")
Back to Journals » Clinical Interventions in Aging » Volume 19
Does Walking Have an Association with Osteoarthritis? A Two-Sample Mendelian Randomization Analysis
Authors Xu J , Zhang L , Wang P, Zhang C , Ji S
Received 3 October 2023
Accepted for publication 21 January 2024
Published 31 January 2024 Volume 2024:19 Pages 153—161
DOI https://doi.org/10.2147/CIA.S442259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Jiankang Xu,1,2,* Longyao Zhang,1,2,* Ping Wang,1,2 Chao Zhang,1,2 Shuqing Ji3
1Orthopedics Department, The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 2Orthopedics Department, National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, People’s Republic of China; 3Orthopedics Department, Tianjin Jizhou District Traditional Chinese Medicine Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Zhang, Orthopedics Department, The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China, Email [email protected]
Objective: Osteoarthritis (OA) is one of the major disabling human diseases. The related studies indicate a potential correlation between walking and OA. However, there is still a lack of evidence in genetics to support the correlation between walking and OA. Therefore, this study aimed to explore the relationship between walking and OA at the genetic level.
Methods: The publicly available Genome Wide Association Study (GWAS) data were used, with inverse variance weighting (IVW, the random-effects model) as the main analysis method, whereas MR-Egger, Weighted median, Simple mode, and Weighted mode as the secondary analysis methods. In addition, Cochran’s Q test, pleiotropy test, and MR-Egger intercept test were conducted to examine the heterogeneity and pleiotropy of the outcome.
Results: In the MR analysis, IVW results showed a negative correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA (KOA or HOA) (odds ratio (OR) = 0.3224, 95% confidence interval (CI): 0.1261 to 0.8243), and the difference was of statistical significance (P = 0.0181). Moreover, IVW results also revealed a negative correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and KOA (OR = 0.1396, 95% CI: 0.0484 to 0.4026), and the difference was statistically significant (P = 0.0003). However, IVW results did not demonstrate any statistical significance types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and HOA (OR = 1.2075, 95% CI: 0.1978 to 7.3727, P = 0.8381).
Conclusion: From genetic studies, types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) is negatively correlated with knee osteoarthritis (KOA), but there is no clear evidence supporting its correlation with hip osteoarthritis (HOA).
Keywords: osteoarthritis, walking, Mendelian randomization
Introduction
Osteoarthritis (OA) is a chronic and progressive degenerative joint disease, which accounts for one of the leading causes of disability in the elderly population. Due to the increasing aging of the population, OA also shows an increasing incidence rate year by year. In recent years, we have gained a deeper understanding of the pain mechanisms and pathogenesis of OA.1 To be specific, the main mechanism of osteoarthritis is the inflammatory response of the synovium, cartilage, and subchondral bone tissue, leading to gradual cartilage wear. This results in alterations in the biomechanical environment of the joint, ultimately causing joint dysfunction.2–5 As a degenerative disease, OA will induce changes in the tissues surrounding the joint, including cartilage, bone, synovium, ligaments, muscles, and fat.6 Such changes can cause joint dysfunction, pain, stiffness, limited mobility, and loss of valuable activities.6 Although OA can affect any joint in the body, it usually affects the hands, knees, hips, and feet.3,6 OA is one of the main causes of disability in the elderly, which significantly reduces the mobility of patients.2 Meanwhile, people with OA often develop more comorbidities and are more likely to sit for a longer period of time than those without OA.6 A lack of physical activity can increase the age-adjusted mortality rate by 20%, since the lack of exercises can increase the risk of cardiovascular disease and other diseases.6,7 OA is one of the main causes of disability in elderly individuals, significantly impacting their quality of life and increasing their economic burden.8,9 Therefore, it is crucial to identify the pathogenic factors of OA and find ways to reduce the likelihood of its occurrence.
Walking is a simple, convenient, low-cost, and beneficial physical activity for health, which does not require special skills or equipment and can be done at any time and any place. As discovered by Chang et al10 from their research, walking exercise improved the cardiorespiratory fitness and balance during walking. Besides, Moghetti et al11 concluded that walking improved blood glucose control in patients with type 2 diabetes, and had positive effects on hypertension, cardiorespiratory health, and weight management. Furthermore, most studies have suggested that walking can increase muscle strength,12,13 which may lower the progression and occurrence of HOA and KOA. However, there is a lack of research support for the specific impact of walking on OA in terms of genetics.
Mendelian randomization (MR) is a randomized control method based on genetic variation, and it is used to evaluate causal relationships in observational studies.14 In MR, researchers use the known genetic variations as a natural randomization factor to randomly assign participants into different genotype groups, thus simulating a randomized controlled trial.15,16 As genetic variation is determined early in life and is not affected by environmental factors, MR analysis can reduce the bias caused by confounding variables and improve the reliability of causal inference.17
Researchers typically use single nucleotide polymorphisms (SNPs) as instrumental variables to assess the impact of biological factors on health outcomes. By associating SNPs with the factors of interest, researchers can determine whether these factors affect the specific health outcomes.18 This method helps address common problems in observational studies, including confounding variables, reverse causality, and measurement errors.19 Therefore, MR has been widely applied in various research fields, and its reliability has been gradually demonstrated. Zheng et al20 applied MR analysis and discovered that the use of glucosamine reduced the risk of dementia. Consequently, in the biomedical field, the application of MR has a wide-ranging and profound impact, which has provided important tools and methods for revealing the impact of biological factors on health.
