")
Back to Journals » Clinical Interventions in Aging » Volume 19
Consequences of Anorexia of Aging in Hospital Settings: An Updated Review
Authors Cox NJ
Received 1 December 2023
Accepted for publication 27 February 2024
Published 11 March 2024 Volume 2024:19 Pages 451—457
DOI https://doi.org/10.2147/CIA.S431547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Natalie J Cox1,2
1Academic Geriatric Medicine, Faculty of Medicine, University of Southampton, Southampton, UK; 2NIHR Applied Research Collaboration (ARC) Wessex, University of Southampton, Southampton, UK
Correspondence: Natalie J Cox, Academic Geriatric Medicine, Faculty of Medicine, University of Southampton, Mail Point 807, University Hospital Southampton, Tremona Road, Southampton, SO16 6YD, UK, Email [email protected]
Abstract: The anorexia of aging is a widespread problem amongst older people, particularly in the hospital setting with up to 60% affected. Despite its high prevalence anorexia often goes undiagnosed in hospital, due to a lack of standardized assessment and evidence-based management, but also lack of knowledge regarding consequences. This review summarizes current evidence for anorexia of aging specific to the hospital setting, giving an overview of correlates of appetite in hospital and consequences of anorexia. It highlights an overall scarcity of research on this important clinical problem for hospitalized cohorts. The few studies point to the importance of anorexia of aging in major health burdens for older people, namely malnutrition, sarcopenia and reduced physical performance, as well as higher mortality. Further research is needed to assess temporal sequence in pathways of causality and to develop effective interventions to combat anorexia.
Keywords: appetite, older people, outcomes, sarcopenia
Introduction
The anorexia of aging is often used to describe appetite loss in older people attributable to aging, rather than a disease-specific symptom.1 It is a multi-faceted phenomenon driven by alterations to physiological mechanisms of energy balance, psychological processes of reward and socioenvironmental cues for eating behaviour.2 Changes to gut hormone signalling which augment feelings of satiety is a now well-established physiological mechanism,3 with chronic pro-inflammatory states and the potential for gut dysbiosis also of interest.4 Alongside this, altered sensory perception (such as reduced taste5) diminishes food-reward, and changes in life circumstance can reduce desire to eat.6
Anorexia in older populations is common but prevalence varies across settings, with estimates of 11–28% in the community, 12–22% in care homes and a rapid rise to 30–60% in hospital.7–11 Even though the anorexia of aging is a common clinical conundrum in hospital, it is often not routinely assessed and diagnosed. This is due to several factors, firstly a lack of consensus on its assessment, with use of different scales or proxy measures such as food intake, or weight, which blurs the line between anorexia and malnutrition.12 However, the Council on Nutrition Appetite Questionnaire (CNAQ), and in particular, its shortened derivative the 4-item Simplified Nutritional Appetite Questionnaire (SNAQ),13 which gives a score out of 20 (<14 suggestive of anorexia) is being increasingly utilized in clinical research settings. Thus it may represent a tool feasible to use in hospital. Additionally, a lack of knowledge regarding the implications of anorexia of aging on health outcomes, alongside scarcity of evidence for management strategies to address the problem when identified, also hinders progress in routine clinical practice.14,15
Given the high prevalence of anorexia in older hospital populations, it is important to understand appetite-related factors in this setting. The multi-dimensional nature of anorexia of aging and effects of environmental cues, also means that the syndrome should be considered in each setting, as findings may not translate from other cohorts. This review aims to give an up-to-date perspective on factors associated with appetite and consequences of the anorexia of aging specific to the hospital setting, which will include acute and rehabilitation (see Supplementary Material S1 for evidence search structure). By highlighting potential consequences of anorexia in hospitalized older people, this may improve rates of diagnosis in this clinical setting, where research shows prevalence is high, and demonstrate the need for future clinical research on interventions for this common problem.
