")
Back to Journals » Clinical Interventions in Aging » Volume 19
Comprehensive Geriatric Assessment in the Emergency Department: A Prospective Cohort Study of Process, Clinical, and Patient-Reported Outcomes
Authors O'Shaughnessy Í, Robinson K, Whiston A, Barry L, Corey G, Devlin C, Hartigan D, Synnott A, McCarthy A, Moriarty E, Jones B, Carroll I, Shchetkovsky D, O'Connor M , Steed F, Carey L, Conneely M, Leahy A, Quinn C, Shanahan E, Ryan D , Galvin R
Received 9 August 2023
Accepted for publication 1 December 2023
Published 7 February 2024 Volume 2024:19 Pages 189—201
DOI https://doi.org/10.2147/CIA.S434641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Íde O’Shaughnessy,1 Katie Robinson,1 Aoife Whiston,1 Louise Barry,2 Gillian Corey,1 Collette Devlin,1 Deirdre Hartigan,1 Aoife Synnott,3 Aoife McCarthy,4 Eoin Moriarty,5 Bryan Jones,6 Ida Carroll,5 Denys Shchetkovsky,7 Margaret O’Connor,5,8 Fiona Steed,9 Leonora Carey,4 Mairéad Conneely,1 Aoife Leahy,5 Colin Quinn,5 Elaine Shanahan,5 Damien Ryan,7,8 Rose Galvin1
1School of Allied Health, Faculty of Education and Health Sciences, Ageing Research Centre, Health Research Institute, University of Limerick, Limerick, Ireland; 2Department of Nursing and Midwifery, University of Limerick, Limerick, Ireland; 3Department of Physiotherapy, University Hospital Limerick, Limerick, Ireland; 4Department of Occupational Therapy, University Hospital Limerick, Limerick, Ireland; 5Department of Ageing and Therapeutics, University Hospital Limerick, Limerick, Ireland; 6Department of Medical Social Work, University Hospital Limerick, Limerick, Ireland; 7Limerick EM Education Research Training (ALERT), Emergency Department, University Hospital Limerick, Limerick, Ireland; 8School of Medicine, Faculty of Education and Health Sciences, Ageing Research Centre, Health Research Institute, University of Limerick, Limerick, Ireland; 9Department of Health, Government of Ireland, Dublin, Ireland
Correspondence: Íde O’Shaughnessy, School of Allied Health, Faculty of Education and Health Sciences, Ageing Research Centre, Health Research Institute, University of Limerick, Ireland, Tel +35361234149, Email [email protected]
Background: This study aimed to explore the process, clinical, and patient-reported outcomes of older adults who received an interdisciplinary Comprehensive Geriatric Assessment (CGA) in the emergency department (ED) over a six-month period after their initial ED attendance.
Patients and Methods: A prospective cohort study recruited older adults aged ≥ 65 years who presented to the ED of a university teaching hospital in Ireland. Baseline assessment data comprising a battery of demographic variables and validated indices were obtained at the index ED attendance. Telephone interviews were completed with participants at 30- and 180-day follow-up. The primary outcome was incidence of hospital admission following the index ED attendance. Secondary outcomes included participant satisfaction, incidence of functional decline, health-related quality of life, incidence of unscheduled ED re-attendance(s), hospital (re)admission(s), nursing home admission, and death.
Results: A total of 133 participants (mean age 82.43 years, standard deviation = 6.89 years; 71.4% female) were recruited; 21.8% of the cohort were admitted to hospital following the index ED attendance with a significant decline in function reported at hospital discharge (Z = 2.97, p = 0.003). Incidence of 30- and 180-day unscheduled ED re-attendance was 10.5% and 24.8%, respectively. The outcome at the index ED attendance was a significant predictor of adverse outcomes whereby those who were discharged home had significantly lower odds of multiple adverse process outcomes at 30- and 180-day follow-up, and significantly higher function and health-related quality of life at 30-day follow-up.
Conclusion: While this study was observational in nature, findings suggest CGA in the ED may improve outcomes by mitigating against the adverse effects of potentially avoidable hospital admissions and focusing on a longitudinal approach to healthcare delivery at the primary-secondary care interface. Future research should be underpinned by an experimental study design to address key limitations in this study.
Keywords: frailty, emergency care, longitudinal study, adverse outcomes, integrated care
Introduction
Older adults are the most frequent users of emergency care, accounting for up to 25% of all international emergency department (ED) attendances.1,2 This demographic shift in healthcare utilization, specifically ED usage, is one factor contributing to the growing problem of ED crowding.3 An aging population is vulnerable to an increasing accumulation of health deficits4,5 giving rise to clinical conditions of frailty.6 Caring for older adults living with frailty presenting to the ED is increasingly recognized as a global public health concern7 and was outlined as a top research priority by the Royal College of Emergency Medicine in a recent Priority Setting Partnership with the James Lind Alliance.8
Compared to younger patients, older adults living with frailty presenting to the ED experience longer ED stays9 and demonstrate higher rates of adverse outcomes such as functional decline,10 unplanned 30-day ED re-attendance,11 and inpatient mortality.12 Application of frailty screening in the ED enables risk-stratification of older adults who would benefit from specialist geriatric assessment and intervention to mitigate against suboptimal clinical and process outcomes.13 While a plethora of international evidence exists to support the diagnostic and predictive accuracy of a number of frailty screening tools in the ED,14–17 no individual screening tool is recommended by experts.18 In essence, frailty identification and stratification in the ED via the use of any tool should serve as a trigger for commencement of Comprehensive Geriatric Assessment (CGA).
CGA is defined as a multidimensional diagnostic and therapeutic process focused on determining a frail older person’s medical, psychological, and functional capability in order to develop a coordinated and integrated plan for treatment and follow-up’.19 CGA is a resource-intensive and evidence-based intervention, which proactively identifies complex and multifactorial needs in older adults with the overall aim of restoring independence and improving quality of life (QoL).21–23 Existing systematic reviews and meta-analyses provide compelling evidence that inpatient CGA is more effective than “usual care” in improving a range of outcomes for hospitalized older adults living with frailty.21 However, despite serving as the main portal of entry to inpatient care, limited high-quality evidence exists to support the effectiveness of CGA in the ED.24,25 Conroy et al (2011) conducted a systematic review and meta-analysis of five randomized controlled trials (RCT), which evaluated the effectiveness of CGA interventions for older adults living with frailty being rapidly discharged from the ED or Acute Medical Unit.24 They found no compelling evidence that CGA in this setting had any effect on mortality, institutionalization, hospital re-admissions, functional status, QoL, or cognition. However, there was significant variation in the content of the CGA delivered across the trials. Similarly, Harding (2020) provided an overview of five studies, which measured the impact of CGA in the ED on subsequent secondary healthcare utilization post index ED attendance.25 No definitive evidence was found that CGA in the ED reduced re-attendances or admissions 30 days post-discharge. Both reviews highlighted the methodological limitations and clinical heterogeneity of the included studies and recommended completion of future high-quality research that adopts a longitudinal approach to follow-up at the acute-community interface as well as standardization of outcome measures.
