")
Back to Journals » Research and Reports in Neonatology » Volume 14
Congenital Malaria in a 20-Day-Old Neonate: A Case Report and Literature Review
Authors Regasa MT , Shibiru T, Tilahun T , Bayisa G, Negari GK
Received 19 December 2023
Accepted for publication 23 February 2024
Published 26 February 2024 Volume 2024:14 Pages 39—42
DOI https://doi.org/10.2147/RRN.S452965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Schelonka
Misganu Teshoma Regasa,1 Tesfaye Shibiru,2 Temesgen Tilahun,3 Gedefa Bayisa,4 Gemechis Kebede Negari2
1Department of Midwifery, Institute of Health Sciences, Wallaga University, Nekemte, Ethiopia; 2Department of Pediatrics and Child Health, School of Medicine, Wallaga University, Nekemte, Ethiopia; 3Department of Obstetrics & Gynecology, Institute of Health Sciences, Wallaga University, Nekemte, Ethiopia; 4Emergency Quality Officer, Wallaga. University Referral Hospital, Wallaga University, Nekemte, Ethiopia
Correspondence: Misganu Teshoma Regasa, Department of Midwifery, Institute of Health Sciences, Wallaga University, P.O Box: 395, Nekemte, Ethiopia, Tel +251917674952, Email [email protected]
Background: Congenital malaria is a relatively rare condition where the Plasmodium parasite is transmitted from the mother to the fetus during pregnancy. It is associated with a high fatality rate if it is not promptly diagnosed and treated.
Case Summary: We report an unusual case of a 20-day-old male baby with Plasmodium vivax malaria from Western Ethiopia, suspected primarily on the basis of positive maternal history that mother had attacks of malaria in the 3rd, 5th, and 8th months of gestation and was cured with artemether-lumefantrine therapy. Infant presented with vomiting and a high-grade fever. The blood film of the baby showed trophozoites stage of Plasmodium vivax with a parasite density of +3. The neonate had severe thrombocytopenia (49,000/micro liter) and Splenomegaly (spleen was palpable 2cm along its line of growth). The patient was admitted to the hospital and treated with artesunate for five days and discharged on the sixth day of admission in stable condition.
Conclusion: Sick neonates born to mothers in malaria-endemic areas or with a history of malaria attack(s) in the index pregnancy should be promptly investigated for malaria.
Keywords: congenital malaria, case, report, western Ethiopia, plasmodium vivax
Introduction
Congenital malaria refers to the transmission of malaria from an infected mother to her unborn child during pregnancy. This can happen if the mother experiences malaria symptoms during pregnancy, but it can also occur in cases where the mother is asymptomatic, making it difficult to diagnose both in the mother and the newborn.1,2 It is a rare but serious condition that can result in significant morbidity and mortality in neonates.1 Plasmodium falciparum is the most prevalent species involved in congenital malaria; however, Plasmodium vivax and Plasmodium malariae can also be involved.2
It is a rare condition that should be included in the differential diagnosis of neonatal infections, sepsis, unexplained fever, or infants presenting with hemolytic anaemia, jaundice, or hepatosplenomegaly in malaria endemic zones.3 Early diagnosis is essential for prompt treatment and may prevent an unfavorable outcome. Early diagnosis of congenital malaria includes the availability and accuracy of diagnostic tests, as well as the potential for false-negative results. Additionally, some infants may not show symptoms of infection until several weeks after birth, which can delay diagnosis and treatment. In general, early diagnosis of congenital malaria involves screening pregnant women for malaria infection, testing newborns for congenital malaria, monitoring for symptoms, and promptly treating any positive cases.3–5 Here we present a case of a neonate with congenital malaria.
Case Presentation
This is a 20-day-old male neonate who was born to a 22-year-old para-I (woman who has been delivered of a child for the first time) mother from Western Ethiopia. The mother had four antenatal care (ANC) contacts at the health center. The mother had received routine care during pregnancy, including the tetanus vaccine, deworming, iron supplementation, and nutritional advice. But she was not provided with insecticide treated mosquito nets. During the index pregnancy, the mother had attacks of malaria in the 3rd, 5th, and 8th months of gestation. She was treated with artemether/lumefantrine as an outpatient. The mother had no history of urinary tract infections, sexually transmitted infections, or other chronic medical problems.
After nine months of amenorrhea, the mother presented to the nearby health center with labour pain. She was evaluated and admitted with the active phase of the 1st stage of labour. The labour progressed smoothly, and she gave birth vaginally to a male, alive neonate with good conditions. The neonate received basic newborn care. Breastfeeding was initiated within one hour of delivery. On the next day, the mother and the neonates were discharged from the health center with good conditions and the necessary advice.
