")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Authors Altalhab S
Received 24 December 2023
Accepted for publication 29 February 2024
Published 15 March 2024 Volume 2024:17 Pages 653—662
DOI https://doi.org/10.2147/CCID.S456470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Saad Altalhab
Department of Dermatology, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia
Correspondence: Saad Altalhab, Department of Dermatology, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), P.O. Box 7544, Riyadh, 13317, Saudi Arabia, Email [email protected]; [email protected]
Background: The utilization of low-dose oral minoxidil (LDOM) has emerged as a relatively new treatment option for hair loss, gaining recognition among dermatologists worldwide.
Objective: To assess the knowledge, attitude, and practice patterns among dermatologists in Saudi Arabia regarding the use of LDOM in the management of hair loss.
Methods: An online survey, which was distributed to dermatologists practicing in Saudi Arabia through email and mobile messages. Both univariate and bivariate analyses were performed to investigate the factors that may be associated with enhanced knowledge and practice patterns concerning the utilization of LDOM for the management of hair loss.
Results: A total of 84 dermatologists was included in this study, with 50 (60%) being male. It was found that 83 (99%) of the participants identified patterned hair loss as the most common indication for LDOM usage. Additionally, 77 (92%) recognized hypertrichosis as a well-known side effect. 48 (82%) of the dermatologists had never prescribed LDOM due to its unavailability in local pharmacies.
Conclusion: The usage of LDOM for hair disorders is increasing. Nonetheless, many dermatologists abstain from prescribing this medication due to its limited availability in local pharmacies.
Keywords: low-dose oral minoxidil, knowledge, attitude, practice, Saudi Arabia
A Letter to the Editor has been published for this article.
Introduction
Initially introduced in the 1970s, minoxidil gained recognition as a therapeutic intervention for severe refractory hypertension owing to its notable vasodilatory properties.1 It exerts a relaxant impact on vascular smooth muscle by facilitating the opening of ATP-sensitive potassium channels.2 The administration of oral minoxidil has led to the unexpected occurrence of hypertrichosis in a considerable proportion of patients.3 Following the evaluation of topical formulations for the treatment of hair loss, minoxidil obtained regulatory approval in 1988.4 Despite the effectiveness of topical minoxidil as a viable treatment choice for hair loss, a significant number of patients exhibit poor compliance. This can be attributed to various factors including undesired changes in hair texture, scalp irritation, unpleasant odor of the formulation, the development of allergies to minoxidil or its excipients, and the requirement to apply the medication twice daily.5
Recently, there has been a notable increase in the use of LDOM as a treatment choice for a diverse range of hair disorders, specifically targeting patterned hair loss (PHL).5 This approach is gaining popularity due to its proven safety, efficacy, and favorable tolerability, making it a reliable therapeutic option.1,6 This study aimed to evaluate the knowledge, attitudes, and practice patterns of dermatologists in Saudi Arabia regarding the utilization of LDOM for hair loss management.
Methods
This was a cross-sectional study that was approved by Imam Mohammad Ibn Saud Islamic University (HAPO-01-R-011, project number 256\2023. After creating and validating the questionnaire, it was then distributed to a database consisting of board-certified dermatologists in Saudi Arabia. To gather data, an anonymous survey in English was conducted using Google Forms® as the survey tool. The survey was distributed to participants via email and SMS messages. The inclusion criteria for this study included any board-certified Saudi dermatologists who were practicing in Saudi Arabia. Participation in the study was voluntary, and participants did not receive any financial incentives for their involvement. Prior to commencing the questionnaire, each participant electronically signed an informed consent form.
The survey consisted of 6 sections and had an estimated completion time of around 3 minutes. The survey gathered information regarding the participants’ demographics, their knowledge about the medication, their knowledge about the side effects, their knowledge about the combination of medications, their practice toward LDOM, and the reasons behind not prescribing the medication. In the questionnaire, participants were given the option to select more than one answer for certain questions.
Data analysis for the survey was conducted using IBM SPSS Statistics 25.0. The first stage involved performing a descriptive analysis, where categorical variables were described using frequencies and percentages. In the second stage, a Chi-squared test was employed to examine the relationships between variables. A P value of ≤ 0.05 was used as an indicator of statistical significance.
Results
The study sample included a total of 84 participants (Table 1). Among them, 50 participants (60%) were male, while 66 participants (79%) fell within the age range of 30 to 50 years. Most of the participants, representing 75 individuals (89%), had been actively practicing dermatology for a range of 5 to 20 years.
