")
Back to Journals » Clinical Interventions in Aging » Volume 18
Effects of Yoga and Aerobic Exercise on Verbal Fluency in Physically Inactive Older Adults: Randomized Controlled Trial (FitForAge)
Authors Welford P , Östh J, Hoy S, Rossell SL, Pascoe M, Diwan V, Hallgren M
Received 20 January 2022
Accepted for publication 20 July 2022
Published 30 March 2023 Volume 2023:18 Pages 533—545
DOI https://doi.org/10.2147/CIA.S359185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Nandu Goswami
Paul Welford,1 Josefine Östh,1 Sara Hoy,2 Susan L Rossell,3 Michaela Pascoe,4 Vinod Diwan,1 Mats Hallgren1
1Department of Global Public Health, Karolinska Institutet, Solna, Sweden; 2Swedish School of Sport and Health Sciences (GIH), Stockholm, Sweden; 3Centre for Mental Health, School of Health Sciences, Swinburne University, Melbourne, Victoria, Australia; 4Institute for Health and Sport, Victoria University, Melbourne, Victoria, Australia
Correspondence: Mats Hallgren, Department of Global Public Health, Karolinska Institutet, Level 6, 1e Solnavägen, Solna, 11365, Sweden, Tel +46852480000, Email [email protected]
Purpose: To compare the effects on verbal fluency of a supported yoga-based exercise intervention to an aerobic exercise intervention and a wait-list control group.
Participants and Methods: Eighty-two physically-inactive but otherwise healthy adults (mean age 72.5 years, range 65– 85, 77% female) were recruited into a 12-week, three-group, parallel randomized controlled trial. Participants were supported to complete ≥ 3 Hatha yoga classes per/week or ≥ 3 structured aerobic exercise sessions/week. A wait-list control group continued usual daily activities only. Verbal fluency, including total-FAS, animals, and verbs, was assessed before and after interventions. Group effects were assessed using analysis of covariance (ANCOVA).
Results: Twenty-seven participants were randomized to yoga, 29 to aerobic exercise and 26 to a waitlist. At 12-week follow-up, compared to baseline, there were increases in mean total-FAS in the yoga (+5.0 words, p=0.002) and aerobic exercise groups (+6.6 words, p=0.004). Mean total-FAS in the wait-list control group remained stable (− 0.5 words, p=0.838). There were medium-magnitude estimated treatment effects on total-FAS for yoga versus wait-list control and aerobic exercise versus wait-list control: Hedges’ g=0.51 (p=0.213) and 0.57 (p=0.098) respectively. In addition, small-to-medium magnitude estimated treatment effects were seen on animals and verbs for yoga versus wait-list control and aerobic exercise versus wait-list control: g=0.28 (p=0.155), 0.19 (p=0.766) and 0.50 (p=0.085), 0.59 (p=0.233) respectively.
Conclusion: Participation in yoga or aerobic exercise was associated with estimated improvements in verbal fluency compared to a non-active control group. Yoga and aerobic exercise may be promising approaches by which to promote cognitive function among older adults.
Trial Registration: DRKS00015093, U1111-1217-4248.
Keywords: physical activity, verbal fluency test, executive function, cognitive aging, healthy aging
Introduction
Aging is associated with a gradual decline in cognitive functions, including poorer memory, attention, and verbal fluency.1,2 These changes are often not severe enough to warrant a clinical diagnosis (eg, dementia), but may be noticeable to others and negatively impact self-esteem, autonomy, and life quality.3 Language is one of the most complex functions in humans and is essential for communication and autonomy. Studies on normal aging have shown that some language skills are resilient to age-related declines; comprehension, semantic abilities, and vocabulary remain stable or even improve with age.4,5 By contrast, verbal fluency and naming are among the most vulnerable cognitive functions to aging.6
Aerobic exercise has well established mental health benefits,7 including improved cognitive functioning, and is recommended for older adults.8,9 Despite this, physical inactivity (ie, engaging in <150 minutes of moderate-to-vigorous physical activity/week) is prevalent among older adults, ranging from 5% (Sweden) to 29% (Portugal) in the European Union.10
Musculoskeletal injuries are common impediments to participation in some forms of aerobic exercise (eg, running) and tend to increase with age.11 Yoga is a form of structured physical activity that combines physical postures with breathing and meditative exercises and is shown to be suitable for older adults, including those with mobility problems.12–15 This combination of physical and “mindful” elements distinguishes yoga from conventional aerobic training, and may confer additional mental health benefits.16 Participation in yoga-based exercise is increasing,17 alongside yoga related research.18–20 The reported benefits of yoga include improved mental health (reduced depression and anxiety), sleep, and life quality.21–23 Improvements in cardiovascular fitness, body composition, and blood pressure have also been reported.24–26
Emerging evidence suggests that yoga-based exercise may also improve cognitive functioning in older adults.19,27–29 Three systematic reviews30–32 and a meta-analysis33 each concluded that yoga-based interventions improved executive functions in older adults. A systematic review comparing the effects of three different types of exercise on executive functioning in the elderly showed that yoga-based exercise had stronger effects (g = 0.38) than both resistance training (g = 0.22) and aerobic exercise (g = 0.14), respectively.34 A notable limitation of these reviews is that they included participants with diagnosed mental disorders and/or cognitive deficits, including depression and dementia and therefore may not be generalizable to physically inactive but otherwise healthy older adults. A recent systematic review of randomized controlled trials by Hoy, Osth, Pascoe, Kandola and Hallgren32 examined the effects of yoga on cognition in older adults without known mental or physical comorbidities. Participation in yoga was associated with improved cognitive functioning, including gross memory and executive functions. However, the review was limited to only five trials, each with a high overall risk of bias, and none of the included studies compared yoga to aerobic exercise.35,36 Such direct comparisons are needed to inform clinicians who may advise patients on the potential effects of different exercise regimes.