This study aimed to employ MR analysis to examine the association between walking for pleasure (not as a means of transportation) and OA over the past four weeks, so as to validate the preventive and therapeutic effects of walking on OA from a genetic perspective.
Materials and Methods
Data Source and Population
We obtained our research data from the ieu Open GWAS project (https://mrcieu.ac.uk), which is a public database comprising whole-genome association study (GWAS) data from the UK Biobank (UKB) and the European Bioinformatics Institute (EBI). Therefore, no ethical approval is required for this study. To control for the influence of the population on the results, only individuals of European ancestry were selected as the study subjects, and corresponding screening of exposure and outcome was conducted to ensure the reliability and accuracy of our results.21
Exposure data were GWAS ID: ukb-b-7337, which consisted of types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport).22 The sample size was 460,376 individuals, including 329,755 walkers and 130,621 controls, with a total of 9,851,867 SNPs. The data was evaluated based on the participants’ responses to the question “In the last 4 weeks did you spend any time doing the following?” (https://biobank.ndph.ox.ac.uk/showcase/refer.cgi?id=100475). Walking for pleasure (not as a means of transport) was one of the options, different from “Other exercises (eg: swimming, cycling, keep fit, bowling)”, “trenuous sports”, “Light DIY (eg: pruning, watering the lawn)”, and “Heavy DIY (eg: weeding, lawn mowing, carpentry, digging)”.
Outcome data included OA of the hip or knee joint (HOA or KOA), with GWAS ID: ebi-a-GCST007092,23 which involved 417,596 individuals, including 39,427 OA patients and 378,169 controls, with altogether 30,265,359 SNPs. KOA with GWAS ID: ebi-a-GCST00709023 had a sample size of 403,124 individuals, including 24,955 KOA patients and 378,169 normal controls, with 29,999,696 SNPs in total. HOA with GWAS ID: ebi-a-GCST00709123 contained 393,873 individuals, including 15,704 HOA patients and 378,169 normal controls, with a total of 29,771,219 SNPs.
Selection of Instrumental Variables
When selecting instrumental variables for the exposure, the instrumental variable should have a strong correlation with the exposure, which is determined upon the thresholds of P < 5×10−8, linkage disequilibrium (LD) r2 < 0.001, clumping distance (kb) = 10,000, and F-statistic > 1024,25 (Figure 1). Confounding factors in the instrumental variables should be excluded, and SNPs in the instrumental variables related to the outcome should also be removed. In this study, coronary artery disease, hypertension, body mass index, and type 2 diabetes were considered as confounding factors related to the outcome.26–29 In addition, SNPs were queried by Phenoscanner (PhenoScanner (cam.ac.uk)), and the confounding factors were manually removed.30
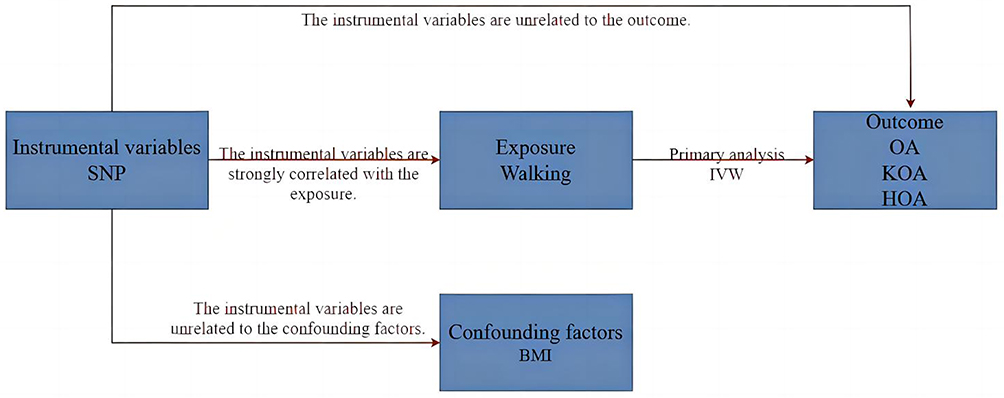 |
Figure 1 Selecting instrumental variables. Abbreviations: SNP, Single nucleotide polymorphism; BMI, Body Mass Index; OA, Osteoarthritis; KOA, Knee osteoarthritis; HOA, Hip osteoarthritis; IVW, Inverse variance weighting. |
Statistical Analysis
The statistical method used in MR analysis is mainly the two-sample random effects model with inverse variance weighting (IVW) as the primary analysis method. The IVW method assumes that all hypotheses in MR analysis are valid.31 However, instrumental variables may still affect the results via other pathways, leading to horizontal pleiotropy and errors in the results.24 In view of this, MR-Egger, weighted median, simple mode, and weighted mode were used as the secondary analysis methods.32 A p-value ≤0.05 was considered statistically significant. When the IVW method shows statistical significance but the other methods do not, OR values of the other methods must be consistent with the direction of IVW, otherwise, they are considered not statistically significant.33
The heterogeneity test for MR was performed using Cochran’s Q test, where P > 0.05 indicating the absence of heterogeneity, while P ≤ 0.05 suggesting the presence of heterogeneity. If there is heterogeneity, Mendelian randomization pleiotropy residual sum and outlier global test (MR-PRESSO) is used to remove outlier SNPs, ie, SNPs of P < 0.05.32,34 MR analysis is later performed again after removing outlier values to observe the differences in results.34 Besides, MR-Egger intercept and pleiotropy test are used to test horizontal pleiotropy, with P > 0.05 and MR-Egger intercept < 0.05 indicating no horizontal pleiotropy and more reliable results, otherwise, the result is considered invalid due to horizontal pleiotropy.35
In this study, the two-sample MR method was utilized to evaluate the relationship between exposure and outcome based on odds ratio (OR) and 95% confidence interval (95% CI). Data were analyzed with R 4.2.3 TwoSampleMR package to obtain reliable research results.