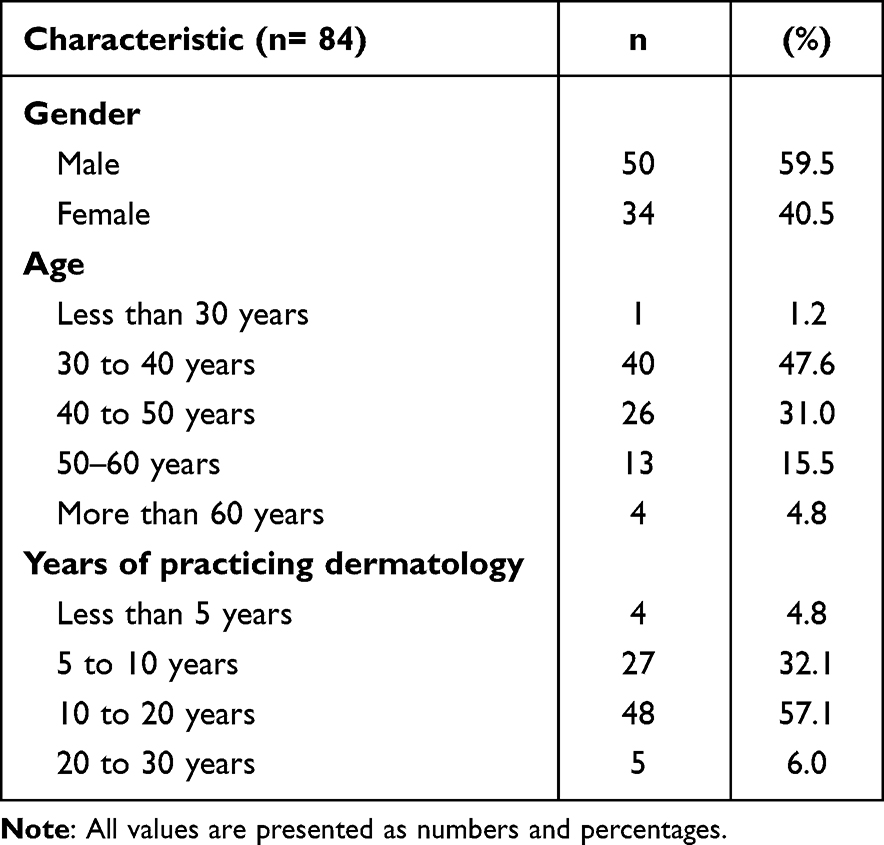 |
Table 1 Demographics |
In the first section, which focused on participants’ knowledge about the medication based on the available literature, the majority of participants (99%) identified PHL as an indication for LDOM (Table 2). Additionally, (44%) of participants recognized telogen effluvium (TE) as another indication for LDOM. Regarding the dosing of LDOM, the survey revealed that (67%) of the participants selected 2.5 mg as the most commonly used dose according to the literature. In addition, it is noteworthy that (60%) of the participants reported 1.25 mg as a commonly used dose for LDOM, while none of the participants selected 10 or 15 mg as indicated doses for hair treatment. (57%) of the participants believed that the typical response time to LDOM is within the range of 3 to 6 months.
 |
Table 2 Knowledge About Medication |
In the second section, which was about the knowledge about side effects, (92%) consider hypertrichosis as a well-known side effect of the LDOM (Table 3). Furthermore, it was interesting to note that (82%) of the participants believed that hypotension is a well-known side effect of this medication. When asked about the common side effects of LDOM, the survey revealed that (61%) of the participants identified hypertrichosis as the most frequently reported side effect. Additionally, (23%) of the participants indicated that headache as the most commonly experienced side effect.