Given the growing challenge of reducing adverse outcomes for older adults living with frailty following an ED attendance and the ambiguity about the content and effectiveness of CGA for this patient population in this setting, further research is warranted. To inform the design of future robust trials of CGA in this setting, we conducted a prospective cohort study aimed at exploring the process, clinical and patient-reported outcomes of older adults who received CGA in the ED of a university teaching hospital in Ireland over a period of six months after their initial ED attendance.
Material and Methods
Study Design and Setting
A prospective cohort study was conducted and reported in accordance with The STrengthening the Reporting of the OBservational studies in Epidemiology (STROBE) guidelines26 with a completed checklist outlined in Supplementary Information 1. The study protocol was registered on Clinicaltrials.gov (NCT05252182) and was published elsewhere.27 Study participants were recruited from the ED of University Hospital Limerick (UHL), which is a university teaching hospital with a large catchment area in the Mid-West of the Republic of Ireland. UHL is the central hub for a larger hospital group with six hospital sites, all functioning as a single hospital system caring for a substantially rural population of approximately 470,000. The university teaching hospital is the only hospital in the group that has a 24/7/365 emergency care and critical care service and has 487 inpatient beds. In 2022, 79,892 ED attendances were recorded of which 20,526 were older adults aged ≥65 years.
The study adheres to the Declaration of Helsinki and received ethics approval from the Research Ethics Committee, Quality and Safety Department, University of Limerick Hospital Group Hospital (Ref: 107/2021).
Participants and Data Collection
Recruitment
Participants were recruited between February–July 2022 and were eligible for participation in the study if they were aged ≥65 years, had a Manchester Triage System (MTS) category of 2 to 5,28 presented to the ED with a medical complaint between the hours of 08:00–17:00, Monday–Friday, and scored ≥2 on the Identification of Seniors at Risk (ISAR) tool.29 Consecutive participants were identified through the ED triage system by a member of a dedicated interdisciplinary team. In accordance with the Data Protection Act 2018 (Section 36(2)),30 all participants signed informed consent forms and received both written and verbal information about the study prior to recruitment.
Older adults who presented with acute cardiac and/or neurological pathology, injuries requiring surgical intervention, or high illness acuity, which necessitated treatment in the resuscitation room throughout their ED attendance, were excluded from recruitment.
Baseline Data Collection
Each participant underwent a baseline assessment, which comprised a battery of demographic variables and validated indices. Demographic information included participant’s gender, age, marital status, residential status, ethnicity, socioeconomic status, source of referral, mode of arrival to the ED, index complaint, and triage category as per the MTS.28 The health assessment comprised the following measurements: the 21-item Charlson Comorbidity Index (CCI) score31 to profile baseline comorbidities; a list of prescribed medications; frailty identification and stratification through Rockwood’s Clinical Frailty Scale (CFS);5 the ISAR tool;29 a global measure of functional ability through the self-rated Barthel Index (BI) for activities of daily living (ADLs);32 delirium and cognitive screening through the 4AT;33 and health-related QoL through the EuroQoL survey 5-dimension and 5-levels form (EQ-5D-5L).34
Exposure
Study participants received an interdisciplinary CGA, which focused on determining an older adult’s medical, psychosocial, and functional capabilities and limitations with the view to developing a holistic treatment plan.19 The interdisciplinary team comprised a registrar in geriatric medicine, specialist geriatric nurse, senior occupational therapist, senior physiotherapist, and senior medical social worker with dual governance from consultants in Emergency Medicine and Geriatric Medicine. Interventions delivered by the interdisciplinary team included, but were not limited to, medical assessment, diagnostics and treatment, provision of information to older adults and those important to them on the outcome of CGA and ED discharge plan, completion of timely handover to community-based or inpatient services following ED discharge, medication reconciliation, prescription of enabling equipment to compensate for unresolved functional or mobility deficits, provision of home exercise/activity programs, and patient and family education on self-management strategies, as appropriate. Individualized care planning and referrals to out-of-hospital pathways, as appropriate, were at the forefront of the teams’ practice, which aimed to promote an integrated and longitudinal approach to care. In keeping with the elements of CGA reported by Ellis et al in the 2017 Cochrane review,21 the core components of CGA are outlined in greater detail in Supplementary Information 2.
Follow-Up Data Collection and Outcome Variables
A research nurse completed follow-up telephone interviews with participants at 30 days and six months after their index ED attendance. The primary outcome of interest was incidence of hospital admission following the index ED attendance. Secondary outcomes included participant satisfaction with the index ED attendance, incidence of functional decline (including functional decline at hospital discharge among the admitted cohort), health-related QoL, incidence of unscheduled ED re-attendance(s), unscheduled hospital (re)admission(s), nursing home (NH) admission, healthcare utilization, and death within 30 days and six months of the index ED attendance.
Satisfaction with the index ED attendance was assessed via the 18-item Patient Satisfaction Questionnaire (PSQ-18),35 which was completed with participants at 30-day telephone follow-up by the research nurse. Functional decline was assessed via the BI32 at hospital discharge for those admitted following the index ED attendance and at 30- and 180-day telephone follow-up. Health-related QoL was assessed via the EQ-5D-5L34 at 30- and 180-day telephone follow-up. Healthcare utilization (for example, specialist geriatric ambulatory care services, general practitioner, public health nurse, home care support, Health and Social Care Professionals input, NH admission, etc) was assessed via a structured questionnaire at 30- and 180-day telephone follow-up. Data on objective measures such as unscheduled ED re-attendance, hospital (re)admission(s), etc, were gleaned from routine hospital data.
Statistical Analyses
Sample size calculation was based on a review of the international literature coupled with local metrics where the primary outcome of incidence of hospital admission was estimated to be in the region of 55%.36,37 We calculated our sample size a priori based on a predicted reduction of at least 25% in admission rate post exposure to the interdisciplinary team in the ED.27 It was determined that a sample size of at least 128 participants was required to detect this reduction, at 5% level of significance and with 80% power.
