")
Back to Journals » Medical Devices: Evidence and Research » Volume 16
Efficiency of Medical Equipment Utilization and Its Associated Factors at Public Referral Hospitals in East Wollega Zone, Oromia Regional State, Ethiopia
Authors Tesfaye Geta E , Terefa DR , Desisa AE
Received 11 December 2022
Accepted for publication 16 February 2023
Published 22 February 2023 Volume 2023:16 Pages 37—46
DOI https://doi.org/10.2147/MDER.S401041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Edosa Tesfaye Geta, Dufera Rikitu Terefa, Adisu Ewunetu Desisa
Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Oromia, Ethiopia
Correspondence: Edosa Tesfaye Geta, Department of Public Health, Institute of Health Science, Wollega University, Nekemte, Oromia, Ethiopia, Tel +251912701713, Email [email protected]
Background: The significance of effectively using medical equipment has received widespread public attention. Due to its complex effects on healthcare costs and quality, the relationship between hospital features and medical equipment consumption has drawn increased attention. Therefore, the study aimed to evaluate the efficiency of medical equipment utilization and its associated factors.
Methods: The study was conducted at public referral hospitals in East Wollega, Oromia Regional National State, Ethiopia, in 2021. A cross-sectional study design was mixed with observation and document review. The study included approximately 192 pieces of equipment. Descriptive statistics and Pearson Chi-square (χ2) were used to identify associations between each independent and dependent variable at p< 0.05 to declare level of significance.
Results: Using 95% confidence interval (CI), the level of utilization coefficient was estimated to be 0.49 (0.44– 0.55). As a result, 111 pieces of equipment (57.8%) were used efficiently, while 81 (42.2%) were underutilized. The form in which the hospitals received the equipment (χ2=7.7.2; P=0.005), regular availability (χ2=19.30; P=0.00), equipment breakdown (χ2=11.57; P=0.001), the availability of trained staffs operating the equipment (χ2=26.14; P=0.00), performing preventive maintenance (χ2=91.54; P=0.00), the availability of spare parts (χ2=32.36; P=0.00), and the availability of accessories (χ2=43.91; P=0.00) were statistically significant factors affecting the medical equipment utilization.
Conclusion: On average, the utilization coefficient of medical equipment in the study hospitals was low compared to other study findings, which indicated that 2 out of 5 pieces of medical equipment were under-utilized, which could be significantly affected by the form in which the hospital received the equipment, its regular availability, equipment breakdown, availability of trained staff operating the equipment, performing preventive maintenance, and availability of adequate spare parts and accessories. Every hospital should develop an appropriate strategic framework to manage and utilize the available medical diagnostic equipment based on its level and demand.
Keywords: medical equipment, efficient utilization, public hospitals, Ethiopia
Introduction
Medical equipment is any device, substance, or other item that may be used alone or in conjunction to diagnose, prevent, treat, monitor, or lessen a disease.1 When providing health services, medical equipment is utilized for a number of functions, including disease diagnosis and treatment as well as rehabilitation after illnesses or accidents. This apparatus may be used separately or in conjunction with other medical devices, consumables, or accessories.2
The provision of high-quality diagnostic services and clinical patient management can be impacted by the availability and effective use of medical equipment in healthcare facilities.3 The significance of effective medical equipment use has been fully publicized in the contemporary healthcare system.4 The connection between hospital features and the employment of high-tech medical equipment has also drawn considerable attention due to its complex consequences for health-care expenditures.5