Ethical Approval
No ethical approval was needed because the present work did not use primary data.
Results
GWAS Data Related to Walking Behavior
In the GWAS database, there are 20 SNPs that meet the criteria for being associated with walking (P < 5 × 10−8, LD r2 < 0.001, Clumping distance (kb) = 10,000). There were no unharmonizable palindromic SNPs. Due to the association of rs34898535, rs11648192, rs12042107, and rs2679059 with confounding factors related to body mass index, they have been excluded. As a result, 16 SNPs were finally selected, all of which met the criterion of F-statistic > 10 (Table 1).
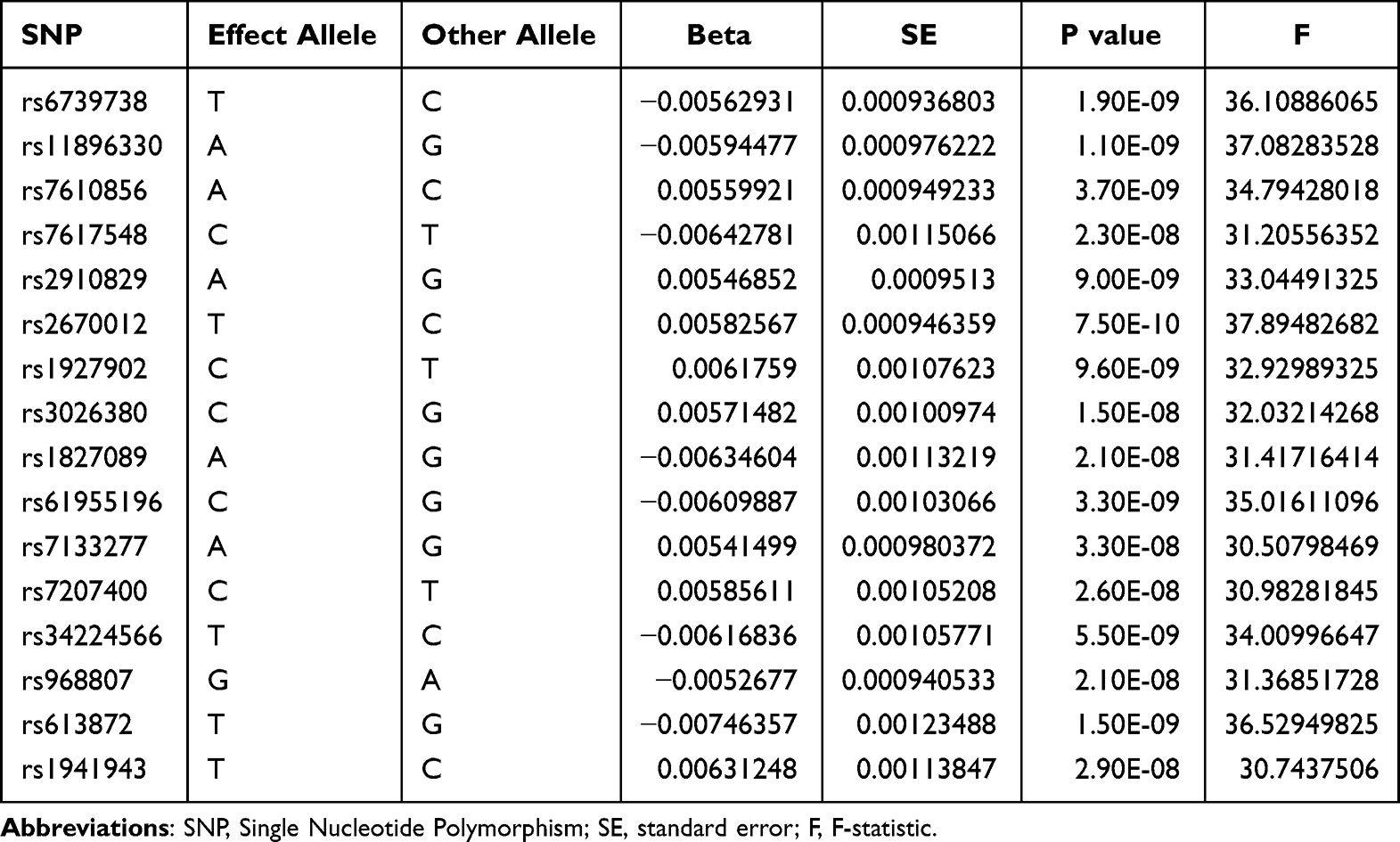 |
Table 1 SNPs Strongly Associated with Exposure |
MR Analysis
Upon MR analysis of the relationship between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA, the IVW results indicated that there is a statistically significant and negative correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA (OR=0.3224, 95% CI (0.1261, 0.8243), P=0.0181). Although the results of MR Egger, weighted median, simple mode, and weighted mode were not statistically significant (P > 0.05), the OR values were all less than 1. Therefore, it is considered that there is a relationship between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA (Table 2, Supplementary Figure 1).