Factors Associated with Anorexia in the Hospital Setting
Physical factors related to eating have been the most described correlates with appetite in hospital. The effect of oral health is notable and a recent study in Japanese rehabilitation patients noted anorexia (defined as SNAQ13 score ≤14) was associated with 2.7 times the odds of poorer oral health status using the Oral Health Assessment Tool (OHAT).16 The OHAT assesses the status of the teeth, mucous membranes, and saliva, with different subcategories. In this study the subcategories of poorer oral cleanliness and presence of dentures were associated with anorexia. This mirrors findings by Donini et al,17 who observed older adults in hospital and rehabilitation settings in Italy with anorexia had a lower number of natural teeth (5±7 vs 10±11), with anorexia defined as ≥ 3 days of reduction in food intake ≥ 50% of a standard meal in the absence of physical factors limiting eating. The presence of chewing difficulty and dysphagia was also observed to associate with anorexia in this study cohort,17 as well as in a group of older Danish adults attending an emergency department (using SNAQ13 score <14).18 In addition, use of texture modified diets (defined as International Dysphagia Diet Standardization Initiative (IDDSI) levels 3 to 5) has also been shown in a Japanese study to increase likelihood of anorexia (odds ratio 3.443).19 Other physical factors related to appetite in hospital include the presence of pain and constipation17 as well as lower cognition16 and the presence of polypharmacy (defined in the study as ≥5 different medications).20
The role of inflammation and associated inflammatory cytokines relating to anorexia is pertinent to consider in the hospital setting. This has been explored in observational studies, with cross-sectional associations between higher C-reactive protein (CRP) and reduction in food intake in older inpatients.17,21 A further longitudinal study on German older inpatients explored appetite (defined by two methods: The first domain in the SNAQ questionnaire13 and the appetite domain of the Edmonton Symptom Assessment System (ESAS) palliative care symptom assessment tool22) and inflammatory marker levels at baseline and seven days.23 They again observed a significant association between changes in CRP level and level of appetite for the study population independent of the effects of presence of infection or chronic inflammatory disease, age and sex (coefficients not specified). When looking further at inflammatory cytokines, there were differences depending on the method of appetite assessment between ESAS and SNAQ on comparing changes in mean concentration with appetite level, with changes to IL-6 and IL-18 associated with change in ESAS-appetite and IL-10 and IL-33 associated with changes in SNAQ-appetite level.24 When modelling associations, changes in IL-18 levels were the major independent predictor for changes of patients’ appetite according to ESAS-appetite accounting for age, sex, infection, and disease.24 Higher circulating inflammatory markers have also been linked to anorexia in community dwelling older adults,25 suggesting a wider role of chronic inflammation and potential immunosenescence aside from the effects of acute illness, which warrant further investigation.4
Mood is widely described as associated with level of appetite in men and women across settings. In hospital, lower levels of mood when assessed using the Geriatric Depression Scale Short Form 1526 are associated with poorer appetite when measured using the SNAQ.10,13,20,27 These lower mood states do not reach thresholds constituting a diagnosis of depression (median scores from all the studies were 4 out of 15, with threshold of ≥5 for depression26), raising the risk of being overlooked. Although clinical diagnosis is also associated with appetite in the community28 and the lack of evidence in hospital is likely in part due to paucity of studies. Lower mood is linked to the hedonic aspect of appetite, which encompasses the reward and pleasure in consuming food, driving desire to initiate or continue eating.2 Importantly, there is a lack of research exploring the effects of acute illness and inflammation on mood and hence potentially appetite in hospitalized older people, which would be a key factor in this setting.
Physical activity has also been linked with appetite, including in hospitalized populations. Survey data using the Physical Activity Scale for the Elderly (PASE)29 demonstrated higher amounts of physical activity in the week prior to hospital admission was associated with better appetite (measured with the SNAQ13) in United Kingdom (UK) older inpatients.27 Habitual physical activity is postulated to attune a person’s response to their appetite physiological signaling mechanisms, ensuring they consume amounts appropriate to need.30 However, this relationship is likely to be more complex for those in later life given effects of aging on appetite physiological signaling mechanisms.31 A link between physical activity level during hospital admission and appetite is currently unclear, yet it is an important unmet area in research, given the notably lower levels of activity during hospital stay.32
Consequences of Anorexia of Aging in the Hospital Setting
A large amount of the information regarding potential consequences of anorexia in the hospital setting comes from cross-sectional observational studies, hence the basis of the observations as consequential are mostly theoretical. There are some longitudinal data giving temporal sequence and suggestion of causality, however the area overall is still limited by a lack of research.
