")
Back to Journals » Clinical Audit » Volume 16
Documentation of Inpatient Medical Records: A Clinical Audit
Authors Awad MSA , Mohamednour MF, Rafat FA, Altijani M, Elfatih A, Hamed FJM, Muhammed A , Awad I, Alkheder MA, Elhado MAO, Yahya A
Received 6 December 2023
Accepted for publication 24 February 2024
Published 28 February 2024 Volume 2024:16 Pages 9—17
DOI https://doi.org/10.2147/CA.S451630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zoka Milan
Mustafa Sabir Abakar Awad,1 Mohamed FA Mohamednour,2 Fakher Aldeen Rafat,3 Mohaned Altijani,4 Abdelrahman Elfatih,3 Faris Jamalaldeen Mohammed Hamed,4 Abubakr Muhammed,5 Ibrahim Awad,6 Mohammed Alsiddig Alkheder,7 Mohammed Almubarak Omer Elhado,1 Aymen Yahya8
1Department of Community Medicine, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 2Department of Physiology, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 3Department of Internal Medicine, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 4Department of Surgery, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 5Department of Anatomy, Gezira University Faculty of Medicine, Gezira, Sudan; 6Department of Microbiology, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 7Department of Anatomy, Al-Neelain University Faculty of Medicine, Khartoum, Sudan; 8Managil Teaching Hospital, Managil, Gezira, Sudan
Correspondence: Mustafa Sabir Abakar Awad, Email [email protected]
Background: Effective documentation is essential for ensuring high-quality clinical practice. Medical notes serve as a crucial form of communication among all those who are involved in a patient’s care. Therefore, it is important to have a quality assurance mechanism in place to ensure that medical records comply with established standards.
Objective: To evaluate the quality of medical notes writing in different departments of Mangail Teaching Hospital, and to implement some possible solutions to improve the quality of existing medical records and overcome the deficiencies.
Methodology: A retrospective, prospective observational audit carried out in Managil Teaching Hospital, we included 108 files in both audit cycles, 54 in each. Sampling was done through a systematic simple random sampling method over a period of one week for every cycle. Data were collected and each file was compared to the Royal College of Physician standards, the collected data were entered into an Excel sheet, cleaned then analyzed using Statistical Package for Social Sciences (SPSS) version 25 using frequency tables test.
Results: A total of 108 samples were included. In the 1st cycle only 16.1% of doctors wrote the patient’s occupation, and 14.3% wrote the contact number, regarding the history section only 41.1% documented the patient’s history of presenting complaint. In the 2nd cycle, 74% documented the occupation, 76% wrote the contact number. One hundred percent have documented the patient’s history of presenting complaint. The overall impression was excellent in 0% in the 1st cycle and 55.6% in the 2nd cycle.
Conclusion: Documentation practice in our teaching hospital did not meet the standards and the evaluating parameters used in the assessment showed high percentage of poor and unsatisfactory practice during the 1st cycle, however after a series of medical practitioner’s orientation a significant improvement was observed regarding inpatient medical records filling.
Keywords: medical records, clinical audit, quality improvement
Introduction
Clinical audit is a quality improvement process in patient care by looking at current practice, identifying the defects and how far it is from the current standards of practice, and then applying modification where necessary. It constitutes one of the best methods for raising the standard of patient care.1
Effective documentation is essential for maintaining high standards in clinical practice. The General Medical Council (GMC) emphasizes in its primary text, “Good Medical Practice”, that doctors are required to maintain clear, precise, and easily readable records when giving care.2 Nevertheless, a dearth of knowledge, apathy, established routines, or a combination of these factors lead to inadequate records, thus exposing both the patient and the practitioner to potential harm. This can be ascribed to the sporadic, and frequently non-existent, nature of schooling on this subject.
Effective clinical documentation enhances the optimization of patient care. Medical notes serve as a crucial method of communication among healthcare providers and facilitate important communication with patients and their family members.
Medical records are becoming increasingly crucial in medico-legal issues and litigation. Records can serve as evidentiary support for legal claims, even if they are made months or years after the incident. Therefore, it is crucial to ensure accuracy in such cases. Clinical records moreover furnish data for utilization in audit and study. This is an essential element of clinical governance, encompassing the monitoring of hospital targets and performance. Hence, it is evident that there exist numerous justifications for upholding medical records to the utmost quality.