We conducted a 12-week randomized controlled trial to compare the effects of a supported yoga-based exercise intervention to an aerobic exercise intervention and a wait-list control group (usual activities) on verbal fluency, in physically inactive but otherwise healthy older adults. We hypothesized that participation in yoga and aerobic exercise would be associated with equivalent magnitude improvements in verbal fluency compared to control conditions.
Materials and Methods
Design and Setting
We conducted a twelve-week, three-group, single-blinded, parallel randomized controlled trial (RCT) in accordance with the CONSORT statement (Table S1, Supplementary Materials) and the Helsinki Declaration for research involving humans.37 This study was conducted at the Karolinska Institute (KI) in central Stockholm and approved by the Regional Ethics Committee in Stockholm (2017/1862-31/2, amendment number 2018/2156-32). The trial was prospectively registered with German Clinical Trials (DRKS 00015093). A study protocol is publicly available.38
Participants
A total of 82 community-dwelling participants were recruited via three separate advertisements in a newspaper distributed throughout central Stockholm (“Mitt-I”, April 2019–January 2020). Inclusion criteria: Age 65–85 years, resident of Stockholm County and fluent in Swedish. Informed consent was obtained prior to enrollment. Exclusion criteria: (a) Participation in regular, structured exercise ≥ two days/week, moderate-to-vigorous activities ≥ 75 min/week, or light-to-moderate activities ≥150min/week during the previous three months; (b) Physical disability, injury or severe cognitive deficit (diagnosed dementia); (c) Major surgery during the past year (or planned the coming year) that would impair physical activity or movement; (d) Insulin-dependent diabetes, irregular pulse, uncontrolled blood glucose or blood pressure; (e) Advised against moderate exercise by a medical professional; (f) Recent diagnosis of serious mental illness (major depressive disorder, bipolar disorder, or schizophrenia spectrum disorders) or acutely suicidal; (g) Unable to attend the yoga studio or a fitness centre used in the study. A more detailed description of the inclusion criteria is available in the study protocol.38
Procedure
Individuals who were interested in the trial were advised to contact (by phone or email) a research assistant who conducted a 20-minute telephone screening interview to determine eligibility (section 2.2). Those eligible were invited to a baseline assessment (~1.5 hours) between one and three weeks later, during which demographic, questionnaire and anthropometric data were collected by a research assistant. Participants were referred to have baseline blood samples taken at the Karolinska University Hospital laboratory (in collaboration with Karolinska Trial Alliance). Follow-up appointments were booked at 6 weeks (midpoint) and 12 weeks (endpoint). Midpoint assessments involved a brief (~15 minutes) assessment for adverse events and aimed to resolve adherence issues (eg, accessing exercise classes). Follow-up assessments were identical to baseline assessments but were conducted by a different research assistant.
Randomization and Blinding
A sex-stratified randomization list was generated by an independent statistician using a random number computer program. The allocation sequence was then transferred into sealed, opaque envelopes by an independent research assistant. Participants opened envelopes immediately after the baseline assessment. Group allocation was recorded on separate forms that were not readily available to follow-up assessors and participants were asked to avoid revealing group allocation. Research assistants were therefore blinded to group allocation at follow-up.
Measures
Verbal fluency was tested at baseline and at 12-week follow-up. To assess phonological fluency, participants were required to recall as many unique words as possible beginning with the letters F, A and S, within 60 a second period for each letter (total-FAS). Participants were then asked to name as many animals and verbs as they could, in 60 seconds for each category, in order to test semantic fluency. All tests were audio recorded, and the number of unique words (total-FAS, animals and verbs) were calculated by the research assistant following each test. Verbal fluency tests are widely reported as valid, reliable measures of executive functioning and language in older adults; phonological fluency, in particular, is considered to depend heavily on executive functions.39–41
Baseline assessments involved collecting demographic data including age, gender and education), along with indicators of somatic health, such as self-reported information about comorbidities, medications, smoking, alcohol consumption and physical activity behaviours (International Physical Activity Questionnaire) were collected at baseline.42 We assessed blood pressure and resting heart rate using the Omron M3 Comfort monitor. Body mass index was calculated from objective measurements, waist circumference was measured, and balance examined using the Berg Balance Scale.43 Grip strength for the dominant hand was assessed with an electronic hand-held dynamometer. Blood samples were analysed for total cholesterol, high-density lipoprotein (HDL) and low-density lipoprotein (LDL). Participants recorded their exercise adherence using a training calendar which indicated when a scheduled yoga or aerobic exercise session was completed. Participants were asked to aim to complete at least three classes/week for a period of 12 weeks and also to record any additional, informal sessions of moderate-vigorous physical activity. Exercise intensity was estimated at six-weeks via Borg’s Rating of Perceived Exertion scale (RPE); scored from six (no exertion) to 20 (maximal exertion).44 Mid-ranges on the RPE (the target of this intervention) are as follows: 11 = fairly light, 13 = somewhat hard, 15 = hard. Scores between these values have no narrative values. The mean RPE reported for three exercise sessions during the previous week was calculated. Adverse events were assessed at weeks six and 12 by asking participants if they had experienced any injuries caused by participating in the trial. All participants who reported adverse events were referred to see their doctor (general practitioner).
