")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Developing a Mobile Health Application to Communicate Adverse Drug Reactions – Preconditions, Assessment of Possible Functionalities and Barriers for Patients and Their General Practitioners
Authors Wakob I, Schmid GL, Nöhring I, Elze R, Sultzer R, Frese T, Schiek S , Bertsche T
Received 6 April 2022
Accepted for publication 17 June 2022
Published 8 July 2022 Volume 2022:15 Pages 1445—1455
DOI https://doi.org/10.2147/JMDH.S369625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ines Wakob,1,2 Gordian Lukas Schmid,3 Ingo Nöhring,3 Romy Elze,4 Ralf Sultzer,5 Thomas Frese,6 Susanne Schiek,1,2,* Thilo Bertsche1,2,*
1Clinical Pharmacy, Institute of Pharmacy, Medical Faculty, Leipzig University, Leipzig, Germany; 2Drug Safety Center, Faculty of Medicine, University Hospital of Leipzig and Leipzig University, Leipzig, Germany; 3Department of General Practice, Medical Faculty of the University of Leipzig, Leipzig, Germany; 4University Computer Center, Department of Research and Development, Leipzig University, Leipzig, Germany; 5Sana Geriatric Centre, Zwenkau, Germany; 6Institute of General Practice and Family Medicine, Martin-Luther-University, Halle (Saale), Germany
*These authors contributed equally to this work
Correspondence: Thilo Bertsche, Clinical Pharmacy, Institute of Pharmacy, Medical Faculty, Leipzig University and Drug Safety Center, University Hospital of Leipzig and Leipzig University, Bruederstr 32, Leipzig, Germany, Tel +49 341 97 11800, Email [email protected]
Purpose: Mobile health (mHealth) applications offer structured and timely communication between patients and general practitioners (GPs) about adverse drug reactions (ADR). Preconditions, functionalities and barriers should be studied to ensure safe implementation.
Methods: We performed a cross-sectional questionnaire survey addressing (i) preconditions, (ii) users’ assessment of functionalities and (iii) barriers to mHealth managing ADR communication.
Results: A total of 480 patients and 31 GPs completed the survey. (i) A total of 269 (56%) patients and 13 (42%) GPs were willing to use mHealth for ADR communication. Willingness was negatively correlated with age for both patients (r = − 0.231; p < 0.001) and GPs (r = − 0.558; p = 0.002). (ii) Most useful functionalities mentioned by patients (> 60%) included “Rapid feedback on urgency of face-to-face consultations.” GPs valued information on “Patient’s difficulties in medication administration.” (iii) In free-text answers, the barrier reported most frequently by patients was “preferred personal GP contact” (6%), whereas GPs claimed, “uncomplicated use with low expenditure of time and personnel” (19%).
Conclusion: Older patients and GPs mainly show reservations about mHealth for ADR communication but recognize possible benefits. mHealth implementation should avoid a negative effect on GPs’ time budgets; the primary goal should not be to reduce the number of GP-patient contacts but to optimize them.
Keywords: mHealth, adverse drug reaction, patient, general practitioner, questionnaire survey
Introduction
Adverse drug reactions (ADR) can endanger patient safety and lead to hospital admission or even death.1–3 Less harmful but disturbing ADRs potentially result in non-adherence: by not taking the drug as prescribed, the patient is potentially harmed due to a lack of effect.4,5 Especially after medication changes, observed ADRs should be reported immediately to the GP, not delayed until the next routine consultation. Mobile health (mHealth) applications offer new opportunities for direct communication from patient to GP and vice versa. They enable structured reports of relevant ADRs to the GPs, who, if necessary, can take measures such as initiating a personal medical consultation. In cases where the observed ADR is not critical, prompt GP feedback could prevent patient anxiety and support adherence. Advantages for the GPs are receiving structured information about the ADR, which can support their clinical risk assessment. In rural areas with limited medical care or when appointments are scarce, mHealth applications could enable a low-threshold exchange with the attending GP. However, many mHealth applications do not yet contain such structured information on individual patients’ ADRs.6 mHealth applications for ADR communication addressing patients have focused mainly on pharmacovigilance by supplementing the ADR reports from medical professions to national medical authorities.7–9 Such solutions are not yet tailored to an individual patient’s case and do not enable the assessment of causality. Despite possible positive effects, mHealth applications can cause harm.10,11 To reduce the risk of harm to the patients, future users, ie, patients and GPs, should be involved early in the conceptual process to provide a solid basis for interdisciplinary discussion.12,13 For this reason, we evaluated preconditions for using those technologies, users’ assessment of possible functionalities, and barriers to implementation.