We adhere to the medical record keeping guidelines established by the Royal College of Physicians (RCP) in 2007. These standards state that medical notes must be accessible at all times to individuals providing input to the patient and should be stored properly. The current admission should be filed in chronological order in the appropriate section of the notes. Each page must display the patient’s name, date of birth, and a unique identifier. All entries should be dated and timed using the 24-hour clock. Each entry should be concluded with the signature, printed name, and designation of the person making the entry, as well as a contact number. Additionally, the content of the entry should be organized and easy to read.3
The guidelines provided by The Royal College of Surgeons of England for physicians on medical records and notes encompass not just the aforementioned requirements, but also offer detailed instructions on nursing records, records of patients undergoing surgery, anesthetic records, and discharge documents.4
To the author’s knowledge, there have been no published audits on inpatient medical records documentation in Sudan. Therefore, this audit is the first of its kind in the country. The knowledge gap is substantial, and it is hoped that this study will serve as the foundation for future research aimed at enhancing clinical practice.
Aims and Objectives
The aim of the current audit was to improve the quality of documentation of the medical notes at Managil Teaching Hospital. The aim was also to evaluate the quality of medical notes writing in different departments at the hospital, and to propose some possible solutions to improve and overcome the deficiencies.
The Standards
The RCP Standard consists of nine parameters, as illustrated in Figures 1–6, and an overall grade would be given for each parameter as follows: excellent, good, poor and not satisfactory depending on how they were completed and the quality of their completion.
 |
Figure 1 RCP Personal data and History section. |
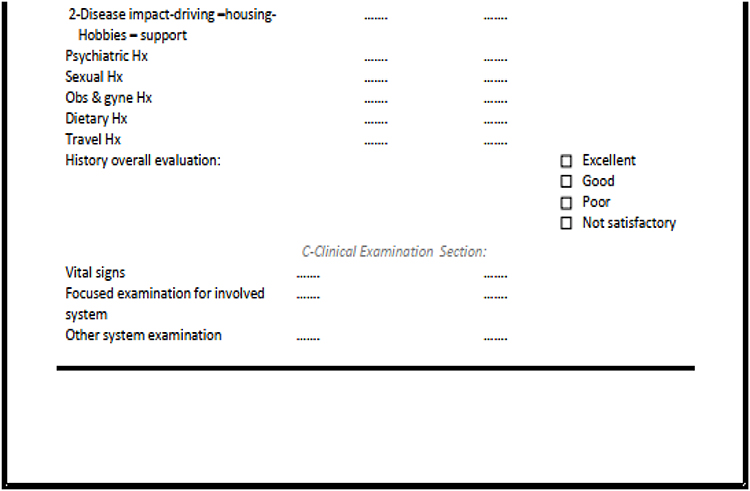 |
Figure 2 RCP the rest of the History section and Clinical examination section. |
 |
Figure 3 RCP Investigation and Management plan sections. |
 |
Figure 4 RCP Diagnosis and Progress Notes section. |
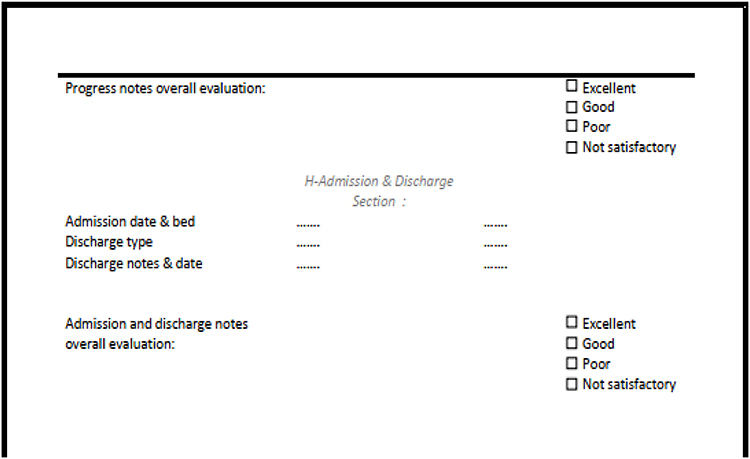 |
Figure 5 RCP Admission & Discharge section. |
 |
Figure 6 RCP Attending doctors and legibility of notes section. |
Assessment Parameters: Personal data Figure 1, History section Figures 1 and 2, Examination Figure 2, Investigation Figure 3, Management plan Figure 3, Diagnosis Figure 4, Progress notes Figure 4, Admission & discharge details Figure 5, Attending doctors details and legibility of the notes Figure 6.
Methodology
Audit Design
A retrospective, prospective observational study. We audited the existing medical records in the medical record office in the hospital retrospectively and after the implemented changes were carried out a second cycle.
Audit Area/Population
Managil Teaching Hospital, Managil locality, Gezira state, Sudan. This comprises the main health provider sector at the locality with a capacity of over 200 beds, on the period from September to November 2023. The study included all the four major divisions at the hospital, Medicine, Surgery, Pediatrics and Obstetrics & Gynecology, with a main focus on the Medicine department. The inclusion criteria included all files of admitted patients at the time of the audit and duration of hospital stay not less than one week.