Interventions
Yoga
Each yoga group participant received a free 12-week membership to a centrally located yoga studio. Classes were one hour in length, designed for older adults and beginners and also available to adults not participating in the study. Classes were offered at least three times/week. Yoga participants were also provided with access to “Yogobe”, an online platform with yoga classes adapted for seniors. These could be used for home yoga practice. The intervention was based on Hatha yoga which involves gentle physical postures (asanas) plus breathing exercises and is appropriate for older adults.45 Opening postures included: Cat/Cow pose, Mountain pose and Partial Sun Salute. Classic Hatha yoga postures were then instructed, including Chair pose, Plank, Tree pose, Warrior I and II, Downward facing dog, Side stretch, Spine twist, Cobra pose and Bridge pose. The finishing series included relaxation exercises such as Dead man’s pose. A detailed description of these movements has been reported previously.45 Around 50 minutes was devoted to physical postures and 10 to breathing exercises and relaxation. Between two and 10 people participated in each class.
Aerobic Exercise
The aerobic exercise group received a free 12-week membership with ‘Friskis & Svettis’, permitting access to fitness centres across Stockholm. Participants were asked to complete three 60-minute supervised group aerobic exercise classes/week. All classes were suitable for older adults. To optimize adherence, participants were given the option of three different types of aerobic exercise: cycling/spinning, dance-based exercise, and light-to-moderate intensity aerobics (synchronized movement to music). Participants met a personal trainer (~30 minutes) for an introduction to the web-based booking system and to help them choose classes. Participants also received a DVD produced by the fitness centre that contained several seated aerobic exercise workouts suitable for older adults, and could also access online classes as part of their fitness centre membership. Participants were encouraged to increase gradually to a subjectively “moderate” exercise intensity. All classes were delivered by qualified fitness instructors and were available to adults not taking part in the study. Typically, classes were attended by 10–25 people.
Wait-List Control
The wait-list control group was instructed to continue usual daily activities without increasing physical activity levels or commencing a new exercise regime. To improve adherence, a free cinema ticket and a 12-week membership (to begin after the study ended) to either the yoga studio or the aerobic exercise facility was offered to those who adhered to the wait-list condition and completed a follow-up assessment.
Effects of COVID-19 on Recruitment, Exercise Adherence and Assessment
Trial recruitment commenced in April 2019 and concluded in March 2020 due to COVID-19 restrictions, which mandated closure of the yoga and aerobic exercise facilities. There was, however, no formal lockdown or restriction of unsupervised, outdoor physical activity. Prior to restrictions, 82 trial participants were enrolled; 41 had completed a 12-week intervention and 41 were in various stages of completion. To facilitate intervention continuation, we provided enrolled participants with verbal and written instructions on how to continue their exercise regimes. Yoga participants received a leaflet produced by the trial’s yoga teacher with instructions and diagrams illustrating the postures and sequences used at the studio. Participants were asked to continue yoga sessions at home three times/week using the booklet or online materials as a guide. Similarly, those randomized to aerobic exercise were instructed to continue their preferred form(s) of aerobic exercise from home and, where possible, to replicate the exercises offered during the trial. All follow-up assessments that occurred after restrictions were introduced were conducted via telephone. Thus, post-COVID-19 follow up assessments did not include physical examinations such as blood pressure and heart rate.
Data Analysis Plan
Sample Size
A sample size calculation is described in the published protocol.38 Based on a previous related study46 and a predicted small effect size (0.2) – favouring yoga compared to aerobic exercise – a total sample of 180 participants was estimated. Due to COVID-19 restrictions this target could not be met; the trial is thus underpowered to detect statistically significant differences. Instead, our analyses focus on the magnitude of group differences (estimated effect sizes).
Statistical Methods
Descriptive statistics were stratified according to intervention group. Primary analyses followed intention-to-treat (ITT) principals. Between-group differences in verbal fluency were assessed using Analysis of Covariance (ANCOVA) with baseline score included as the covariate. Within-group changes in mean verbal fluency test scores (baseline to 12-weeks) are reported with 95% confidence intervals (CIs). Independent samples t-tests with Bonferroni corrections were used to explore contrasts between differences in the three groups at follow-up (yoga versus aerobic exercise; yoga versus wait-list control; aerobic exercise versus wait-list control). Estimated effect sizes (Hedges’ g) with p-values are reported for the three groups and interpreted using the following criteria; 0.2, small, 0.5, medium and 0.8 or higher, a large effect size.47 Assumptions were examined using the Shapiro–Wilk test for normality and Levene’s homogeneity of variance test. Patterns in missing follow-up data were assessed using Little’s missing completely at random (MCAR) test. Pre-planned sensitivity analyses consisted of repeating the methods described above after imputing missing follow-up data (last observation carried forward (LOCF) method).38 As no interim analyses were performed, results were not known at the point of ceasing recruitment into the trial. Analyses were conducted using SPSS v27.
Results
Participants
As this trial stopped early due to COVID-19, final follow-up took place in May 2020. The flow of participants’ progress through the trial is reported in Figure 1.