Materials and Methods
Study Design
We conducted a cross-sectional questionnaire study with patients and their GPs to assess their opinions of preconditions, possible functionalities and barriers concerning an mHealth application to communicate adverse drug reactions.
Development of Questionnaires for Patients and GPs
An expert panel formed of GPs, pharmacists, and IT scientists with the additional involvement of a psychologist and a communication and media scientist developed two questionnaires (one for patients, one for GPs). The questionnaires addressed (i) preconditions, which represent the basic requirements such as usage of mobile electronic devices by patients, general necessity and willingness to use an mHealth application for ADR communication. (ii) The users (patients and GPs) were asked how useful they perceive the possible concrete functionalities to be for the content and procedural implementation of mHealth applications for ADR communication. The expert panel had compiled the functionalities according to the guiding questions, what might be necessary for a reasonable evaluation of an ADR report, should queries about ADR be totally standardized or customizable, how frequently should they take place, and how should feedback be provided. Finally, (iii) users were asked about the barriers they see to a smooth implementation. Answer options (closed questions) were rated on Likert scales or as categorical items for sections i and ii. Free text answers (open questions) addressing barriers (iii) were summarized in superordinate (Appendix 1).
Pretest
The questionnaires were pretested for comprehensibility using test persons independent from the main study. Each pretest step was followed by a revision of the questionnaires. The pretest of the patient’s questionnaire included cognitive pretests with pharmacists (n=2) and medical laypersons (n=4), an item accuracy revision by computer scientists (n=2), standard observation pretests with medical laypersons (n=7) and finally, a pilot in a general practice with medical laypersons (n=8). Pretesting of the GP’s questionnaire included a cognitive pretest with (n=3) pharmacists and standard observation pretesting with (n=2) GPs and (n=1) pharmacist. As a consequence of the pretesting, questionnaires were refined, particularly regarding the wording. Focusing on data analysis, a filter question was introduced into the patient questionnaire prior to part ii because the pretest revealed a lack of understanding of the term “app” (Appendix 1). This understanding was necessary to obtain answers relevant to the evaluation.
Study Sampling
We first chose a random sample of 50 practices from the publicly accessible register of the Association of Statutory Health Insurance Physicians Saxony; these were contacted via telephone by a GP (IN). Due to the low positive response, we extended the recruitment to the 122 teaching general practices of Leipzig University and a local network of GPs and specialists. The general practices were contacted consecutively until the 20 practices were recruited in Leipzig, Germany and surrounding areas. The participating general practices provide ambulatory care for patients across age and gender or specialty boundaries. Some are joint practices that employ more than one GP. We expected about 40 to 50 patients to visit each general practice per study day, generating 800 to 1000 eligible patients. Data collection took place from October 9, 2018 to March 8, 2019. One day of data collection was scheduled per general practice during consultation hours.
Participants
On the study day, all patients who visited the general practice were consecutively invited to participate in the survey. Inclusion criteria were either age over 18 years and fully contractually capable or children and adolescents with written informed consent from their legal guardians. Furthermore, sufficient knowledge of the German language was required to perform the survey. Exclusion criteria were missing written informed consent from the patient or the legal guardian or lack of fulfilment of the other inclusion criteria. In addition, every GP working in the general practice on the study day was also invited to participate. There were no exclusion criteria for GPs.
