")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Emotional Intelligence and Resilience “PROGRAM” Improves Wellbeing and Stress Management Skills in Preclinical Medical Students
Authors Versel JL, Plezia A, Jennings L, Sontag-Milobsky I, Adams W , Shahid R
Received 5 October 2023
Accepted for publication 17 November 2023
Published 20 November 2023 Volume 2023:14 Pages 1309—1316
DOI https://doi.org/10.2147/AMEP.S437053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Julia L Versel,1 Alexandra Plezia,1 Lauren Jennings,1 Isaac Sontag-Milobsky,1 William Adams,2 Ramzan Shahid1,3
1Loyola University Chicago Stritch School of Medicine, Maywood, IL, USA; 2Department of Medicine, Loyola University Chicago, Maywood, IL, USA; 3Department of Pediatrics, Stritch School of Medicine, Loyola University Medical Center, Maywood, IL, USA
Correspondence: Ramzan Shahid, Department of Pediatrics Loyola University Medical Center, 2160 South First Ave, Maywood, IL, 60153, USA, Tel +1 708 327 9125, Fax +1 708327 9132, Email [email protected]
Purpose: The purpose of this study was to determine if implementation of a new educational curriculum focusing on Emotional Intelligence (EI) and Resilience improved second year medical student scores in these areas.
Methods: Our EI-Resilience curriculum was offered as an elective for second year medical students to voluntarily enroll in. The elective consisted of six 2-hour sessions taught by a single faculty member over eight months. Sessions focused on development of EI skills and teaching a Resilience “PROGRAM” (Positive thinking, Reframing, Optimism, Gratitude, Reflection, Altruism, Meaning). Participants’ EI levels were assessed before and after the elective using the Bar-On Emotional Quotient Inventory 2.0 (EQ-i 2.0).
Results: Over a period of 2 years, 70 students participated in the elective. The overall mean EI score significantly improved after the educational elective (100.05 ± 12.94 versus 108.14 ± 12.36, p < 0.001). Compared to the baseline scores, there was significant improvement in all EI components, including all five composite scales, all fifteen content subscales, and the well-being score (all p < 0.05). In a post-intervention survey assessing student perception of the elective, most students found the elective to be helpful (95%, 64/67), most students felt the elective should continue to be available for future students (95%, 64/67), and most would recommend the elective to other students (93%, 62/67).
Conclusion: An EI-Resilience curriculum offered as an elective to second year medical students was well received by students. Our outcomes showed significant improvement in students’ EI scores and all sub-scores, including all components of the stress management composite and well-being score. Teaching EI skills and Resilience strategies in the preclinical setting might be an opportune time for this type of educational intervention.
Keywords: wellness, medical education, curriculum, elective
A Letter to the Editor has been published for this article.
Introduction
In the ever-evolving landscape of medical education, the focus on holistic development of future physicians has gained increasing attention.1,2 In addition to academic excellence, emotional intelligence (EI), resilience, professionalism, and communication skills have emerged as important attributes for healthcare providers, enabling them to navigate the challenges and emotional demands of their profession and provide compassionate patient care.3–5
EI refers to the ability to perceive, understand, and manage emotions, both in oneself and in others. Several models of EI have been proposed, each highlighting different dimensions of this multifaceted construct.6–9 Overall, EI encompasses a set of skills that include self-awareness, social awareness, self-management, and relationship management.10 EI enables individuals to recognize and regulate emotions, develop empathy, and engage in meaningful interpersonal interactions. Resilience is closely linked with EI, and refers to the capacity to withstand adversity, maintain a sense of well-being, and cope with challenges inherent in medical practice.3
Several studies have underscored the importance of EI and resilience in medicine, as both have been associated with improved patient care, reduced burnout, improved job satisfaction, and increased patient satisfaction.5,11–15 Therefore, cultivating EI and resilience skills in medical school may positively contribute to patient care and professional fulfillment.