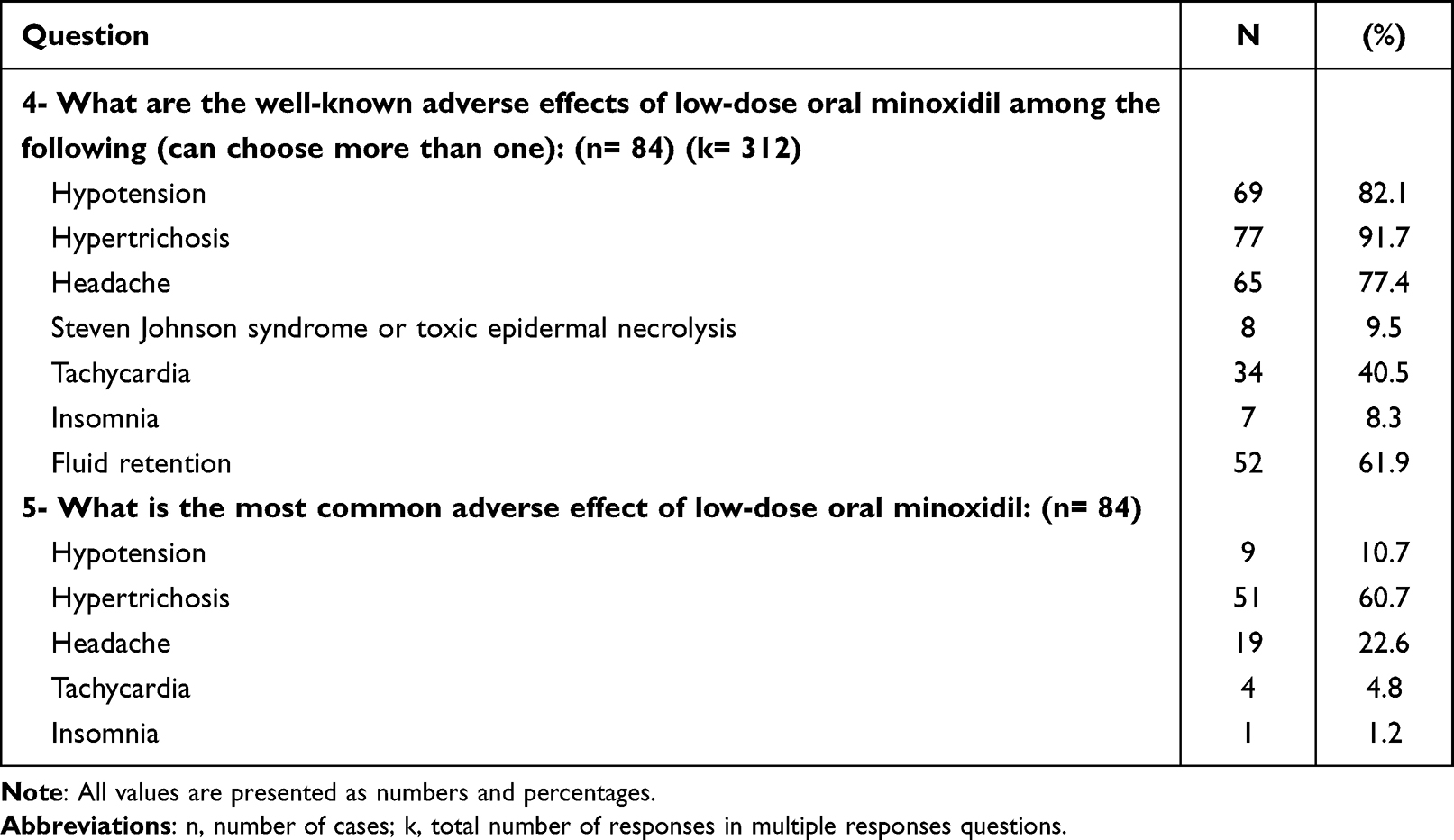 |
Table 3 Knowledge About Side Effects |
According to the survey results, nearly (98%) of the participants were aware that LDOM could be combined with other treatment modalities to address hair disorders (Table 4). Among the participants, the highest chosen modality was hair injectables, with (82%) indicating its use in combination with LDOM. This was followed by oral finasteride, selected by (74%) of the participants, and spironolactone, chosen by (49%). Additionally, (43%) of the participants mentioned topical minoxidil as another modality that can be combined with LDOM.