Data Collection and Analysis
On the study day, two or three study assistants (advanced pharmacy students, 4th year) recruited the patients and GPs in the general practices. Before data collection, the study assistants were instructed about relevant background information, the questionnaire and the organizational procedure. A checklist ensured standardized data collection. To ensure standardization of the study, the study assistants received a list with standardized responses and definitions for anticipated frequent patient questions. Data collection was piloted for 4 hours in a general practice. Pilot data were not included in the main study. The paper-based questionnaires were electronically scanned and converted into the data analysis form using FormPro3 (OCR system, Leipzig, Germany).
A basic understanding was required for the utility assessment of concrete functionalities. We therefore introduced a filter question (“Can you imagine anything under the term ‘app’?”) and included only participants who responded affirmatively in the evaluation of this part (ii).
Statistics
We performed a Spearman correlation to assess associations between the respondents’ age and the use of mobile electronic devices (only patients), and the willingness to use an mHealth technology for ADR communication (patients and GPs). The threshold for statistical significance was set at P < 0.05.
Ethics
The Ethics Committee of the Medical Faculty of Leipzig University and the Saxony Chamber of Physicians (325/18 ek; EK BR 68/18 1/281,062) approved this study. This study conforms to the ethical standards of the Declaration of Helsinki. All patients participated voluntarily, and written informed consent was obtained from all patients prior to inclusion. Patients could withdraw from participation at any time without giving any reason.
Results
Characteristics
Of the 144 contacted general practices, 20 (14%) agreed to participate. A total of 480 of their patients and 31 GPs (1–3 per general practice) were enrolled in the survey (Figure 1, Table 1).
 |
Table 1 Characteristics of Participants; GP: General Practitioner |
 |
Figure 1 Flow chart descriptive of study population at patient level. |
(i) Preconditions
Patients
Of the patients, 375 (78% of 480) stated they owned a mobile electronic device and 340 (71%) carried it with them. Younger patients were more likely to have a mobile electronic device with them (r=−0.430, weak correlation; p<0.001). A total of 269 (56%) of the patients would be willing to use an mHealth application for ADR communication. The willingness to use such an mHealth application was negatively correlated with the patients’ age (r=−0.231, weak correlation; p<0.001).
General Practitioners (GPs)
Of the participating GPs, 13 (42%) expressed their willingness to use such an mHealth technology. The willingness to use such an mHealth application was negatively correlated with the GPs’ age (r=−0.558, moderate correlation; p=0.002, Figure 2A and B).
 |
Figure 2 (A) Patients’ willingness to use an mHealth application for ADR communication, depending on their age. Question to patient: “Would you use an app as described to report ADRs to your GP?” Values refer to the relative number of patients answering yes (dark grey), rather yes (light grey), rather no (light grey-hatched), no (dark grey-hatched); answers not specified or not classifiable (black). n=41 patients did not specify age and, therefore, are not represented in the Figure. (B) GPs’ willingness to use an mHealth application for ADR communication, depending on their age. Question to GP: “Would you use a software as described?” Values refer to the relative number of GPs answering yes (dark grey), rather yes (light grey), rather no (light grey-hatched), no (dark grey-hatched); answers not specified or not classifiable (black). n=1 GP did not specify age and, therefore, is not represented in the Figure. The remaining age groups compared to (A) result with n=0 each. |
(ii) Users’ Assessment of Possible Functionalities
Patients
Out of 480 patients, 378 were familiar with the term “app” and were, therefore, included in the evaluation of part (ii). The three functionalities rated most useful for the realization of an mHealth application for ADR communication were (positive affirmation by more than 60% of the patients, respectively): “Rapid feedback on urgency of face-to-face consultations” “Report of ADR to GP by the patient at any time” and “Parameters measured by the patient” (Figure 3). Eighty-seven of the patients (23%) preferred a standardized ADR communication “selected from a prepared medication specific list” (Table 2). One hundred eighty-one out of 378 (48%) patients rejected a totally automatic “IT-supported query for specific ADRs at a specific time.”
