")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Development and Validation of IBSA Photographic Scale for the Assessment of Inner Upper Arm Laxity
Authors Cassuto D , Pellacani G, Tateo A, Artzi O , Ingallina FM, Salti G, Rossi E, Lanzarotti A, Laouedj M, Dapis N, Bellia G
Received 17 June 2021
Accepted for publication 22 September 2021
Published 12 October 2021 Volume 2021:14 Pages 1465—1471
DOI https://doi.org/10.2147/CCID.S317857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Daniel Cassuto,1 Giovanni Pellacani,2 Antonello Tateo,1 Ofir Artzi,3 Fabio Massimo Ingallina,4 Giovanni Salti,5 Elena Rossi,2 Arturo Lanzarotti,6 Malika Laouedj,7 Nicolas Dapis,7 Gilberto Bellia8
1Private Practice, Milan, Italy; 2Department of Dermatology, University of Modena and Reggio Emilia, Modena, Italy; 3Department of Dermatology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel; 4Private Practice, Catania, Italy; 5Private Practice, Florence, Italy; 6IBSA Institut Biochimique SA, Lugano, Switzerland; 7Quantificare SA, Valbonne, France; 8IBSA Farmaceutici Italia, Lodi, Italy
Correspondence: Gilberto Bellia
IBSA Farmaceutici Italia, Lodi, Italy
Email [email protected]
Objective: To describe the development and validation of the 5-grade photographic IBSA inner upper arm scale.
Methods: From 2 real-life pictures, a scale made up of 5 morphed images showing increasing severity of inner upper arm laxity was created. For validation, a set of 50 images (half of which real and the other morphed) was developed and sent to 5 trained physicians in two rounds 30 days apart. Raters’ task was to make a selection of each image according to the given scale. Inter-rater and intra-rater reliability were evaluated in both rounds.
Results: As to intra-rater reliability, single-rater kappa scores between 0.74 and 1.00 and a global kappa score of 0.846 were observed, while inter-rater agreement was calculated with intra-class correlation coefficient reporting scores higher than 0.91, which indicate excellent reliability.
Conclusion: IBSA inner upper arm laxity scale proved to be a validated and reliable tool.
Keywords: photographic scale, upper inner arm, laxity, aesthetic medicine, scale validation, scale development
Introduction
Rejuvenation therapies are becoming increasingly popular as people are concerned about improving the appearance of exposed areas of the body other than the face, such as the arms. The current need is to have a younger look, therefore arm-related rejuvenation therapies are increasingly requested. This growing demand requires physicians to be able to confidently face different clinical presentations, selecting the most appropriate treatment.
A pleasant looking upper arm is lean, tapering both at the elbow and axilla with an anterior convexity in the deltoid region that merges with the biceps. Because of ageing, the skin of the upper arm loses elasticity and firmness, moreover the underlying layers of fat, muscle and bone undergo an inevitable process of deterioration.1 The upper arm contains deep and superficial fat layers (Figure 1). The deep fat layer is thin and located in the posterior and deltoid region of the arm, while the superficial fat layer is circumferential and it is prone to hypertrophy, especially in the posterior one-third. A larger volume of fat is therefore found in the more proximal area of the arm. The anterior surface and distal third of the arm tend to have thinner adipose tissue.2 The skin of the medial aspect of the arm is thin, prone to sag and with no hair follicles. Weakening of the connections between the superficial fascial system (SFS) and the axillary fascia, as well as loosening of the axillary fascia itself due to ageing, weight fluctuations and gravitational pull, result in an evident ptosis of the posteromedial arm. Flaccidity of the posterior arm muscles caused by age along with a lack of exercise may worsen the deformity.3 This phenomenon is generally referred to as brachial ptosis of the internal surface of the arm and results in skin laxity, which may extend from the chest wall to the olecranon, leading to a loss of muscular mass, as well as an enlargement of the inferior curve of the arm.4