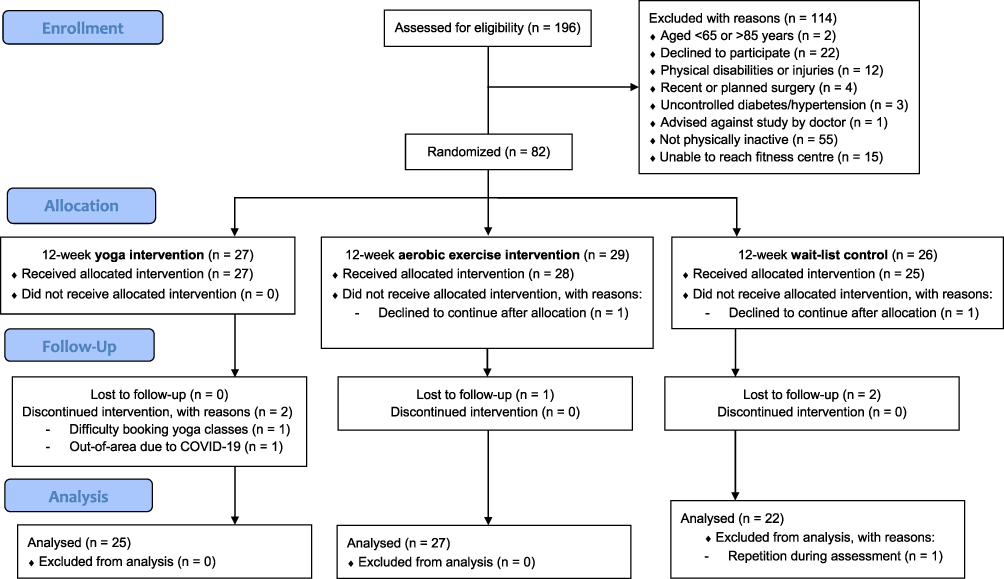 |
Figure 1 Flow diagram of participants’ progress through the trial. |
Baseline characteristics for the 82 participants are presented in Table 1. The mean age was 72.5 years (65–85, standard deviation (SD) 5.3). Despite a preponderance of females (77%), the distribution of sexes was similar between groups. About 78% of participants were retired and 65% were university educated. Participants reported having, on average, one (0—4) pre-existing medical condition (eg, controlled hypertension) and taking one (0–4) medication. The majority of participants were ex-smokers (55%), followed by non-smokers (40%) and only a minority were current smokers (5%). Alcohol consumption was generally below hazardous levels;48 Approximately 7% reported consuming nine units/week or more (where one unit = 12g of pure ethanol). Participant physical activity levels were lower than those recommended by WHO (ie, ≥150 minutes of moderate-to-vigorous physical activity/week);49 The mean self-reported amount of time spent undertaking moderate-to-vigorous physical activity was about 44 minutes/week. Cholesterol, grip strength and cognition (verbal fluency) scores were similar among the three groups at baseline. Body mass index and waist circumference measurements indicated that, on average, participants were overweight at baseline.
 |
Table 1 Baseline Demographic, Clinical and Physical Characteristics of Participants (N = 82) |
Completeness of Follow-Up and Adherence
Baseline verbal fluency test scores were available for 80/82 participants; baseline data was missing for one wait-list control group participant and another wait-list participant was excluded from analyses due to difficulty following instructions during verbal fluency testing. Twelve-week follow-up was completed for 74/80 included participants (25/27 randomized to yoga, 27/29 to aerobic exercise and 23/26 to wait-list control). Participants in the yoga group reported completing a median of 28 (0–54) yoga sessions, versus 16 exercise sessions (0–51) in the aerobic exercise group (t = 2.569, p = 0.013). Yoga participants also reported completing a median of eight (0–36) informal sessions of moderate-to-vigorous physical activity, versus 17 (0–66) in the aerobic exercise group and 17 (0–90) among wait-list control group participants. On average (mean), Borg’s RPE was 14.5 (SD 1.4) per aerobic exercise session, slightly higher than a mean of 12.9 (SD 1.8) per yoga session (t = 3.17, p = 0.003).
Intervention Effects on Verbal Fluency
Table 2 shows within-group changes in mean verbal fluency at 12-week follow-up, with between-group comparisons and estimated effect sizes. Figure 2 illustrates these changes over time. Over the study duration, there were within-group increases (ie, improvements) in mean total-FAS among yoga participants (+5.0 words, p = 0.002) and aerobic exercise participants (+6.6 words, p = 0.004). Mean total-FAS in the wait-list control group, on the other hand, remained stable (−0.5 words, p = 0.838). Small increases in mean verbal fluency for animals in all three groups; yoga (+2.1 words, p = 0.071), aerobic exercise (+1.5 words, p = 0.127) and wait-list control (+1.1 words, p = 0.671) were not statistically significant. There were similar, non-significant increases in mean verbal fluency test scores for verbs in the yoga (+2.0 words, p = 0.194) and aerobic exercise (+1.4 words, p = 0.114) groups, and a slight decrease in the wait-list control group (−1.1 words, p = 0.195). There were medium-magnitude, positive estimated treatment effects on total-FAS for yoga versus wait-list control and aerobic exercise versus wait-list control: Hedges’ g = 0.51 (p = 0.213) and 0.57 (p = 0.098) respectively). However, no significant between-group differences were detected at the study endpoint (p = 0.075). Similar, medium-sized treatment effects were estimated for verbs (yoga vs wait-list control, g = 0.50, p = 0.085; aerobic exercise vs wait-list control, g = 0.59, p = 0.233), along with small treatment effects for animals (yoga vs wait-list control, g = 0.28, p = 0.155; aerobic exercise vs wait-list control, g = 0.19, p = 0.766).
 |
Table 2 Within- and Between-Group Treatment Effects on Cognition (Verbal Fluency), Intention-to-Treat Analyses (N = 74) |
 |
Figure 2 Changes in verbal fluency test over time (N = 74): (a): Increases in mean total-FAS for yoga (+5.0 words, p=0.002) and aerobic exercise groups (+6.6 words, p=0.004) over time. (b): Mean animals for yoga (+2.1 words, p=0.071), aerobic exercise (+1.5 words, p=0.127) and wait-list control (+1.1 words, p=0.671) groups over time. (c): Mean verbs for yoga (+2.0 words, p=0.194), aerobic exercise (+1.4 words, p=0.114), and wait-list control groups (−1.1 words, p=0.195) over time. |
Adverse Events
Of 82 participants, 17 (21%) reported minor adverse events, including 6/27 (22%) in the yoga group, 10/27 (37%) in the aerobic exercise group reported adverse events and 1/25 (4%) in the wait-list control group. Common adverse events included minor strains and sprains.