On the 20th day postpartum, the neonate presented to the nearby Health center with vomiting, and a high-grade fever for one day. However, the neonate had no history of fast breathing, no history of abnormal body movement, and no history of yellowish discoloration of the eyes and skin. At the Health Centre, blood film (BF) was done and showed trophozoite of P. vivax. Then, the patient was referred to Wallaga University Referral Hospital for further evaluation and management after paracetamol suppository was inserted for the high-grade fever.
On examination, the neonate was acutely sick-looking. His vital signs were pulse rate (PR) = 160 beats per minute, respiratory rate (RR) = 48 breaths per minute, a temperature of 37.6°C, oxygen saturation = 96%, weight = 3000 grammes, height = 53 centimeters, and head circumference = 36 centimeters. He had pink conjunctiva. The neonate had Splenomegaly (Spleen was palpable 2cm along its line of growth). The lymph glandular system, respiratory system, cardiovascular system, and genitalia were normal. On neurologic examination, all the neonatal reflexes were intact. At Wallaga University Referral Hospital, blood film (BF) was repeated and showed trophozoites stage of Plasmodium vivax with a parasite density of +3. parasite density means that there are a large number of parasites present in the blood sample, indicating a severe infection. The scale ranges from 0 to 4+, with 0 indicating no parasites seen and 4+ indicating a very high number of parasites present in the blood. Neonate had severe thrombocytopenia (49,000/micro liter) (Table 1).
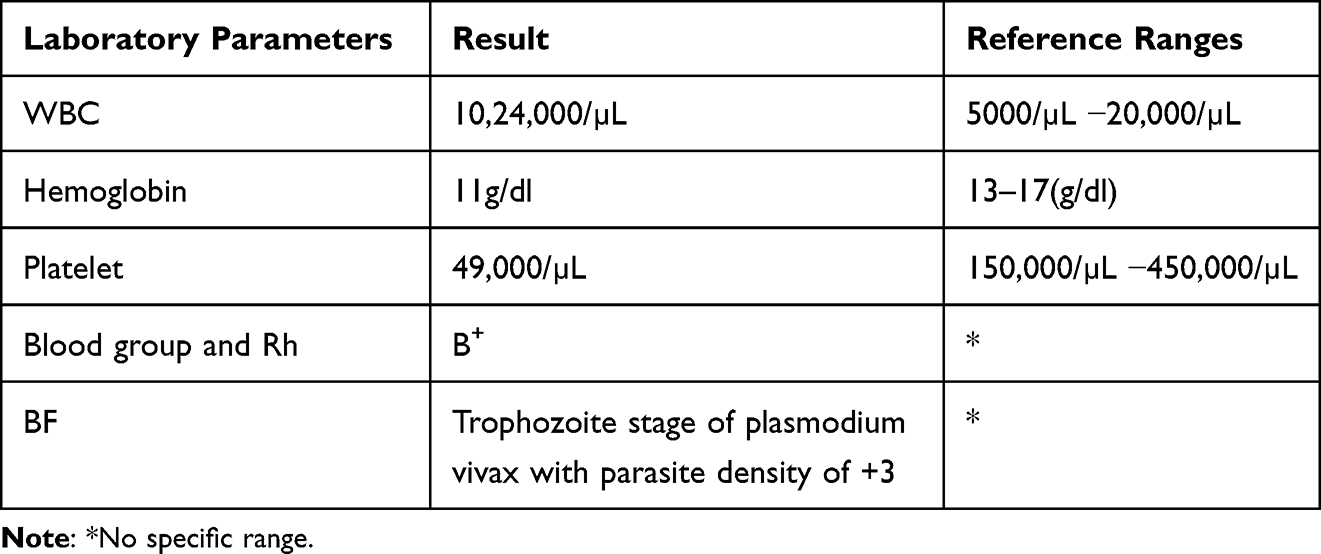 |
Table 1 Laboratory Investigation Results of a 20-Day-Old Neonate at Wallaga University Referral Hospital, Western Ethiopia, 2023 |
With the final diagnosis of congenital malaria, the neonate was admitted with congenital malaria and treated with artesunate 3mg/kg IV at admission, 12 hours later, 24 hours later, and then daily for five days. On the sixth day, the neonate showed significant improvement and was discharged with advice on prevention of malaria and postpartum follow-up.
Discussion
Malaria is a parasitic disease that is spread by female Anopheles mosquitoes during their blood meals. It is caused by a protozoan parasite belonging to the genus Plasmodium, which has five different species. In this particular case report, the neonate was diagnosed with P. Vivax as the underlying cause of malaria. Congenital malaria is a rare condition where the plasmodium parasite is transmitted from the mother to the fetus during pregnancy. It is important to note that the onset of signs may be delayed. This delay can be attributed to several factors, including the transmission of the infection in late pregnancy or during delivery, or the presence of maternal antibodies (IgG) that were acquired trans placentally. In cases where the mother has been infected with malaria during pregnancy, the parasite can cross the placenta and infect the fetus. This can occur at any stage of pregnancy, but it is more likely to happen in the later stages. The presence of maternal antibodies (IgG) acquired trans placentally can also play a role in delaying the onset of signs in newborns with congenital malaria. These antibodies can provide some protection against the infection, but they may not be enough to prevent the development of signs in all cases.5–9 In our case, the neonate presented to the health center within a day of onset of the signs, and the diagnosis was made on arrival. The referral to a better facility and initiation of treatment were completed on time. This early diagnosis and treatment might explain the good outcome.