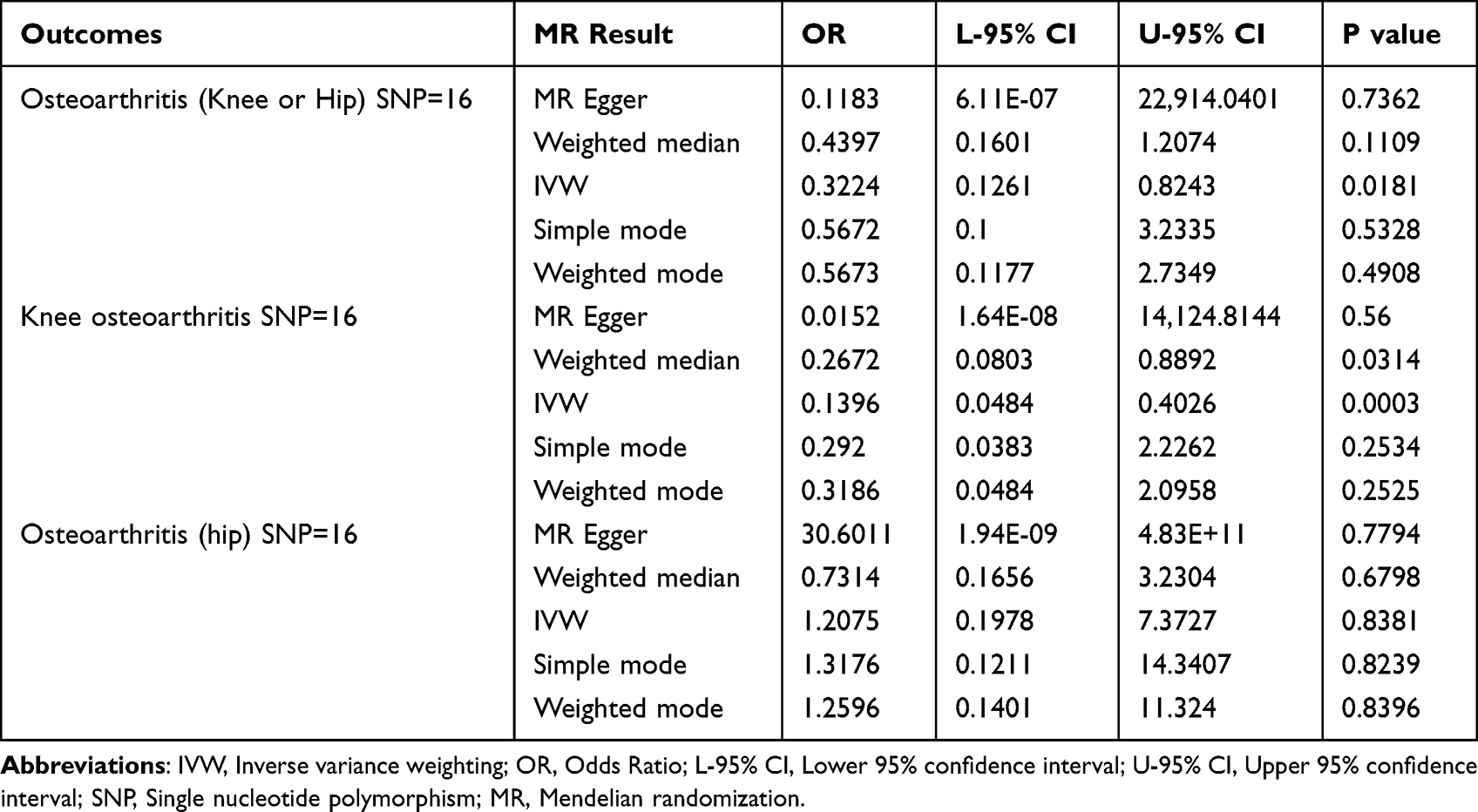 |
Table 2 MR Result |
According to MR analysis of the association between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and KOA, the IVW estimate showed that there is a statistically significant and negative correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and KOA (OR=0.1396, 95% CI (0.0484, 0.4026), P=0.0003). The weighted median estimate supported the IVW results (OR=0.2672, 95% CI (0.0803, 0.8892), P=0.0314). Although the P-values of MR Egger, simple mode, and weighted mode estimates were greater than 0.05, their OR values were all less than 1. Therefore, it was concluded that there is a relationship between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and KOA (Table 2, Supplementary Figure 1).