Sensitivity Analyses
Sensitivity analyses are presented in Supplementary Table S2 (Supplementary Materials). In general, the results following imputations were consistent with those of the main analyses, but with slightly attenuated effect sizes.
Discussion
Verbal fluency is one of the executive functions central to healthy aging, and while exercise appears to have positive effects on cognition, physical activity levels among older adults are decreasing.50,51 This 12-week RCT compared the effects of yoga, aerobic exercise, and usual activities on verbal fluency in 82 physically inactive, but otherwise healthy adults aged 65–85 years. Participants in both the yoga and aerobic exercise groups showed improvements in mean verbal fluency test scores (total-FAS). Compared to a wait-list control group, yoga and aerobic exercise interventions were estimated to have small-to-medium magnitude, positive effects on verbal fluency.
The findings of this study are consistent with a growing body of evidence suggesting that physical activity interventions, including yoga programmes, may improve cognitive function in healthy older adults.30–32,34,52 A 2021 systematic review of RCTs by Hoy et al, for example, reported beneficial effects of yoga-based interventions on cognition among healthy older adults.32 Four of the six studies included in that review reported positive effects on various aspects of cognition, including executive function, although a high risk of bias was identified in all studies. A 2020 systematic review and meta-analysis of 33 RCTs indicated that effects on executive function may vary according to the frequency, duration and type of exercise, but not the intensity level.34 The authors reported a combined effect size for yoga and Tai Chi (g = 0.38, p <0.05), comparing favourably to that for aerobic exercise (g = 0.14, p <0.05). The estimated effect sizes in our study, by comparison, were somewhat larger than those reported by Chen et al, particularly in the case of aerobic exercise. We also note that yoga and aerobic exercise had similar estimated effects on verbal fluency, despite higher adherence in the yoga group and marginally higher RPE in the aerobic exercise group. Our findings, however, are in keeping with those of the largest trial (N = 792) in this field to date, which reported that once-weekly supervised yoga classes, with independent home practice, resulted in improved Mini-Mental State Examination (MMSE) and Rivermead Behavioural Memory Test (third edition) scores in older adults (mean age = 67.1 years, SD 3.2), when compared to a wait-list control group (yoga intervention versus wait-list, d = 0.43, p = 0.04; yoga intervention follow-up versus baseline, d = 0.46, p = 0.02).53 This is the first study to examine the effects of yoga on verbal fluency in older adults. One study54 showed that introducing an aerobic exercise regimen (spin cycling) in previously sedentary older adults (n=20) improves semantic fluency over a period of 12 weeks, which is consistent with the current findings.
Within-group changes in verbal fluency in the yoga and aerobic exercise groups in the current study may suggest the presence of intervention effects. Baseline scores for total-FAS, animals and verbs were equal to, or greater than existing normative mean values for Swedish adults aged 65–89 (total-FAS 36.6–45.2, animals 17.8–20.6 and verbs 14.9–19.4, dependent on educational level),55 observed changes are therefore unlikely to be explained by regression to the mean. Verbal fluency scores also remained stable for the wait-list control group, suggesting that improvements in the yoga and aerobic groups are not adequately explained by test practice effects. Unfortunately, due to unforeseeable exercise facility closures that occurred due to COVID-19, this trial was insufficiently powered to detect between-group differences. We speculate that, had our intended sample size been reached and supervised training proceeded as planned, group differences – favouring yoga and aerobic exercise – may have reached statistical significance. It is unclear whether the within-group increments in verbal fluency that occurred among the yoga and aerobic exercise group participants reflect meaningful changes in executive function. Previous longitudinal work has tended to address the decline in verbal fluency that accompanies the progression of cognitive impairment, rather that increases in verbal fluency among healthy older adults.2 It is widely acknowledged, however, that executive functions are vital for participation in daily activities even among older adults without cognitive impairment.56
While we did not investigate the potential mechanism underlying improvements in verbal fluency in the current study, we speculate that findings may be explained by neurobiological, psychological, and social processes. Exercise appears to regulate the hypothalamo-pituitary-adrenal (HPA) axis, leading to reductions in glucocorticoid stress hormones.57 Reducing the levels of circulating stress hormones may, in turn, ameliorate the detrimental effects of chronic stress on cognition.58 Similarly, reduced psychological stress and improved cognitive efficiency have been suggested to explain the effects of yoga on cognition.28,59 While the primary focus of interventions in our study was physical activity, rather than meditation, earlier work suggests that the meditative aspect of yoga may increase resting-state activity in multiple cortico-striatal circuits;60 offering a putative explanation for improvements in executive function.29 The psychological effects of increasing physical activity may also be important; exercise can act as a distraction from stressful life events, improve self-esteem, and may reduce negative attentional biases.61 The well-documented beneficial effects of exercise on mood may in itself lead to improved executive functions.62 Finally, social isolation is suggested to be detrimental for cognition in later life and has recently been amplified by the effects of COVID-19.63,64 We suggest that, in the current study, social interactions that occurred when attending yoga or aerobic exercise classes may have provided a further stimulus for improvements in verbal fluency.