Descriptive statistics were used to profile the baseline characteristics of the total cohort split by outcome at index ED attendance – admission, discharge home, transitional care, and inpatient rehabilitation. Categorical measures, for example, marital status, were analyzed in terms of frequencies and percentages; continuous measures, for example, BI, were analyzed in terms of means and standard deviations (SD); median and interquartile ranges (IQR) for continuous measures, which showed evidence of skewness, for example, ED length of stay. Separate multivariate logistic regressions were conducted where sufficient counts of incidence (≥10) were available to explore predictors of adverse outcomes at 30-days and 180-days for example, unscheduled ED re-attendance, hospital admission, and NH admission. Based on previous literature, age, gender, polypharmacy, and frailty (CFS) were the predictors explored using the enter method.38 A subsequent set of multivariate logistic regression models were then estimated to explore if outcomes at index ED attendance – hospital admission versus discharge home, predicted aforementioned adverse outcomes at 30- and 180-days controlling for any significant predictors identified from the first set of logistic regression models. For all logistic regression models, odds ratios with 95% odds ratio scale confidence intervals (CI) were reported. Independent Samples T-Test and where necessary their non-parametric equivalent, Mann–Whitney U-tests, were conducted to explore the differences in PSQ-18, BI, EQ-5D-5L index value, and EQ visual analogue scale (VAS) scores across admitted versus discharged home participants within various time-points. The PSQ-18 comprises seven subscales: general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with doctor, and accessibility and convenience. The sum score of all subscales ranges from 18 to 90 with higher scores indicating higher levels of satisfaction.35 The BI measures performance across 10 ADLs using an ordinal scale, which ranges from 20 to 0 in 1-point increments, with higher scores indicating greater functional independence.30 The EQ-5D-5L comprises five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems.34 EQ-5D-5L data were converted to an index value using utility values for health states in Ireland.39 Health state index scores generally range from less than 0 (where 0 is the value of a health state equivalent to dead) to 1 (the value of full health), with higher scores indicating higher health utility. Additionally, the EQ VAS records the patient’s self-rated health on a vertical VAS ranging from 100 to 0, where the endpoints are labelled “The best health you can imagine” and “The worst health you can imagine”.34 All analyses were computed with JASP statistical software.
Results
A total of 133 participants were recruited over a 6-month period. Table 1 illustrates participants’ baseline characteristics including demographic and health measurements for the overall sample and by group based on outcome post index ED attendance, that is, inpatient admission, discharge home, transfer to transitional care (NH facility for a period of convalescence), and transfer to an inpatient rehabilitation facility.
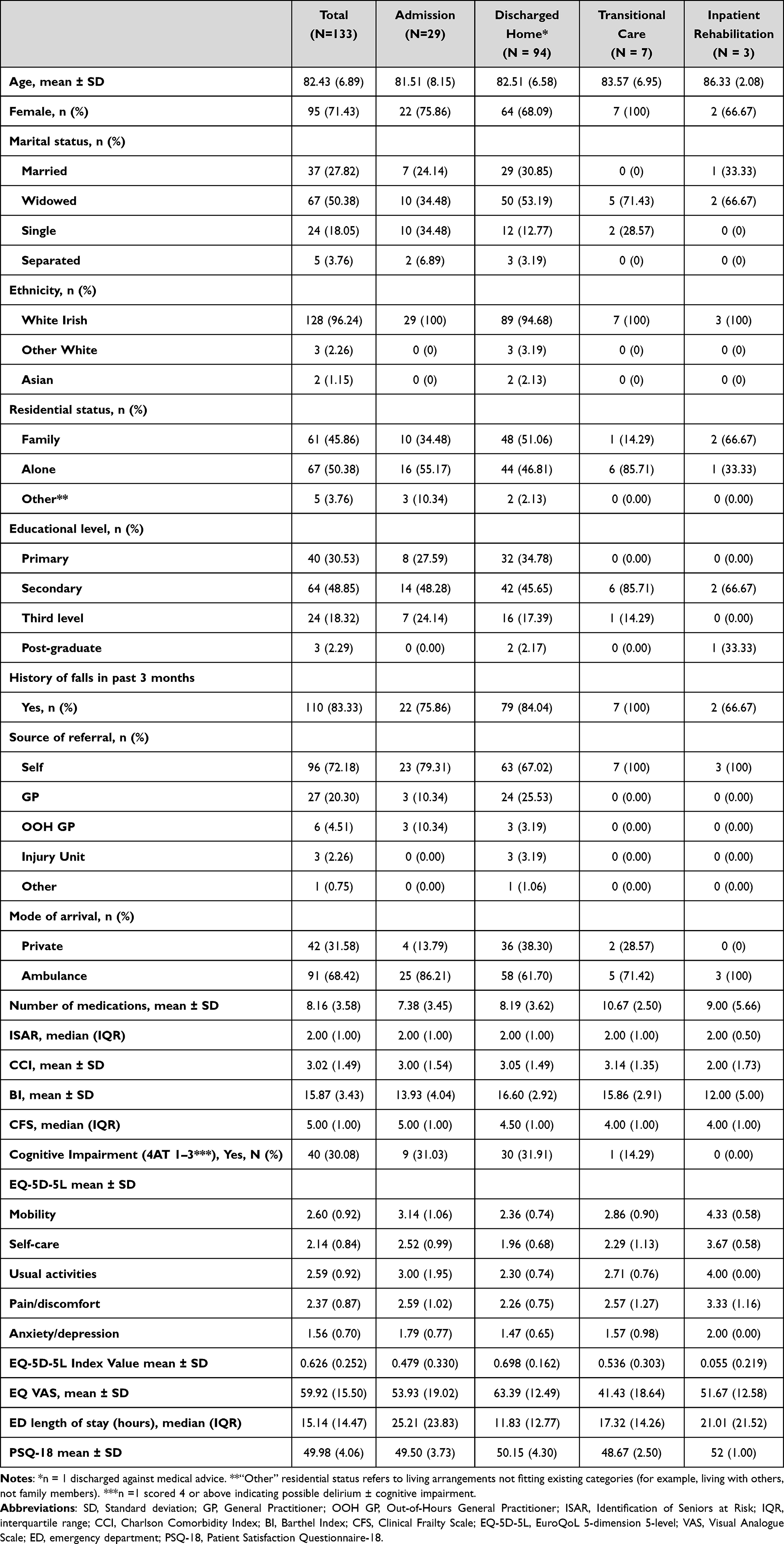 |
Table 1 Baseline Characteristics and Outcomes Post Index ED Attendance |
The mean age of the participants was 82.43 years (SD = 6.89 years) with females representing 71.43% of the total cohort. Almost three-quarters of participants self-referred to the ED (72.18%) and 68.42% were conveyed via ambulance. The mean BI score was 15.87 (SD = 3.43) and 83.33% of participants experienced at least one fall in the 3-month period preceding their index ED attendance. The mean number of prescribed medications was 8.16 (SD = 3.58). In terms of frailty and risk stratification, participants had a median CFS score of 5.00 (IQR = 1.00) that is, living with mild frailly and a median ISAR score of 2.00 (IQR = 1.00).