 |
Table 2 Aspects of Patients’ Preconditions and Users’ Assessment of Possible Functionalities for Realization of an mHealth Application for ADR Communication; Closed Questions (Answers Presented as Likert Scales or Categorical Items); Number of Responses in % Based on the Number of Participating Patients (n=480; n=378a) |
 |
Figure 3 Question to GP: “How useful do you rate the support of the mHealth technology in managing ADRs in your patients … [with the following concrete possible functionalities]”. Questions to patient: “In what cases would you rate the app as useful?” Alternative questions, concerning functionalities patients might have trouble with to assess its “usefulness” due to the pretest: “Would you be willing to use the app to … ”. The difficulties to rate “usefulness” are related to the layperson’s limited ability to recognize the relevance of the information in relation to the evaluation of the ADR and its causality. *Patients were asked about their willingness to supply the information. |
General Practitioners (GPs)
The three functionalities rated most useful by the GPs were (positive affirmation by more than 60%, respectively): “Patient’s difficulties in medication administration” “Patient’s deviations from GPs advice” and “Parameters measured by patient.” Of the 31 GPs, 12 (39%) preferred a standardized ADR communication “Selected from a prepared medication specific list” (Table 3). Twenty-one out of 31 (68%) GPs rejected a totally automatic “IT-supported query for specific ADRs at a specific time.” Eighteen (58%) GPs rated “Visualization of urgency (eg, traffic scheme)” to be useful (Figure 3).
 |
Table 3 Aspects of General Practitioners’ (GP) Preconditions and Utility Assessment for Realization of an mHealth Application for ADR Communication. Closed Questions (Answers Rated on Likert Scales or as Categorical Items); Number of Responses in % Based on the Number of Participating GPs (n=31) |
Eighteen GPs (58%) considered it as a limitation if the “Report of ADRs needed to be opened via a link in the email inbox”; 20 GPs (65%), if the “Report of ADRs needed to be opened via an additional password entry.”