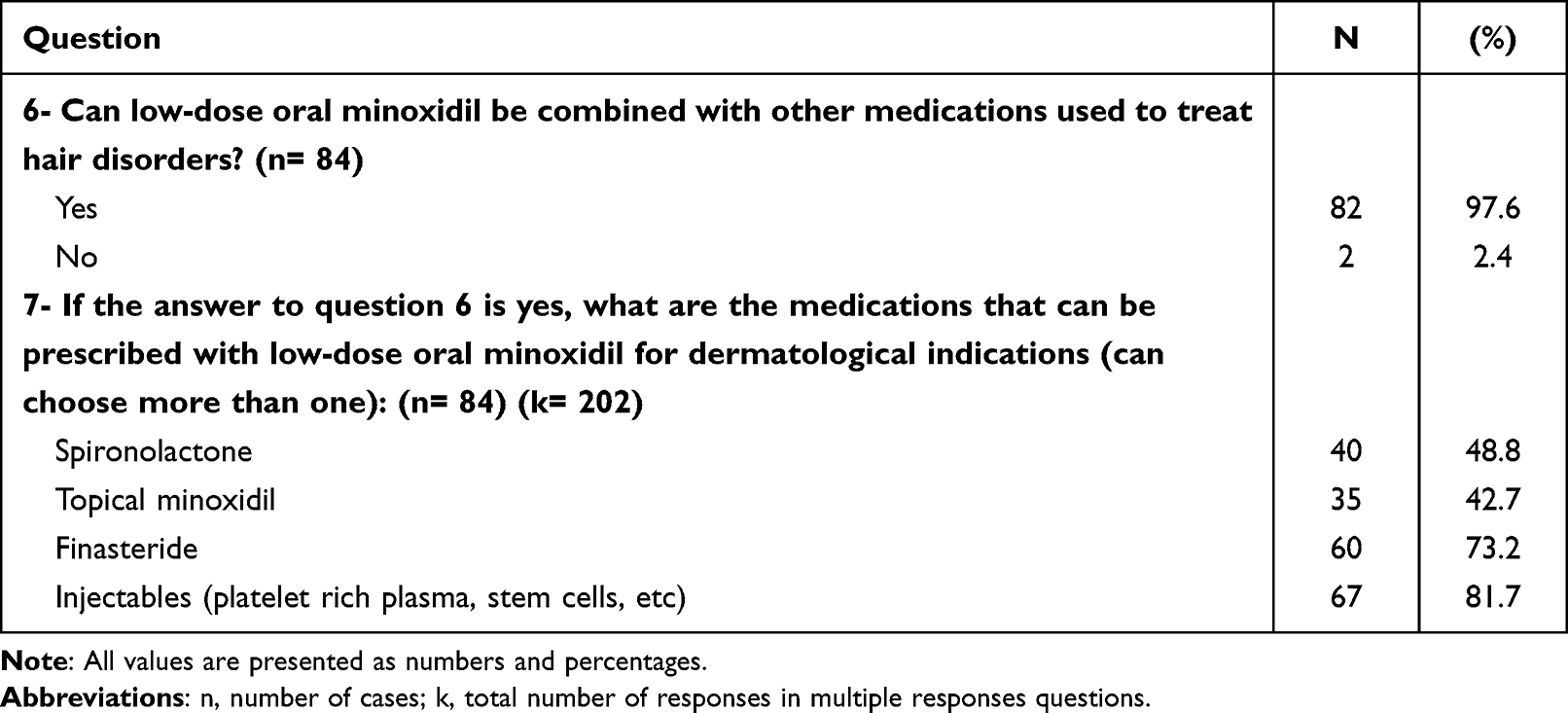 |
Table 4 Knowledge About Combination |
According to the survey results, approximately (48%) of the participants reported prescribing LDOM for their patients (Table 5). However, the majority of them prescribed LDOM to less than five patients per month. When it comes to the starting dose of LDOM, a significant portion of the participants (83%) prescribed a dose range of 1.25–2.5 mg. This dose range was commonly recommended regardless of gender. Specifically, for male patients, (77%) of the participants prescribed a starting dose of 1.25–2.5 mg of LDOM. On the other hand, for female patients, (62%) of the participants prescribed a lower starting dose of 0.75–1.25 mg of LDOM. Based on the survey findings, the primary reason cited by participants (82%) for not prescribing LDOM was the unavailability of the drug in local pharmacies (Table 6).
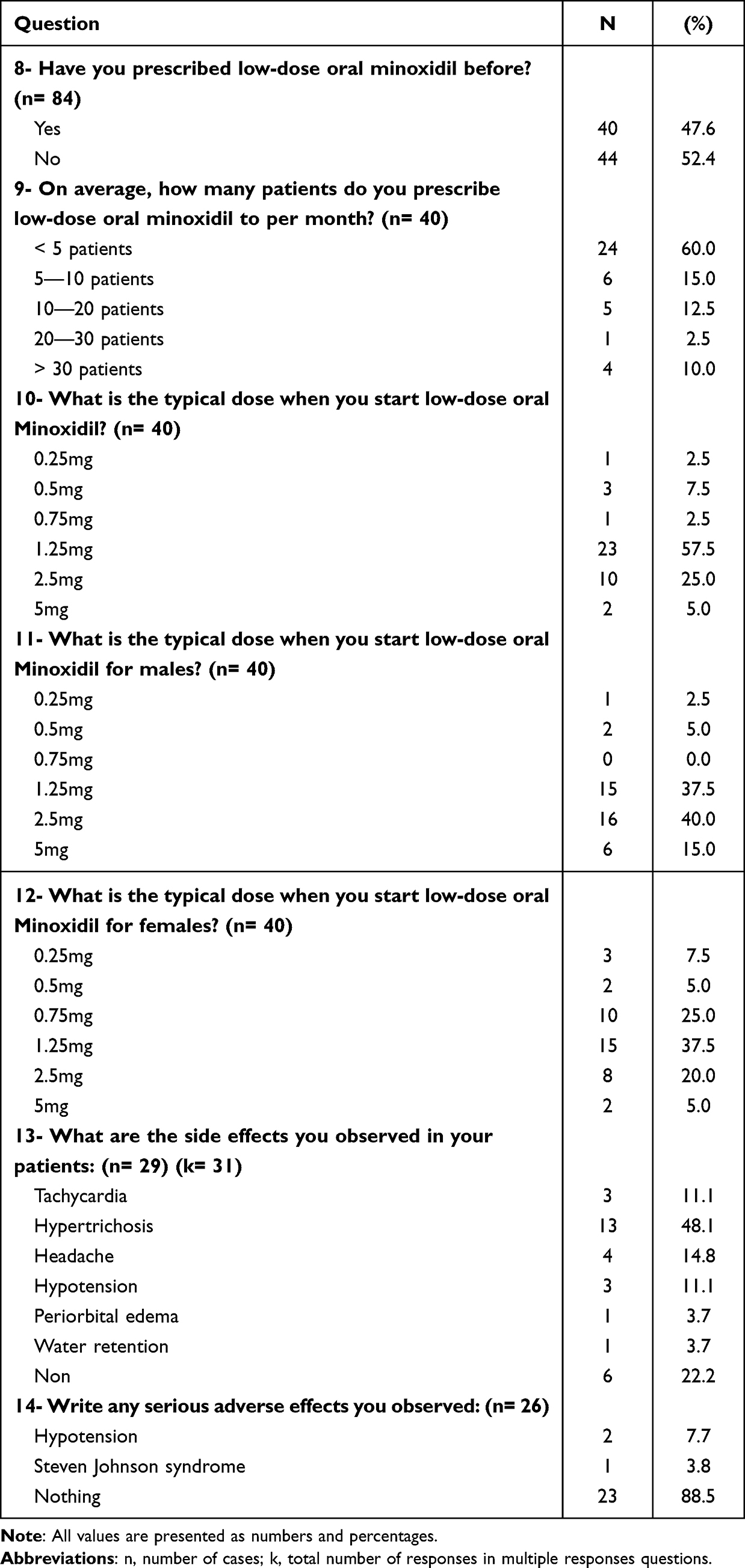 |
Table 5 Practice |
 |
Table 6 Cause of Not Prescribed Medication |
Significant associations were observed between the use of LDOM in treating TE and dermatologists’ age (p-value=0.038) (Figure 1), as well as between LDOM use in TE, alopecia areata, and tractional alopecia, and their years of experience (p-value<0.05) (Table 7) (Figures 2–4). The analysis also revealed significant associations between combining LDOM with spironolactone and dermatologists’ age and years of experience (p-value=0.010, p-value=0.033) (Figures 5 and 6).
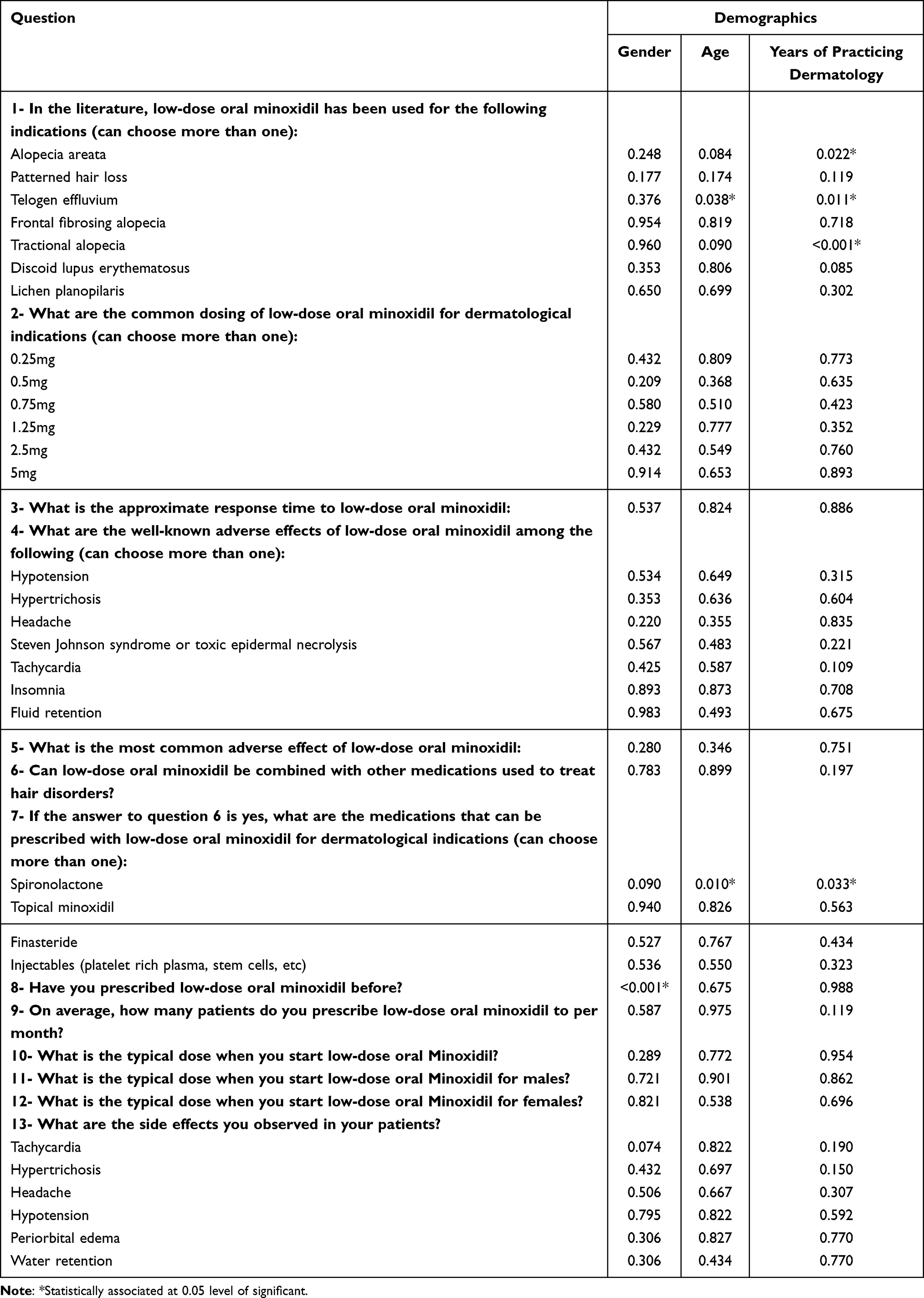 |
Table 7 Association in Dermatologists’ Knowledge and Practice According to Gender, Age, and Years of Practicing Dermatology |
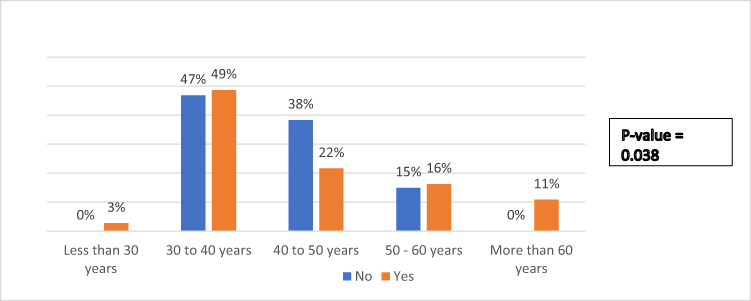 |
Figure 1 Relation between the usage of low-dose oral minoxidil in telogen effluvium with dermatologists’ age. |