Outcomes at Index ED Attendance
At the index ED attendance, data pertaining to the number of prescribed medications were unavailable for 20 participants, CCI score for two participants, and EQ-5D dimensions for three participants. A total of 11 participants did not complete the satisfaction questionnaire (n = 1 lost to follow-up and n = 10 declined completion of the measure in its entirety).
In terms of the primary outcome of interest, 21.8% (n = 29) of participants were admitted to hospital following the index ED attendance. There were no significant differences in PSQ-18 scores comparing the admission (M = 49.50, SD = 3.73) versus discharge (M = 50.15, SD = 4.29) cohort (U = 1026.00, p = 0.583). A significant difference in BI (U = 806.50, p = 0.001), EQ-5D-5L index value (U = 784.00, p < 0.001), and EQ VAS (U = 894.50, p = 0.014) scores was observed comparing the admission (MBI = 13.93, SDBI = 4.04; MEQ-5D index = 0.479, SDEQ-5D index = 0.330; MED VAS = 53.93, SDED VAS = 19.02;) versus discharge (MBI = 16.65, SDBI = 2.90; MEQ-5D index = 0.698, SDEQ-5D index = 0.162; MED VAS = 63.37, SDED VAS = 12.56) cohort at index.
Functional Decline at Hospital Discharge
There was a significant decline in function as measured by the BI for participants admitted to hospital following the index ED attendance to their eventual discharge (Z = 2.97, p = 0.003) (Figure 1). Participants had a median length of hospital stay of 14.00 days (IQR = 15), with 62% experiencing functional decline.
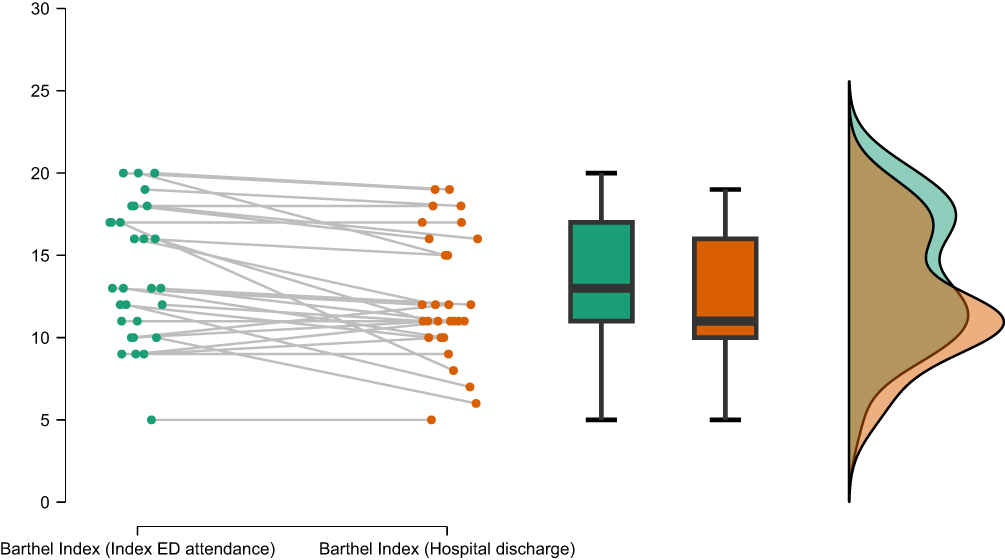 |
Figure 1 Functional decline at hospital discharge. Abbreviation: ED, emergency department. Notes: Colour key: Green = Index ED attendance; Orange = Hospital discharge. |
Outcomes at 30 Days
At 30-day follow-up, data on process measures (unscheduled ED re-attendance, unscheduled hospital admissions, and NH admissions) were available for all participants; two participants died during this timeframe. Data on function were unavailable for two additional participants (n = 1 lost to follow-up and n = 1 declined), and data on EQ-5D dimensions were unavailable for four participants (n = 1 lost to follow-up and n = 3 declined).
In terms of process outcomes, 10.5% participants (n = 14) experienced an unscheduled ED re-attendance, 7.5% (n = 10) experienced an unscheduled hospital admission and 13.5% (n = 18) of participants were admitted to a NH facility within 30-days after their index ED attendance. Of note, 7/18 participants were discharged to a NH facility for a period of convalescence post index ED attendance and all seven transitioned back home after that period. Incidence of functional decline across the entire cohort was reported at 30.8% (n = 41) with 24.1% (n = 32) of participants maintaining their functional ability at 30-day follow-up as measured via the BI. Increasing age was a significant predictor of higher primary care (PC) service use OR 1.11 [1.00, 1.23] (Table 2).