Sample Size and Sampling Technique
A systematic simple random sampling method was applied to include files from medicine, surgery, obstetrics and gynecology and pediatrics departments which were admitted during the period from September 2023 to November 2023 with a time gap of one week between both cycles. The first cycle was conducted between 27 September to the third of October and the 2nd cycle between 11 and 18 October, with a total of 108 files for both cycles, 54 in the 1st and 54 in the 2nd cycle.
Data Collection Methods and Analysis
The data were collected from case files available at medical record office in the hospital. The techniques applied were survey and observation. A structured checklist was adopted from the Royal College of Physicians, and the patient’s information’s were entered into a pre-designed form having all the relevant details. Each file was assessed individually and compared to the Standard checklist, each parameter was assessed separately and an overall grade was given. The majority of the data 20 in the 1st cycle and 27 in the 2nd cycle were obtained from the medicine department, the obstetrics and gynecology department was not included in the 2nd cycle due to data access difficulties. A series of doctors training and orientation sessions were carried out between the two cycles it was carried out by the audit team in terms of lecture presentations and focused group sessions, nearly all the working medical staff were oriented. A new and improved medical record structure was proposed. The changes included expanding the patient’s personal details by adding job, adding a systemic review, psychiatric, travel, sexual and dietary history in the history section. Expanding the examination section and making space for different systems examination. Introducing a Diagnosis/Summary page which contains patient case summary, problem list, provisional and final diagnosis. Adding a doctor’s signature at the end of every page. Adjusting the investigation sheet to include radiological requests. Introducing an Admission and discharge section that included admission and discharge date, discharge type and discharge note. The new file was endorsed by the hospital administration. The data were analyzed using Microsoft Excel® 2016 and Statistical Package for Social Sciences (SPSS) version 25. The data analysis plan encompassed several key components, namely: a master sheet for organizing the data, a data cleaning process to ensure accuracy and reliability, the utilization of descriptive statistics and summary measures to gain insights, and the presentation of the data through tables and figures.
Ethical Clearance
The study's ethical clearance was obtained from the ethical committee at Managil Teaching Hospital, and locally from the health affairs at Managil locality.
Results
A total of 108 samples were included in the study, 54 in the 1st cycle and 54 in the 2nd cycle. In the first cycle, the samples were collected from medicine, surgery, pediatrics and obstetrics and gynecology departments, and then they were compared with the standard. The second cycle included the same sample size as the 1st cycle 54 samples from all departments except for obstetrics and gynecology, and the collected data were compared with the RCP standards. In the 1st cycle, only 16.1% of doctors wrote the patient’s occupation, and 14.3% wrote the contact number, regarding the history section only 41.1% documented the patient’s history of presenting complaint, 37.5% wrote the systemic review while 0% documented the impact of the disease and 55.4% wrote the patient’s vitals. In the 2nd cycle however, 74% documented the occupation, 76% wrote the contact number. One hundred percent have documented the patient’s history of presenting complaint and 64.8% wrote the impact of the disease. Vital signs were written in all files 100 as shown in Table 1. The overall impression in the 1st cycle was excellent in 0%, good in 33.3%, poor in 55.6% and non-satisfactory in 11.1%, in the 2nd cycle it was excellent in 44.4% and good in 55.6%, both poor and non-satisfactory scores were 0% as demonstrated in Table 2.
 |
Table 1 Standard Criteria and Assessment Parameter Application |
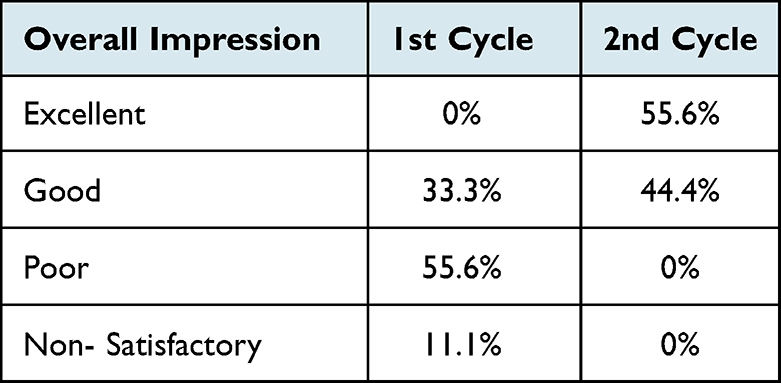 |
Table 2 Overall Impression |
Discussion
The audit aimed to examine the current practice at Managil Teaching Hospital regarding the inpatient medical records filling and to improve the ongoing practice to meet the international (RCP) standards.