When the health care facilities use the available medical equipment to its full potential, that is very important so that the realistic performance that may be set is considered as the equipment being optimally utilized. An optimal utilization of the equipment could result in optimal patient handling and rapid turnover, minimum possible cost, quality of care, and patient satisfaction,6 and in an era of cost-intensive medical care, every piece of equipment installed in health care facilities needs to be fully and properly utilized.7
Health institutions ranging from a small rural clinic to a major specialized hospital require medical equipment ranging from a simple scissor to more complicated and advanced ones. However, the majority of these healthcare facilities are unaware of these necessary medical devices. This is a typical issue, especially in underdeveloped nations where health technology assessments are uncommon.8
Increasing the number of investigations and offering high-quality, affordable care are priorities for successful use of the medical equipment. Advanced medical gadgets are an essential component of medical care in the processes of illness prevention, accurate diagnosis, and treatment, according to an appraisal of the worldwide health experience.9
A component of health technologies, medical equipment gives healthcare professionals the tools they need to carry out their duties successfully and efficiently. Medical equipment has the potential for improved health services, but the absence of a national structure for its selection, procurement, usage, and administration may result in an unjustified rise in the price of providing healthcare.10
Health systems in both affluent and developing nations are struggling to manage the delivery of healthcare in the face of global resource restrictions.11 It is estimated that every day, medical establishments all around the world utilize more than 50,000 unique types of gadgets. While some are complicated and include many technologies, the majority of the devices are rather straightforward.12 According to the World Health Organization, roughly 50% of the medical equipment in underdeveloped nations is inoperable, not utilized properly or to its full potential, and is almost always not maintained.13
Efficiency of medical equipment is one of the aspects that management in the healthcare delivery system commonly overlooks, which can result in losses by lowering output. Low standards of diagnosis and treatment will result from inadequate preventive maintenance of the equipment, which will also raise the cost of equipment maintenance.7
The delivery of healthcare suffers greatly when there is a dearth of operating equipment in settings with limited resources. Up to 95% of medical equipment and 50% of laboratory and medical equipment are said to be inoperable in the poor world, according to a frequent statistic.14
High-quality, life-saving medical equipment is largely unattainable in African healthcare institutions, and 40% of the physical equipment that low-resource hospitals throughout the world own is inoperable.15
In Ethiopia, it is believed that more than 40% of the medical equipment used in healthcare institutions is constantly malfunctioning. The ability of medical institutions to provide quality healthcare has been hampered by improper management of medical equipment. Only 60% of the medical equipment present in public hospitals and other healthcare institutions are thought to be operational at any one moment.16,17 The utilization index is an important parameter for monitoring the functional status of medical equipment or assessing the productivity of equipment service.18
The ability of healthcare practitioners to offer effective healthcare services has been hampered in Ethiopia by the poor use of healthcare technology. A functioning healthcare system requires the use of health technology.16 To evaluate the effective use of the medical equipment and related aspects in the nation, the proper study is required. Hence, the study aimed to assess the level of medical equipment utilization and its associated factors in public referral hospitals in East Wollega Zone, Oromia Regional State, Ethiopia.