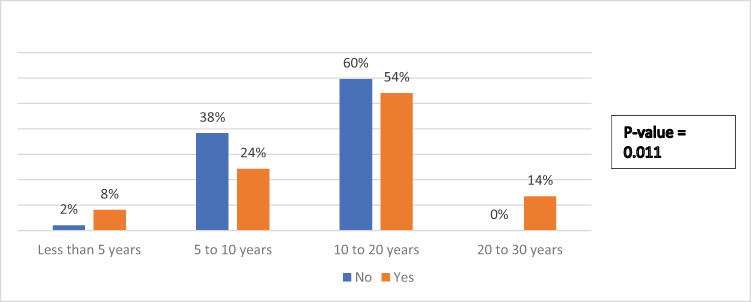 |
Figure 2 Relation between the usage of low-dose oral minoxidil in telogen effluvium with years of practicing dermatology. |
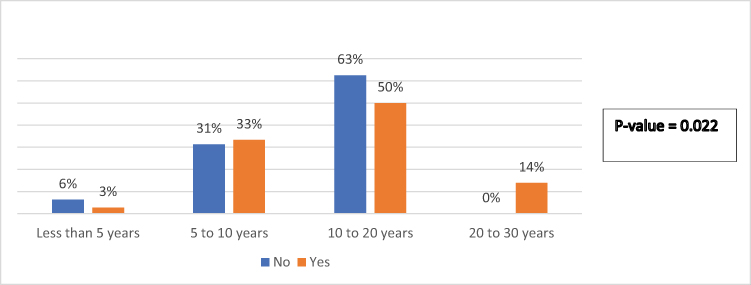 |
Figure 3 Relation between the usage of low-dose oral minoxidil in alopecia areata with years of practicing dermatology. |
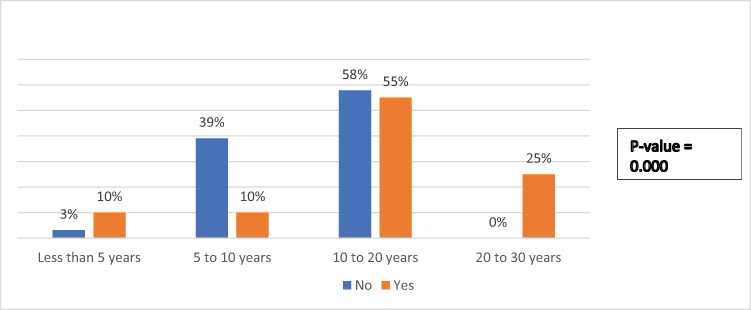 |
Figure 4 Relation between the usage of low-dose oral minoxidil in tractional alopecia with years of practicing dermatology. |
 |
Figure 5 Relation between combining LDOM with spironolactone and dermatologists’ age. |
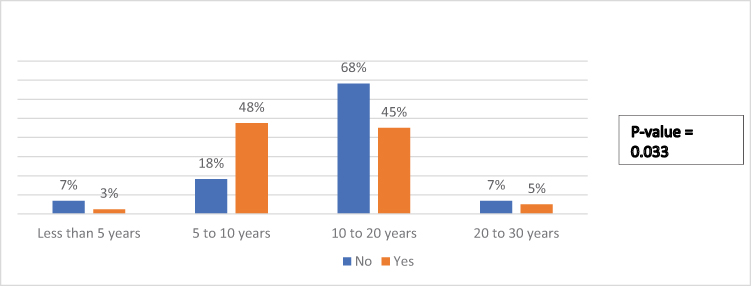 |
Figure 6 Relation between combining LDOM with spironolactone and years of practicing dermatology. |
Discussion
LDOM is a safe and effective treatment for various hair disorders.3 The most common indications supported by literature are PHL and TE.6 LDOM has also shown potential in treating traction alopecia, monilethrix, frontal fibrosing alopecia, and chemotherapy-induced hair loss, although more research is needed in these areas.6 In the current survey, the most common indication for LDOM use was PHL followed by TE, which is consistent with the evidence available in the literature. A systematic review supports these findings, indicating that LDOM was predominantly used for female PHL (4 studies; 286 patients), followed by male PHL (4 studies; 98 patients), and chronic TE (2 studies; 37 patients).6 The study participants in this survey has selected the doses of 1.25 mg and 2.5 mg as the most frequently used doses for treating hair disorders. This aligns with a review that indicates lower doses of oral minoxidil (< 5 mg) are generally well-tolerated