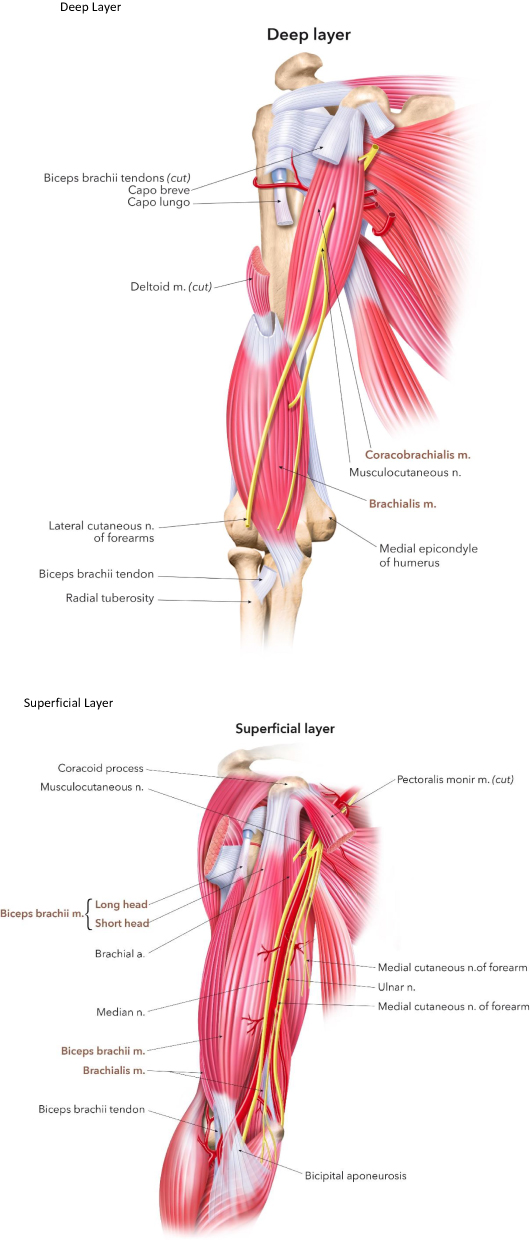 |
Figure 1 Structure of the upper arm. Deep Layer. Superficial Layer. |
While exercise may enhance muscle tone and upper arm strength, it will not improve the tone or laxity of the skin, which is normally corrected by skin excision and removal of subcutaneous fat, which requires an extensive incision which might lead to complications.5 Dermal fillers represent a less invasive option for arm contouring and show unquestionable advantages compared to surgery in terms of inter- and post-operative management, leading to fewer complications as to nervous, vascular, lymphatic and muscular structures, and absence of any scarring.
There are currently a large number of non-invasive body-contouring treatments based on devices that cause adipocyte disruption or apoptosis among which radiofrequency (RF) is the most commonly used, while other methods include ultrasound, cryolipolysis and low-level laser therapy (LLLT).6
Several variables linked to patient’s characteristics influence therapeutic choices. Despite possible complications, surgery is usually the best option in case of severe laxity and tissue deterioration. However, in intermediate stages fillers could be the right solution. Evaluation of treatment options is up to the personal assessment, experience and aesthetic judgement of physicians. To make this tough task easier and provide an early assessment, IBSA in collaboration with physicians designed a photographic scale which consists of 5 grades that differ according to the laxity of inner upper arm tissues.
According to Italian law, this scale validation was exempt from ethic committee approval as no human beings have been involved, and it was conducted according to the ethics of the Declaration of Helsinki. Information and data were generated, recorded, documented, and processed in accordance with a specific procedure, based on The International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) Good Clinical Practice (GCP). All validators signed an informed consent form at the time of the enrolment in order to collect the clinical data. The development and validation processes of this innovative photographic aid are the topics of this publication.
This trial was carried out by means of pictures only, therefore no approval by any Ethical Committee was needed, moreover all subjects had signed informed consent prior to any use of their images.
Methods
Scale Development (Figure 2)
The scale was developed and validated following previously developed and published photonumeric scales, whose methods were adjusted and customized for the purposes of the tool here described.7–10
 |
Figure 2 Algorithm of development and assessment of the IBSA inner arm laxity scale. |
 |
Figure 3 Continue. |
 |
Figure 3 The 5-grade IBSA inner arm laxity scale. Grade 1. Grade 2. Grade 3. Grade 4. Grade 5. |
A team made up of a plastic surgeon, IBSA Scientific Responsible for Dermoaestetics, and QuantifiCare R&D Head chose two photographs one of an inner upper arm with a healthy look, and another with the most severe degree of laxity to represent a borderline stage, beyond which the use of a filler would not be suggested.