Malnutrition
Malnutrition in hospital is a considerable problem, with a prevalence of 20–50% (older adults are over-represented within this) and nutritional decline during hospital stay present in 10–65%.33 This nutritional decline, with greater levels of malnutrition on discharge from hospital, puts individuals at greater risk of poor health outcomes, including readmission (termed the malnutrition carousel). Cross-sectional observations within older hospital populations have identified an association between malnutrition and malnutrition risk with anorexia. A diagnosis of malnutrition using the Global Leadership Initiative on Malnutrition (GLIM) defined criteria34 had threefold higher odds in Japanese older inpatients with anorexia, even after adjusting for number of medications, cognition, grip strength, functional independence, and swallow ability.16
Use of malnutrition risk screening tools have also demonstrated association of higher risk with anorexia in hospitalized older adults. A study conducted in the Netherlands20 assessed malnutrition risk using the Short Nutritional Assessment Questionnaire (SNAQ(M)),35 with a score of ≥3 indicating malnutrition. The authors identified those with anorexia were more likely to be malnourished, however they defined anorexia using the appetite domain within the SNAQ(M) itself. Nonetheless, in a UK based study of older female inpatients higher level of malnutrition risk (assessed by the Malnutrition Universal Screening Tool (MUST)36) was also associated with anorexia (defined as SNAQ <14), with double the odds compared with those without anorexia.10 In addition, assessment of malnutrition risk using the Mini Nutritional Assessment (MNA)37 in Italian inpatients identified a higher prevalence of greater malnutrition risk in those with anorexia (screening scores of 6.9 ±2 vs 10.5 ±2 without anorexia).17
When looking at other nutritional parameters, which might be considered proxy measures for malnutrition, associations with anorexia in hospitalized older people are also observed. Body Mass Index (BMI) is consistently lower in hospitalized populations with anorexia, as well as lower levels of nutritional biomarkers.10,16,17 One study in Japanese inpatients assessed the association between anorexia (defined subjectively by the patient, family or healthcare staff) and vitamin B12 deficiency, finding that anorexia was associated with greater odds of B12 deficiency, independent of the effects of age, albumin levels, alcohol consumption, hepatic cirrhosis, loop diuretics, diabetes, chronic kidney disease, and dementia.38 These findings highlight potential deficiencies in qualitative nutrition due to dietary insufficiency, which may be overlooked. Donini et al, explored this further by assessing eating patterns in their hospitalized older population, identifying that those with anorexia consumed significantly less protein-rich foods and had higher usage of dietary supplements.17 This suggests a mechanism through which anorexia may lead to nutritional decline and malnutrition.
Sarcopenia
Sarcopenia in the older population is of great importance due to its relationship with reduced independence, falls, mortality, and healthcare utilisation.39 The hospital setting is particularly important because of illness or injury and sedentary behaviour leading to deconditioning and accelerated loss of muscle mass and function, acknowledged through the concept of acute sarcopenia.39 In the cross-sectional studies on appetite in the hospital setting, participants with anorexia often showed reduced hand grip strength compared with those with normal appetite.10,16,17,20 In addition, the study by Van Dronkelaar et al, on older inpatients in the Netherlands, demonstrated poorer appetite (measured by the appetite domain in the SNAQ(M)35) during admission was a predictor of reduced muscle strength 3 months post hospital discharge, including when adjusted for the effects of age, sex, cognitive impairment, fatigue, depression, comorbidity and skeletal muscle mass.20
Muscle mass has not been demonstrated to correlate with appetite in hospital populations, a finding which mirrors that of community cohorts.40,41 This may be due to limitations in the measurement of muscle mass, which has led to alterations in current European guidance on the diagnosis of sarcopenia, recommending muscle strength as a more meaningful marker.39 It has also been suggested that reduced muscle strength associated with anorexia may be related to dietary alterations, qualitative nutrition, and resultant deficiencies in micronutrients important for muscle health.40
Healthcare Utilisation
Differences in utilisation of healthcare and its relationship with anorexia in hospital is very minimally studied, despite potentially important implications for service management strategies and delivery. A greater length of hospital stay (median 6.6 vs 5.2 days) was observed for the older inpatients with anorexia studied in the Netherlands.20 Conversely, in the UK study on female older inpatients, presence of anorexia was not associated with increased length of hospital stay or readmission to hospital.10 However, in this group appetite was a predictor of hospital-acquired infection, independent of the effects of length of stay and number of comorbidities. There are several factors which impact on length of stay for older adults, for example illness severity, functional ability before admission and trajectory of recovery, as well as care requirements for discharge. Therefore, measurement of all these variables concurrently is needed to understand any true impact of anorexia.