The growing recognition of EI’s importance in the development of well-rounded and empathetic future physicians has prompted calls to consider its integration into medical school admissions criteria.4 Moreover, the significance of EI in medical education is underscored by its alignment with key competencies emphasized by medical governing bodies, including the Liaison Committee on Medical Education (LCME) and American Council for Graduate Medical Education (ACGME).16,17
Since EI can be taught and improved, educational interventions aimed at teaching these skills have gained increased recognition in medical education.18–20 However, it remains unclear how to best incorporate EI training into medical education curricula. Furthermore, despite the growing body of literature on EI in medical education, few formalized curricula exist to hone these skills in medical trainees, especially at the preclinical medical student level. Consequently, there remains a need to further explore EI and resilience interventions at the undergraduate medical education level in order to best harness their potential to allow medical students to thrive in their roles as future physicians.
We aim to address this gap by describing a novel multi-session EI-Resilience curriculum offered as an elective for preclinical medical students. The elective curriculum focused on developing EI skills and teaching a Resilience “PROGRAM” (Positive thinking, Reframing, Optimism, Gratitude, Reflection, Altruism, Meaning). We investigate the impact of this “PROGRAM” on students’ EI levels, resilience, and well-being. By focusing on pre-clinical undergraduate medical students, our research offers valuable insights into the potential benefits of introducing EI training early on in medical education. Through this study, we aim to contribute to the growing body of evidence supporting the integration of EI training in medical education, with the ultimate goal of enhancing the well-being and effectiveness of future medical professionals.
Methods
A curriculum for a new elective entitled Emotional Intelligence-Resilience Elective was developed and implemented for second-year medical students over the 2021–2022 and 2022–2023 academic years at a US allopathic medical school. The elective consisted of six sessions delivered longitudinally across the year to preclinical students. All incoming second-year medical students were eligible to voluntarily enroll in the elective.
Each session was delivered in-person and lasted two hours in length with additional pre-session and post-session reading, asynchronous lecture recordings, and/or assignments related to each session. Elective sessions were led by one experienced faculty member who facilitated all elective sessions, and two medical students participating in the elective also served as teaching assistants for administrative and logistics coordination.
Each elective session focused on specific topics relevant to EI and resilience, including positive thinking, reframing, optimism, gratitude, reflection, altruism, service, finding meaning and purpose, social support, relationships, mentorship, self-care skills, mindfulness, and self-compassion. Each session also included several self-care and resilience-building post-session exercises and assignments for students to practice building their skills between course sessions (Table 1).