Photos of the arms of 47 patients ranging between 42 and 79 years of age were selected. All photos were taken with a Canon Eos 650D camera and had a resolution of 6 mega-byte (MB). Once this first selection was made, QuantifiCare and the 3 experts developed a photographic scale composed of 5 images by means of a morphing program. The images show the left arm outstretched and abducted 90 degrees from the body, with the palm facing downwards, as this is the best position for assessing tissue laxity (Figure 3).
According to the tone and degree of laxity of the tissues, the 5 grades are described as follows:
Grade 1: Normal trophism of the tissues of the inner upper arm
Grade 2: Mild laxity of the tissues of the inner upper arm
Grade 3: Moderate laxity of the tissues of the inner upper arm
Grade 4: Moderate to severe laxity of the tissues of the inner upper arm
Grade 5: Severe laxity of the tissues of the inner upper arm
A set of 25 real plus 25 morphed photographs was created for the validation by 5 selected raters. To double-check the newly born scale, the raters had previously been shown the 5 morphed images for a ranking test that included the 5 selected Grades along with other non-selected morphed images: during this exercise, validators were given the descriptors and they had to match what they recognized as the most suitable image. This procedure was repeated in two sessions with a break of a week, and the previously developed scale was confirmed.
Software Characteristics
Software development and validation followed GAMP5 methodology, compliant to 21 CFR part 11, based on pseudonymized photographic data sorted in a folder architecture to generate a Microsoft Access Database file followed by a Comma Separated Value file. A Phase one XF IQ150 camera was used to acquire photographic data. Windows 10 and DirectX 9 or superior was the software required, and at least 2GB of free space on the hard drive, 4GB of RAM memory as a hardware, and a screen resolution of a minimum of 1024 × 768 were needed. Each page of the software displayed 1 photo and the user had to score it before submitting and go to the next page. During the Webex training session, experts were presented a demo of the tool to clarify any possible doubt. Validators had the possibility to restart and make use of the training module whenever they needed to. Users were given a personal login. Score options were five (Grade 1, Grade 2, Grade 3, Grade 4, and Grade 5), and only one could be selected. One photo per patient was displayed by the application, and full-screen visualization and image enlargement were available by clicking on the photo. Users could interrupt the evaluation any time to resume it later. It was not allowed to go to next subject without having scored the previous one; yet, it was possible to modify any of the scores already assigned with no time limit. IBSA received the final results in a CSV file, along with a report as specified for each subject and name of evaluators.
Scale Validation (Figure 2)
Raters were given 30 days one month apart for each of two evaluation rounds. Images were the same in both sessions, but their order was different. Data were eventually collected by QuantifiCare for IBSA statistical analysis for inter-rater and intra-rater assessments.
Results
Intra-Rater Reliability (Table 1)
Weighted kappa scores with Fleiss-Cohen weights were used to calculate intra-rater reliability between the first and the second evaluation performed by the same expert, by analysing each one of them individually, and all the first and the second available evaluations together.
 |
Table 1 Intra-Rater Reliability with the Weighted Kappa Scores Calculated with the Fleiss-Cohen Weights and Upper and Lower Confidence Interval Limits Combined |
Kappa scores were between 0.71 and 1.00 according to expert analysis and when the 5 expert evaluations were analysed together score was 0.846, indicating substantial/almost perfect agreement between the first and second evaluations performed on the same image. An exact method was used to estimate the 95% confidence interval limits for the weighted kappa scores.
Inter-Rater Reliability (Table 2)
Inter-rater agreement was calculated by means of Shrout and Fleiss intra-class correlation coefficient, considering the first and the second evaluation separately, and analyzing the two evaluations together. Outcomes showed good/excellent reliability.
 |
Table 2 Overall Inter-Rater Reliability as Described by Shrout-Fleiss |
Study Limitations
This study was carried out only on female subjects of Caucasian ethnicity, without taking into account few variables, such as the Fitzpatrick scale. Therefore, this tool might need a future adjustment according to other objective parameters, in order to be reliable for subjects of different or mixed ethnicity, phototype, and males as well.