Based on MR analysis of the relationship between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and HOA, the P-values of all the IVW, MR Egger, Weighted median, Simple mode, and Weighted mode results were greater than 0.05. In this regard, there was no statistically significant evidence supporting the correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and HOA (OR=1.2075, 95% CI (0.1978, 7.3727), P=0.8381). In other words, types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) might not be associated with HOA.(Table 2, Supplementary Figure 1).
Heterogeneity Analysis and Pleiotropy Analysis
In this study, heterogeneity analysis and pleiotropy analysis were completed to confirm the credibility of IVW results. According to the MR Egger and IVW results, there was heterogeneity between the association of types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA (P<0.05) (Table 3); but no heterogeneity was detected between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and KOA (P>0.05) (Table 3); while heterogeneity was observed between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and HOA (P<0.05) (Table 3). Moreover, according to the results from MR-PRESSO and leave-one-SNP-out analyses, rs7207400 might have affected the outcomes in OA and HOA (Supplementary Figure 2). In addition, pleiotropy test indicated that there was no multiple-effects between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and OA, KOA, or HOA, as evidenced by the results of P > 0.05 and MR-Egger intercept < 0.05 (Table 3, Supplementary Figure 2). Thus, it was concluded that the results were of high universality and applicability.
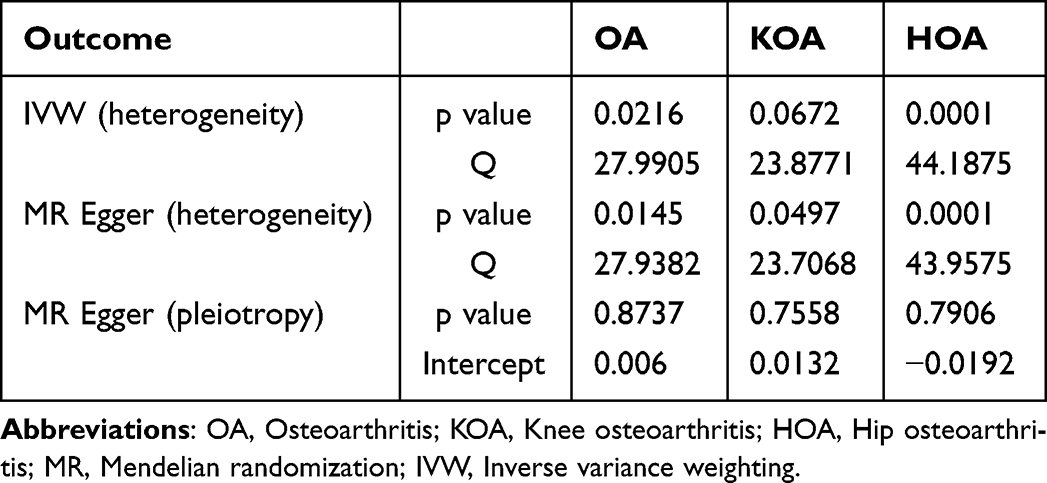 |
Table 3 Sensitivity Analysis and Pleiotropy Test |
MR Analysis After Heterogeneity Removal
After removing outliers based on the MR-PRESSO and The leave-one-SNP-out analysis results, the main result was further analyzed using IVW. As a result, there was still a negative correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and the risk of developing OA and KOA, indicating that types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) might reduce the risk of OA (OR=0.2377,95% CI (0.1121, 0.5040), P=0.0002) and KOA (OR=0.1396, 95% CI (0.0484, 0.4026), P=0.0003) (Figure 2, Supplementary Table 1). However, there was no significant correlation between types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) and HOA (OR=0.5674,95% CI (0.1915, 1.6808), P=0.3064) (Figure 2, Supplementary Table 1). Moreover, after excluding heterogeneity, no heterogeneity was detected in the results of OA or HOA (P > 0.05) (Supplementary Table 2). Therefore, the results were considered to be highly stable.36
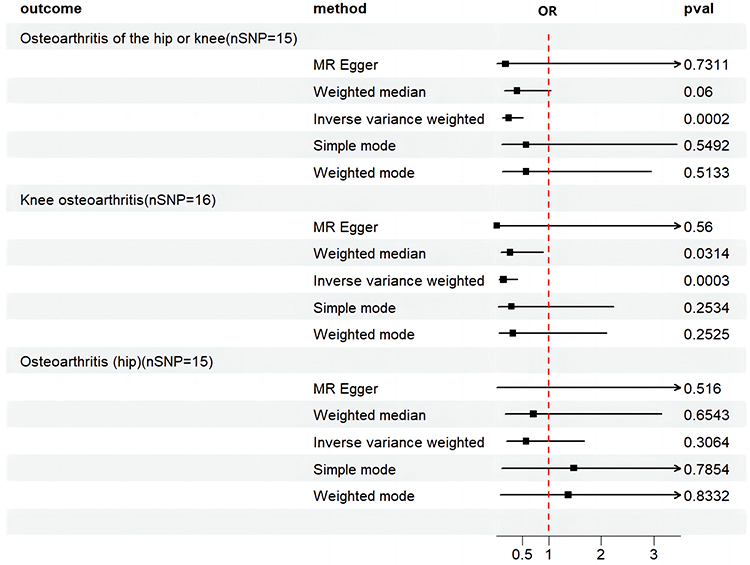 |
Figure 2 Mendelian randomization forest plot, after removing heterogeneity, depicting the impact of walking on OA. Abbreviations: OR, odds ratio; pval, p-value. |
Discussion
The MR results indicate that types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) is negatively correlated with knee osteoarthritis KOA and OA, but not correlated with HOA. Consequently, this study suggested that types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) mainly had a positive effect on KOA patients, but no significant impact on HOA. This paper provides new evidence from a genetic perspective on the clinical implications of the types of physical activity, specifically walking for pleasure (not as a means of transportation), over the past four weeks in relation to KOA.