and associated with few and mild side effects.1 According to the survey participants, the expected response time for LDOM in hair disorders is typically three to six months. While this timeframe may not be extensively documented in the literature, it has been observed that the initial hair growth-promoting effects of minoxidil can occur after approximately two months, with maximum effects observed at around four months.7 The majority of participants agreed with the literature, recognizing hypertrichosis as a widely acknowledged (92%) and frequently encountered (61%) side effect of LDOM.1 Interestingly, 10% of the participants selected hypotension as the most common side effect, despite the fact that it is rarely reported in the literature with LDOM.7 The participants likely chose hypotension due to the fact that oral minoxidil is traditionally known as an antihypertensive medication. The majority of participants (98%) believed that LDOM can be combined with other treatment modalities, which is consistent with the literature and clinical practice. Combination therapy is commonly used in the treatment of hair disorders to achieve better results, as supported by both literature and clinical practice.8,9 The participants specifically selected hair injectables (82%) as the most commonly combined therapy with LDOM, followed by finasteride (74%). These findings are expected, as hair disorders in Saudi Arabia are frequently treated in private sectors where injectables are commonly used. Finastride, a well-established oral treatment for PHL, is also commonly combined with other treatments in clinical practice. Only (48%) of the dermatologists included in this survey had prescribed LDOM. In Saudi Arabia, many dermatologists have