Conceptual Framework
According to the many reviews of the literature, institutional factors, device-related variables, and professionally operated aspects are the main contributors to the effective use of medical diagnostic equipment (Figure 1).
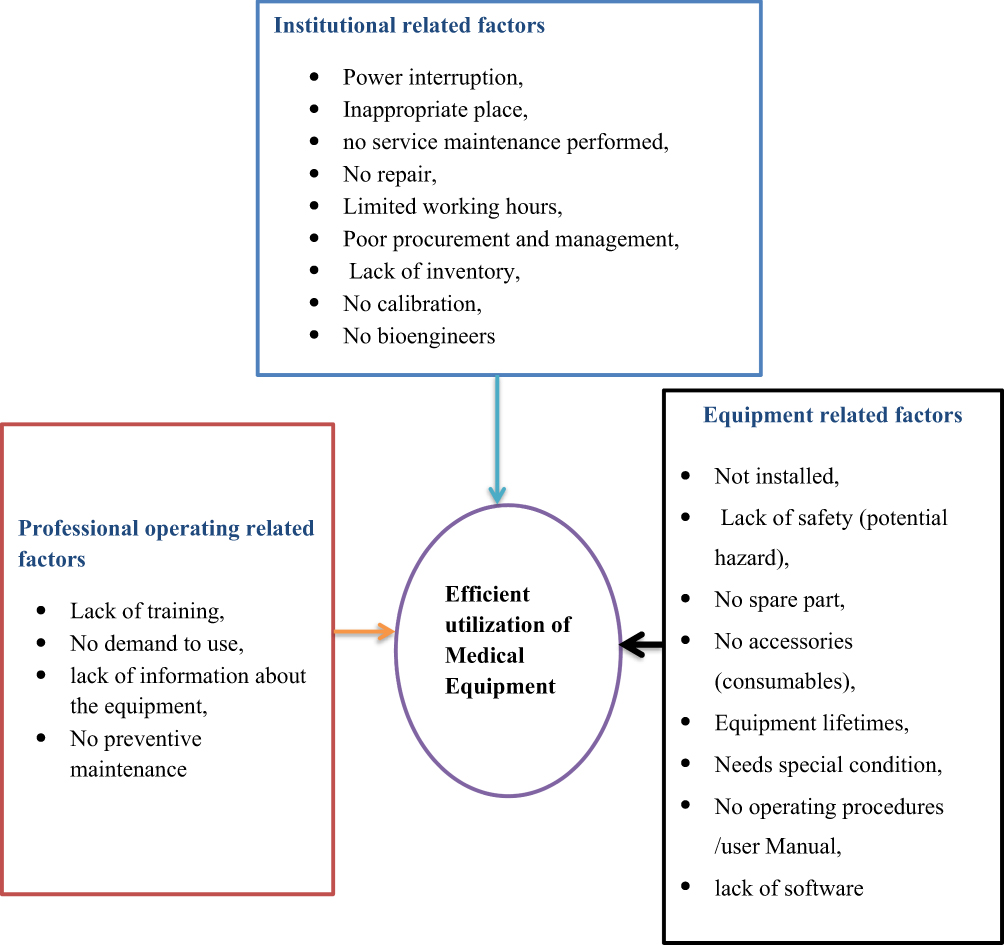 |
Figure 1 Conceptual framework for medical equipment utilization in public referral hospitals. |
Methods and Materials
Study Area and Design
The study was conducted at public referral hospitals in East Wollega Zone, Oromia Regional National State, Ethiopia from July 01, 2021 to August 30, 2021. A cross-sectional study with mixed observation and document review was conducted.
Source and Study Population
The study included all public referral hospitals in the East Wollega Zone, including Nekemte specialized hospital and Wollega University referral hospital. The study subjects were selected medical equipment in study hospitals.
Inclusion and Exclusion Criteria
All major medical equipment that were used for the purposes of diagnosis and treatment monitoring, and available in the study hospitals during the data collection period was included in the study, and any medical equipment on shipment to the study hospitals during the data collection period was excluded from the study. As a result, magnetic resonance imaging (MRI) and CT scan were excluded from the study.
Sample Size and Sampling Technique
At the study hospitals, a list of all medical equipment that were used for the purposes of diagnosis and treatment monitoring with unique or serial numbers was created. The total number of these medical equipment items available in all hospitals was determined. From the available equipment, 192 of them fulfilled the inclusion criteria and were included in the study. As a result, the study included both Nekemte Specialized Hospital (94 pieces of equipment) and Wollega University Referral Hospitals (98 pieces of equipment). Health care professionals involved in the operation, handling, and maintenance of this medical equipment were purposefully chosen to be interviewed about the equipment during the observation and document review.
Data Collection Tool and Technique
A structured check list was used to conduct observations of the selected equipment and professionals involved in the operation, handling, and maintenance of the equipment were interviewed. The checklist included a list of medical equipment that were available in the hospital.
For the purpose of this particular study, four data collectors and two supervisors were assigned. Both supervisors and data collectors who had a BSc degree and experience working in hospitals were assigned. These data collectors and supervisors were trained and well oriented before the pre-test and actual data collection started.
To gather data retroactively for the 12-month period spanning July 01, 2020 to June 30, 2021, a variety of departmental records, including purchase files, inventory registers, log books, and service records of specific medical equipment, were reviewed using a checklist and professionals involved in the operation were interviewed for each piece of equipment they handled and maintained.
Study Variables
The use of medical equipment was considered a dependent variable, and institutionally related factors (power interruption, inappropriate location, no service maintenance performed, no repair, limited working hours, poor procurement and management, lack of inventory, no calibration, no bioengineers), equipment-related factors (not installed, lack of safety (potential hazard), no spare part, no accessories (consumables), equipment lifetimes, need for special condition) and professional operated related factors (lack of training, lack of demand to use, lack of information about the equipment, no preventive maintenance) were considered independent variables (Figure 1).