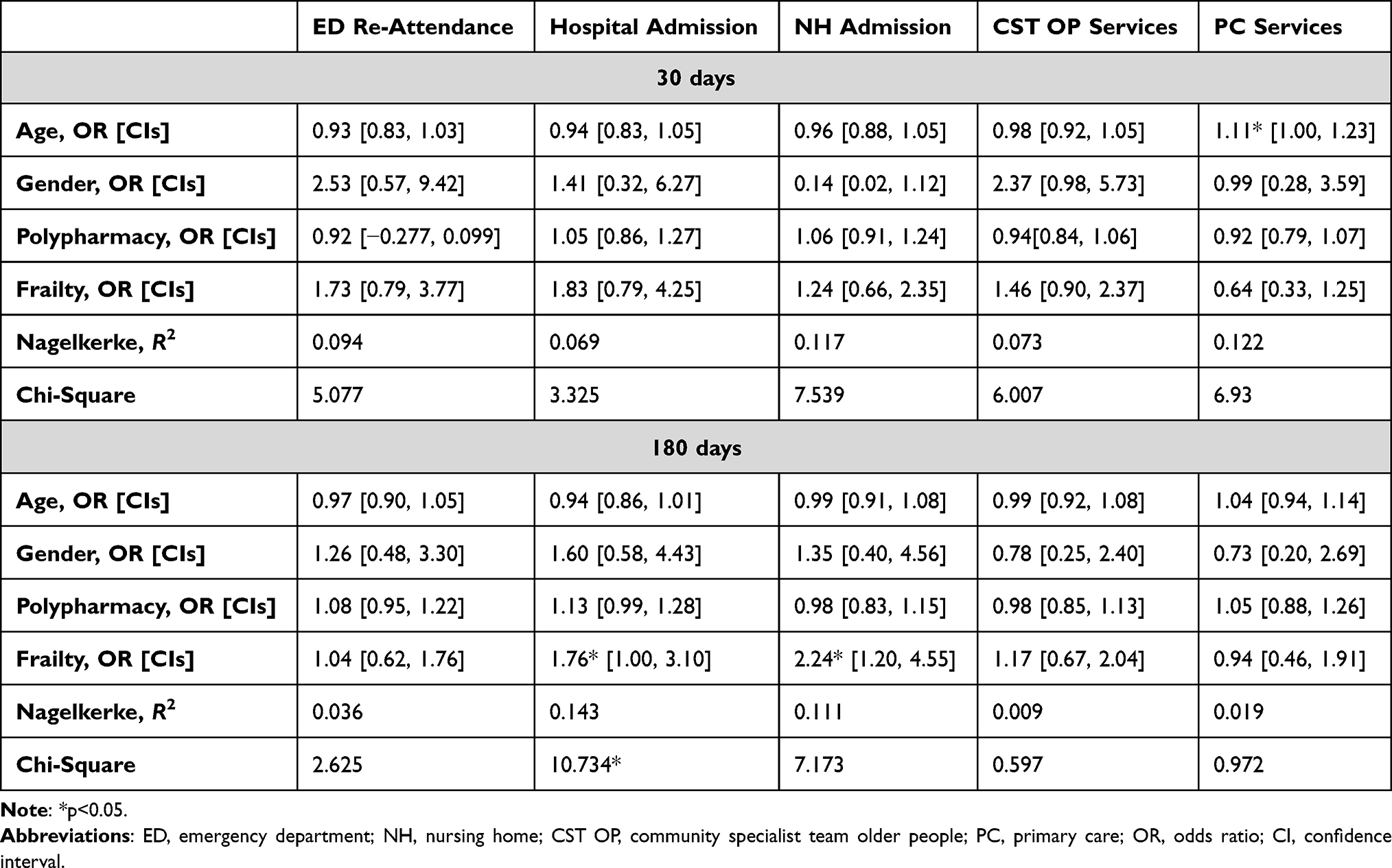 |
Table 2 Total Sample Logistic Regression Models |
Separate logistic regression models were estimated to explore if the outcome at the index ED attendance (hospital admission or discharge home) predicted the aforementioned binary controlling for variables known to influence outcomes at 30-and 180-day follow-up based on the previous regression models (Supplementary Information 3). At 30-day follow-up, the control variable was age. Findings showed that outcome at the index ED attendance that is, discharge home was a significant predictor in NH admission OR 0.13 [0.04, 0.43], Community Specialist Team Older People (CST OP) use OR 25.02 [3.24, 193.40], and PC service use OR 7.55 [2.23, 25.55] suggesting those who were discharged home had lower odds of NH admission and higher odds of CST OP and PC service use 30 days after the index ED attendance. Moreover, the admitted group (MBI = 13.82, SDBI = 3.93; MEQ-5D index = 0.650, SDEQ-5D index = 0.330; MEQ VAS = 62.31, SDEQ VAS = 21.64) had significantly lower 30-day BI (U = 778.50 p = 0.002), EQ-5D index value (U = 898.00, p = 0.040), and EQ VAS (U = 834.00, p = 0.035) scores when compared to the discharged group (MBI = 16.38, SDBI = 3.52; MEQ-5D index = 0.768, SDEQ-5D index = 0.229; MEQ VAS = 71.65, SDEQ VAS = 19.35).
Outcomes at 180 Days
At 180-day follow-up, data on process measures (unscheduled ED re-attendance, unscheduled hospital admissions, NH admissions) were available for all participants; nine participants died during this timeframe. Data on function were unavailable for four participants (n = 2 lost to follow-up and n = 2 declined), and data on EQ-5D dimensions were unavailable for four participants (n = 2 lost to follow-up and n = 2 declined).
In terms of process outcomes, 24.8% participants (n = 33) experienced an unscheduled ED re-attendance, 24.8% (n = 33) experienced an unscheduled hospital admission and 15.8% (n = 21) of participants were admitted to a NH facility within 180-days of the index ED attendance with 6.8% (n = 9) of the total cohort transitioning to long-term care residency. Incidence of functional decline was 32.3% (n = 43) with 15% (n = 18) of participants maintaining their functional ability at 180-day follow-up. Frailty was a significant predictor of hospital admission OR 1.76 [1.00, 3.10] and NH admission OR 2.34 [1.20, 4.55], indicative of higher CFS scores resulting in greater probability of hospital and NH admission (Table 2).
The outcome at index ED attendance that is, discharge home was a significant predictor in unscheduled ED re-attendance OR 0.29 [0.10, 0.84], hospital admission OR 0.22 [0.07, 0.67], and NH admission OR 0.25 [0.07, 0.88], suggesting those who were discharged home at the index ED attendance had significantly lower incidences of these outcomes at 180-day follow-up. It was also a significant predictor of CST OP service use OR 8.53 [1.05, 69.38], suggesting those discharged home at the index ED attendance had higher odds of this service use at 180-day follow-up. No significant differences were observed in BI (p = 0.34), EQ-5D-5L index value (p = 0.268), and EQ VAS (p = 0.08) scores comparing the admission versus discharge cohort.
Discussion
This prospective cohort study explored the process, clinical, and patient-reported outcomes of older adults who received CGA in the ED of a university teaching hospital in Ireland over a period of six months after their initial ED attendance.
Our findings pertaining to the primary outcome of interest, that is, incidence of admission following the index ED attendance, draw parallels with those reported in a systematic review that assessed whether consultant geriatrician-led CGA in the ED can reduce admission rates.40 All five studies included in the review (four pre-post analyses, one prospective non-randomized study) reported a statistically significant reduction in admission rates (ranging between 2.5% and 19.7%). However, no pooled statistical analysis was provided, and given the variation in the magnitude of the results and intervention methods employed across studies, the authors highlighted difficulties in generalizing the results due to uncertainty related to the clinical and economic benefits of the intervention. Furthermore, given that our study was observational, it is difficult to draw inferences on the true reduction in admission rate and causal links between exposure to the interdisciplinary team and outcomes measured.
