")
Back to Journals » Journal of Pain Research » Volume 17
Effectiveness of Different Noninvasive Physiotherapy in Relieving Postlaparoscopic Shoulder pain: A Protocol for Systematic Review and Network Meta-Analysis
Received 7 December 2023
Accepted for publication 2 April 2024
Published 24 April 2024 Volume 2024:17 Pages 1555—1561
DOI https://doi.org/10.2147/JPR.S453767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Hefeng Tian, Haiou Qi
Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Haiou Qi, Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Background: Shoulder pain is one of the most common symptoms after laparoscopic surgery, which seriously affects people’s health and quality of life. Many clinical studies have shown that noninvasive physiotherapy is the most beneficial treatment for patients, but the best approach for various noninvasive physiotherapy is unclear. The purpose of this study protocol is to compare the effectiveness of different noninvasive physiotherapy in relieving postlaparoscopic shoulder pain (PLSP).
Methods: We will search ten electronic databases including PubMed, Web of Science, Medline, Scopus, CINAHL, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), CNKI, WanFang Data and VIP databases from their inception to November 2023. We will select randomized controlled trials (RCTs) to evaluate the effectiveness of noninvasive physiotherapy on PLSP. Our primary outcome will be to measure the intensity of shoulder pain at 24 and 48 hours after the end of the noninvasive intervention in the included study. Secondary outcomes include incidence of shoulder pain at 24 and 48 hours, postoperative nausea / vomiting and incidence of other complications after noninvasive intervention. Then, standard network meta-analysis will be conducted using Review Manager 5.4 and STATA 18.
Results: Our systematic review and network meta-analysis will identify the best noninvasive physiotherapy for PLSP patients.
Conclusion: This systematic review will address the existing knowledge gap regarding best practice for relieving PLSP with noninvasive physiotherapy. The results of this network meta-analysis will help medical staff and patients choose the best method to relieve the PLSP. Furthermore, we hope that the results of this study will provide evidence-based for the improvement of guidelines and facilitate the decision sharing process.
Systematic review registration: PROSPERO CRD42023481829.
Keywords: physiotherapy, shoulder pain, protocol, systematic review, network meta-analysis
Introduction
The use of laparoscopic technology in clinical practice has increased significantly and has been characterized by an increasing emphasis on minimally invasive techniques. Compared with traditional open surgery, its small trauma, less bleeding and fast recovery have become the recognized advantages, and laparoscopic surgery is a reliable alternative to open surgery.1 Despite these advantages, laparoscopic surgery still brings common shoulder pain to patients. According to statistical survey, the incidence of postoperative laparoscopic shoulder pain in cholecystectomy, appendectomy, diagnostic laparoscopic surgery and adjustable gastric band surgery is 35%~80%,2,3 and this relatively high morbidity is a challenging problem.4 Sometimes, the extent of this postlaparoscopic shoulder pain exceeds the pain caused by the incision site. Severe symptoms may lead to prolonged discharge and readmission with additional medical expenses and seriously affecting the physical and mental health and quality of life.5
The underlying pathogenesis of PLSP is uncertain, but the earliest previous studies have shown that the acidic environment produced by the residual abdominal carbon dioxide dissolved in the abdominal fluid, which subsequently stimulates the diaphragm, reflexively causes shoulder pain.6–8 In a subsequent period of time, some researchers have proposed another theory that carbon dioxide gas enters the abdominal cavity, leading to overstretching of the fibers in the diaphragm, resulting in complete occlusion of the intraneural vessels and complete nerve ischemia, causing partial vascular tear and traumatic nerve pulling.9,10 This factor causes stimulation of the phrenic nerve located on the peritoneum, leading in reflex shoulder pain. Numerous studies suggest that the pathogenesis of PLSP is complex. Currently, these mechanisms are all thought to be factors contributing to PLSP.
At present, the treatment goal of PLSP is mainly to relieve the symptoms, and it is difficult to achieve a complete cure. Clinically common treatments include drug therapy and nerve block therapy. Common analgesic drugs are lidocaine,1 duloxetine,11 and clonidine,12 ropivacaine13 and parecoxib sodium.14 Nerve block therapy is the most basic treatment modality for pain diseases. For some patients with neurologic disorders, invasive nerve block therapy is often used for treatment, such as phrenic nerve block,15,16 stellate ganglion block,17,18 cervical plexus block, suprascapular nerve block19 and plane block of erector spinal muscles.20,21 Invasive nerve therapy is more traumatic and expensive, and improper operation will also cause nerve damage, vascular damage and some sequelae. In recent years, many noninvasive physiotherapy gradually appear in clinical treatment, such as transcutaneous electrical nerve stimulation (TENS), acupuncture and massage.