not prescribed LDOM due to various factors. The primary factor, cited by 82% of dermatologists, is the unavailability of the drug in local pharmacies. Other factors include dermatologists’ preference for topical minoxidil, which is perceived to have a safer profile. Additionally, the relative novelty of LDOM as an approach and insufficient knowledge about the drug among dermatologists may contribute to its limited prescription rate. According to the survey results, the typical starting dose of LDOM chosen by (58%) of participants was 1.25 mg. When considering the typical starting dose of LDOM based on gender, (40%) of participants selected (2.5 mg) as the typical starting dose for males, while (38%) chose 1.25 mg as the typical starting dose for females. In the literature, it is commonly reported that the typical doses of LDOM in males range from 2.5 mg to 5 mg.1,10 On the other hand, in females, the typical doses range from 0.25 mg to 1.25 mg.1,11 The reason for this dose difference is to reduce the risk of hypertrichosis in females, as higher doses are more likely to be associated with this side effect.11,12 The most commonly reported side effect of LDOM in the survey was hypertrichosis, and this finding is consistent with what is reported in the literature.7 However, it is important to note that there was one dermatologist reported a case of LDOM associated Steven Johnson Syndrome (SJS). Up to our knowledge, SJS has not been previously associated with LDOM in the literature. Since the current study is based on a survey, the accuracy and reliability of this specific piece of information cannot be confirmed. It would require further investigation and evidence to establish any potential association between LDOM and SJS.