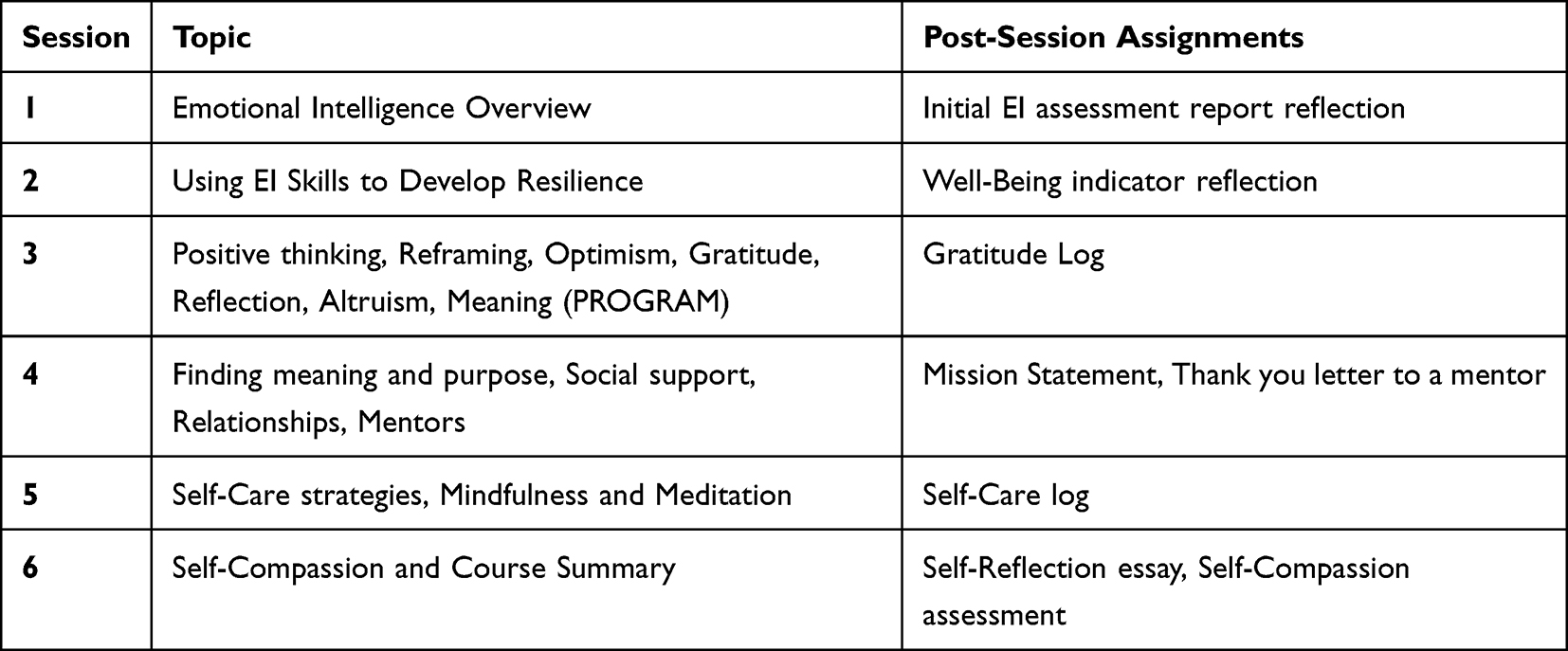 |
Table 1 Overview of Elective Curriculum |
Students completed two surveys at the beginning and end of the curriculum each year. Students were provided their own reports to review for their own personal development and educational benefit as a part of the course curriculum. Prior to group analyses, responses were de-identified by a third-party representative to ensure anonymity and confidentiality.
To evaluate EI and resilience skills, we used the Bar-On Emotional Quotient Inventory 2.0 (EQ-i 2.0®) assessment tool, a validated and reliable tool developed to assess the Bar-On model of emotional-social intelligence.21 This EI inventory is a 133-item self-report assessment that measure EI using one cumulative score, five composite scores, and 15 content subscale scores. The assessment uses a 5-point Likert scale per item (1=never; 5=always), and scores are standardized to a national mean of 100 and a standard deviation of 15. EI was evaluated using all sections, and the stress management composite score and related content subscales were used as an indicator of resilience skills.
To evaluate student knowledge of EI skills and use of EI skills in their daily lives, we used an internally developed 10-item survey that used a 5-point Likert scale per item (1=strongly disagree; 5=strongly agree). A post-curriculum survey included five additional items and three free-text comment sections to assess the acceptability and student perception of the elective curriculum.
This study met the criteria for exemption from the Loyola University Chicago Health Sciences Division Institutional Review Board approval; therefore, the requirement for informed consent was waived.
Statistical Analysis
Participants’ EI and survey responses are reported as mean with standard deviation stratified by occasion. We used generalized estimating equation (GEE) models to estimate the mean change in EI responses from pre-intervention to post-intervention (adjusted for respondents’ sex). In these models, we specified a normal distribution with identity link for each EI construct and used an unstructured matrix to account for the participants’ dependent (paired) responses. GEE models were also used to estimate the log odds of stronger agreement to the survey items following the intervention (adjusted for respondents’ sex). In these models, we specified a multinomial distribution with cumulative logit link for each ordinal survey item and used robust (empirical) standard errors to account for the participants’ dependent (paired) responses. All analyses were completed using SAS version 9.4 (Cary, NC).
Results
A total of 70 medical students participated in the EI-Resilience elective during the 2021–2022 and 2022–2023 academic years. Each medical school class is comprised of 170 students; therefore, 20% (70 of 340) of students participated in the elective during these two academic years. Among the 70 students who completed the preintervention surveys and EI assessment, 96% (67 of 70) completed the curriculum and postintervention surveys, and 97% (65 of 67) completed the EI postintervention assessment.