As the most commonly used noninvasive and inexpensive neuromodulation physiotherapy, TENS provides alternating current through skin electrodes to activate large-diameter afferent fibers (A-beta fibers) of the nervous system, thus reducing pain neurotransmission in the spinal cord.22 Acupuncture points will make local tissues produce acid, swelling and numbness. The signals caused by acupuncture will be transmitted to the peripheral or central parts (various limbic structures, such as hypothalamus, amygdala, cerebellum and hippocampus) of the brain so as to achieve analgesic effect.23,24 Unlike TENS and manual acupuncture, massage is the operation of soft tissue throughout the body to improve overall health, such as eliminating fatigue, enhancing physical fitness and anti-aging.25 Furthermore, there are also some physical activity (like deep breathing, walking or moderate exercise activities), psychological / psychiatric treatments (like imagery, praying, visualization or meditation)26–28 as well as distractions (like listening to music or watching TV).29,30 Although many studies have confirmed their effectiveness, the advantages and disadvantages of different noninvasive physiotherapy have rarely been found. Therefore, this study aims to evaluate the effectiveness of different noninvasive physiotherapy interventions and to identify the most effective way to improve PLSP by a systematic review and network meta-analysis (NMA). This will largely help to reduce patients’ healthcare costs, improve patients’ postoperative comfort and raise patients’ satisfaction with medical treatment.
Methods and Design
We will conduct a systematic review of randomized controlled trials reporting the incidence and potential determinants of postoperative shoulder pain after laparoscopy. Our review design follows the methodological recommendations for the systematic review of interventions in the Cochrane Handbook31 and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.32 If any program situation requiring adjustment is encountered throughout the study period, we will correct and update them in the final systematic review and NMA report. The protocol for this review has been registered on the PROSPERO International Prospective Register of Systematic Reviews (CRD42023481829).
Eligibility Criteria
The eligibility criteria for this study will be implemented following the population, interventions, comparison, outcomes and study design (PICOS) approach.
Study Design
Only randomized controlled trials (RCTs) of PLSP related to noninvasive physiotherapy intervention were included. There are no restrictions on language. The corresponding study will be excluded if these conditions are present.
Population
Our population of interest is adults over 18 years who had undergone laparoscopic surgery with postoperative shoulder pain. There are no restrictions on the type of laparoscopic surgery performed. Such studies are excluded if a patient is forced to switch from laparoscopic surgery to open surgery midway through the procedure. Studies involving patients with psychological disorders or mental disorders are not included in this study. Similarly, studies in patients with other substantial physical conditions that affect the surgery will also be excluded.
Interventions
The experimental group used noninvasive treatment based on conventional treatment (postoperative observation, health education, dietary guidance, complication prevention and psychological intervention). If the control group implemented a noninvasive treatment, the experimental group received a combination of multiple noninvasive treatments, and whether we exclude these trials, we need to judge based on the specific situation of the analysis problem and refer to the inclusion criteria, quality assessment, consistency analysis and other aspects of information. It is best for experts in the field to discuss them together to make the most accurate and scientific decisions. Eligible noninvasive physiotherapy mainly includes the following types, such as physical therapies (acupuncture, TENS, hot or cold package), physical activities (deep breathing, walking or light to moderate sportive activities), psychological / psychiatric therapies (imagery, praying, visualization, meditation, relaxation, listening to music, talking to people or watching TV), massage / Tuina (soft tissue massage and acupressure), multidisciplinary rehabilitation (physical therapy and psychological / psychiatric therapy, physical activity + psychological / psychiatric therapies + massage / Tuina).
Comparison
The control group received the conventional treatment (including placebo, usual care or no intervention). Conventional treatment generally includes postoperative condition observation, health education, dietary guidance, complication prevention, psychological intervention and so on.