Operational Definitions
- Medical equipment: Any equipment intended for use in the diagnosis of disease or other condition or for use in the life support and monitoring of patients in the study hospitals which included chemistry a analyzer, electrolyte analyzer, hematology analyzer, coagulation analyzer, PCR machine, ELISA machine, microscopy, centrifuges, CD4 count machine, X-ray Machine, Ultrasound machine, magnetic resonance imaging (MRI), CT scan, ECG Monitor, ventilators, Anesthesia machine, ABGA machine, corneal topography, and Visual Yag III laser system.
- Use coefficient (UC): UC was applied to assess the utilization of equipment, ie, whether the equipment was optimally utilized or underutilized. It was measured by the following formula; UC = (A × B/C × D) × 100, where, A is the number of days, the medical diagnostic equipment was actually used during for 12 months from July 01, 2020 to June 30, 2021. B is the number of hours the equipment was actually used on a working day during the 12-month period from July 01, 2020 to June 30, 2021 (average time taken by a procedure by that equipment average number of procedures performed on a working day). “C” is the number of days the medical diagnostic equipment could have been available (if the equipment was put in working order). For this, the total number of working days in 12 months from July 01, 2020 to June 30, 2021, was found out as mentioned above. “D” is the number of hours the medical equipment could have been available on a working day (if the equipment was put in working order).19 To assess the UC of the equipment, the working hours of the study hospitals were recorded. If the UC is ˂50%, it is considered to be underutilized and hence a bad investment due to inefficient utilization.3
- Efficient utilization: If the percentage of the average number of hours the medical equipment was used per day divided by the maximum number of hours the equipment could be used per day in study hospitals was ≥50% for the past 12 months from July 01, 2020 to June 30, 2021.
- Equipment related factors: Any factors that were expected to be inherited from the selected medical equipment in the study hospitals and could affect the efficient utilization of the equipment for the past 12 months from July 01, 2020 to June 30, 2021.
- Institutional related factors: Any factors related to the study referral hospitals that could affect the efficient utilization of the selected equipment in the study hospitals for the past 12 months, from July 01, 2020, to June 30, 2021.
- Professional operated related factors: Any factors related to the professional personnel in charge of operating the medical equipment that could have an impact on the efficient utilization of the selected equipment in study hospitals over the previous 12 months, from July 01, 2020 to June 30, 2021.
Data Quality Assurance
The check lists were pre-tested using some medical equipment and operating professional personnel, and then corrections were made accordingly. Data collectors were instructed to check the completeness of each checklist at the end of each interview and observation. The completeness of the checklists at the end of the day was rechecked by supervisors. This was also double-checked by the principal investigators.
Data Management and Analysis
The completed check lists were checked for completeness and consistency by supervisors. After the completeness of each check list was checked, data entry and analysis were made using SPSS version 25 software.
All study variables were subjected to descriptive statistics. The UC of equipment was calculated for all selected equipment to determine whether it is utilized efficiently or not. The Pearson Chi-square (χ2) was performed to identify associations between each independent and dependent variable, at P< 0.05, the level of significance was declared.
Results
Medical Equipment Utilization Efficiency
A total of 192 items of equipment were selected from the study hospitals and evaluated for their degree of use and related characteristics. The level of UC was calculated using a 95% CI interval and was estimated to be 0.49 (0.44–0.55). Equipment with a UC score of less than 0.5 was deemed to be underused (using it inefficiently), whereas equipment with a UC score of at least 0.5 (0.5) was seen to be using it optimally (efficient utilization). Consequently, 111 pieces of equipment (57.8%) were used optimally, compared to 81 (42.2%) that were underused (Figure 2).
 |
Figure 2 Level of medical equipment utilization in public referral hospitals in East Wollega, Oromia Regional State, Ethiopia, 2021. |


A total of 110 pieces of equipment (57.3%) were purchased, with 42 pieces (42.7%) obtained through donations from various organizations and agencies. Almost all of the equipment were installed during the study period; only 11 (5.7%) were uninstalled, and 144 (75% of the equipment) were functional, while 48 (25% of the equipment) were not functional.
