")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Emotional Distress in a Patients Following Polytrauma
Authors Anghele M, Marina V , Moscu CA, Dragomir L, Anghele AD, Lescai AM
Received 25 January 2023
Accepted for publication 29 March 2023
Published 27 April 2023 Volume 2023:16 Pages 1161—1170
DOI https://doi.org/10.2147/JMDH.S405904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mihaela Anghele,1 Virginia Marina,2 Cosmina Alina Moscu,3 Liliana Dragomir,1 Aurelian-Dumitrache Anghele,2 Alina-Maria Lescai1
1Clinical-Medical Department, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University of Galati, Galati, 800201, Romania; 2Medical Department of Occupational Health, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University of Galati, Galati, 800201, Romania; 3Emergency Hospital, Faculty of Medicine and Pharmacy, “Dunarea de Jos” University of Galati, Galati, 800201, Romania
Correspondence: Virginia Marina, Tel +40-770-89-82-74, Email [email protected]
Introduction: Emotional affectivity can be described under two general dimensions: positive affectivity and negative affectivity. It is often assessed by means of questionnaires completed retrospectively by the subjects. The most common scales used are PANAS, DES, and PANA-X. All these scales are based on the concept of two dimensions, negative and positive affective emotions, respectively. Both dimensions mentioned, positive and negative affectivity, can be associated with a bipolar dimensional entity called pleasant-unpleasant. Specifically, a high level of positive emotions and a low level of negative emotions are associated with pleasant/positive feelings (happiness, well-being, satisfaction, cheerfulness, etc.), while a low level of positive emotions and a high level of negative emotions are associated with negative feelings (sadness, anger, nervousness, depression, anxiety, etc.).
Materials and Methods: This study is an observational and cross-sectional study. The elements that led to the production of the final database were collected by means of a questionnaire, which included 43 items, 39 of which were specific questions found in the affective distress profile. The questionnaire was administered to 145 patients who had suffered polytrauma and were admitted to the Emergency Hospital of Galati in October 2022. The final centralizing tables included the characteristics of 145 patients, aged between 14 and 64 years.
Results: The aim of this study is to identify the level of emotional distress in patients who have suffered polytrauma, so the following scores were evaluated, obtained after the application of PDA: STD, ENF, END. The total distress score was obtained by summing all the negative items found in the PDA questionnaire.
Conclusion: Men show a high level of emotional distress compared to women. Polytrauma has a negative effect on patients’ emotional status, with a worrying prevalence of negative functional and dysfunctional emotions. The level of distress in polytrauma patients is high.
Keywords: emotional distress, polytrauma, affective dysfunctions, emotions
Introduction
According to WHO, “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”.1
Emotional distress and polytrauma are interrelated concepts that can significantly impact an individual’s mental health and overall well-being.2 Polytrauma refers to the experience of multiple traumatic events, which can result in physical and emotional injuries, including PTSD, depression, anxiety, and other mental health conditions.3 In addition to the immediate effects of trauma, polytrauma can lead to long-term physical and mental health complications.4
On the other hand, emotional distress refers to a range of negative emotions and feelings that can arise from trauma, such as fear, anger, sadness, guilt, and shame.4 Emotional distress can impact an individual’s ability to function daily and may require therapeutic interventions.
When an individual experiences polytrauma, they may be at a higher risk of developing emotional distress due to the cumulative impact of multiple traumatic events.4 Emotional distress can also complicate recovery from physical injuries and impair healing.2
Treating emotional distress and polytrauma requires a multidisciplinary approach that may include medical care, therapy, and social support.4 Mental health professionals may use various therapeutic interventions, such as CBT, EMDR, and exposure therapy, to address the emotional distress associated with polytrauma.3 In addition, social support networks and community resources can play a critical role in promoting healing and recovery.2
It is essential to recognize the interconnectedness of emotional distress and polytrauma and to provide comprehensive, compassionate care that addresses the unique needs of individuals experiencing these challenges.4
A link between mental and physical health has been identified in the literature.5,6 Non-specific symptoms such as stress, anxiety or depression define the concept of psychological distress. Thus, identifying a high level of psychological distress is associated with decreased mental health and with common mental disorders such as anxiety or depressive disorders.7
The ability to experience states and emotions is a fundamental part of human existence. However, humans differ in the frequency and intensity of these emotions.8,9
Emotional affectivity can be described under two general dimensions: positive affectivity and negative affectivity. It is often assessed by means of questionnaires completed retrospectively by the subjects. The most common scales used are PANAS,10 DES,8 and PANA-X.11 All these scales are based on the concept of two dimensions, negative and positive affective emotions, respectively.