Functional Status
Changes in level of functional ability have been covered by many of the studies on anorexia in the older hospital population. Different measures have been identified as correlates in the cross-sectional studies, including a lower Functional Independence Measure (FIM)42 score in older Japanese inpatients with anorexia16 and lower Modified Barthel Index score43 in UK female inpatients with anorexia.10 This suggests that the presence of anorexia is associated with a higher degree of functional dependence. In a study on Italian inpatients, a lower Instrumental Activities of Daily Living (IADL) score was seen in anorexic participants, while their activity of daily living score measured by Modified Katz Index Scale-6 (ADL-KATZ6)44 was not significantly different.17 However, findings from the Dutch study by van Dronkelaar et al, are counter to this, with inpatients with anorexia having a higher level of independence when measured by the ADL-KATZ6,20 which makes findings difficult to interpret. Interestingly, the authors did observe poorer mobility (measured by the de Morton Mobility Index45) associated with anorexia during admission, and on follow up anorexia was a strong predictor of physical performance (measured by the Short Physical Performance Battery (SPPB)46) one month after hospital discharge, even after accounting for the effects of age, gender, cognitive impairment, fatigue, depression, comorbidity, and fear of falling.20
The differences observed may then be in part due to the different tools used to assess aspects of functional ability, which make them less comparable. The FIM42 and Modified Barthel43 have elements that assess higher levels of mobility and hence perhaps a degree of physical performance, which the ADL-KATZ644 does not, and the IADLs are skills more complex than the basic activities of daily living that the other measures address. It may therefore be that anorexia has a relationship with mobility and physical performance of individuals, rather than ability to undertake basic activities of daily living.
Mortality
The relationship between mortality following hospital discharge has been explored in only two studies, both in UK populations. Pilgrim et al, identified anorexia (defined by SNAQ score <14) during hospital admission was associated with increased risk of death by 6 months post discharge for older females.10 This association identified individuals with anorexia had twice the risk of dying by 6 months and was robust to the effects of length of hospital stay and number of comorbidities. This finding was confirmed in a later study which included males, showing odds of death at 6 months post discharge from hospital were over 2 times greater for individuals with in-hospital anorexia (defined by the SNAQ score <14), when adjusting for the effects of comorbidities, length of hospital stay, and gender.47 The association between anorexia and mortality requires further assessment in other hospitalized populations as the findings are limited by assessment for other confounders of relevance, particularly presence of frailty and diagnosis of malnutrition. The importance of these confounders is indicated by a study in community dwelling older adults, where presence of weight loss combined with anorexia held a higher risk of mortality compared with anorexia alone.28
Conclusion
The anorexia of aging1 is a common problem in older populations, particularly in the hospital setting where it has up to 60% prevalence. Physical factors such as poor dental health and presence of dysphagia, inflammation, low mood and perhaps physical activity may all have a role in anorexia in hospitalized older people. Potential implications of anorexia of aging in the hospital setting include malnutrition (or risk of), reduced muscle strength, poorer physical performance, and mortality following hospital discharge but a less clear relationship with healthcare utilization (Figure 1).