Unequivocal evidence indicates that acute hospitalization among older adults accelerates functional decline,41 a phenomenon more commonly referred to in the literature as hospital-associated-disability [HAD].42 In line with the international evidence base, our study reported a 62% incidence of functional decline among the cohort of older adults admitted to hospital (n = 29) following the index ED attendance. Participants had a mean BI score of 13.93 (SD = 4.04) on admission to hospital, indicating a requirement for assistance across a number of the 10 ADLs contained in the measure, at that time-point. Identification of inpatient risk factors and availability of interventions aimed at reducing the incidence of HAD were beyond the scope of our study. Our findings contrast those reported in a meta-analysis of 15 studies that determined the combined prevalence of HAD among hospitalized older adults aged ≥65 years on acute medical and surgical units as 30% (95% CI, 24–33%).43 However, a number of clinical and methodological differences exist between our prospective cohort study and this meta-analysis. Firstly, there was notable heterogeneity across populations of interest. Apart from mean age, Loyd et al did not profile the baseline health characteristics of the study sample, for example, comorbidity index, frailty, polypharmacy, etc. Secondly, two studies included older adults in specialty units, that is, psychiatry, cardiology, and neurology units as well as two community-based cohorts, that is, participants were recruited from the community and followed over multiple years during which time acute care hospitalization data were collected. Thirdly, of the hospital-based studies, there was variation in the timing of assessment of function, eight studies assessed functional status two weeks prior to admission to hospital discharge, one assessed functional status two weeks prior to admission to one-week post-discharge, three assessed functional status from admission to discharge, and one assessed functional status from admission to 3 months post-discharge. Finally, the authors highlighted the lack of standardized methods for assessing function among hospitalized older adults observed in the meta-analysis. This outcome heterogeneity has implications for reviewing research evidence and for generating policy recommendations. Therefore, there is a need for a robustly developed core outcome set for studies involving older adults in the ED and across all healthcare settings, which will enhance transparency and availability of comparable data nationally and internationally.
A central tenet of the CGA process is the identification of multifactorial needs and the formulation of an integrated and coordinated plan for follow-up.19 A recent qualitative systematic review and meta-ethnography on stakeholders’ experiences of CGA in an inpatient hospital setting found that while healthcare professionals, older adults, and caregivers’ values and ambitions related to CGA broadly align, their experiences often differ.44 Healthcare professionals experience CGA as enhancing holistic care, enabling the involvement of older adults and caregivers in relational aspects of care and improving continuity of care following hospital discharge. However, the predominant experience of older adults and caregivers is lack of clarity about what CGA is, insufficient involvement in care planning, care discontinuity, and unmet healthcare needs following hospital discharge. In this prospective cohort study, the interdisciplinary team engaged in individualized care planning and shared decision-making with older adults and those important to them. This involved engaging in bidirectional communication regarding the outcome of CGA and ED discharge plan and referring older adults to specialist geriatric ambulatory care pathways and community-based services as an alternative to hospital admission, where appropriate. Outcomes at 180-day follow-up highlighted that older adults who were discharged home following the index ED attendance experienced lower rates of unscheduled ED re-attendance, unscheduled hospital admission, NH admission, and higher rates of CST OP. These findings align with international evidence, suggesting that CGA in the ED may improve outcomes by mitigating against the adverse effects of potentially avoidable hospital admissions45 and focusing on a left-shift and integration of services across the healthcare system.46 Consideration of patient care as a continuum rather than episodic encounters has the potential to identify an integrated approach at the primary-secondary care interface. This longitudinal approach to healthcare delivery is further illuminated by the findings of a recent review of reviews (15 reviews describing 83 primary studies), which summarized evidence on interventions to improve outcomes for older adults attending the ED.47 The authors concluded that no individual intervention was found to be more beneficial, but interventions initiated in the ED and continued into other settings resulted in more favorable outcomes.
Implications for Research and Practice
Given that CGA in the ED is a resource-intensive intervention, it is important to stratify a patient cohort who will derive the greatest benefit. Frailty screening affords an understanding of complexity as well as informing clinical decisions and identification of a target cohort for CGA in the ED.48 Findings from a recent retrospective cohort study found that assessing frailty status at ED triage using the CFS might assist clinicians with immediate clinical decision-making and realistic goal setting.49 The authors also highlighted that where the decision is for admission, higher levels of frailty can assist channel the older adult to frailty-attuned ward environments where CGA is available. In our study, the ISAR tool29 was included in our pre-defined inclusion criteria to stratify a cohort of older adults at risk of adverse outcomes and to focus resource-allocation of CGA to those in greatest need. Acknowledging the challenges imposed by time-based targets in the ED environment, clinicians and researchers should be guided by pragmatic and feasibility factors related to the use of frailty screening tools in the ED.50
Future research focused on CGA in the ED should be underpinned by an RCT methodology as it is the most appropriate study design to answer a research question related to a complex intervention.51
The 2017 Cochrane review by Ellis et al21 on the effectiveness of CGA for older adults admitted to hospital should serve as a reference standard when describing the core team and components of CGA in future research studies. In their review, they outline the following components: clinical leadership, structured assessment, multidisciplinary team meetings, goal setting, involving patients and carers in goal setting, outpatient follow-up, ward environment, adequate time, specialty knowledge, experience and competence, and tailoring treatment plans to the individual. Application of this reporting template will serve as a roadmap for successful implementation of similar models of care in the future and will enhance transparency of reporting CGA studies.
Strengths and Limitations
The study adopted a longitudinal approach to exploring older adults’ outcomes following index ED attendance and in doing so explored the interface between primary-secondary care. The model of CGA was well described, and we included a comprehensive range of key outcome measures, which explored the impact of CGA in the ED at both the patient and process level. In particular, the study was strengthened by the use of patient-reported outcome measures, and, to the best of our knowledge, this is the first evaluation of CGA in the ED to incorporate a person-centered perspective rather than focusing on process outcomes only. Furthermore, our low attrition rate at 30- and 180-day follow-up adds to our confidence in findings.
However, there are limitations to observational studies of this type. The lack of randomization and comparison data in the form of a control group is an inherent limitation of observational studies.52 While our analyses controlled and adjusted for a number of confounding factors, the interplay of such factors and the effect of the exposure and outcomes cannot be ruled out. Participants were recruited during the operational hours (08:00–17:00) of the interdisciplinary team on a Monday-Friday basis, which presents limitations with respect to a representative sample of the target population whereby older adults who presented out-of-hours were excluded from recruitment. Finally, the study was conducted at a single-center tertiary hospital, which may constrain the generalizability of findings to international healthcare systems.