Our research shares many of the same arguments as numerous clinical studies. Master et al37 found that walking not only did not increase the risk of knee replacement, but also significantly reduced the risk of joint replacement in KOA patients within 5 years. Similarly, Lo et al38 believed that for KOA patients aged 50 years and above, walking exercise reduced the frequency of knee joint pain and had an effect on improving the disease, so they encouraged these patients to take walking exercise to alleviate their burdens. Additionally, another study39 suggests that walking can not only relieve joint pain in OA patients, but also improve their quality of life. As discovered by Bell et al,40 walking significantly increased the physical activity level of KOA patients in a short period of time. This type of exercise may be the simple and effective intervention that can be used to improve various symptoms and quality of life of KOA patients. According to Fenton et al,41 KOA patients or high-risk individuals should maintain the moderate to high intensity (more than 100 steps per minute) when walking, so as to reduce the risk of developing a critical slow gait speed. Collectively, these studies indicate that walking is mainly applied in the treatment and prevention of KOA, but there is a lack of the same argument for its effect on HOA.
The mechanisms by which walking as a physical activity can reduce the incidence of KOA are diverse, which are generally considered to be related to the following points. First, walking is a low-intensity exercise that can help reduce weight and lower the load on joints.42 Body weight (body mass index (BMI) ≥ 30 Kg/m2) is one of the main factors affecting joint load, and overweight can increase joint load, and accelerate the wear and tear of articular cartilage and the formation of osteophytes.6,43,44 Weight loss is found to effectively reduce pain and mobility impairment in KOA patients.38,45 Second, walking can help improve fluid circulation in the joint, thereby increasing the supply of nutrients to articular cartilage and synovial fluid, and enhancing the self-repair function of the joint cartilage and synovium.46 Third, walking can promote the increase in muscle strength and improve the physical function.47 As reported in some studies, walking can promote the increase in muscle strength, improve physical activity ability, and reduce joint stress and damage.48,49 Therefore, it is believed that walking as a physical activity can have positive effects on KOA patients from multiple perspectives.
This study conducted a correlation analysis of walking and OA using two-sample Mendelian randomization. It has several advantages. Firstly, as an MR analysis, this study avoided the ethical limitations of clinical research. Secondly, the use of a large number of participants in the GWAS provided a high level of credibility for our research. Lastly, in the selection of SNPs, strict screening criteria were applied, and SNPs related to confounding factors were removed.
Nonetheless, certain limitations should be noted in this study, despite its implications for clinical practice. First, The MR analysis method used in this study relied on genetic variation, and it only reflected its effects at the population level, but did not consider the impact of individual differences. Second, the data used in this study are from European populations, and while the application is highly adapted to European populations, caution should be exercised in applying it to other populations such as Asian and American. We will closely monitor the publication of GWAS data related to other populations to supplement the study of walking and OA in other populations as soon as possible. Third, the GWAS data has its own limitations, such as the inability to perform stratified analysis based on demographic variables like gender and age, which is a common limitation in many MR analyses and not unique to this study.50,51 Additionally, due to the limitations of the GWAS data, it only focuses on walking activity in the past 4 weeks and does not provide detailed descriptions of walking speed, distance, duration, and stride, making it difficult to apply comprehensively. We will continue to monitor updates to the relevant data in order to improve the study as soon as possible. Lastly, OA is a disease caused by multiple factors. This study utilized only considered the influence of a single genetic variation on the relationship between walking and OA, rather than the joint effects of multiple genetic variations. At the same time, there are many factors that can lead to OA, and clinical applications should also focus on other factors.
Conclusion
From genetic studies, types of physical activity in last 4 weeks: Walking for pleasure (not as a means of transport) can reduce the risk of KOA occurrence, but in this study, it did not have a significant impact on HOA.
Data Sharing Statement
Summary statistics for the genetic associations with OA GWAS were obtained from EBI, and the walking GWAS obtained from UKB.
Acknowledgments
We would like to sincerely thank the original GWASs and the related consortiums for sharing and managing the summary statistics.