EI scores for preintervention and postintervention assessments are summarized in Table 2. The preintervention mean total EI was 100.05 ± 12.94 and the postintervention mean was 108.14 ± 12.36 (p < 0.001). Compared to the baseline response, there was a significant improvement in all EI scores, including all five composite scales, all fifteen content subscales, and the well-being score (all p < 0.05).
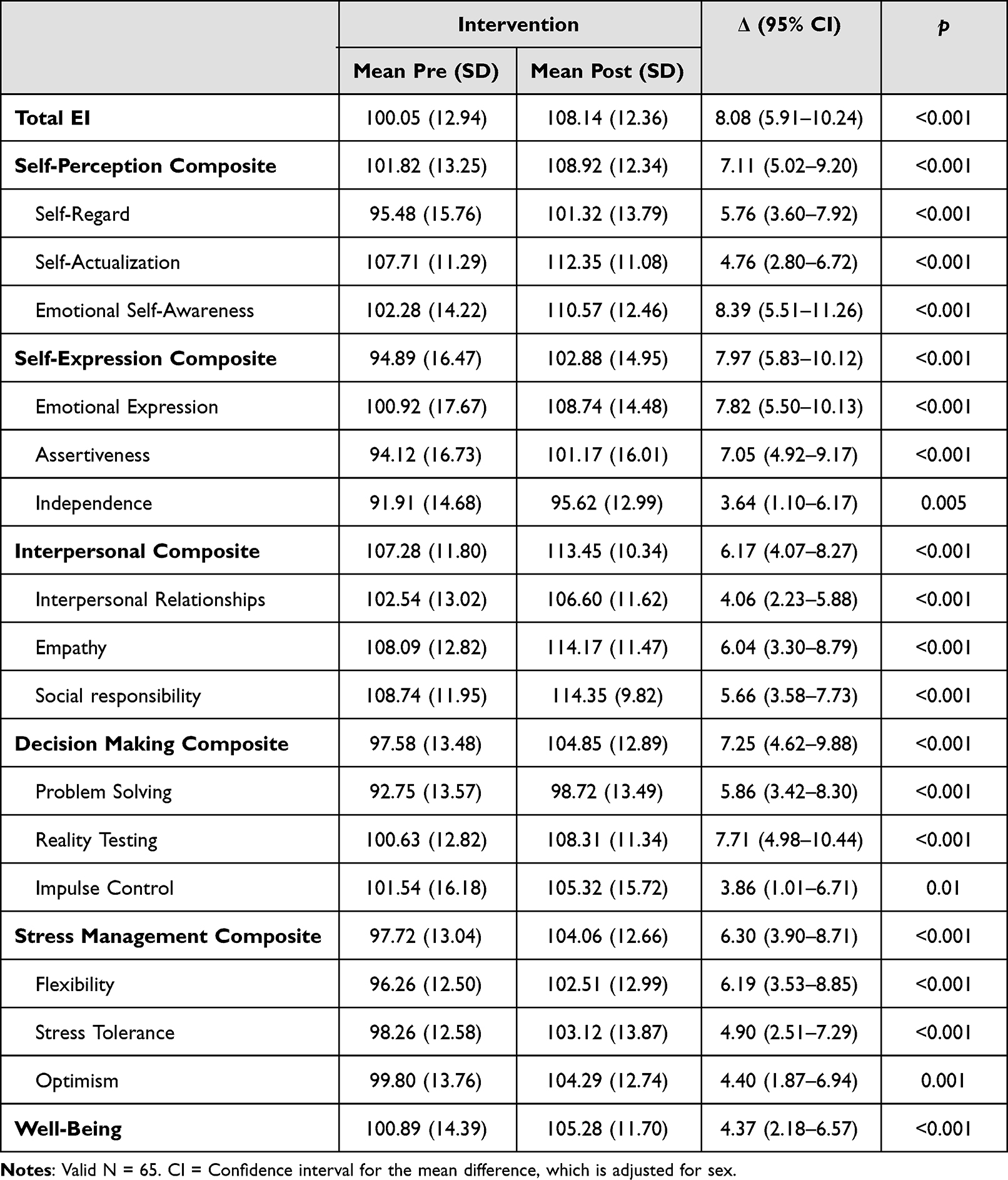 |
Table 2 Change in Emotional Intelligence Scores |
Similarly, student understanding and application of EI significantly increased between the preintervention and postintervention period (Table 3; all p < 0.05). Students reported higher responses (stronger agreement) in their familiarity with the concept of EI, ability to describe how EI can help them in the clinical setting and how it can be a useful skill for doctors, ability to outline strategies to improve their own EI, and frequency of using EI/resilience strategies and thinking about EI when interacting with others. Higher responses were noted for students’ feelings that EI and resilience strategies are an important skill set and in student perception that they have the skills to manage stress and burnout.