Both dimensions mentioned, positive and negative affectivity, can be associated with a bipolar dimensional entity called pleasant-unpleasant. Specifically, a high level of positive emotions and a low level of negative emotions are associated with pleasant/positive feelings (happiness, well-being, satisfaction, cheerfulness, etc.), while a low level of positive emotions and a high level of negative emotions are associated with negative feelings (sadness, anger, nervousness, depression, anxiety, etc.).12,13 Russell and Carroll (1999) state that the existence of these bipolar dimensions is evidence that PA and PA are not independent of each other.14
General affect as well as specific emotions persist over time. Thus, it can be understood that emotional affect has both global and sub dimensions, characterized by the specific emotions or mood of the individual.8,15
According to information found in the literature, trauma patients frequently show increased levels of anxiety, depression, or other emotional disturbances, both in the short and long term.16–19
Emotional distress includes many negative emotional states, which affect the functional level of patients, often also their interpersonal relationships. The presence of emotional distress can affect rehabilitation outcomes.20 Specifically, depression can reduce patients’ motivation to engage in rehabilitation activities. Subsequently, they may develop anxiety about re-injury which may lead to avoidance of activities in general. Patients may also experience pain associated with polytrauma for a long time, which is associated with avoidance of activities as well as anxiety and depression. Increased levels of emotional distress are associated with increased comorbidity.21
Patients who experience polytrauma are more likely to develop emotional distress than those who experience a single traumatic event. The cumulative impact of multiple traumatic events may lead to more significant emotional distress, such as symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD). Additionally, the severity and nature of the injuries sustained in polytrauma may exacerbate emotional distress, impairing recovery and poorer overall health outcomes. Therefore, the hypothesis is that emotional distress is more prevalent in patients following polytrauma than in those following a single traumatic event.5
The aim of this work is to identify the level of distress in polytrauma patients admitted to the Emergency Hospital of Galati.
Materials and Methods
This is an observational and cross-sectional study. The elements that led to the production of the final database were collected by means of a questionnaire, administered individually, on paper, which included 43 items, 39 of which were specific questions found in the affective distress profile and sociodemographic data. The questionnaire was administered to patients who had suffered polytrauma and were admitted to the Emergency Hospital of Galati in October 2022. The final centralizing tables included the characteristics of 145 patients, aged between 14 and 64 years. Statistical evaluation was performed using SPSS v26 software and Microsoft Excel version 2019.There was only one inclusion criterion in this study, namely the presence of polytrauma in October. No exclusion criteria were applied, as all patients who had polytrauma during this time were invited to answer the questionnaire.
The questionnaire used can be found in Annex 1.
The criteria used to define polytrauma were: Injury severity: The injuries sustained by the person must be severe enough to require hospitalization and potentially involve more than one body system: Complexity: The injuries must be complex, meaning that they require the involvement of multiple medical specialties for treatment; Time frame: The injuries must have occurred within a relatively short time frame, typically within hours to days; Mechanism of injury: The injuries must be the result of a traumatic event, such as a car accident, fall, or explosion; Functional impairment: The injuries must result in functional impairment that significantly affects the person’s ability to perform daily activities or work.
The PDA scale consists of 39 items designed to identify and measure functional and dysfunctional negative emotions as well as positive emotions. It allows the calculation of an overall distress score, which involves summing the values obtained within all items, the calculation of an overall distress score, achieved by summing the values obtained within the negative values. Separate scores can then be calculated for functional negative emotions, dysfunctional negative emotions, and separate scores specifically for worry, anxiety, sadness and depression.
The rating for the 39 items is done by allocating from 1 to 5 points as follows:
- For direct ratings: Not at all=1, Very little=2, Medium=3, A lot=4, Very much=5,
- For reverse ratings: Not at all=5, Very little=4, Medium=3, A lot=2, Very much=1.
The global distress score is obtained by summing the scores for the 26 negative items rated directly and for the 13 positive items rated inversely. Scores can also be calculated on subscales by summing the scores of the items that compose them; in this case, they are scored directly for each subscale. The total distress score is calculated by summing the scores from the 26 negative items, rated directly. The cut-off points for each subscale can be found further in Annex 2 (Annex 2.1; Annex 2.2; Annex 2.3; Annex 2.4).