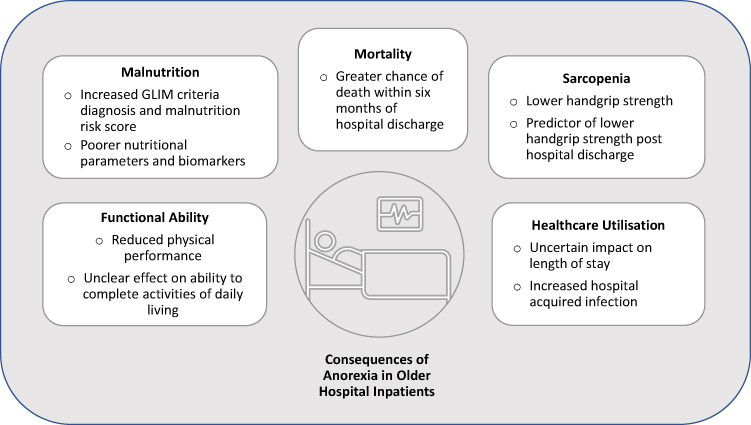 |
Figure 1 Consequences of Anorexia in Older Hospital Inpatients. |
The findings come from a small number of predominantly cross-sectional studies, making any assessment of causative nature undeterminable, alongside this there is more than likely interplay and reciprocal effects of a poor appetite on many of the factors and potential consequences themselves. It is also important to note the lack of research around frailty and anorexia of aging in hospital. This makes it challenging to draw meaningful conclusions and highlights the need for robust longitudinal studies in this cohort of older adults, to determine pathways of causality for anorexia and aid in development of effective interventions.
Abbreviations
ADL-KTAZ6, Modified Katz Index Scale-6; BMI, Body Mass Index; CNAQ, Council on Nutrition Appetite Questionnaire; ESAS, Edmonton Symptom Assessment System; FIM, Functional Independence Measure; GLIM, Global Leadership Initiative on Malnutrition; IDDSI, International Dysphagia Diet Standardization Initiative; MUST, Malnutrition Universal Screening Tool; OHAT, Oral Health Assessment Tool; PASE, Physical Activity Scale for the Elderly; SNAQ, Simplified Nutritional Appetite Questionnaire; SNAQ(M), Short Nutritional Assessment Questionnaire; SPPB, Short Physical Performance Battery.
Acknowledgments
N.J.C. receives support from the National Institute for Health Research (NIHR) Applied Research Collaborative (ARC) Wessex and the NIHR Clinical Academic Training Scheme. The views expressed are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Disclosure
The author reports no conflicts of interest in this work.
References
1. de Souto Barreto P, Cesari M, Morley J, et al. Assessment and management of appetite loss in older adults: an ICFSR task force report. J Fra Aging. 2023;12(1):1–6.
2. Cox NJ, Morrison L, Ibrahim K, Robinson SM, Sayer AA, Roberts HC. New horizons in appetite and the anorexia of ageing. Age Ageing. 2020;49(4):526–534. doi:10.1093/ageing/afaa014
3. Johnson KO, Shannon OM, Matu J, Holliday A, Ispoglou T, Deighton K. Differences in circulating appetite-related hormone concentrations between younger and older adults: a systematic review and meta-analysis. Aging Clin Experim Res. 2020;32:1233–1244. doi:10.1007/s40520-019-01292-6
4. Picca A, Calvani R, Coelho-Júnior HJ, Landi F, Marzetti E. Anorexia of aging: metabolic changes and biomarker discovery. Clin Interv Aging. 2022;17:1761–1767. doi:10.2147/cia.S325008
5. Chia CW, Yeager SM, Egan JM. Endocrinology of Taste with Aging. Endocrinol Metab Clin. 2023;52(2):295–315. doi:10.1016/j.ecl.2022.10.002
6. Walker-Clarke A, Walasek L, Meyer C. Psychosocial factors influencing the eating behaviours of older adults: a systematic review. Ageing Res Rev. 2022;77:101597. doi:10.1016/j.arr.2022.101597
7. Okamoto K, Harasawa Y, Shiraishi T, Sakuma K, Momose Y. Much communication with family and appetite among elderly persons in Japan. Arch Gerontol Geriatr. 2007;45(3):319–326. doi:10.1016/j.archger.2007.01.062
8. Landi F, Lattanzio F, Dell’Aquila G, et al. Prevalence and potentially reversible factors associated with anorexia among older nursing home residents: results from the ULISSE project. J Am Med Directors Assoc. 2013;14(2):119–124. doi:10.1016/j.jamda.2012.10.022
9. Donini LM, Dominguez LJ, Barbagallo M, et al. Senile anorexia in different geriatric settings in Italy. J Nutr Health Aging. 2011;15(9):775–781. doi:10.1007/s12603-011-0048-y
10. Pilgrim AL, Baylis D, Jameson KA, et al. Measuring appetite with the simplified nutritional appetite questionnaire identifies hospitalised older people at risk of worse health outcomes. J Nut Health Aging. 2016;20(1):3–7. doi:10.1007/s12603-016-0668-3