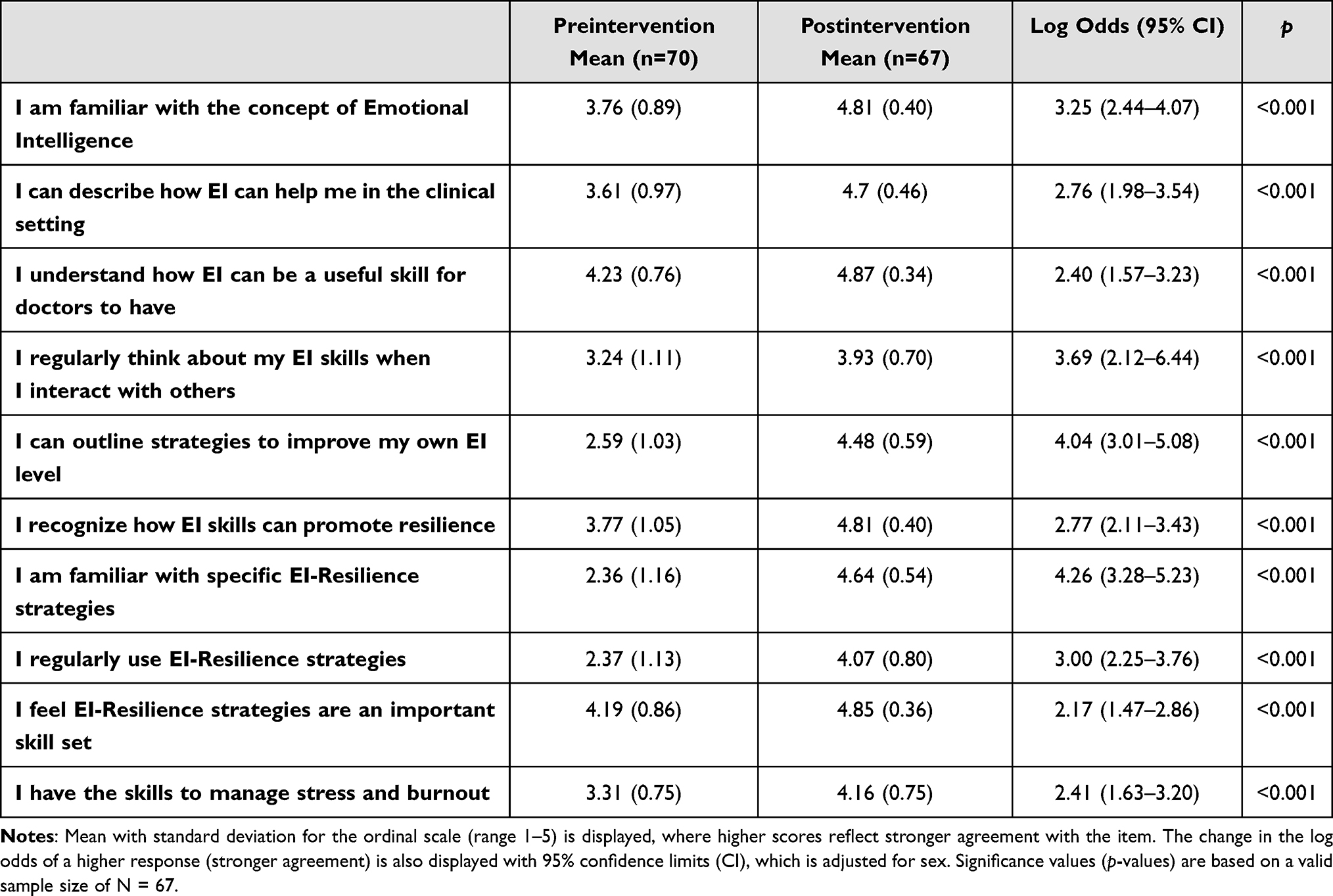 |
Table 3 Change in Survey Response |
In the postintervention evaluation survey, most students (n = 64/67 or 95.5%) stated that the elective should be continued (Table 4). Most students (n = 64/67 or 95.5%) also reported that they plan to use what they learned in the course in the future, and many (n = 60/67 or 89.6%) agreed or strongly agreed that they learned new ways to approach stress and burnout through the elective curriculum. Most students (n = 64/67 or 95.5%) also found the