(iii) Barriers
Patients
The barrier reported most frequently by 31 out of 480 (6%) patients in free-text answers was “preferred personal GP contact.” Other concerns were related to “data privacy” (12; 3%) and “lack of technical affinity” (11; 2%). The additional requirement reported most frequently by patients was “easy handling” (20; 4%; Table 4).
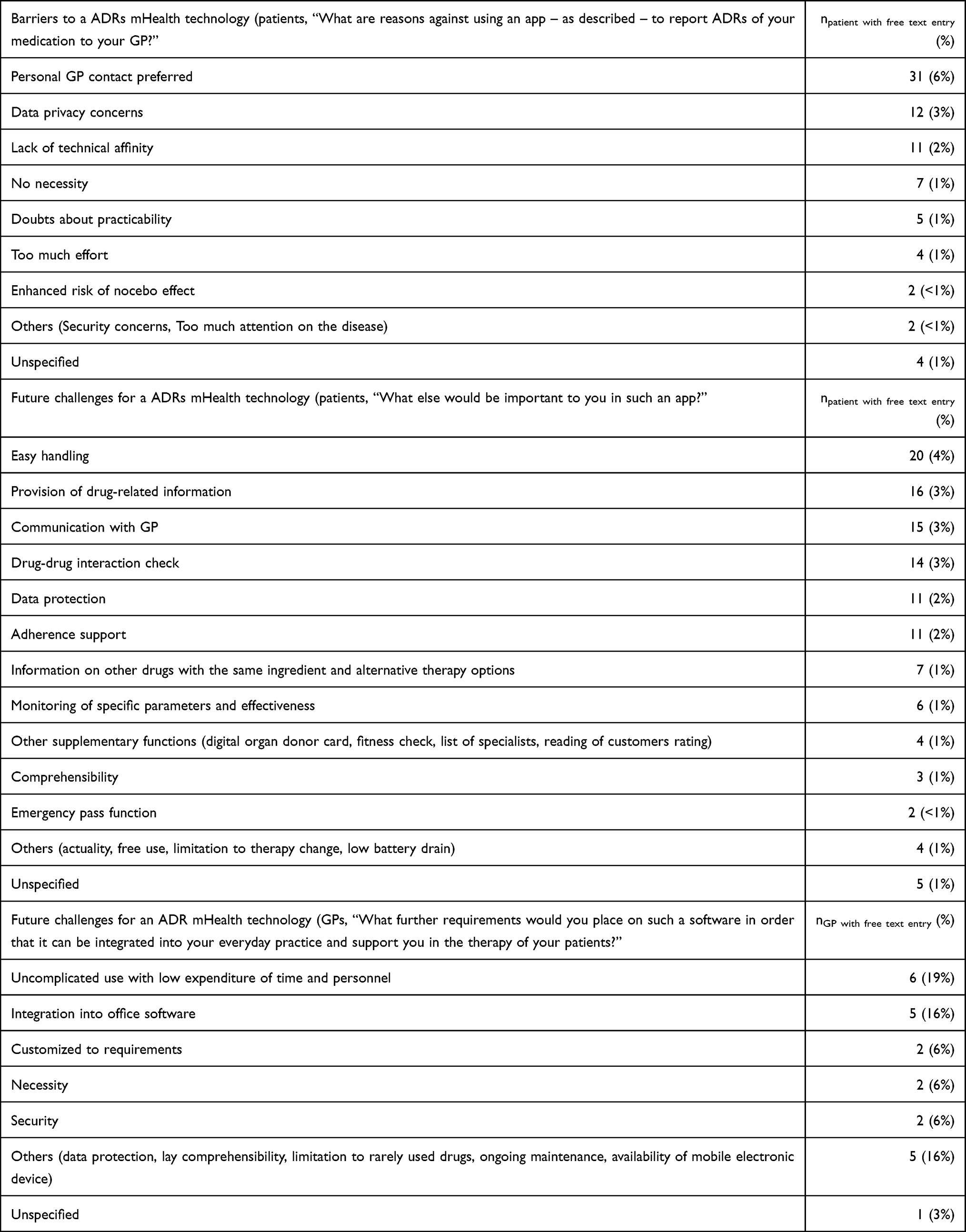 |
Table 4 Barriers to Use mHealth Technology in ADR Communication and Future Challenges. Answers to Open Question Were Categorized; Answers Mentioned Only Once are Subsumed in “Others”; Number of Responses in % Based on the Number of Participating Patients (n=480) and General Practitioners (GPs; n=31) |
General Practitioner (GP)
The additional requirement reported most frequently by GPs was “uncomplicated use with low expenditure of time and personnel” (6; 19%; Table 4).
Discussion
The decision to start therapies or change medication in outpatient care represents a critical time frame due to the challenges of ADR monitoring and communication. mHealth applications offer new options to reduce communication gaps. We therefore queried patients and GPs’ about their willingness to use such applications, how they rate possible functionalities and what barriers to implementation they perceive to facilitate a user-oriented conceptual design. We found in this study of a total of 480 patients and their 31 GPs that 56% of patients and 42% of GPs were willing to use mHealth for ADR communication. Both patients and GPs were more likely to use such technologies at younger ages. Patients saw a particular advantage of mHealth technologies in the rapid feedback on the urgency of face-to-face consultation. GPs especially considered supporting information on the patient’s difficulties with medication administration to be useful in assessing potential ADRs. Patients perceived preventing personal GP contact as a particular barrier to mHealth implementation. GPs especially feared an increase in time and personnel requirements.