Funding
This work was supported by grants from Tianjin Municipal Commission of Education and Science (2021ZD013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
2. Yao Q, Wu X, Tao C, et al. Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther. 2023;8(1):56. doi:10.1038/s41392-023-01330-w
3. Motta F, Barone E, Sica A, Selmi C. Inflammaging and osteoarthritis. Clin Rev Allergy Immunol. 2023;64(2):222–238. doi:10.1007/s12016-022-08941-1
4. Pettenuzzo S, Arduino A, Belluzzi E, et al. Biomechanics of chondrocytes and chondrons in healthy conditions and osteoarthritis: a review of the mechanical characterisations at the microscale. Biomedicines. 2023;11(7):1942. doi:10.3390/biomedicines11071942
5. Fontanella CG, Belluzzi E, Pozzuoli A, et al. Exploring anatomo-morphometric characteristics of infrapatellar, suprapatellar fat pad, and knee ligaments in osteoarthritis compared to post-traumatic lesions. Biomedicines. 2022;10(6):1369. doi:10.3390/biomedicines10061369
6. Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. doi:10.1001/jama.2020.22171
7. Abramoff B, Caldera FE. Osteoarthritis: pathology, diagnosis, and treatment options. Med Clin North Am. 2020;104(2):293–311. doi:10.1016/j.mcna.2019.10.007
8. Murphy LB, Cisternas MG, Pasta DJ, Helmick CG, Yelin EH. Medical expenditures and earnings losses among US adults with arthritis in 2013. Arthritis Care Res. 2018;70(6):869–876. doi:10.1002/acr.23425
9. Yue L, Berman J. What is osteoarthritis? JAMA. 2022;327(13):1300. doi:10.1001/jama.2022.1980
10. Chang KW, Lin CM, Yen CW, Yang CC, Tanaka T, Guo LY. The effect of walking backward on a treadmill on balance, speed of walking and cardiopulmonary fitness for patients with chronic stroke: a pilot study. Int J Environ Res Public Health. 2021;18(5):2376. doi:10.3390/ijerph18052376
11. Moghetti P, Balducci S, Guidetti L, et al. Walking for subjects with type 2 diabetes: a systematic review and joint AMD/SID/SISMES evidence-based practical guideline. Nutr Metab Cardiovasc Dis. 2020;30(11):1882–1898. doi:10.1016/j.numecd.2020.08.021
12. Bai X, Soh KG, Omar Dev RD, Talib O, Xiao W, Cai H. Effect of brisk walking on health-related physical fitness balance and life satisfaction among the elderly: a systematic review. Front Public Health. 2022;9:829367. doi:10.3389/fpubh.2021.829367
13. Hall KS, Hyde ET, Bassett DR, et al. Systematic review of the prospective association of daily step counts with risk of mortality, cardiovascular disease, and dysglycemia. Int J Behav Nutr Phys Act. 2020;17(1):78. doi:10.1186/s12966-020-00978-9
14. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
15. de Leeuw C, Savage J, Bucur IG, Heskes T, Posthuma D. Understanding the assumptions underlying Mendelian randomization. Eur J Hum Genet. 2022;30(6):653–660. doi:10.1038/s41431-022-01038-5
16. Birney E. Mendelian randomization. Cold Spring Harb Perspect Med. 2022;12(4):a041302. doi:10.1101/cshperspect.a041302
17. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization. The STROBE-MR statement JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
18. Boehm FJ, Zhou X. Statistical methods for Mendelian randomization in genome-wide association studies: a review. Comput Struct Biotechnol J. 2022;20:2338–2351. doi:10.1016/j.csbj.2022.05.015
19. Li J, Li C, Huang Y, et al. Mendelian randomization analyses in ocular disease: a powerful approach to causal inference with human genetic data. J Transl Med. 2022;20(1):621. doi:10.1186/s12967-022-03822-9
20. Zheng J, Ni C, Zhang Y, et al. Association of regular glucosamine use with incident dementia: evidence from a longitudinal cohort and Mendelian randomization study. BMC Med. 2023;21(1):114. doi:10.1186/s12916-023-02816-8
21. Cao Z, Wu Y, Li Q, Li Y, Wu J. A causal relationship between childhood obesity and risk of osteoarthritis: results from a two-sample Mendelian randomization analysis. Ann Med. 2022;54(1):1636–1645. doi:10.1080/07853890.2022.2085883
22. Bycroft C, Freeman C, Petkova D, et al. The UK biobank resource with deep phenotyping and genomic data. Nature. 2018;562(7726):203–209. doi:10.1038/s41586-018-0579-z
23. Tachmazidou I, Hatzikotoulas K, Southam L, et al. Identification of new therapeutic targets for osteoarthritis through genome-wide analyses of UK Biobank data. Nat Genet. 2019;51(2):230–236. doi:10.1038/s41588-018-0327-1
24. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
25. Chen S, Chen T, Chen Y, Huang D, Pan Y, Chen S. Causal association between tea consumption and bone health: a Mendelian randomization study. Front Nutr. 2022;9:872451. doi:10.3389/fnut.2022.872451
26. Wang Z, Kang C, Xu P, et al. Osteoarthritis and cardiovascular disease: a Mendelian randomization study. Front Cardiovasc Med. 2022;9:1025063. doi:10.3389/fcvm.2022.1025063
27. Cui Z, Feng H, He B, Xing Y, Liu Z, Tian Y. Type 2 diabetes and glycemic traits are not causal factors of osteoarthritis: a two-sample Mendelian randomization analysis. Front Genet. 2021;11:597876. doi:10.3389/fgene.2020.597876