Outcomes
Our primary outcome will be to measure the intensity of shoulder pain at different time points after the end of the noninvasive intervention in the included study. The type of assessment instrument is selected by the most recognized Visual Analogue Score (VAS). The degree of pain from low to high is 0 to 10 points. Higher ratings will indicate more severe pain levels. The score is based on the pain when the patient lying still. The degree of shoulder pain is assessed at 24 and 48 hours after the noninvasive intervention. Secondary outcomes include the incidence of shoulder pain, nausea / vomiting and other complications at 24 and 48 hours after noninvasive intervention.
Search Strategies
To identify potential eligible studies, we searched a series of literature, mainly from ten electronic databases including PubMed, Web of Science, Medline, Scopus, CINAHL, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), CNKI, WanFang Data and VIP databases from their inception to November 2023. In order to ensure the comprehensiveness of the literature search, the search strategy adopted the combination of truncated words, free words and subject words, and adjusted the search words appropriately according to the search results. Truncation included “laparoscop*”, free word included “RCT”, and subject words included “shoulder”, “pain” and “randomized controlled trial”. Then, two investigators cross-browsed and examine the references of the selected studies to find other eligible studies. We conducted a search of three clinical trial registries (World Health Organization, the Clinical Trials.gov and the International Clinical Trials Registry Platform) to identify ongoing experiments. Meanwhile, we searched the grey literature in OpenGrey (http://www.opengrey.eu/) to avoid omission.
Study Selection
After the literature search, the summary results of the ten databases were imported into Endnote X9 software. Duplicate studies were automatically retrieved and removed. Two investigators will independently screen all potentially eligible literature according following the inclusion and exclusion criteria to make a preliminary choice. Thereafter, the full text deemed potentially eligible for the study will be independently assessed by two investigators. The study selection process is performed independently by two authors and the results are cross-checked. If there is a disagreement, the two authors will settle it through negotiation, and if there is still a disagreement, the third author is need to help the ruling. The flowchart of the study selection is shown in Figure 1.
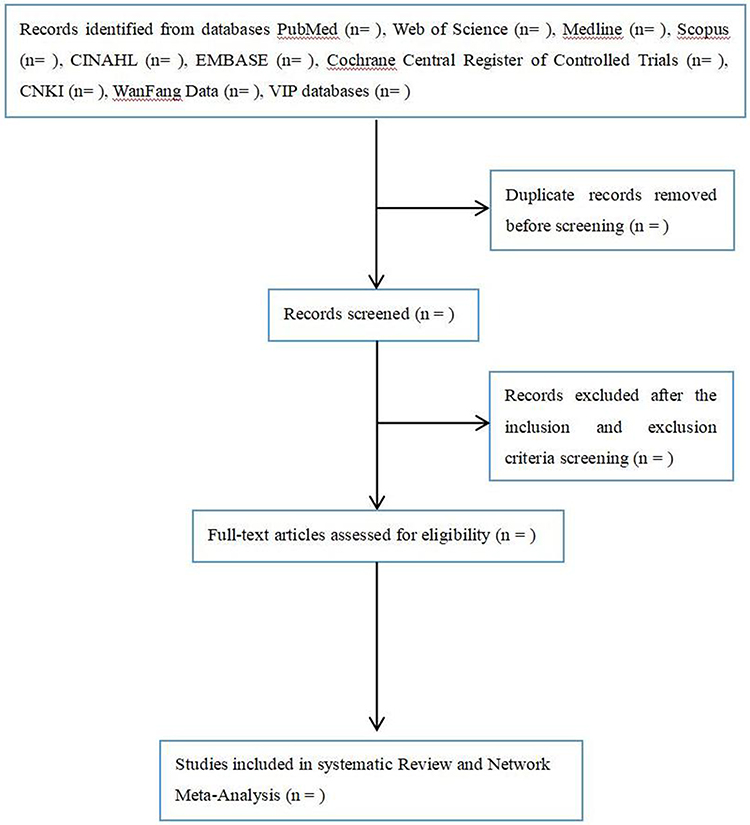 |
Figure 1 Flowchart of study selection. |
Data Extraction
Data extraction will be performed independently by two investigators. Then a data comparison will be made, and if there is a disagreement, it will be negotiated by a third party. Data extraction was performed using Excel software, mainly including the basic characteristics of the studies included in the literature (year of publication, first author, country, sample size, etc.), participant characteristics (surgery type, population type, etc.), interventions (method, intensity, frequency, duration, follow-up time, etc.), outcome indicators (intensity and incidence of shoulder pain at different time periods, incidence of nausea / vomiting and other complications, etc.) (Table 1). If the relevant study data is missing, we will contact the first author or the corresponding author of the original study to ensure data integrity. If no reply is received from the authors of the original study, we can only regret to exclude this study.33
 |
Table 1 Basic characteristics of the included studies |
Risk of Bias Assessment
Statistical Analysis
First, we will give a narrative overview of all the interventions and outcomes included in this study. Then conventional pairwise meta-analyses will be performed using Review Manager 5.4 and network plot will be performed using STATA 18 software. In the conventional meta-analysis process, the continuity variables were expressed by the weighted mean difference (WMD), standardized mean difference (SMD) and 95% confidence interval (CI). When the methods or units of measurement for the same intervention are exactly the same, WMD should be chosen. When different measures or units are used for the same intervention, SMD should be selected as the combined statistic. We also choose to use SMD when the results are measured on different scales or when the means differences between different studies are too large. We rigorously assess the clinical and methodological heterogeneity by examining the characteristics of the included