Strengths and Limitations
Strengths of this study include the randomized design with blinded follow-up assessments, the comparison of two forms of community-based physical activity and the inclusion of a non-active control group. Physically inactive, but otherwise healthy older adults represent a growing but understudied population group. Verbal fluency testing included both phonological and semantic variations, providing a valid and reliable estimation of executive control processes.41 Adherence and Borg’s RPE were assessed, allowing the intervention dose to be considered, although compliance with allocated interventions and exercise intensity were not measured objectively.
As noted previously, this trial was underpowered due to COVID-19 restrictions and half of the participants were affected by necessary changes to the study protocol. We recognise that conducting some follow-up assessments of verbal fluency via telephone may have disadvantaged certain participants, such those with hearing-impairments. Our rationale for reporting pre- and post-COVID-19 participants together was as follows. Firstly, all three groups were affected equally by restrictions, except for the termination of supervised exercises classes. We consider that, while this may have attenuated treatment effects, it is unlikely that significant bias was introduced. Secondly, as COVID-19 policy in Sweden did not include a formal lockdown, or curfews, participants were able to continue non-supervised physical activity and a degree of social contact, consistent with the original study protocol. Thirdly, we felt that reporting separate analyses would have introduced an unnecessary loss of statistical power, given that measures such as online materials were put in place to allow participants to continue planned interventions as closely as possible.
Study generalizability is likely to be limited by a healthy entrant effect, where participants were at a stage of readiness to change their physical activity habits, as well as by the predominance of female participants. The limited follow-up period also prevents any inference of longer-term cognitive benefits.
Conclusion
Participation in either a 12-week yoga-based intervention or a 12-week aerobic exercise intervention was associated with an increase in phonological (total-FAS) verbal fluency. When compared to a wait-list control group, small-to-medium magnitude estimated treatment effects were seen for participation in either yoga or aerobic exercise. Overall, these findings support the recommendation of both yoga and aerobic exercise to promote healthy aging in physically inactive older adults. The results may inform the design of an appropriately powered RCT. Such work should also aim to evaluate the effects of yoga and aerobic exercise on other domains of cognitive function, as well as on brain structure, to better understand the mechanisms underlying potential cognitive changes.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Helsinki Declaration and approved by the Regional Ethics Committee in Stockholm (2017/1862-31/2, amendment number 2018/2156-32).
Acknowledgments
The authors would like to acknowledge Hugo Sjöqvist for assistance with randomization, blinding and statistical advice and Patricia Eustachio Colombo for conducting assessments.
Funding
This study is supported by Swedish Research Council for Health, Working Life and Welfare (FORTE), grant number 2017-00024. The funding body had no involvement in the collection, analysis or interpretation of data, the writing of the manuscript or the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stein J, Luppa M, Luck T, et al. The assessment of changes in cognitive functioning: age-, education-, and gender-specific reliable change indices for older adults tested on the CERAD-NP battery: results of the German study on ageing, cognition, and dementia in primary care patients (AgeCoDe). Am J Geriat Psychiat. 2012;20(1):84–97. doi:10.1097/JGP.0b013e318209dd08
2. Clark LJ, Gatz M, Zheng L, Chen YL, McCleary C, Mack WJ. Longitudinal verbal fluency in normal aging, preclinical, and prevalent Alzheimer’s disease. Am J Alzheimers Dis Other Demen. 2009;24(6):461–468. doi:10.1177/1533317509345154
3. Jessen F, Amariglio RE, Buckley RF, et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020;19(3):271–278. doi:10.1016/S1474-4422(19)30368-0
4. Shafto MA, Tyler LK. Language in the aging brain: the network dynamics of cognitive decline and preservation. Science. 2014;346(6209):583–587. doi:10.1126/science.1254404
5. Ansado J, Marsolais Y, Methqal I, Alary F, Joanette Y. The adaptive aging brain: evidence from the preservation of communication abilities with age. Eur J Neurosci. 2013;37(12):1887–1895. doi:10.1111/ejn.12252
6. Machado A, Barroso J, Molina Y, et al. Proposal for a hierarchical, multidimensional, and multivariate approach to investigate cognitive aging. Neurobiol Aging. 2018;71:179–188. doi:10.1016/j.neurobiolaging.2018.07.017
7. Schuch FB, Vancampfort D, Firth J, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiat. 2018;2018:1.
8. Guadagni V, Drogos LL, Tyndall AV, et al. Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology. 2020;94(21):E2245–E2257. doi:10.1212/Wnl.0000000000009478
9. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
10. Gomes M, Figueiredo D, Teixeira L, et al. Physical inactivity among older adults across Europe based on the SHARE database. Age Ageing. 2017;46(1):71–77. doi:10.1093/ageing/afw165
11. Hootman JM, Macera CA, Ainsworth BE, Addy CL, Martin M, Blair SN. Epidemiology of musculoskeletal injuries among sedentary and physically active adults. Med Sci Sports Exerc. 2002;34(5):838–844. doi:10.1097/00005768-200205000-00017
12. Reid H, Foster C. Infographic. Physical activity benefits for adults and older adults. Br J Sports Med. 2017;51(19):1441. doi:10.1136/bjsports-2016-096811
13. United States Department of Health and Human Services. Physical Activity Guidelines for Americans 2nd edition; 2020. Available from: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf.