Conclusion
CGA in the ED may improve outcomes by mitigating against the adverse effects of potentially avoidable hospital admissions and focusing on integration of services across the continuum of care. The outcome at the index ED attendance was a significant predictor of adverse outcomes whereby those who were discharged home had significantly lower odds of multiple adverse outcomes at 30- and 180-day follow-up. Two out of three older adults experienced functional decline during the course of hospitalization. However, older adults who were admitted to hospital following the index ED attendance had lower levels of functional ability as measured via the BI compared to those who were discharged home at index. One out of four older adults experienced an unscheduled ED re-attendance and hospital admission at 180-day follow-up; higher levels of frailty as measured via the CFS resulted in a greater probability of unscheduled hospital and NH admission at this time-point. Future research on CGA in the ED should be underpinned by an RCT methodology.
Data Sharing Statement
All deidentified data files and data dictionary, and no analytic code can be obtained by contacting the corresponding author.
Consent for Publication
Written informed consent was obtained from all participants who were recruited during the duration of the study.
Acknowledgments
The corresponding author is grateful to all the older adults and those important to them who were recruited to this study and engaged in follow-up after their ED attendance. She is also grateful to all the co-authors who shared their time and expertise during the period of study completion.
Author Contributions
ÍO’S was responsible for conceptualization of the study, design of the work, analysis, and interpretation of the data, and writing the initial draft of the manuscript. RG obtained research grant funding and was responsible for conceptualization of the study, design of the work, analysis and interpretation of the data, supervision, and revised the manuscript from a critical perspective to enhance its contents. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Research Board (HRB) of Ireland (Health Research Board, Grattan House 67-72 Lower Mount Street, Dublin 2, D02 H638 under the HRB Research Leader Award RL-2020-010). The funder had no role in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ukkonen M, Jämsen E, Zeitlin R, Pauniaho SL. Emergency department visits in older patients: a population-based survey. BMC Emerg Med. 2019;19(1):1–8. doi:10.1186/s12873-019-0236-3
2. Samaras N, Chevalley T, Samaras D, Gold G. Older patients in the emergency department: a review. Ann Emerg Med. 2010;56(3):261–269. doi:10.1016/j.annemergmed.2010.04.015
3. Morley C, Unwin M, Peterson GM, et al. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316
4. Salisbury C. Multimorbidity: redesigning health care for people who use it. Lancet. 2012;380:7–9. doi:10.1016/S0140-6736(12)60482-6
5. Rockwood K, Theou O. Using the clinical frailty scale in allocating scarce health care resources. Can Geriatr Jl. 2020;23(3):210. doi:10.5770/cgj.23.463
6. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381:752–762. doi:10.1016/S0140-6736(12)62167-9
7. Adja KYC, Lenzi J, Sezgin D, et al. The importance of taking a patient-centered, community-based approach to preventing and managing frailty: a public health perspective. Front Public Health. 2020;8:599170. doi:10.3389/fpubh.2020.599170
8. Cottey L, Smith J, Whiting C on behalf of the JLA EM PSP Steering Group. A Refresher for Emergency Medicine; 2023. Available from: https://www.jla.nihr.ac.uk/news/a-refresh-for-emergency-medicine/32639.
9. Brouns SHA, Stassen PM, Lambooij SLE, Dieleman J, Vanderfeesten ITP, Haak HR. Organisational factors induce prolonged emergency department length of stay in elderly patients – a retrospective cohort study. PLoS One. 2015;10(8):e0135066. doi:10.1371/journal.pone.0135066
10. Nagurney JM, Fleischman W, Han L, Leo-Summers L, Allore HG, Gill TM. Emergency department visits without hospitalization are associated with functional decline in older persons. Ann Emerg Med. 2017;69(4):426–433. doi:10.1016/j.annemergmed.2016.09.018
11. Lowthian JA, McGinnes RA, Brand CA, Barker AL, Cameron PA. Discharging older patients from the emergency department effectively: a systematic review and meta-analysis. Age Ageing. 2015;44(5):761–770. doi:10.1093/ageing/afv102
12. Khandelwal D, Goel A, Kumar U, Gulati V, Narang R, Dey AB. Frailty is associated with longer hospital stay and increased mortality in hospitalized older patients. J Nutr Health Aging. 2012;16(8):732–735. doi:10.1007/s12603-012-0369-5
13. Brousseau AA, Dent E, Hubbard R, et al. Identification of older adults with frailty in the Emergency Department using a frailty index: results from a multinational study. Age Ageing. 2018:242–248. doi:10.1093/ageing/afx168
14. Jørgensen R, Brabrand M. Screening of the frail patient in the emergency department: a systematic review. Eur J Intern Med. 2017;45:71–73. doi:10.1016/j.ejim.2017.09.036
15. O’Caoimh R, McGauran J, O’Donovan MR, et al. Frailty screening in the emergency department: comparing the variable indicative of placement risk, clinical frailty scale and PRISMA-7. Int J Environ Res Public Health. 2022;20:290. doi:10.3390/ijerph20010290
16. Leahy A, Corey G, Purtill H, et al. Screening instruments to predict adverse outcomes for undifferentiated older adults attending the emergency department: results of SOAED prospective cohort study. Age Ageing. 2023;52(7):afad116. doi:10.1093/ageing/afad116
17. Galvin R, Gilleit Y, Wallace E, et al. Adverse outcomes in older adults attending emergency departments: a systematic review and meta-analysis of the Identification of Seniors At Risk (ISAR) screening tool. Age Ageing. 2017;46(2):179–186. doi:10.1093/ageing/afw233
18. Apóstolo J, Cooke R, Bobrowicz-Campos E, et al. Predicting risk and outcomes for frail older adults: an umbrella review of frailty screening tools. JBI Database Syst Rev Implement Rep. 2017;15:1154. doi:10.11124/JBISRIR-2016-003018
19. Rubenstein LZ, Stuck AE, Siu AL, Wieland D. Impacts of geriatric evaluation and management programs on defined outcomes: overview of the evidence. J Am Geriatr Soc. 1991;39(9 Pt 2):8S–16S;discussion 17S–18S. doi:10.1111/j.1532-5415.1991.tb05927.x
20. Parker SG, McCue P, Phelps K, et al. What is comprehensive geriatric assessment (CGA)? An umbrella review. Age Ageing. 2018;47:149–155. doi:10.1093/ageing/afx166
21. Ellis G, Gardner M, Tsiachristas A, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2017;9:CD006211. doi:10.1002/14651858.CD006211.pub3
22. Van Craen K, Braes T, Wellens N, et al. The effectiveness of inpatient geriatric evaluation and management units: a systematic review and meta-analysis. J Am Geriatr Soc. 2010;58:83–92. doi:10.1111/j.1532-5415.2009.02621.x
23. O’Shaughnessy Í, Robinson K. Effectiveness of acute geriatric unit care on functional decline, clinical and process outcomes among hospitalised older adults with acute medical complaints: a systematic review and meta-analysis. Age Ageing. 2022;51:1–11. doi:10.1093/ageing/afac081
24. Conroy SP, Stevens T, Parker SG, Gladman JR. A systematic review of comprehensive geriatric assessment to improve outcomes for frail older people being rapidly discharged from acute hospital: ‘interface geriatrics’. Age Ageing. 2011;40:436–443. doi:10.1093/ageing/afr060
25. Harding S. Comprehensive geriatric assessment in the emergency department. Age Ageing. 2020;49:936–938. doi:10.1093/ageing/afaa059
26. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/j.ijsu.2014.07.013
27. O’Shaughnessy Í, Robinson K. Comprehensive geriatric assessment in the emergency department: a protocol for a prospective cohort study. HRB Open Res. 2022;5:26. doi:10.12688/hrbopenres.13504.2