A total of 163 pieces of equipment (84.9%) were utilized daily, while 29 items (15.1%) were not used daily but were nevertheless accessible with permission or upon request and 75 (39.1%) of the items of equipment experienced breakdown in the preceding year.
Only 44 (22.9%) items of equipment had uninterrupted electricity over the previous 12 months. Uninterruptible power supplies (UPS) were installed in these items of equipment. When the equipment were in use, there were frequent power outages for more than 7 in 10 pieces of equipment (77%).
Almost all equipment, 181 (94.3%), were placed in the appropriate place in the hospitals according to the manufacturer’s instructions; only 11 (5.7%) were misplaced. For more than half of the equipment, 107 (55.7%) service maintenance were performed according to the schedule.
More than half 47 (62.7%) of the 75 damaged pieces of equipment were not repaired in a timely manner to make them functional, and more than half 133 (69.3%) were not calibrated according to the manufacturer’s instructions and schedule.
For 80 (41.7%) of the workers who operated the equipment, there was insufficient training regarding equipment operation and 15 (7.8%) of the hospitals’ available equipment items were not in demand. Preventive maintenance was completed on time for more than 64.6% of the equipment. Only 15 (7.8%) of the equipment lacked safety features and posed a risk to the operators.
For more than half of the equipment, 127 (66.1%) adequate spare parts were available, and 124 (64.6%) adequate accessories (consumables) for the equipment were not available in the market when needed. Only 31 (16.1) pieces of equipment required special conditions to operate. There were no operating procedures or user manuals for 78 (40.6%) pieces of equipment.
Factors Affecting Medical Equipment Utilization Efficiency
The study has identified significant factors that could affect the efficient utilization of medical equipment in the study hospitals. As a result, the form in which the hospital received the equipment (purchased or donated) (χ2 = 7.72; P = 0.005), the regularly availability of the equipment (χ2= 19.30; P = 0.00), the equipment breakdown in the previous 12 months (χ2 = 11.57; P = 0.001), the availability of adequate staffs operating the equipment with adequate training (χ2 = 26.14; P = 0.00), performing preventive maintenance according to the manufacturer’s instructions and schedule (χ2 = 91.54; P = 0.00) were significantly associated with efficient utilization of medical equipment (Table 1).