ADR Communication via mHealth Between Patient and GP
Our survey confirms the need for more effective ADR communication, with almost one-third of the patients reporting they had previously felt insecure about a newly prescribed medication. However, unsettling the patients due to careless queries about ADRs and over-alerting of the GP by electronic systems should be avoided.14,15 To ask about ADRs – even when they did not actually occur for the individual patient – bears the risk of nocebo effects.16 This concern of “an enhanced risk of nocebo effect” was also mentioned by patients in our survey as a barrier to using mHealth. Therefore, a consideration of risk versus benefit based on the frequency and severity of possible ADRs should be included. In addition, patient-understandable language should be used for queries transmitted via app to the patient.
If the queries are tailored to a superordinate group of medicines having heterogenous properties instead of precisely to the patient’s medication due to a lack of appropriate databases, patients run the risk of being asked about ADRs that do not even apply to them. Individualized adjustments by the GP could address this problem. Standardization should be carefully weighed against individualization options as well as individualization necessities.
Implementation of mHealth applications can be achieved only for patients who carry a mobile electronic device with them. This precondition was given to our participants, but our results support that this is especially the case at younger ages.12,17,18 However, handling errors could impair the safe use of such mHealth applications. “Lack of technical affinity” and “Easy handling” were frequently mentioned by patients as barriers and further requirements, respectively, underlining the need for tailored digital training. The application should enable clear and unambiguous handling procedures and should be supplemented with tutorials.
Patients’ Perspectives
mHealth applications could optimize the communication between patient and GP in two ways: First, as structured information on ADRs, including supplementary aspects for the assessment from the patient to the GP. Second, therapy consequences depending on urgency can be communicated from the GP to the patient, eg, scheduling an appointment. “Personal GP contact” is still preferred by many of the patients. It should, therefore, be clarified that such mHealth applications are not primarily about replacing GP’s consultations but about optimizing their structure for higher efficiency in healthcare in general, and in particular related to the individual patient’s pharmacotherapy, because a structured report on ADRs facilitates their assessment by the GP.19 Our findings also underline the need to prioritize and visualize the most important information for the GP.20 The patients in our survey confirmed the priority request for fast feedback on their ADR reports.7,21 This result emphasizes that such mHealth applications need to guarantee that the patients receive fast feedback to avoid deceptive feelings of security because of an information transfer delay. In this context, it is not surprising that about one-third of the participating patients doubt the benefit of mHealth applications on ADR communications or are unwilling to provide the corresponding information. Implementation should therefore be accompanied by well-founded information and education.
GPs’ Perspective
None of the proposed functionalities seem completely superfluous to the participating GPs, and none absolutely necessary. However, our results indicate that GPs particularly appreciate information on medication administration supplementary to the ADR report, as “Patient’s difficulties in medication administration“ and ”Patient’s deviation from GP’s advice” were judged to be the most useful information supporting causality assessment delivered by the mHealth application. The lack of communication about adherence could explain this.22 In contrast to already implemented mHealth applications that focus mainly on adherence,12,23,24 we considered adherence as one supplementary piece of information allowing the GP to properly assess the occurrence of an ADR due to overdosing or missed doses.
“Uncomplicated use with low expenditure of time and personnel” was the most frequently mentioned further requirement by GPs. GPs are skeptical about the expenses of integrating such applications in their routine, eg, due to additional password entries meant to ensure data protection. On the one hand, this demonstrates the need for simplification by limited process steps and the best possible integration in office software and routine procedures.7 But on the other hand, it must not be at the expense of data protection; this is demonstrated by the concerns regarding data protection raised by both patients and GPs in our study. These findings propose that IT developers focusing on the theoretical aspects of digital feasibility and GPs observing the practical, real-life aspects should intensify their collaboration during the conceptual design process of such digital solutions and integrate the patient perspective.