14. Sivaramakrishnan D, Fitzsimons C, Kelly P, et al. The effects of yoga compared to active and inactive controls on physical function and health related quality of life in older adults- systematic review and meta-analysis of randomised controlled trials. Int J Behav Nutr Phys Act. 2019;16(1):33. doi:10.1186/s12966-019-0789-2
15. Northey JM, Cherbuin N, Pumpa KL, Smee DJ, Rattray B. Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med. 2018;52(3):154–160. doi:10.1136/bjsports-2016-096587
16. Pascoe MC, de Manincor M, Tseberja J, Hallgren M, Baldwin PA, Parker AG. Psychobiological mechanisms underlying the mood benefits of meditation: a narrative review. Comp Psychoneuroendocrinol. 2021;6:100037. doi:10.1016/j.cpnec.2021.100037
17. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;2008(12):1–23.
18. McCall MC. In search of yoga: research trends in a western medical database. Int J Yoga. 2014;7(1):4–8. doi:10.4103/0973-6131.123470
19. Schmalzl L, Powers C, Henje Blom E. Neurophysiological and neurocognitive mechanisms underlying the effects of yoga-based practices: towards a comprehensive theoretical framework. Hypothesis and Theory. Front Hum Neurosci. 2015;9:235. doi:10.3389/fnhum.2015.00235
20. Wieland LS, Cramer H, Lauche R, Verstappen A, Parker EA, Pilkington K. Evidence on yoga for health: a bibliometric analysis of systematic reviews. Complement Ther Med. 2021;60:102746. doi:10.1016/j.ctim.2021.102746
21. Cramer H, Lauche R, Anheyer D, et al. Yoga for anxiety: a systematic review and meta-analysis of randomized controlled trials. Depress Anxiety. 2018;35(9):830–843. doi:10.1002/da.22762
22. Hariprasad VR, Sivakumar PT, Koparde V, et al. Effects of yoga intervention on sleep and quality-of-life in elderly: a randomized controlled trial. Indian J Psychiat. 2013;55(7):S364–S368. doi:10.4103/0019-5545.116310
23. Cramer H, Lauche R, Dobos G. Characteristics of randomized controlled trials of yoga: a bibliometric analysis. BMC Complement Altern Med. 2014;14:328. doi:10.1186/1472-6882-14-328
24. Cramer H, Haller H, Lauche R, Steckhan N, Michalsen A, Dobos G. A systematic review and meta-analysis of yoga for hypertension. Am J Hypertens. 2014;27(9):1146–1151. doi:10.1093/ajh/hpu078
25. Sovova E, Cajka V, Pastucha D, Malincikova J, Radova L, Sovova M. Positive effect of yoga on cardiorespiratory fitness: a pilot study. Int J Yoga. 2015;8(2):134–138. doi:10.4103/0973-6131.158482
26. Cramer H, Lauche R, Haller H, Steckhan N, Michalsen A, Dobos G. Effects of yoga on cardiovascular disease risk factors: a systematic review and meta-analysis. Int J Cardiol. 2014;173(2):170–183. doi:10.1016/j.ijcard.2014.02.017
27. Büssing A, Michalsen A, Khalsa SBS, Telles S, Sherman KJ. Effects of yoga on mental and physical health: a short summary of reviews. Evid Based Complement Alter Med. 2012;2012:165410. doi:10.1155/2012/165410
28. Gothe NP, Khan I, Hayes J, Erlenbach E, Damoiseaux JS. Yoga effects on brain health: a systematic review of the current literature. Brain Plast. 2019;5(1):105–122. doi:10.3233/BPL-190084
29. Brunner D, Abramovitch A, Etherton J. A yoga program for cognitive enhancement. PLoS One. 2017;12(8):e0182366. doi:10.1371/journal.pone.0182366
30. Luu K, Hall PA. Hatha yoga and executive function: a systematic review. J Altern Complement Med. 2016;22(2):125–133. doi:10.1089/acm.2014.0091
31. Chobe S, Chobe M, Metri K, Patra SK, Nagaratna R. Impact of Yoga on cognition and mental health among elderly: a systematic review. Complement Ther Med. 2020;52:102421. doi:10.1016/j.ctim.2020.102421
32. Hoy S, Osth J, Pascoe M, Kandola A, Hallgren M. Effects of yoga-based interventions on cognitive function in healthy older adults: a systematic review of randomized controlled trials. Complement Ther Med. 2021;2021:58. doi:10.1016/j.ctim.2021.102690
33. Gothe NP, McAuley E. Yoga and cognition: a meta-analysis of chronic and acute effects. Psychosom Med. 2015;77(7):784–797. doi:10.1097/psy.0000000000000218
34. Chen FT, Etnier JL, Chan KH, Chiu PK, Hung TM, Chang YK. Effects of exercise training interventions on executive function in older adults: a systematic review and meta-analysis. Sports Med. 2020;23:23. doi:10.1007/s40279-020-01292-x
35. Lam FM, Huang MZ, Liao LR, Chung RC, Kwok TC, Pang MY. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: a systematic review. J Physiother. 2018;64(1):4–15. doi:10.1016/j.jphys.2017.12.001
36. Cammisuli DM, Innocenti A, Franzoni F, Pruneti C. Aerobic exercise effects upon cognition in mild cognitive impairment: a systematic review of randomized controlled trials. Arch Ital Biol. 2017;155(1–2):54–62. doi:10.12871/000398292017126
37. Bennett JA. The consolidated standards of reporting trials (CONSORT) - Guidelines for reporting randomized trials. Nurs Res. 2005;54(2):128–132.