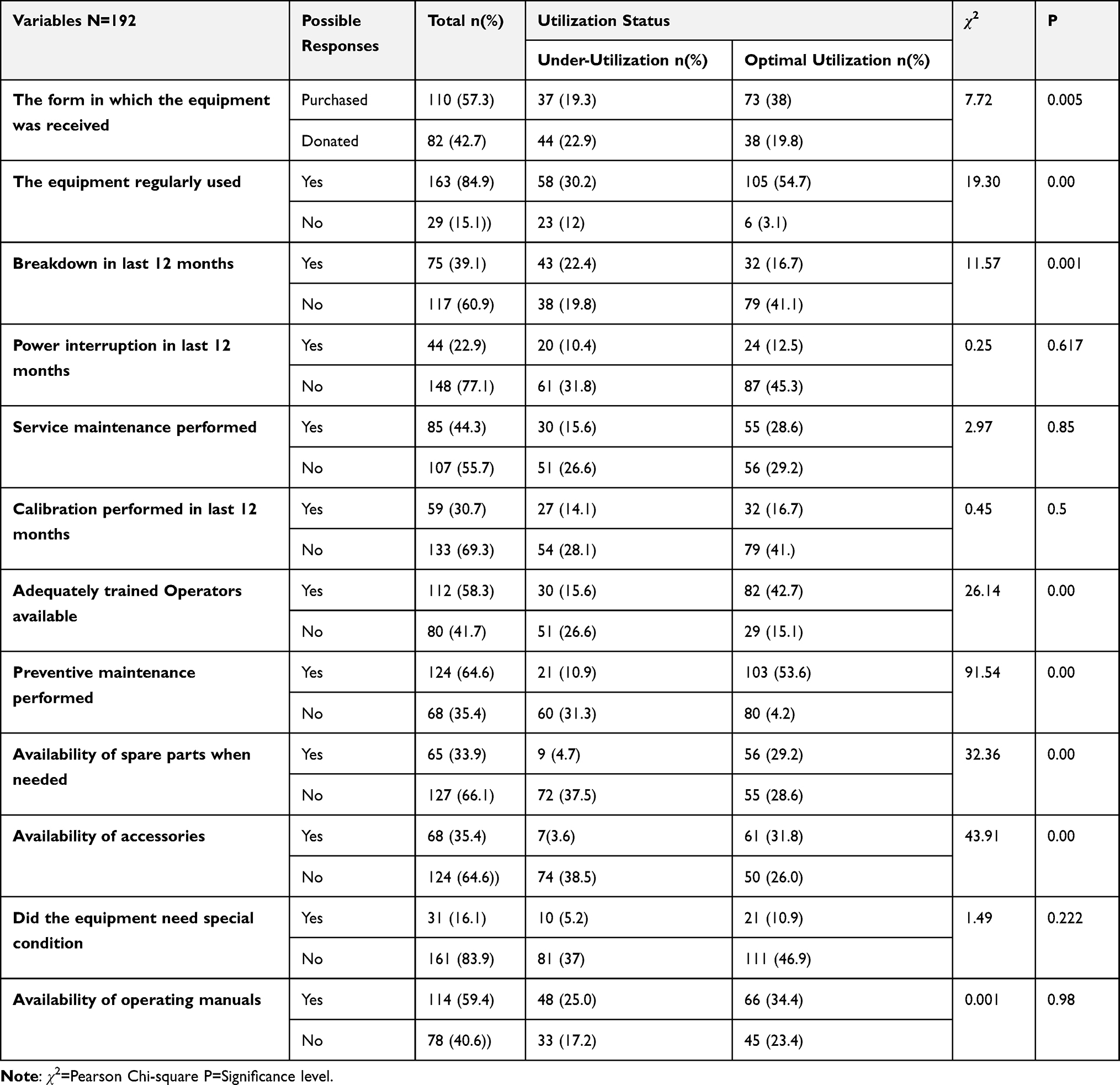 |
Table 1 Factors Influencing Efficient Utilization of Medical Equipment at Public Referral Hospitals, in East Wollega, Oromia Regional State, Ethiopia, 2021 |
Discussion
The utilization index is a crucial factor in determining how well equipment is being serviced or tracking its functioning state. An appropriate use of the equipment will lead to the best patient handling, a quick turn-around, the lowest cost, high-quality patient care, and satisfied patients.18 The utilization coefficient and variables influencing effective utilization in public referral hospitals were thus identified by the study.
Based on the utilization coefficient, which was 57.8% and showed that around 42.2% of the equipment were inefficiently used in the hospitals, the study calculated the degree of medical equipment usage. The level of UC was calculated to be 0.49 using the 95% CI interval (0.44–0.55). The survey also revealed that at least 2 out of 5 items of medical equipment were not being used to their full potential.
This finding is almost identical to WHO estimates that around 50% of medical equipment in developing countries is not functioning and is not used correctly and optimally,13 and high-quality life-saving medical devices are inaccessible to the vast majority of health facilities in Africa. 40% of equipment physically in the possession of low-resource hospitals all over the world is not usable,15 and 41% of equipment in first-level hospitals studied in Nigeria did not have a functioning radiograph.20
This extremely high underutilization of medical equipment is contrasted with study results from China, which revealed that 77% of the equipment under consideration had an appropriate UC and that just 33% of the equipment used for medical diagnostics was underused.3 This discrepancy can be brought on by the standard of the study hospitals and the operating staff’s training there.
As opposed to earlier study in India, which found that almost 50% of this medical equipment was underused, the results showed that the degree of underutilization of medical equipment in the study institutions was lower.7 The study done in India concentrated on dental institutions, but the current study estimated the utilization level of all medical equipment used for diagnosis and treatment monitoring purposes in the study hospitals. This discrepancy may be the result of the study institutions utilized.