elective helpful and would recommend (n = 62/67 or 92.5%) the elective to other students.
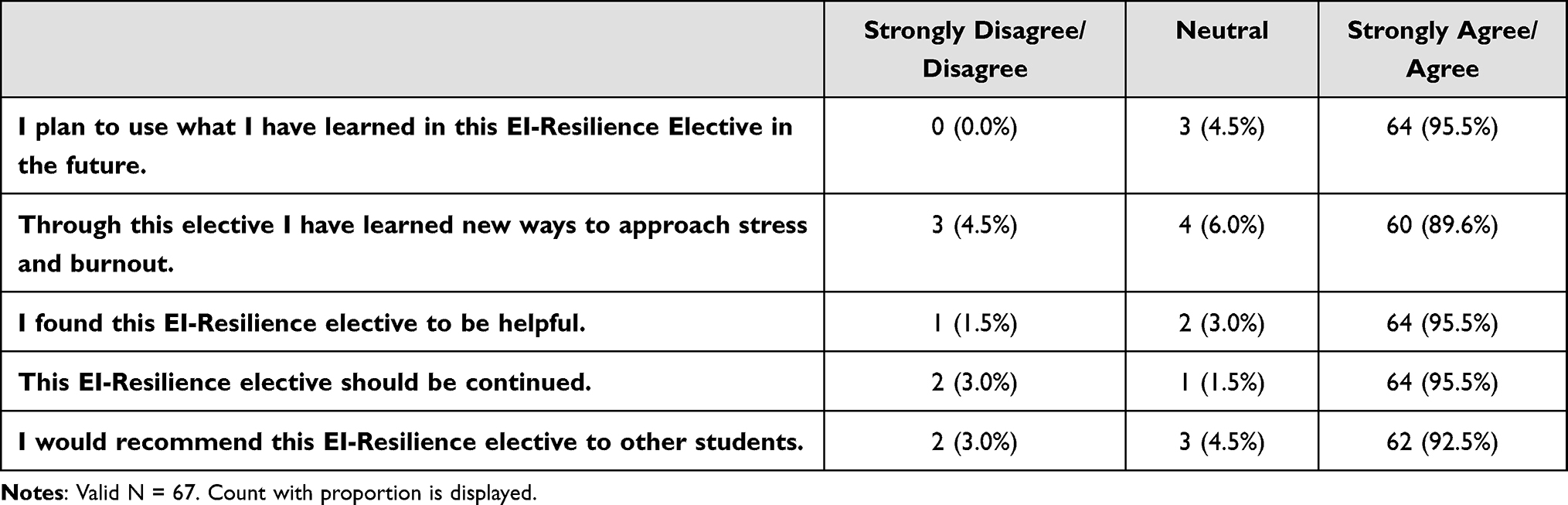 |
Table 4 Postintervention Evaluation Questions |
In the open-ended feedback on the curriculum, participants praised the elective for the opportunities to reflect individually and in group settings, commenting that
being able to intentionally have time and space for these reflections will be sure to serve [students] in [the] future as a person, as a medical student, and as a future physician.