studies. Our included studies score ≥ 4 on the improved Jadad scale, as these related studies can be considered of high methodological quality and sufficient similarity in clinical characteristics. Heterogeneity between different studies will be assessed by I2 and P value. If the P value is > 0.1 and I2 < 50%, indicating low heterogeneity between studies, a meta-analysis will be performed using a fixed-effect model. The random-effects model can also be used because the results of the random-effects model are more conservative than the fixed-effects model. Secondly, the smaller the statistical heterogeneity, the results of the random-effects model are closer to the results of the fixed-effects model. If the P value is ≤ 0.1 and I2 ≥ 50%, indicating high heterogeneity between studies, sensitivity analysis and subgroup analysis will be used to explore the source of heterogeneity and random-effects model will be used to draw forest plot and funnel plot to evaluate publication bias. The funnel plot method of Begg’s and Egger’s will be used to detect publication bias, where allowed. The NMA includes drawing the network plot for the data, area under the curve and league table The network plot will be used to analyze which interventions can be directly compared in the included studies and how the indirect interventions are presented. In the network plot, the large and small nodes represent the large and small sample sizes focused on the intervention. The connection between nodes represents a direct comparison between studies. The wider the connected lines, the more studies showing focus on comparison. We will assess the potential transitivity issues of the NMA with two approaches. First, we will examine the distribution of effect modifiers of the interventions across studies, such as gender, age, marital status, body mass index, educational level, surgical history as well as pain assessment tools, to make sure that no significant differences exist in these factors. Second, we will carry out a test of inconsistency to determine whether there is statistical evidence of overall inconsistency. The need for an inconsistency test is evaluated by assessing the presence of closed rings in the network plot. In the presence of a closed loop, the inconsistency between direct comparison and indirect comparison is judged by the node splitting values (P value). Although the multi-arm trials can form a closed loop structure, there is no inconsistency, so there is no need to detect. The relevant data of the target intervention should be extracted for the analysis.
The Bayesian NMA will be performed using the GeMTC package of R software and the Markov chain Monte Carlo method with 10000burn-ins and 100000iterations. The probability plots will be plotted for the probability ranking. We will use the potential scale reduction factor (PSRF) to evaluate the convergence of the results. When PSRF tends to 1 and reaches stability, the convergence of the model is satisfactory. Finally, we used the surface under the cumulative ranking curve (SUCRA) to rank the effects of different noninvasive therapies in relieving postlaparoscopic shoulder pain. The range of SUCRA is 0 to 1. When SUCRA is 1, this suggests that the intervention is absolutely effective. When SUCRA is 0, this suggests that the intervention is absolutely ineffective. The larger the SUCRA value, the better the intervention effect.
Discussion
The PLSP is an easily overlooked but not uncommon postoperative complaint. This symptom causes additional physical discomfort and pain in the postoperative recovery period, which also causes significant psychological and mental burden and reduces the postoperative satisfaction of patients. Regardless of its clinical importance, although the occurrence of PLSP has gradually attracted the attention of clinicians, there is a lack of adequate prevention and treatment in the actual clinical work. In general, the current treatment for PLSP focuses on the administration of analgesics, including opioids and various invasive techniques. The invasive techniques involved are epidural analgesia, placement of a nerve catheter around the phrenic nerve of the neck and ultrasound-guided injection of analgesics into the phrenic nerve of the neck. However, these interventions may cause diaphragmatic paralysis and an underlying movement impairment of the shoulder muscles. Therefore, in this study, we will investigate clinical trial studies related to noninvasive treatment methods for relieving PLSP. To a large extent, our study will facilitate clinical evidence-based treatment decisions and fill the evidence gap that disturbs patients in PLSP management.