According to the study conducted in Ethiopia, roughly 25% were not functioning during the time of the investigation. Similar to this, a study done in various hospitals in Ethiopia revealed that 35.2% of the available equipment at Shenen Gibe General Hospital and 32% of those at Jimma University Specialized Hospital were not working.21
The study once more revealed that performing preventive maintenance in accordance with schedule was statistically correlated with the use of medical equipment (χ2 = 91.54; P = 0.00) for about 35.4% pieces of medical equipment. Similar findings were found in the Indian, which revealed that just 33% of medical equipment received routine preventative maintenance.7
The study also identified the factors causing underutilization of medical equipment in the study hospitals, Accordingly, the form in which the hospital received (purchased or donated) the equipment (χ2=7.7.2; P=0.005), the regular availability of the equipment (χ2=19.30; P=0.00), the equipment breakdown in the last 12 months (χ2=11.57; P=0.001) and performing preventive maintenance according to the schedule (χ2 = 91.54; P = 0.00) were the statistically significant associated factors associated with the utilization of the equipment.
Similar to this, the study carried out in Ethiopia identified the following factors as affecting the functionality of the available medical devices: being dependent on donations, a lack or absence of spare parts for donated medical devices, a lack of training while medical devices were installed, taking responsibility to operate machines without the proper training, not being available on the market, power outages, and a lack of maintenance staff.21,22
Similarly, the study done in China also revealed comparable reasons causing underutilization of medical equipment: breakdown, affordability, availability of trained labor, non-availability of consumables and replacements, maintenance delays, limited working hours, and restricted availability.3
The study also found that the statistically significant linked factors with equipment usage were the availability of suitable replacement parts when needed (χ2 = 32.36; P = 0.00) and the availability of accessories (consumables) when needed (χ2 = 43.91; P = 0.00). Similar to the study done in Benin, it was shown that one of the key variables that might influence the availability and usage of medical equipment in healthcare facilities is a shortage of spare parts.16,23
The study found that one important linked factor impacting the effective use of medical equipment was the availability of competent professionals operating the equipment with proper training (χ2 = 26.14; P = 0.00). Similar to this, the World Health Organization found that if a structured and consistent training program is put in place, critical care equipment may be used more efficiently, affordably, and safely.16,22
The study is expected to provide insight and useful information for the efficient utilization of medical equipment in referral hospitals. However, it might be prone to a lack of adequate information on some medical equipment that were available in the study hospitals.
Conclusion
On average, the utilization coefficient of medical equipment in the study hospitals was low compared to other study findings, which indicated that 2 out of 5 pieces of medical equipment were underutilized.
The hospital’s method of acquisition (purchased or donated), the frequency of equipment availability, equipment breakdown, the availability of adequate staff operating the equipment with adequate training, performing preventive maintenance according to the schedule, the availability of adequate spare parts, and the availability of accessories (consumables) were the significant associated factors that could affect the efficient utilization of the equipment.
Therefore, based on its level and demand, each hospital should create an appropriate strategic framework to manage and utilize the medical equipment that is now available. This strategic plan should cover the following topics: the equipment procurement process, taking into account the market’s supply of spare parts and accessories, the hospitals’ demand for the equipment, the form that the equipment can be obtained (purchase or donation), the equipment’s regular availability for daily use, repairs, staff training, and maintenance.
Data Sharing Statement
The corresponding author will provide the data sets produced and/or analyzed during the current investigation upon reasonable request.
Ethics Approval and Consent to Participate
The ethical clearance was obtained from the ethical review committee of Wollega University, Institute of Health Science. The necessary permission was obtained from the East Wollega zonal health department and study hospitals. This study was conducted in accordance with the Declaration of Helsinki. All study participants who were professionals operating the equipment in the study hospitals were well informed about the purpose of the study and informed written consent was secured from the study participants prior to the interview. The study participants’ confidentiality was maintained and no personal identifiers were used in the data collection tools and codes were used in place of it. All paper-based and computer-based data were kept in protected and safe locations. The recorded data were not accessed by a third person, except the research team and data sharing will be enacted based on the ethical and legal rules of data sharing.
