36. Zawadka M, La Via L, Wong A, et al. Real-time ultrasound guidance as compared with landmark technique for subclavian central venous cannulation: a systematic review and meta-analysis with trial sequential analysis*. Crit Care Med. 2023;51(5):642–652. doi:10.1097/CCM.0000000000005819
37. Nazir A, Niazi K, Zaidi SMJ, et al. Success rate and complications of the supraclavicular approach for central venous access: a systematic review. Cureus. 2022;14(4):e23781. doi:10.7759/cureus.23781
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.