We used the affective distress profile because it includes items that measure functional negative emotions from the “worry/anxiety” and “sadness/depression” categories and positive emotions. Also, this scale allows the calculation of a general distress score, a negative emotions score, and a positive emotions score, as well as separate scores for “worry”, “anxiety”, “sadness”, and “depression”. The tool’s efficiency increases because it allows both the estimation of a global value of distress and the calculation of separate scores for functional and dysfunctional negative emotions. In addition, compared to other scales, the affective distress profile contains a relatively small number of items formulated in an accessible language, being easy to administer and rate.
The study was carried out with the consent of the local Ethics Committee no:7580/14.04.2020.
Results
In the first instance we assessed the distribution of the research group according to the gender of the subjects. Thus, we observed a quasi-symmetrical distribution between the two genders, males and females (Figure 1).
 |
Figure 1 Distribution of studied group by gender. |
Socio-demographically, this study group predominantly included subjects from urban areas and rural areas. This difference may be due to the high accessibility to health services among urban patients (Figure 2).
 |
Figure 2 Distribution of studied group by background. |
The aim of this study is to identify the level of emotional distress in patients who have suffered polytrauma, so the following scores were evaluated, obtained after the application of PDA: STD, ENF, END.
The total distress score was obtained by summing all the negative items found in the PDA questionnaire (Annex 1).
The level of distress and the prevalence of functional negative emotions within the studied group are presented in Figures 3 and 4.
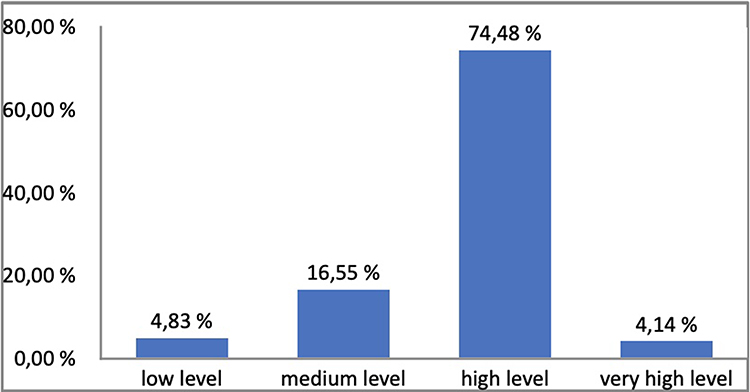 |
Figure 3 Distribution by the level of distress. |
 |
Figure 4 Distribution by the prevalence of functional negative emotions. |
The assessment of dysfunctional negative emotions is shown in Figure 5.
 |
Figure 5 Studied group distribution by dysfunctional negative emotions. |
Next, the interaction between the scores presented above and the gender of the subjects was evaluated and was observed that a certain level of stress is more frequently associated with female or male gender. Following these corroborations, we identified a higher prevalence of a high level of distress among men compared to women. While women showed a higher prevalence of a low level of distress (Table 1). Likewise, high levels of dysfunctional negative emotions were most common, with a higher percentage among men. (Table 1). No very low levels of negative emotions were found. Correlation between subjects’ gender and distress and negative emotions scores are presented in Tables 2–4.
 |
Table 1 Studied Group Distribution by Total Distress Levels, Functional Negative and Dysfunctional Negative Emotions |
 |
Table 2 Interpretation of Total Distress Score and Distribution by Gender |
 |
Table 3 Tabel Interpretation of Functional Negative Emotions and Distribution by Gender |
 |
Table 4 Interpretation of Dysfunctional Negative Emotions and Distribution by Gender |
Also, the highest high level of functional negative emotions was recorded among men. In addition, the most common medium level of negative emotions was recorded among women (Table 3).
In addition, specific statistical tests were applied to this corroboration to determine whether there was a statistically significant dependence relationship between them or, consequently, to identify whether these variables could be independent.
Thus, a chi-square test of independence was conducted to determine whether there was a dependence relationship between the subjects’ gender and their total level of distress. According to these results, there was no statistically significant dependence relationship between the gender of the subjects and the total level of distress (Table 5). Also, no statistically significant relationship could be identified between subjects’ gender and the level of functional.
 |
Table 5 Chi-Square Tests Between Subjects’ Gender and Levels of Distress and Negative Emotions Found in the Group |
Discussion
Several co-occurring injuries are known as polytrauma, a complicated medical disease that affects many people yearly. This illness frequently necessitates long-term medical care and rehabilitation since it can lead to severe physical and emotional anguish. A person’s quality of life can be significantly impacted by the emotional discomfort brought on by polytrauma, which can result in despair, anxiety, and other mental health problems.