Acknowledgments
We would like to acknowledge Wollega University for funding for data collection, Nekemte Specialized Hospital, and Wollega University referral hospital staffs for their due cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Wollega University covered the data collection fees.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Medicines and Health Care Products Regulatory Agency. Medical Devices and Medicinal Products. London: Medicines and Health Care Products Regulatory Agency; 2011:15.
2. World Health Organization. Medical Device Technical Series: Introduction to Medical Equipment Inventory Management. Geneva, Switzerland: World Health Organization Press; 2011.
3. Chaudhary P, Kaul P. Factors affecting utilization of medical diagnostic equipment: a study at a tertiary healthcare setup of Chandigarh. CHRISMED J Health Res. 2015;2:316. doi:10.4103/2348-3334.165741
4. Mengqi H. A study on medical imaging equipment productivity and utilization; 2015.
5. Yan W, Hao Y, Jingsong G, et al. Hospital efficiency and utilization of high-technology medical equipment: A panel data analysis. Health Policy Tech. 2018;7:65–72.
6. Gupta S, Kant S. Hospital Stores Management an Integrated Approach.
7. Gupta V, Gupta N, Sarode GS, Sarode SC, Patil S. Assessment of equipment utilization and maintenance schedule at a dental institution in Bengaluru, India. World J Dent. 2017;8(2):104–108. doi:10.5005/jp-journals-10015-1421
8. Ethiopian Food, Medicine and Health Care Administration and Control Authority (EFMHACA). Ethiopian list of medical instrument with minimum specification. Addis Ababa; 2013. Available from: http://www.fmhaca.gov.et/wp-content/uploads/2019/03/ethopian_list_of_medical_instrument_with_minimum_specification.pdf.
9. Sontea V, Morgoci S, Turcanu G, Pislaru C. Medical devices management strategy in the republic of Moldova. 3rd international conference on nanotechnologies and biomedical engineering; 2016:55. Available from: https://link.springer.com/chapter/10.1007/978-981-287-736-9_113.
10. World Health Organization. Technical discussions Medical devices in contemporary health care systems and services, WHO Regional Committee for the Eastern Mediterranean EM/RC53/Tech.Disc; 2006.
11. World Health Organization. Medical device technical series, Health technology assessment of medical devices; 2011.
12. Epsicom Business Intelligence. Medistat: Medical Devices Market Analysis and Country Profiles. UK: Print Binders; 2003.
13. World Health Organization. Health Technologies: The Backbone of Health Services. Geneva: World Health Organization; 2003.
14. Bryce C, Cline K. The supply and use of selected medical technologies. Health Aff. 1998;17:213–224. doi:10.1377/hlthaff.17.1.213
15. Perry L, Malkin R. Effectiveness of medical equipment donations to improve health systems: how much medical equipment is broken in the developing world? Med Biol Eng Comput. 2011;49:719–722. doi:10.1007/s11517-011-0786-3
16. Ethiopian FMOH. Ethiopian Hospital Reform Implementation Guidelines. Vol. 2. Ethiopian Hospital Management Initiative; 2010.
17. Ethiopian Standard Agency. Ethiopian standard; comprehensive specialized hospital; requirements; 2012.
18. Hospital Equipment Utilization: increasing Operational Efficiency; 2008. Available from: http://www.medicalbuyer.
19. Kumar PN. Utilization study of CT scan in a multi-specialty hospital. Int J Sci Res. 2014;3(7):1–2.
20. Oluwasoga O. Creating affordable access to medical equipment in Africa using system design; 2017. Available from: https://sdm.mit.edu/wp-content/uploads/2017/02/MDAAS-Presentation-3-13-17.pdf.
21. Ademe BW, Tebeje B, Molla A. Availability and utilization of medical devices in Jimma zone hospitals, Southwest Ethiopia: a case study. BMC Health Serv Res. 2016;16:287. doi:10.1186/s12913-016-1523-2
22. World Health Organization. Increasing Complexity of Medical Technology and Consequences for Training and Outcome of Care. World Health Organization; 2010.
23. Houngbo PT, Medenou D, Dakpanon LY, Bunders J, Ruitenberg J.Policy and management of medical devices for the public health care sector in Benin; 2012:320.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.