11. Dent E, Chapman I, Piantadosi C, Visvanathan R. Nutritional screening tools and anthropometric measures associate with hospital discharge outcomes in older people. Australas J Ageing. 2015;34(1):E1–E6. doi:10.1111/ajag.12130
12. Cox NJ, Ibrahim K, Sayer AA, Robinson SM, Roberts HC. Assessment and treatment of the anorexia of aging: a systematic review. Nutrients. 2019;11(1):144. doi:10.3390/nu11010144
13. Wilson MM, Thomas DR, Rubenstein LZ, et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am J Clin Nutr. 2005;82(5):1074–1081. doi:10.1093/ajcn/82.5.1074
14. Aprahamian I, Coats AJ, Morley JE, et al. Anorexia of aging: an international assessment of healthcare providers’ knowledge and practice gaps. J Cach Sarcop Musc. 2023;14(6):2779–2792. doi:10.1002/jcsm.13355
15. de Souto Barreto P, Cesari M, Morley J, et al. Appetite loss and anorexia of aging in clinical care: an ICFSR task force report. J Fra Aging. 2022;11(2):129–134.
16. Nomoto A, Shimizu A, Ohno T, et al. Poor oral health and anorexia in older rehabilitation patients. Gerodontology. 2022;39(1):59–66. doi:10.1111/ger.12600
17. Donini LM, Savina C, Piredda M, et al. Senile anorexia in acute-ward and rehabilitations settings. J Nutr Health Aging. 2008;12(8):511–517. doi:10.1007/BF02983203
18. Hansen T, Nielsen RL, Houlind MB, et al. Dysphagia prevalence, time course, and association with probable sarcopenia, inactivity, malnutrition, and disease status in older patients admitted to an emergency department: a secondary analysis of cohort study data. Geriatrics. 2021;6(2):46. doi:10.3390/geriatrics6020046
19. Shimizu A, Fujishima I, Maeda K, et al. Texture-modified diets are associated with poor appetite in older adults who are admitted to a post-acute rehabilitation hospital. J Am Med Dir Assoc. 2021;22(9):1960–1965. doi:10.1016/j.jamda.2021.05.018
20. van Dronkelaar C, Tieland M, Aarden JJ, et al. Decreased appetite is associated with sarcopenia-related outcomes in acute hospitalized older adults. Nutrients. 2019;11(4):932. doi:10.3390/nu11040932
21. Pourhassan M, Böttger S, Janssen G, Sieske L, Wirth R. The association of inflammation with food intake in older hospitalized patients. J Nutr Health Aging. 2018;22(5):589–593. doi:10.1007/s12603-017-0976-2
22. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Pall Care. 1991;7(2):6–9. doi:10.1177/082585979100700202
23. Pourhassan M, Sieske L, Janssen G, Babel N, Westhoff TH, Wirth R. The impact of acute changes of inflammation on appetite and food intake among older hospitalised patients. Br J Nutr. 2020;124(10):1069–1075. doi:10.1017/S0007114520002160
24. Pourhassan M, Babel N, Sieske L, Westhoff TH, Wirth R. Longitudinal changes of cytokines and appetite in older hospitalized patients. Nutrients. 2021;13(8):2508. doi:10.3390/nu13082508
25. Sánchez-Sánchez JL, Guyonnet S, Lucas A, Parini A, Rolland Y, de Souto Barreto P. Plasma inflammatory biomarkers and anorexia of ageing among community-dwelling older adults: an exploratory analysis of the MAPT study. J Nutr Health Aging. 2023;27(11):1127–1131. doi:10.1007/s12603-023-2024-8
26. Yesavage JA, Sheikh JI. 9/Geriatric depression scale (GDS) recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1–2):165–173. doi:10.1300/J018v05n01_09
27. Cox NJ, Howson F, Ibrahim K, et al. Mood and physical activity are associated with appetite in hospitalised older men and women. Age Ageing. 2022;51(12):afac297. doi:10.1093/ageing/afac297
28. Landi F, Liperoti R, Lattanzio F, et al. Effects of anorexia on mortality among older adults receiving home care: an observational study. J Nut Health Aging. 2012;16(1):79–83. doi:10.1007/s12603-011-0064-y