38. Osth J, Diwan V, Jirwe M, et al. Effects of yoga on well-being and healthy ageing: study protocol for a randomised controlled trial (FitForAge). BMJ Open. 2019;9:5. doi:10.1136/bmjopen-2018-027386
39. Bryan J, Luszcz MA, Crawford JR. Verbal knowledge and speed of information processing as mediators of age differences in verbal fluency performance among older adults. Psychol Aging. 1997;12(3):473–478. doi:10.1037//0882-7974.12.3.473
40. Torralva T, Laffaye T, Báez S, et al. Verbal fluency as a rapid screening test for cognitive impairment in early Parkinson’s disease. J Neuropsychiatry Clin Neurosci. 2015;27(3):244–247. doi:10.1176/appi.neuropsych.14060139
41. Shao Z, Janse E, Visser K, Meyer AS. What do verbal fluency tasks measure? Predictors of verbal fluency performance in older adults. Front Psychol. 2014;5:772. doi:10.3389/fpsyg.2014.00772
42. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.Mss.0000078924.61453.Fb
43. Berg K. Measuring balance in the elderly: preliminary development of an instrument. Physiother Can. 1989;41:304–311. doi:10.3138/ptc.41.6.304
44. Borg G, Ljunggren G, Ceci R. The increase of perceived exertion, aches and pain in the legs, heart-rate and blood lactate during exercise on a bicycle ergometer. Eur J Appl Physiol. 1985;54(4):343–349. doi:10.1007/Bf02337176
45. Greendale GA, Kazadi L, Mazdyasni S, et al. Yoga Empowers Seniors Study (YESS): design and asana series. J Yoga Phys Ther. 2012;2:1. doi:10.4172/2157-7595.1000107
46. Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med. 2006;12(1):40–47.
47. Durlak JA. How to select, calculate, and interpret effect sizes. J Pediatr Psychol. 2009;34(9):917–928. doi:10.1093/jpepsy/jsp004
48. Wood AM, Kaptoge S, Butterworth AS, et al. Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet. 2018;391(10129):1513–1523. doi:10.1016/S0140-6736(18)30134-X
49. World Health Organizatio. Global Recommendations on Physical Activity for Health; WHO Guidelines Approved by the Guidelines Review Committee. World Health Organization; 2010.
50. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–257. doi:10.1016/S0140-6736(12)60646-1
51. Sanders LMJ, Hortobágyi T, la Bastide-van Gemert S, van der Zee EA, van Heuvelen MJG. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: a systematic review and meta-analysis. PLoS One. 2019;14(1):e0210036. doi:10.1371/journal.pone.0210036
52. Ludyga S, Gerber M, Pühse U, Looser VN, Kamijo K. Systematic review and meta-analysis investigating moderators of long-term effects of exercise on cognition in healthy individuals. Nat Hum Behav. 2020;4(6):603–612. doi:10.1038/s41562-020-0851-8
53. Pandya SP. Yoga education program for improving memory in older adults: a multicity 5-year follow-up study. J Appl Gerontol. 2020;39(6):576–587. doi:10.1177/0733464818794153
54. Nocera JR, McGregor KM, Hass CJ, Crosson B. Spin exercise improves semantic fluency in previously sedentary older adults. J Aging Phys Act. 2015;23(1):90–94. doi:10.1123/JAPA.2013-0107
55. Tallberg IM, Ivachova E, Jones Tinghag K, Östberg P. Swedish norms for word fluency tests: FAS, animals and verbs. Scand J Psychol. 2008;49(5):479–485. doi:10.1111/j.1467-9450.2008.00653.x
56. World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
57. Matta Mello Portugal E, Cevada T, Sobral Monteiro-Junior R, et al. Neuroscience of exercise: from neurobiology mechanisms to mental health. Neuropsychobiology. 2013;68(1):1–14. doi:10.1159/000350946
58. Jett JD, Morilak DA. Too much of a good thing: blocking noradrenergic facilitation in medial prefrontal cortex prevents the detrimental effects of chronic stress on cognition. Neuropsychopharmacology. 2013;38(4):585–595. doi:10.1038/npp.2012.216
59. Pascoe MC, De Manincor M, Hallgren M, Baldwin PA, Tseberja J, Parker AG. Psychobiological mechanisms underlying the mental health benefits of yoga-based interventions: a narrative review. Mindfulness. 2021;2021:1. doi:10.1007/s12671-021-01736-z
60. Gard T, Taquet M, Dixit R, Hölzel BK, Dickerson BC, Lazar SW. Greater widespread functional connectivity of the caudate in older adults who practice kripalu yoga and vipassana meditation than in controls. Origin Res. 2015;2015:9. doi:10.3389/fnhum.2015.00137
61. Hallgren M, Dunstan DW, Owen N. Passive versus mentally active sedentary behaviors and depression. Exerc Sport Sci Rev. 2020;48(1):20–27. doi:10.1249/jes.0000000000000211
62. Suwabe K, Hyodo K, Fukuie T, et al. Positive mood while exercising influences beneficial effects of exercise with music on prefrontal executive function: a functional NIRS study. Neuroscience. 2021;454:61–71. doi:10.1016/j.neuroscience.2020.06.007
63. Banerjee D, Rai M. Social isolation in Covid-19: the impact of loneliness. Int J Soc Psychiatry. 2020;66(6):525–527. doi:10.1177/0020764020922269
64. Evans IEM, Martyr A, Collins R, Brayne C, Clare L. Social isolation and cognitive function in later life: a systematic review and meta-analysis. J Alzheimers Dis. 2019;70:S119–S144. doi:10.3233/JAD-180501
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.