Discussion
Due to the growing number of patients who demand rejuvenation procedures of the inner upper arm, a tool that can help physicians evaluate the laxity of this anatomical region represents a real clinical need. In addition to surgery, which is still the best treatment in case of severe tissue impairment, the use of dermal fillers is becoming increasingly popular due to their unquestionable advantages over more invasive solutions.
This scale was developed using digital techniques and real photos, it is a simple tool that makes it possible to quickly discriminate between different clinical presentations, doctors validated it basing their responses on their clinical experience, highlighting its reliability.
The tool here described identifies ageing-related conditions which affect the volume and shape of the inner upper arm, and each severity degree is represented by an image and its corresponding descriptor, which are affected by real-life and individual variables, including substantial differences related to the appearance of the dominant arm, possible skin discolouration, and anatomical changes due to trauma, congenital or environmental reasons (eg, sports, job, life-style), which represent an intrinsic and understandable limitation to the classification by means of a scale of any aesthetic condition related to other body parts. Hence, the best way to evaluate the advantages of this scale is in clinicians’ daily practice, and from the Authors’ viewpoint it might be used to complete the manual examination that it is normally performed to assess tissue structure and laxity.
Moreover, subjects who are willing to undergo procedures for improving the look of the inner upper arm have often already undergone surgery in other more socially exposed areas (for example, the face and the neck), and they are therefore looking for some sort of homogeneity and evenness in their appearance. Thus, an instrument such as the one here described might be helpful in making them more self-aware of their own appearance and therapeutic options.
Capsule Summary
- A tool that can help physicians evaluate the laxity of the inner upper arm needs to be developed due to the growing demand for rejuvenation procedures in this anatomical region by patients.
- The IBSA upper inner arm scale uses 5 images developed using digital techniques and real photos. It is a simple tool that makes it possible to quickly discriminate among different clinical conditions.
Conclusions
Both inter- and intra-rater results indicate overall consistency and reliability of the scale created.
Acknowledgments
The authors are grateful to Marta Castano, who helped with the writing of this manuscript.
Funding
This project has been sponsored by IBSA Farmaceutici Italia.
Disclosure
AL is an employee of IBSA SA Switzerland. ML & ND are employees of Quantificare SA France. GB is an employee of IBSA Farmaceutici Italia. The authors report no other conflicts of interest in this work.
References
1. Glanz S, Gonzalez-Ulloa M. Aesthetic surgery of the arm: part I. Aesthet Plast Surg. 1981;5:1–17.
2. Chamosa M, Murillo J, Vazquez T. Lipectomy of arms and lipograft of shoulders balance the upper body contour. Aesthet Plast Surg. 2005;29(6):567–570. doi:10.1007/s00266-004-0101-x
3. Lockwood T. Brachioplasty with superficial fascial system suspension. Plast Reconstr Surg. 1995;96:912. doi:10.1097/00006534-199509001-00022
4. de Souza Pinto EB, Erazo PJ, Matsuda CA, et al. Brachioplasty technique with the use of molds. Plast Reconstr Surg. 2000;105(5):1864–1865. doi:10.1097/00006534-200004050-00037
5. Correa-Iturraspe M, Fernandez JC. Dermolipectomiabraquial [Brachial dermolipectomy]. Prensa Med Argent. 1954;41:2432–2436. Spanish.
6. Nassab R. The evidence behind non invasive body contouring devices. Aesthet Surg J. 2015;35(3):279–293. doi:10.1093/asj/sju063
7. Jones D, Donofrio L, Hardas B. Development and validation of a photonumeric scale for evaluation of volume deficit of the hand. Dermatol Surg. 2016;42(1):S195–S202. doi:10.1097/DSS.0000000000000850
8. Sykes JM, Carruthers A, Hardas B. Development and validation of a photonumeric scale for assessment of chin retrusion. Dermatol Surg. 2016;42(1):S211–S218. doi:10.1097/DSS.0000000000000849
9. Donofrio L, Carruthers A, Hardas B. Development and validation of a photonumeric scale for evaluation of facial skin texture. Dermatol Surg. 2016;42(1):S219–S226. doi:10.1097/DSS.0000000000000852
10. Jones D, Carruthers A, Hardas B. Development and validation of a photonumeric scale for evaluation of transverse neck lines. Dermatol Surg. 2016;42(1):S235–S242. doi:10.1097/DSS.0000000000000851
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.