To the best of our knowledge, this is the first systematic review and NMA to compare the effectiveness of different noninvasive physiotherapy in relieving PLSP. This systematic review will address the existing knowledge gap regarding best practice for relieving PLSP with noninvasive physiotherapy. An NMA approach to evidence synthesis will be used to evaluate trials of different noninvasive physiotherapy to better identify strategies that improve shoulder pain outcomes and cause minimal harm. Noninvasive physiotherapy can not only provide cost-effective treatment options for patients, but also provide therapeutic ideas for clinicians. This approach is relatively novel and will provide a comparison of multiple interventions for more medical staff. We believe that the results of this NMA will help medical staff and patients choose the best method to relieve the PLSP. Furthermore, we also hope that the results of this study will provide evidence-based for the improvement of guidelines and facilitate the decision sharing process.
Data Sharing Statement
Data available on request from the authors.
Funding
No funds were received to conduct this study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kim HY, Choi JB, Min SK, et al. A randomized clinical trial on the effect of a lidocaine patch on shoulder pain relief in laparoscopic cholecystectomy. Sci Rep. 2021;11(1):1052.
2. Cunniffe MG, Mcanena OJ, Dar MA, et al. A prospective randomized trial of intraoperative bupivacaine irrigation for management of shoulder-tip pain following laparoscopy. Am J Surg. 1998;176(3):258–261. doi:10.1016/S0002-9610(98)00150-0
3. Dixon JB, Reuben Y, Halket C, et al. Shoulder pain is a common problem following laparoscopic adjustable gastric band surgery. Obes Surg. 2005;15(8):1111–1117. doi:10.1381/0960892055002149
4. Li XY, Tian M, Li AZ, et al. The risk of shoulder pain after laparoscopic surgery for infertility is higher in thin patients. Sci Rep. 2021;11(1):13421.
5. Meng D, Mao YF, Song QM, et al. Efficacy and safety of Transcutaneous Electrical Acupoint Stimulation (TEAS) for postoperative pain in laparoscopy: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:1–17. doi:10.1155/2022/9922879
6. Riedel HH, Semm K. The post-laparoscopic pain syndrome (author’s syndrome). Geburtshilfe Frauenheilkd. 1980;40(7):635–643. doi:10.1055/s-2008-1037224
7. Alexander JI, Hull MG. Abdominal pain after laparoscopy: the value of a gas drain. Br J Obstet Gynaecol. 1987;94(3):267–269. doi:10.1111/j.1471-0528.1987.tb02366.x
8. Joris J, Cigarini I, Legrand M, et al. Metabolic and respiratory changes after cholecystectomy performed via laparotomy or laparoscopy. Br J Anaesth. 1992;69(4):341–345. doi:10.1093/bja/69.4.341
9. Schoeffler P, Diemunsch P, Fourgeaud L. Ambulatory celioscopy. Cah Anesthesiol. 1993;41(4):385–391.
10. Reuben SS, Buvanendran A. Preventing the development of chronic pain after orthopaedic surgery with preventive multimodal analgesic techniques. J Bone Joint Surgery-Am Volume. 2007;89A(6):1343–1358. doi:10.2106/JBJS.F.00906
11. Abo Elfadl GM, Osman AM, Ghalyoom MF, et al. Preoperative duloxetine to prevent postoperative shoulder pain after gynecologic laparoscopy: a randomized controlled trial. Braz J Anesthesiol. 2022.