Congenital malaria occurs when the mother has an active malaria infection during pregnancy, and the parasite crosses the placenta and infects the fetus.6 In our case, the mother of the neonate had repeated attacks of malaria during pregnancy at the 3rd, 5th, and 8th months of gestation.
Congenital malaria can be difficult to diagnose because the signs are nonspecific and might mimic other neonatal infections. However, Presence of fever, anemia, and splenomegaly is a pointer towards congenital malaria.10 In our case, the neonate presented with vomiting, and a high-grade fever of one day duration and the neonate had splenomegaly (spleen was palpable 2cm along its line of growth). CBC result also indicates severe thrombocytopenia (49,000/micro liter). At the same time the mother had repeated malaria attack during the index pregnancy. Therefore, malaria endemic areas or travel histories, a high index of suspicion is very important to diagnose malaria, as noted in this case. Therefore, we highlight the importance of considering congenital malaria as a differential diagnosis of neonatal sepsis in neonates born to mothers from malaria endemic areas, with travel history, or with a history of malaria attack during pregnancy.
Prevention of congenital malaria is essential. It can be prevented by using insecticide-treated bed nets and protective clothing, and by prompt diagnosis and treatment of malaria in pregnant women.6,8,10 In our case, the mother was not provided with insecticide treated bed nets. This led her to have repeated attacks of malaria, which were treated with artemether/lumefantrine.
Conclusion
In conclusion, congenital malaria is a serious condition that can have detrimental effects on newborns. It is important to note that newborns born to mothers in malaria-endemic areas or who have a history of malaria attack(s) during pregnancy are at a higher risk of developing congenital malaria. Therefore, sick neonates born to mothers in malaria-endemic areas or history of malaria attack(s) in the index pregnancy should be promptly investigated for malaria.
Abbreviations
ANC, antenatal care; BF, blood film; CBC, Complete blood count.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Research Ethics Review Committee of Wallaga University Referral. The study protocol is performed per the relevant guidelines.
Consent for Publication
Written informed consent was obtained from parent of the patient for publication of this case report and any accompanying images.
Acknowledgment
We thank the parent of the patient for allowing the publication of this case report. Institutional approval not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
No funding source.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mbanzulu P, Kapepela K, Organization WH. Paludisme congénital clinique à la maternité des cliniques universitaires du Mont Amba à Kinshasa, Zaire. World Health Organization; 1988.
2. Tahirou I, Zara M, Moustapha M, et al. Congenital malaria and its associated factors at issaka gazobi maternity of Niamey in Niger. Int J Pediatr. 2020;2020:1–6. doi:10.1155/2020/7802560
3. Rai P, Majumdar K, Sharma S, Chauhan R, Chandra J. Congenital malaria in a neonate: case report with a comprehensive review on differential diagnosis, treatment and prevention in Indian perspective. J Parasitic Dis. 2015;39(2):345–348. doi:10.1007/s12639-013-0342-1
4. Olupot-Olupot P, Eregu EI, Naizuli K, Ikiror J, Acom L, Burgoine K. Neonatal and congenital malaria: a case series in malaria endemic eastern Uganda. Malaria j. 2018;17(1):1–5. doi:10.1186/s12936-018-2327-0
5. Del Castillo Calderón JG, Cárdenas Silva AM. Malaria congénita por Plasmodium falciparum. Revista Chilena de Pediatría. 2020;91(5):749–753. doi:10.32641/rchped.v91i5.1283
6. Organization WH. Guidelines for the Treatment of Malaria. World Health Organization; 2015.
7. Pengsaa K. Congenital malaria in Thailand. Annals of tropical paediatrics. Annals Tropl Paedi. 2007;27(2):133–139. doi:10.1179/146532807X192507
8. Akindele J, Sowunmi A, Abohweyere A. Congenital malaria in a hyperendemic area: a preliminary study. Ann Trop Paediatrics. 1993;13(3):273–276. doi:10.1080/02724936.1993.11747658
9. McGregor IA. Epidemiology, malaria and pregnancy. American JTrop Med Hyg. 1984;33(4):517–525. doi:10.4269/ajtmh.1984.33.517
10. Bhatia R, Rajwaniya D, Agrawal P. Congenital malaria due to plasmodium vivax infection in a neonate. Case Report Pedi. 2016;2016:1–2. doi:10.1155/2016/1929046
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.