Limitations
This study has the following limitations: General practices were predominantly located in urban areas. Transferability to rural areas is not guaranteed but should be examined within subsequent studies, as appropriate digitalization measures can be of particular value in structurally backward areas due to limited personnel resources. Because of the small number of GPs interviewed, findings in this user group ought to be interpreted with caution. In addition, we conducted the survey mainly with GPs involved in medical training who had a lower age and an expected higher level of interest concerning such projects. A GP’s support or refusal of technical applications may have been communicated to the patients and influenced them. Patients, however, were surveyed prior to their respective visits to the GPs. We included patients of all ages, although a tendency towards a higher willingness to participate among younger patients cannot be ignored. However, they will be the future target group as well.
Conclusion
About half of patients and GPs showed a moderate acceptance of mHealth applications in ADR communication. Younger patients and GPs are particularly open-minded to such technologies. Our results suggest that the greatest challenge in developing such mHealth applications is finding balanced approaches between standardization and individualization and between simplicity of use and data protection. Time aspects concerning GPs’ time budget and personal contact are essential for the successful implementation of such technologies. To utilize the mHealth applications’ potential contribution to patient safety, user skepticism and barriers should be managed in further developments.
Abbreviations
GP, general practitioner; mHealth, mobile health; ADR, adverse drug reaction.
Acknowledgments
We thank Dr. rer. med. Tobias Deutsch (Independent Department of General Medicine, Faculty of Medicine, Leipzig University) for his helpful support in the development of the questionnaires. We thank VITAL SERVICES, MOGIC GmbH, and HEALTHY SAXONY eV for their cooperation within the EMMA project. We thank the Federal State of Saxony and the European Union for their financial support of the EMMA project. We thank the participating elective students for their active support in carrying out the survey. We thank Jana Schuster for proofreading and Katharine Worthington for the language correction of the manuscript.
Funding
The authors announced that this work was supported by a grant from the European Regional Development Fund (ERDF) [100293110]. We acknowledge support from Leipzig University for Open Access Publishing.
Disclosure
Mr Ingo Nöhring reports being physician in German Armed Forces. The authors report no other conflicts of interest in this work.
References
1. Oscanoa TJ, Lizaraso F, Carvajal A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur J Clin Pharmacol. 2017;73(6):759–770. doi:10.1007/s00228-017-2225-3
2. Meier F, Maas R, Sonst A, et al. Adverse drug events in patients admitted to an emergency department: an analysis of direct costs. Pharmacoepidemiol Drug Saf. 2015;24(2):176–186. doi:10.1002/pds.3663
3. Schneeweiss S, Hasford J, Göttler M, Hoffmann A, Riethling AK, Avorn J. Admissions caused by adverse drug events to internal medicine and emergency departments in hospitals: a longitudinal population-based study. Eur J Clin Pharmacol. 2002;58(4):285–291. doi:10.1007/s00228-002-0467-0
4. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: looking beyond cost and regimen complexity. Am J Geriatr Pharmacother. 2011;9(1):11–23. doi:10.1016/j.amjopharm.2011.02.004
5. Hsu KL, Fink JC, Ginsberg JS, et al. Self-reported medication adherence and adverse patient safety events in CKD. Am J Kidney Dis. 2015;66(4):621–629. doi:10.1053/j.ajkd.2015.03.026
6. Dormann H, Maas R, Eickhoff C, et al. [Standardized national medication plan: The pilot projects MetropolMediplan 2016, model region Erfurt, and PRIMA]. Bundesgesundheitsbl. 2018;61(9):1093–1102. German. doi:10.1007/s00103-018-2789-9
7. De Vries ST, Denig P, Lasheras Ruiz C, et al. IMI Web-RADR Work Package 3b Consortium. Interest in a mobile app for two-way risk communication: a survey study among European healthcare professionals and patients. Drug Saf. 2018;41(7):697–712. doi:10.1007/s40264-018-0648-0
8. Pierce CE, De Vries ST, Bodin-Parssinen S, et al. Recommendations on the use of mobile applications for the collection and communication of pharmaceutical product safety information: lessons from IMI WEB-RADR. Drug Saf. 2019;42(4):477–489. doi:10.1007/s40264-019-00813-6
9. Montastruc F, Bagheri H, Lacroix I, et al. Adverse drug reaction reports received through the mobile app, VigiBIP®. A comparison with classical methods of reporting. Drug Saf. 2018;41(5):511–514. doi:10.1007/s40264-017-0630-2
10. Graber ML, Siegal D, Riah H, Johnston D, Kenyon K. Electronic health record–related events in medical malpractice claims. J Patient Saf. 2019;15(2):77–85. doi:10.1097/PTS.0000000000000240
11. Schneider EC, Ridgely MS, Meeker D, Hunter LE, Khodyakov D, Rudin RS. Promoting patient safety through effective health information technology risk management. Rand Health Q. 2014;4(3):7.