Several variables may contribute to the emotional distress polytrauma patients suffer. Physical injuries can cause pain and suffering that can be difficult to manage, which can cause mental anguish and lower quality of life. Further exacerbating emotional suffering is the long-term nature of many polytrauma injuries, which can cause emotions of hopelessness and powerlessness.
According to different studies, polytrauma frequently results in mental distress as a complication. Six months following their injury. More than one-third of those with polytrauma showed signs of depression a year after their injury, according to another study by Bosse et al.22
A person’s psychological well-being may suffer long-term effects from the emotional discomfort brought on by polytrauma. According to 2007 research by Zatzick et al, those who experience emotional distress following a severe injury are more likely to face long-term mental health problems, including PTSD, depression, and drug misuse disorders. They emphasize how crucial early intervention and assistance are for those who have experienced several traumas in order to stop the emergence of persistent mental health issues.23
Six months after their injury, almost 50% of people with polytrauma showed signs of PTSD, according to a study by Skogstad et al. They demonstrate polytrauma’s profound effects on a person’s mental health, even years after the physical wounds have healed.24
People with polytrauma must receive ongoing assistance and care to handle the long-term repercussions of their injuries on their mental health.
Efficient therapies are available to manage the emotional suffering connected to polytrauma. Psychotherapy, medicine, and other types of support are some potential therapies included in the review paper by Piazza and Mozzini. Those who have experienced several traumas must seek out these services as soon as possible to avoid long-term mental discomfort and enhance their quality of life.25
In order to determine the prevalence of psychiatric morbidity following injury, including polytrauma, O’Donnell et al undertook research. The study’s 1,345 participants had an average age of 33. The age distribution in our group was similar, with an average of 35.77. However, in research published in 2010, Glaesmer et al investigated the incidence of PTSD, depression, and somatization in elderly trauma victims, including polytrauma. The study’s 415 participants had an average age of 68.26
Compared to people with less severe injuries, O’Donnell et al discovered that people with polytrauma had higher rates of PTSD (24.2% vs 11.2%), depression (20.3% vs 7.8%), and other mental health problems. The study emphasizes how polytrauma patients’ mental suffering has long-term effects.26 Furthermore, in our research most subjects presented a high level of distress 74.48%. The breakdown of interpretation according to functional and dysfunctional negative emotions showed us that most subjects presented a high level of negative emotions. Moreover, Glaesmer et al observed that over half of the individuals (49.4%) had symptoms of at least one of these diseases, the researchers discovered, indicating that PTSD, depression, and somatization were strongly comorbid. The study emphasizes the possibility of emotional discomfort harming the quality of life, especially in older persons.27
In order to better understand the association between emotional distress, pain perception, and disability in people with polytrauma, Schwarzer et al undertook research.6 The average age of the 214 participants in the research was 45, closer to the median age identified above.6
Even after accounting for other variables, such as age and the severity of the injury, the researchers discovered that emotional distress was a significant predictor of pain intensity and impairment. The study emphasizes the value of psychological therapies for those who have experienced several traumas to manage emotional discomfort and enhance physical performance.
In order to determine the prevalence of PTSD in people who had injuries treated in an emergency room, including polytrauma, Skogstad et al carried out the research. The average age of the 510 participants in the research was 37 years. Six months after their injury, approximately 50% of those with polytrauma reported having PTSD symptoms, according to the study. In order to manage the long-term repercussions of their injuries on their mental health, the study emphasizes the high incidence of PTSD among those who have experienced polytrauma and the necessity for continuing assistance and therapy.24
Overall, these studies offer important new information about the incidence and long-term effects of emotional distress in people with polytrauma. These studies’ findings emphasize the high frequency of mental health conditions, such as PTSD and depression, in people who have experienced several traumas and the possible adverse effects of emotional distress on physical health and functioning. These results highlight the significance of early detection and treatment of emotional distress in this group to avoid the emergence of chronic mental health disorders and enhance overall results.
Following the statistical analysis presented in the results chapter, we could not identify a statistically significant relationship between the gender of the subjects and the results obtained from the PDA. However, as can be seen, men had the highest values for high levels of dysfunctional negative emotions and high levels of distress, while women had higher values than men for high levels of functional negative emotions, medium levels of dysfunctional negative emotions and low levels of distress. These results are different from those found in the literature, which finds emotional distress predominantly in females.28
Conclusion
In the 21st century, the term stress has come to encompass both eustress and distress. Every living organism is subject to eustress, being embedded in the environment. Adapting to the environment, be it favorable, is eustress. Trauma, however, physical or emotional, automatically becomes a stressor. How much the human psyche and subsequently the physical body is affected by this stressor - polytrauma - depends largely on the genetic background of each individual and the coping mechanisms developed by adulthood.