28. Zhang L, Zhang W, Wu X, et al. A sex- and site-specific relationship between body mass index and osteoarthritis: evidence from observational and genetic analyses [published online ahead of print, 2023 Mar 6]. Osteoarthritis Cartilage. 2023;S1063-4584(23):00697. doi:10.1016/j.joca.2023.02.073
29. Funck-Brentano T, Nethander M, Movérare-Skrtic S, Richette P, Ohlsson C. Causal factors for knee, hip, and hand osteoarthritis: a Mendelian randomization study in the UK biobank. Arthritis Rheumatol. 2019;71(10):1634–1641. doi:10.1002/art.40928
30. Fan J, Zhu J, Sun L, Li Y, Wang T, Li Y. Causal association of adipokines with osteoarthritis: a Mendelian randomization study. Rheumatology. 2021;60(6):2808–2815. doi:10.1093/rheumatology/keaa719
31. Hemani G, Zheng J, Elsworth B, et al. The MR-base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408. doi:10.7554/eLife.34408
32. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases [published correction appears in Nat Genet. 201850(8):1196]. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
33. Hemani G, Bowden J, Davey Smith G. Evaluating the potential role of pleiotropy in Mendelian randomization studies. Hum Mol Genet. 2018;27(R2):R195–R208. doi:10.1093/hmg/ddy163
34. Huang D, Lin S, He J, Wang Q, Zhan Y. Association between COVID-19 and telomere length: a bidirectional Mendelian randomization study. J Med Virol. 2022;94(11):5345–5353. doi:10.1002/jmv.28008
35. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method [published correction appears in Eur J Epidemiol. 2017 Jun 29]. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
36. Miao R, Li J, Meng C, et al. Diet-derived circulating antioxidants and risk of stroke: a mendelian randomization study. Oxid Med Cell Longev. 2022;2022:6457318. doi:10.1155/2022/6457318
37. Master H, Thoma LM, Neogi T, et al. Daily walking and the risk of knee replacement over 5 years among adults with advanced knee osteoarthritis in the United States. Arch Phys Med Rehabil. 2021;102(10):1888–1894. doi:10.1016/j.apmr.2021.05.014
38. Lo GH, Vinod S, Richard MJ, et al. Association between walking for exercise and symptomatic and structural progression in individuals with knee osteoarthritis: data from the osteoarthritis initiative cohort. Arthritis Rheumatol. 2022;74(10):1660–1667. doi:10.1002/art.42241
39. Exercise is essential for osteoarthritis: the many benefits of physical activity. J Orthop Sports Phys Ther. 2018;48(6):448. doi:10.2519/jospt.2018.0507
40. Bell EC, Wallis JA, Goff AJ, Crossley KM, O’Halloran P, Barton CJ. Does land-based exercise-therapy improve physical activity in people with knee osteoarthritis? A systematic review with meta-analyses. Osteoarthritis Cartilage. 2022;30(11):1420–1433. doi:10.1016/j.joca.2022.07.008
41. Fenton SAM, Neogi T, Dunlop D, et al. Does the intensity of daily walking matter for protecting against the development of a slow gait speed in people with or at high risk of knee osteoarthritis? An observational study. Osteoarthritis Cartilage. 2018;26(9):1181–1189. doi:10.1016/j.joca.2018.04.015
42. Mabire L, Mani R, Liu L, Mulligan H, Baxter D. The Influence of age, sex and body mass index on the effectiveness of brisk walking for obesity management in adults: a systematic review and meta-analysis. J Phys Act Health. 2017;14(5):389–407. doi:10.1123/jpah.2016-0064
43. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022;30(2):184–195. doi:10.1016/j.joca.2021.04.020
44. Horn DB, Damsgaard C, Earles K, Mathew S, Nelson AE. Engagement between patients with obesity and osteoarthritis and primary care physicians: a cross-sectional survey. Postgrad Med. 2021;133(8):979–987. doi:10.1080/00325481.2021.1982588
45. Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2007;66(4):433–439. doi:10.1136/ard.2006.065904
46. Lambova S. Exercise programmes for osteoarthritis with different localization. Curr Rheumatol Rev. 2018;14(2):123–130. doi:10.2174/1573397113666170810153808
47. Alghadir AH, Anwer S, Sarkar B, Paul AK, Anwar D. Effect of 6-week retro or forward walking program on pain, functional disability, quadriceps muscle strength, and performance in individuals with knee osteoarthritis: a randomized controlled trial (retro-walking trial). BMC Musculoskelet Disord. 2019;20(1):159. doi:10.1186/s12891-019-2537-9
48. Hall M, Hinman RS, Wrigley TV, Kasza J, Lim BW, Bennell KL. Knee extensor strength gains mediate symptom improvement in knee osteoarthritis: secondary analysis of a randomised controlled trial. Osteoarthritis Cartilage. 2018;26(4):495–500. doi:10.1016/j.joca.2018.01.018
49. Liang J, Lang S, Zheng Y, et al. The effect of anti-gravity treadmill training for knee osteoarthritis rehabilitation on joint pain, gait, and EMG: case report. Medicine. 2019;98(18):e15386. doi:10.1097/MD.0000000000015386
50. Qiu P, Wu J, Kui L, Chen M, Lv S, Zhang Z. Causal effects of walking pace on osteoarthritis: a two-sample Mendelian randomization study. Front Genet. 2023;14:1266158. doi:10.3389/fgene.2023.1266158
51. Xu Z, Wu X, Xiao C, et al. Observational and genetic analyses of the bidirectional relationship between depression and hypertension. J Affect Disord. 2023. doi:10.1016/j.jad.2023.12.028
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.