Our hospital and public health systems are still maintaining handwritten patient’s notes. Our main area of deficiency was in the domain of documentation of patients’ weight, proper history and examination, documentation of final diagnosis and discharge notes.
Unfortunately, patient’s charts including daily readings of vital signs and renal charts are not documented and even there are no space designed in our patients’ files to keep them, nursing notes are documented in separated records kept by nursing staff instead of being included in patients’ records.
Documenting weight was only done in 12.5% in the 1st cycle which is attributed to weight scale devices are only available in the pediatric department, the improvement by 37% in the 2nd cycle is not the required percentage but it is a step towards the standard, it was proposed to the administration to provide a scale for each department and weight is an essential part in management. The contact number, however, was only documented in only 14.3% of the files from the 1st cycle, such an important tool and an essential element regarding communicating with the patient, in the 2nd cycle it was observed in 76% of the files.
History, on the other hand, showed the lowest percentages observed in our study as the social history (disease impact), psychiatric and sexual history were only documented in 0%, 5.4% and 1.8%, respectively, in the 1st cycle and 64.8%, 29.6% and 40.7%, respectively, in the 2nd cycle, noticed the improvement in the psychiatric and sexual history is not that significant in comparison to the social history which can be explained by the social stigma accompanying the psychiatric illness in our society and the conservative nature of our community abide not to talk openly about ones sexual life. History section overall can be regarded as unsatisfactory in the 1st cycle and good to excellent in the second.
Only 13.2% of doctors in the 1st cycle documented the other system examination of their patients and 55.4% wrote their vitals which is an unusual finding because vital signs checking and full body examination is a mandatory procedure to all admitted patients at the hospital, although most interns do the full body examination supervised by the resident, yet they do not document it this mostly due to indifference or lack of awareness about the importance of documentation. Fortunately, after multiple orientation sessions targeting mainly the interns, the percentage dramatically rose to 100% in the 2nd cycle for both parameters.
Flow chart of investigation was documented in 10.7% of the studied cases in the 1st cycle, an odd finding as well because investigation flow chart constitutes one of the cornerstones in flow up and patients’ progression. The finding can be attributed to the existing structure of medical records, where the investigation flow chart is placed at the end of the file, resulting in poor organization. However, the percentage rose to 96.3% during the 2nd cycle.
The discharge note is another important parameter in the medical record, was only filled by only 1.8% in the 1st cycle, lack of awareness, ignorance and indifference are the main cause of this finding, the improvement was 44.4% in the second cycle, it is expected to rise even more after the introduction of the new file.
Investigations, treatment plans, diagnosis sections and admission-discharge sections were generally documented in a poorly manner in the first cycle.
Overall documentation practice was not satisfactory in (11.1%), poor in (55.6%), and good in (33.3%) of the case notes in the 1st cycle. These results were reflecting alarming flags regarding documentation practice in our department. However, the overall impression improved to be excellent in (44.4%) and good in (55.6%) with no poor nor non-satisfactory.
The element of a possible bias should be considered as some of the assessment parameters were assessed based on the individual evaluator’s point of view and not in an objective manner.
Limitation
The audit was limited by some factors, like the relatively small sample size and the non-inclusion of obstetrics and gynecology department in the 2nd cycle which could induce a selection bias.
Recommendations
- To communicate the importance of medical records and good documentation practice to all staff.
- To improve the pre-existing patient’s files to the standard criteria.
- To reward the best doctors who achieve excellent documentation practice.
- To run a regular sessions for training purposes in documentation of medical records and raise awareness about how important it is to keep up with the standards.
- To evaluate and assess regularly medical records by senior doctors and quality control department.
- To sustain the implemented changes done.
- To conduct a third cycle after the recommendations are implemented.
Conclusion
Medical records are very essential documents in the hospital and health system as general. Documentation practice in our teaching hospital did not meet the standards and the evaluating parameters used in the assessment showed high percentage of poor and unsatisfactory practice during the 1st cycle, however after a series of medical practitioner’s orientation a significant improvement was observed regarding inpatient medical records filling.
Medical records are vital for future care planning, research, and legal considerations. The importance of high-quality medical records should be communicated to all medical staff in the department.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rawlins M, Hine DD. Principles for Best Practice in Clinical Audit-National Institute for Clinical Excellence. Oxford: Radcliffe Medical Press Ltd; 2002.
2. General Medicine Council. Good Medical Practice. London: General Medicine Council; 2013.
3. The Royal College of Physicians. Generic Medical Record Keeping Standards. London: The Royal College of Physicians; 2009.
4. The Royal College of Surgeons on England. Guidelines for Clinicians on Medical Records and Notes. London: The Royal College of Surgeons on England; 1994.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.