29. Washburn RA, Smith KW, Jette AM, Janney CA. The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153–162. doi:10.1016/0895-4356(93)90053-4
30. Beaulieu K, Hopkins M, Blundell J, Finlayson G. Homeostatic and non-homeostatic appetite control along the spectrum of physical activity levels: an updated perspective. Physiol Behav. 2018;192:23–29. doi:10.1016/j.physbeh.2017.12.032
31. Crabtree DR, Cox NJ, Lim SE, Holliday A. Enhancing the management of anorexia of ageing to counteract malnutrition: are physical activity guidelines optimal? Aging Clin Experim Res. 2023;35:1–5. doi:10.1007/s40520-022-02282-x
32. Lim SER, Dodds R, Bacon D, Sayer AA, Roberts HC. Physical activity among hospitalised older people: insights from upper and lower limb accelerometry. Aging Clin Experim Res. 2018;30(11):1363–1369. doi:10.1007/s40520-018-0930-0
33. Cass AR, Charlton KE. Prevalence of hospital-acquired malnutrition and modifiable determinants of nutritional deterioration during inpatient admissions: a systematic review of the evidence. J Hum Nutr Diet. 2022;35(6):1043–1058. doi:10.1111/jhn.13009
34. Cederholm T, Jensen GL, Correia MITD, et al. GLIM criteria for the diagnosis of malnutrition – a consensus report from the global clinical nutrition community. J Cach Sarcop Musc. 2019;10(1):207–217. doi:10.1002/jcsm.12383
35. Kruizenga HM, Seidell JC, de Vet HCW, Wierdsma NJ, van Bokhorst–de van der Schueren MAE. Development and validation of a hospital screening tool for malnutrition: the short nutritional assessment questionnaire (SNAQ©). Clin Nutr. 2005;24(1):75–82. doi:10.1016/j.clnu.2004.07.015
36. Stratton RJ, Hackston A, Longmore D, et al. Malnutrition in hospital outpatients and inpatients: prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br J Nutr. 2004;92(5):799–808. doi:10.1079/BJN20041258
37. Vellas B, Villars H, Abellan G, et al. Overview of the MNA--Its history and challenges. J Nut Health Aging. 2006;10(6):456–463.
38. Ohta R, Ryu Y, Hattori S. Association between transient appetite loss and vitamin B1 deficiency in elderly patients with suspected deficiency. J Gen Fam Med. 2021;22(3):128–133. doi:10.1002/jgf2.404
39. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601. doi:10.1093/ageing/afz046
40. Landi F, Liperoti R, Russo A, et al. Association of anorexia with sarcopenia in a community-dwelling elderly population: results from the ilSIRENTE study. Eur J Nutr Apr. 2013;52(3):1261–1268. doi:10.1007/s00394-012-0437-y
41. Cox NJ, Bowyer RC, Ni Lochlainn M, Wells PM, Roberts HC, Steves CJ. The composition of the gut microbiome differs among community dwelling older people with good and poor appetite. J Cach Sarcop Mus. 2021;12(2):368–377. doi:10.1002/jcsm.12683
42. Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC. The reliability of the functional Independence measure: a quantitative review. Arch Phys Med Rehabil. 1996;77(12):1226–1232. doi:10.1016/S0003-9993(96)90184-7
43. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. doi:10.1016/0895-4356(89)90065-6
44. Katz S, Downs TD, Cash HR, Grotz RC. Progress in development of the index of ADL. Gerontologist. 1970;10(1):20–30. doi:10.1093/geront/10.1_part_1.20
45. de Morton NA, Davidson M, Keating JL, de Morton NA. The de Morton Mobility Index (DEMMI): an essential health index for an ageing world. Health Qual Life Outcomes. 2008;6:1–15. doi:10.1186/1477-7525-6-63
46. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:2.
47. Cox NJ, Lim SE, Howson F, et al. Poor appetite is associated with six month mortality in hospitalised older men and women. J Nut Health Aging. 2020;24:1107–1110. doi:10.1007/s12603-020-1442-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.