12. Mirhosseini H, Avazbakhsh MH, Hosseini Amiri M, et al. Effect of oral clonidine on shoulder tip pain and hemodynamic response after laparoscopic cholecystectomy: a randomized double blind study. Reg Anesth Pain Med. 2017;7(6):e61669. doi:10.5812/aapm.61669
13. Saccardi C, Gizzo S, Vitagliano A, et al. Peri-incisional and intraperitoneal ropivacaine administration: a new effective tool in pain control after laparoscopic surgery in gynecology: a randomized controlled clinical trial. Surg Endosc. 2016;30(12):5310–5318. doi:10.1007/s00464-016-4881-2
14. Zhang H, Liu X, Jiang H, et al. Parecoxib increases muscle pain threshold and relieves shoulder pain after gynecologic laparoscopy: a randomized controlled trial. J Pain Res. 2016;9:653–660. doi:10.2147/JPR.S115889
15. Dogan R, Sahin D, Isbilen C. Laparoscopic cholecystectomy under spinal anesthesia with right phrenic nerve block. Acta Anaesthesiol Scand. 2008;52(3):445–446. doi:10.1111/j.1399-6576.2007.01512.x
16. Yi MS, Kim WJ, Kim MK, et al. Effect of ultrasound-guided phrenic nerve block on shoulder pain after laparoscopic cholecystectomy-a prospective, randomized controlled trial. Surg Endosc. 2017;31(9):3637–3645. doi:10.1007/s00464-016-5398-4
17. Mcdonnell JG, Finnerty O, Laffey JG. Stellate ganglion blockade for analgesia following upper limb surgery. Anaesthesia. 2011;66(7):611–614. doi:10.1111/j.1365-2044.2011.06626.x
18. Kakazu CZ, Julka I. Stellate ganglion blockade for acute postoperative upper extremity. Anesthesiology. 2005;102(6):1288–1289. doi:10.1097/00000542-200506000-00039
19. Abdallah FW, Wijeysundera DN, LAUPACIS A, et al. Subomohyoid anterior suprascapular block versus interscalene block for arthroscopic shoulder surgery a multicenter randomized trial. Anesthesiology. 2020;132(4):839–853. doi:10.1097/ALN.0000000000003132
20. Chin KJ, Adhikary S, Sarwani N, et al. The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72(4):452–460. doi:10.1111/anae.13814
21. Cesur S, Yorukoglu HU, Aksu C, et al. Bilateral versus unilateral erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a randomized controlled study. Braz J Anesthesiol. 2023;73(1):72–77. doi:10.1016/j.bjane.2021.04.020
22. Visconti MJ, Haidari W, Feldman SR. Transcutaneous electrical nerve stimulation (TENS): a review of applications in dermatology. J Dermatological Treat. 2020;31(8):846–849. doi:10.1080/09546634.2019.1657227
23. He Y, Miao F, Fan Y, et al. Acupuncture methods for piriformis syndrome: a protocol for systematic review and network meta. J Pain Res. 2023;16:2357–2364. doi:10.2147/JPR.S417211
24. Tian H, Qi H, Xu X, et al. Research hotspots and trends in postlaparoscopic shoulder pain from 2003 to 2023: a bibliometric analysis. Heliyon. 2024;10(4):e25846–e. doi:10.1016/j.heliyon.2024.e25846
25. Field T. Massage therapy. Med Clin North Am. 2002;86(1):163–+. doi:10.1016/S0025-7125(03)00078-6
26. Jegindo E-ME, Vase L, Skewes JC, et al. Expectations contribute to reduced pain levels during prayer in highly religious participants. J Behav Med. 2013;36(4):413–426. doi:10.1007/s10865-012-9438-9
27. Thomas KM, Sethares KA. Is guided imagery effective in reducing pain and anxiety in the postoperative total joint arthroplasty patient? Orthop Nurs. 2010;29(6):393–399. doi:10.1097/NOR.0b013e3181f837f0
28. Zeidan F, Martucci KT, Kraft RA, et al. Brain mechanisms supporting the modulation of pain by mindfulness meditation. J Neurosci. 2011;31(14):5540–5548. doi:10.1523/JNEUROSCI.5791-10.2011
29. Buhle JT, Stevens BL, Friedman JJ, et al. Distraction and placebo: two separate routes to pain control. Psychol Sci. 2012;23(3):246–253. doi:10.1177/0956797611427919
30. Hole J, Hirsch M, Ball E, et al. Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis. Lancet. 2015;386(10004):1659–1671. doi:10.1016/S0140-6736(15)60169-6
31. Nasser M. Cochrane handbook for systematic reviews of interventions. Am J Public Health. 2020;110(6):753–754. doi:10.2105/AJPH.2020.305609
32. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (vol 8, pg 336, 2010). Int j Surg. 2010;8(8):336–341. doi:10.1016/j.ijsu.2010.02.007
33. Wu T, Fu Y, Song HX, et al. Effectiveness of botulinum toxin for shoulder pain treatment: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2015;96(12):2214–2220. doi:10.1016/j.apmr.2015.06.018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.