28. Mackway-Jones K. Emergency Triage. London: BMJ Publishing Group; 1997.
29. McCusker J, Bellavance F, Cardin S, Trepanier S, Verdon J, Ardman O. Detection of older people at increased risk of adverse health outcomes after an emergency visit: the ISAR screening tool. J Am Geriatr Soc. 1999;47(10):1229–1237. doi:10.1111/j.1532-5415.1999.tb05204.x
30. Health Research Board: data Protection Act 2018 (Section 36(2)) (Health Research) Regulations 2018; 2018. Available from: https://www.hrb.ie/funding/gdpr-guidance-for-researchers/health-research-regulations-2018/.
31. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
32. Wade DT, Collin C. The Barthel ADL Index: a standard measure of physical disability? Int Disabil Stud. 1988;10(2):64–67. doi:10.3109/09638288809164105
33. Bellelli G, Morandi A, Davis DH, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people. Age Ageing. 2014;43:496–502. doi:10.1093/ageing/afu021
34. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–343. doi:10.3109/07853890109002087
35. Marshall GN, Hays RD: The Patient Satisfaction Questionnaire Short Form (PSQ-18). Santa Monica, CA: Rand; 1994. Available from: https://www.rand.org/content/dam/rand/pubs/papers/2006/P7865.pdf.
36. Cassarino M, Robinson K, Trépel D, et al. Impact of assessment and intervention by a health and social care professional team in the emergency department on the quality, safety, and clinical effectiveness of care for older adults: a randomised controlled trial. PLoS Med. 2021;18(7):e1003711. doi:10.1371/journal.pmed.1003711
37. Kennelly SP, Drumm B, Coughlan T, Collins R, O’Neill D, Romero-Ortuno R. Characteristics and outcomes of older persons attending the emergency department: a retrospective cohort study. QJM. 2014;107(12):977–987. doi:10.1093/qjmed/hcu111
38. O’Shaughnessy Í, Romero-Ortuno R, Edge L, et al. Home FIRsT: interdisciplinary geriatric assessment and disposition outcomes in the emergency department. Eur J Intern Med. 2021;85:50–55. doi:10.1016/j.ejim.2020.11.015
39. Hobbins A, Barry L, Kelleher D, et al. Utility values for health states in Ireland: a value set for the EQ-5D-5L. Pharmacoeconomics. 2018;36:1345–1353. doi:10.1007/s40273-018-0690-x
40. Jay S, Whittaker P, Mcintosh J, Hadden N. Can consultant geriatrician led comprehensive geriatric assessment in the emergency department reduce hospital admission rates? A systematic review. Age Ageing. 2017;46(3):366–372. doi:10.1093/ageing/afw231
41. Brown CJ. After three decades of study, hospital-associated disability remains a common problem. J Am Geriatr Soc. 2020;68(3):465–466. doi:10.1111/jgs.16349
42. Covinsky KE, Pierluissi E, Johnston CB. Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure”. JAMA. 2011;306(16):1782–1793. doi:10.1001/jama.2011.1556
43. Loyd C, Markland AD, Zhang Y, et al. Prevalence of hospital-associated disability in older adults: a meta-analysis. J Am Med Dir Assoc. 2020;21(4):455–461. doi:10.1016/j.jamda.2019.09.015
44. O’Shaughnessy Í, Fitzgerald C, Hayes C, et al. Stakeholders’ experiences of CGA in an inpatient hospital setting: a qualitative systematic review and meta-ethnography. BMC Geriatr. 2023;1:4.
45. Conroy S, Ferguson C, Woodard J, Banerjee J. Interface geriatrics: evidence-based care for frail older people with medical crises. Br J Hosp Med. 2010;71(2):98–101. doi:10.12968/hmed.2010.71.2.46488
46. Department of Health 2021 Sláintecare implementation strategy and action plan 2021–2023. Dublin: Government of Ireland; 2021. Available from: https://www.gov.ie/en/publication/6996b-slaintecare-implementation-strategy-and-action-plan-2021-2023/.
47. Preston L, van Oppen JD, Conroy SP, Ablard S, Buckley Woods H, Mason SM. Improving outcomes for older people in the emergency department: a review of reviews. Emerg Med J. 2020;38:882–888. doi:10.1136/emermed-2020-209514
48. Boucher EL, Gan JM, Rothwell PM, Shepperd S, Pendlebury ST. Prevalence and outcomes of frailty in unplanned hospital admissions: a systematic review and meta-analysis of hospital-wide and general (internal) medicine cohorts. EClinicalMedicine. 2023;59:101947. doi:10.1016/j.eclinm.2023.101947
49. Elliott A, Taub N, Banerjee J, et al. Does the clinical frailty scale at triage predict outcomes from emergency care for older people? Ann Emerg Med. 2021;77(6):620–627. doi:10.1016/j.annemergmed.2020.09.006
50. Elliott A, Hull L, Conroy SP. Frailty identification in the emergency department-a systematic review focussing on feasibility. Age Ageing. 2017;46(3):509–513. doi:10.1093/ageing/afx019
51. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. BMJ. 2021;374:n2061. doi:10.1136/bmj.n2061
52. Kingston A, Jagger C. Review of methodologies of cohort studies of older people. Age Ageing. 2018;47(2):215–219. doi:10.1093/ageing/afx183
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.