12. Ernsting C, Dombrowski SU, Oedekoven M, et al. Using smartphones and health apps to change and manage health behaviors: a population-based survey. J Med Internet Res. 2017;19(4):e101. doi:10.2196/jmir.6838
13. Demiris G, Krupinksi E, Washington K, et al. The role of human factors in telehealth. Telemed J E Health. 2010;16(4):446–453. doi:10.1089/tmj.2009.0114
14. Judge J, Field TS, DeFlorio M, et al. Prescribers’ responses to alerts during medication ordering in the long term care setting. J Am Med Inform Assoc. 2006;13(4):385–390. doi:10.1197/jamia.M1945
15. Page N, Baysari MT, Westbrook JI. A systematic review of the effectiveness of interruptive medication prescribing alerts in hospital CPOE systems to change prescriber behavior and improve patient safety. Int J Med Inform. 2017;105:22–30. doi:10.1016/j.ijmedinf.2017.05.011
16. Webster RK, Weinman J, Rubin GJ. Medicine-related beliefs predict attribution of symptoms to a sham medicine: a prospective study. Br J Health Psychol. 2018;23(2):436–454. doi:10.1111/bjhp.12298
17. Carroll JK, Moorhead A, Bond R, LeBlanc WG, Petrella RJ, Fiscella K. Who uses mobile phone health apps and does use matter? A secondary data analytics approach. J Med Internet Res. 2017;19(4):e125. doi:10.2196/jmir.5604
18. Levine DM, Lipsitz SR, Linder JA. Trends in seniors’ use of digital health technology in the United States, 2011–2014. JAMA. 2016;316(5):538–540. doi:10.1001/jama.2016.9124
19. Basch E, Deal AM, Dueck AC, et al. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA. 2017;318(2):197–198. doi:10.1001/jama.2017.7156
20. Kane-Gill SL, O’Connor MF, Rothschild JM, et al. Technologic distractions (part 1): summary of approaches to manage alert quantity with intent to reduce alert fatigue and suggestions for alert fatigue metrics. Crit Care Med. 2017;45(9):1481–1488. doi:10.1097/CCM.0000000000002580
21. De Vries ST, Wong L, Sutcliffe A, et al. Factors influencing the use of a mobile app for reporting adverse drug reactions and receiving safety information: a qualitative study. Drug Saf. 2017;40(5):443–455. doi:10.1007/s40264-016-0494-x
22. Sidorkiewicz S, Tran VT, Cousyn C, Perrodeau E, Ravaud P. Discordance between drug adherence as reported by patients and drug importance as assessed by physicians. Ann Fam Med. 2016;14(5):415–421. doi:10.1370/afm.1965
23. Ali EE, Leow JL, Chew L, Yap KY. Patients’ perception of app-based educational and behavioural interventions for enhancing oral anticancer medication adherence. J Canc Educ. 2018;33(6):1306–1313. doi:10.1007/s13187-017-1248-x
24. Santo K, Richtering SS, Chalmers J, Thiagalingam A, Chow CK, Redfern J. Mobile phone apps to improve medication adherence: a systematic stepwise process to identify high-quality apps. JMIR Mhealth Uhealth. 2016;4(4):e132. doi:10.2196/mHealth.6742
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.