Conclusion
In conclusion, LDOM is recognized as a safe and effective treatment option for hair disorders. However, there is a notable knowledge gap among dermatologists in Saudi Arabia regarding its side effects and safety. This knowledge gap can be attributed to several factors, including limited availability of the drug, its relative novelty in the field, and the existence of perceived safer alternatives such as topical minoxidil.
To address this issue, it is recommended to enhance awareness and understanding of LDOM among dermatologists in Saudi Arabia. This can be achieved through various educational initiatives that specifically focus on the use of LDOM. Moreover, encouraging and conducting further studies in the region would contribute to generating local data on the safety and efficacy of LDOM, thereby increasing awareness and utilization of this effective and safe treatment modality.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board in Imam Mohammad Ibn Saud Islamic University (HAPO-01-R001), project number: 456\2023.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Randolph M, Tosti A. Oral minoxidil treatment for hair loss: a review of efficacy and safety. J Am Acad Dermatol. 2021;84(3):737–746. doi:10.1016/j.jaad.2020.06.1009
2. Meisheri KD, Cipkus LA, Taylor CJ. Mechanism of action of minoxidil sulfate-induced vasodilation: a role for increased K+ permeability. J Pharmacol Exp Ther. 1988;245(3):751–760.
3. Sharma AN, Michelle L, Juhasz M, Muller Ramos P, Atanaskova Mesinkovska N. Low-dose oral minoxidil as treatment for non-scarring alopecia: a systematic review. Int J Dermatol. 2020;59(8):1013–1019. doi:10.1111/ijd.14933
4. Stoehr JR, Choi JN, Colavincenzo M, Vanderweil S. Off-label use of topical minoxidil in alopecia: a review. Am J Clin Dermatol. 2019;20(2):237–250. doi:10.1007/s40257-018-0409-y
5. Ramírez-Marín HA, Tosti A. Role of oral minoxidil in patterned hair loss. Indian Dermatol Online J. 2022;13(6):729–733. doi:10.4103/idoj.idoj_246_22
6. Jimenez-Cauhe J, Saceda-Corralo D, Rodrigues-Barata R, et al. Safety of low-dose oral minoxidil treatment for hair loss. A systematic review and pooled-analysis of individual patient data. Dermatologic Therapy. 2020;33(6):e14106. doi:10.1111/dth.14106
7. Vañó-Galván S, Pirmez R, Hermosa-Gelbard A, et al. Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. J Am Acad Dermatol. 2021;84(6):1644–1651. doi:10.1016/j.jaad.2021.02.054
8. Deoghare S, Sadick NS. Combination therapy in female pattern hair loss. J Cosmet Laser Ther. 2023;25(1–4):1–6. doi:10.1080/14764172.2023.2222942
9. Conic RR, Khetarpal S, Bergfeld W. Treatment of female pattern hair loss with combination therapy. Semin Cutan Med Surg. 2018;37(4):247–253. doi:10.12788/j.sder.2018.043
10. Pirmez R, Salas-Callo CI. Very-low-dose oral minoxidil in male patterned hair loss: a study with quantitative trichoscopic documentation. J Am Acad Dermatol. 2020;82(1):e21–e22. doi:10.1016/j.jaad.2019.08.084
11. Jimenez-Cauhe J, Saceda-Corralo D, Rodrigues-Barata R, et al. Effectiveness and safety of low-dose oral minoxidil in male patterned hair loss. J Am Acad Dermatol. 2019;81(2):648–649. doi:10.1016/j.jaad.2019.04.054
12. Wambier CG, Craiglow BG, King BA. Combination tofacitinib and oral minoxidil treatment for severe alopecia areata. J Am Acad Dermatol. 2021;85(3):743–745. doi:10.1016/j.jaad.2019.08.080
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.