The endocrinologist Hans Selye refers to these coping mechanisms as General Adaptation Syndrome, based on alarm, resilience and exhaustion. From the study we observe that organisms subjected to polytrauma seem to rapidly outgrow the first two stages of alarm and resistance, being directly recovered in the exhaustion stage. This stage corresponds to long-term distress, with implicit psychosomatic damage. It is impossible for the doctor to prevent this phenomenon when interacting with the polytrauma patient. The only tools left are empathy, awareness, psychological support and prevention of the development of psychiatric pathologies due to worsening anxiety and depression. In this regard, we also support the particular importance of the clinical psychologist’s involvement in the treatment of polytrauma, even if initially the patient seems emotionally balanced.
Polytrauma may significantly affect mental health and cause emotional suffering, including PTSD, despair, and anxiety. The long-term nature of many polytrauma injuries can exacerbate emotional distress by causing emotions of helplessness and helplessness. Research has shown that patients with polytrauma have a high frequency of mental health diseases. Early intervention and continued treatment are essential to halt the progression of chronic mental health illnesses and enhance overall outcomes.
There are effective treatments for polytrauma-related mental suffering, including psychotherapy and medication. Research also emphasizes the value of psychological treatments for easing emotional suffering and enhancing physical function in polytrauma patients.
In the current investigation, it was not discovered that gender was a very significant predictor of emotional distress in those who had experienced polytrauma. However, although women tended to have more significant amounts of functioning negative emotions, males typically had higher levels of dysfunctional negative emotions and discomfort.
Overall, these findings highlight the need for more clinical and academic studies to address polytrauma patients’ emotional and mental health requirements. Long-term mental health issues can be avoided, and the quality of life can be improved with early intervention and continued assistance.
Abbreviations
END, dysfunctional negative emotions; ENF, functional negative emotions; PDA, profile of affective dysfunctions; STD, total distress score; PTSD, posttraumatic stress disorder.
Data Sharing Statement
Informed consent was obtained from all subjects involved in the manuscript.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Clinical Emergency Hospital, Galati, Romania. (Project identification code: 479/01/2021).
Consent to Publish
Written informed consent has been obtained from all patients to publish this paper.
Declarations
This is research study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution acquisition of data, analysis and interpretation, or in all these areas; took part.
In drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
V.M.-has made the conception, wrote the final form of article and corresponding author -email: [email protected], M.A.-wrote article and data acquisition; C. A. M- formal analysis; L.D - interpretation of data; A.D.D - data analysis and has drafted the work A.M.L - revised the article.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. OMS, Constitution of the World Health Organization, World Health Organization. Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. World Health Organization; 2006. Available from: https://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1.
2. Brewin CR. Re-experiencing traumatic events in PTSD: new avenues in research on intrusive memories and flashbacks. Eur J Psychotraumatol. 2018;9(1):1412262. doi:10.1080/20008198.2018.1412262
3. American Psychological Association. Trauma; 2021. Available from: https://www.apa.org/topics/trauma.
4. LeardMann CA, Smith B, Smith TC, Wells TS, Ryan MA, Boyko EJ. Post-traumatic stress disorder and depression among U.S. military health care professionals deployed in support of combat operations in Iraq and Afghanistan. Mil Med. 2020;185(9–10):e1442–e1449. doi:10.1093/milmed/usaa157
5. Elliott P, Rai G, McKinley W. Traumatic brain injury and polytrauma: a review and rehabilitation strategies. Adv Mind Body Med. 2011;25(3):12–20.
6. Schwarzer A, Ziegler M, Lücke C, Eich W, Münchberg K. The influence of emotional distress on pain perception and disability in patients with polytrauma. Disabil Rehabil. 2014;36(6):476–482. doi:10.3109/09638288.2013.796832
7. Cuijpers P, Smits N, Donker T, ten Have M, de Graaf R. Screening for mood and anxiety disorders with the five-item, the three-item, and the two-item mental health inventory. Psychiatry Res. 2009;168:250–255. doi:10.1016/j.psychres.2008.05.012
8. Izard CE, Libero DZ, Putnam P, Haynes OM. Stability of emotion experiences and their relations to traits of personality. J Pers Soc Psychol. 1993;64:847–860. doi:10.1037/0022-3514.64.5.847
9. Revelle W, Scherer KR. Personality and emotion. In: Sander D, Scherer KR, editors. Oxford Companion to the Affective Sciences. Oxford: Oxford University Press; 2009.
10. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54:1063–1070. doi:10.1037/0022-3514.54.6.1063
11. Watson D, Clark LA. The PANAS-X: manual for the positive and negative affect schedule – expanded form; 1994b. Available from: http://ir.uiowa.edu/cgi/viewcontent.cgiarticle=1011&context=psychology_pubs.
12. Watson D, Tellegen A. Toward a consensual structure of mood. Psychol Bull. 1985;98:219–235. doi:10.1037/0033-2909.98.2.219
13. Watson D, Wiese D, Vaidya J, Tellegen A. The two general activation systems of affect: structural findings, evolutionary considerations, and psychobiological evidence. J Pers Soc Psychol. 1999;76:820–838. doi:10.1037/0022-3514.76.5.820
14. Russell JA, Carroll JM. The phoenix of bipolarity: reply to Watson and Tellegen. Psychol Bull. 1999;125:611–617. doi:10.1037/0033-2909.125.5.611
15. Watson D. Mood and Temperament. New York: Guilford Press; 2000.
16. Becher S, Smith M, Ziran B. Orthopedic trauma patients and depression: a prospective cohort. J Orthop Trauma. 2014;28:e242–e246. doi:10.1097/BOT.0000000000000128
17. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB. Outcome after major trauma: 12-month and 18-month follow-up results from the trauma recovery project. J Trauma. 2014;46:765–771. doi:10.1097/00005373-199905000-00003
18. Sutherland AG, Suttie S, Alexander DA, Hutchison JD. The mind continues to matter: psychologic and physical recovery 5 years after musculoskeletal trauma. J Orthop Trauma. 2011;25:228–232. doi:10.1097/BOT.0b013e3181ee40a9
19. Vranceanu AM, Bachoura A, Weening A, Vrahas M, Smith RM, Ring D. Psychological factors predict disability and pain intensity after skeletal trauma. J Bone Joint Surg Am. 2014;96:e20. doi:10.2106/JBJS.L.00479
20. Oude Voshaar RC, Banerjee S, Horan M, et al. Fear of falling more important than pain and depression for functional recovery after surgery for hip fracture in older people. Psych Med. 2006;36:1635–1645. doi:10.1017/S0033291706008270
21. Menendez ME, Neuhaus V, Bot AG, Vrahas MS, Ring D. Do psychiatric comorbidities influence inpatient death, adverse events, and discharge after lower extremity fractures? Clin Orthop Relat Res. 2013;471:3336–3348. doi:10.1007/s11999-013-3138-9
22. Bosse MJ, MacKenzie EJ, Kellam JF, et al. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002;347(24):1924–1931. doi:10.1056/NEJMoa012604
23. Zatzick DF, Russo J, Katon W, Sabin JA, Rivara FP. The development and testing of a new screening instrument for use in individuals with acute traumatic injury. Psychosomatics. 2003;44(5):408–419. doi:10.1176/appi.psy.44.5.408
24. Skogstad L, Heir T, Hauff E, Ekeberg Ø. Posttraumatic stress among injured patients treated at an emergency department: one-year follow-up study comparing telephone and in-hospital assessments. J Trauma Stress. 2019;32(5):720–729. doi:10.1002/jts.22451
25. Piazza MG, Mozzini C. Polytrauma and emotional distress: a review of the literature. J Trauma Acute Care Surg. 2020;89(2):e31–e36. doi:10.1097/ta.0000000000002737
26. O’Donnell ML, Creamer M, Pattison P, Atkin C. Psychiatric morbidity following injury. Am J Psychiatry. 2004;161(2):255–261. doi:10.1176/appi.ajp.161.2.255
27. Glaesmer H, Gunzelmann T, Braehler E, Forstmeier S, Maercker A, TraumaRegister DGU. Posttraumatic stress disorder and its comorbidity with depression and somatisation in the elderly—a German community-based study. Aging Ment Health. 2010;14(4):403–412. doi:10.1080/13607860903483081
28. Matud MP. Gender differences in stress and coping styles. Pers Individ Dif. 2004;37(7):1401–1415. doi:10.1016/j.paid.2004.01.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.