Students commented that they “learned multiple facets to handle burnout and fatigue, demonstrate more resilience, and adopt more strategies for self-care and compassion.” Students also commented on the assignments, stating that they were “so simple but so effective” in facilitating “active reflection, mindfulness, and self-care.” Students noted the course sessions could be improved by allowing for more discussion time and group activities into elective sessions, and providing more resources and reading materials for those interested in learning more about EI and resilience topics.
Discussion
In this study, we implemented an Emotional Intelligence-Resilience curriculum as an elective for preclinical second-year medical students. The curriculum integrated small group reflection activities, take-home assignments, and didactic lectures to enhance EI skills. Our results demonstrate that the intervention was well received by students. We found significant improvements in EI scores and all sub-scores, including all components of the stress management composite and well-being score. Our findings demonstrate that educational interventions can effectively improve EI in medical students, and suggests that EI and resilience skills can be improved in this population.
To our knowledge, this is the first study that has investigated the impact of an EI-Resilience curricular intervention in preclinical undergraduate medical students. Comparing our study with existing literature in undergraduate and graduate medical education, we note several similarities and differences in both interventions and outcomes. Studies in residents across specialties have shown varying outcomes in EI after specific interventions to teach EI and resilience skills. Some studies have shown increases in EI scores, resilience measures, or related outcomes whereas several others have had no differences or even decreases in EI associated outcomes at following curricular interventions.22–25 Similarly, studies in medical students show varying degrees of improvements in EI, wellbeing, or resilience at the end of different interventions.26–31 It is important to note that variability in interventions, study populations, and outcomes measured make it difficult to directly compare our study with prior literature.
We postulate that several unique aspects of our study design may have contributed to its success in improving EI and related resilience scores across all measured outcomes. Firstly, our curriculum was delivered in the preclinical phase, specifically to second-year medical students. Research previously suggests that the third-year of medical school stage of medical education may be an ideal “sweet spot” to teach EI skills.32,33 Here, we show that this ‘sweet spot’ may even be as early as preclinical years of medical school when students’ willingness to engage in an EI curriculum may contribute to its effectiveness. Another factor that might have contributed to the success of our intervention was the use of self-selected participants. Students who enrolled in the elective may have had a prior interest in or motivation to learn about EI and resilience. This self-selection process could have resulted in a more engaged and receptive cohort, which may have amplified the curriculum’s impact. Furthermore, the longitudinal nature of the course, spanning the entire academic year, allowed for consistent exposure to EI concepts, potentially reinforcing learning points and fostering deeper integration of EI skills.
However, we must acknowledge several limitations of our study. First, in this single-arm design, the lack of a control group limits the internal validity of the intervention’s effects and we are unable to adequately determine how EI scores may have differed in a group of students who did not receive the EI and resilience “PROGRAM” intervention. Second, the single-institution study design with a relatively small sample size may restrict the generalizability of the findings to other medical schools. Replicating the study using larger samples across multiple institutions would provide more robust evidence of the intervention’s effectiveness. Moreover, the voluntary enrollment of participants may introduce selection bias, potentially influencing the study’s outcomes. Implementing this curriculum as a mandatory component of the medical school curriculum might offer a different perspective on the impact of the intervention, as other studies have done.25,30 Further, the cost of the EI assessment tool used to evaluate EI and resilience skills may be a financial consideration in scaling this study to a greater sample size. Exploring alternative assessment tools may be beneficial to assess the feasibility of implementing similar interventions on a larger scale.
Looking ahead, future research could focus on assessing the long-term efficacy and lasting effects of our EI and resilience “PROGRAM” on participants’ EI. Exploring whether the improvements in EI observed in preclinical years have lasting effects during clinical training and subsequent medical careers could provide valuable insights into the long-term retention of EI skills and their benefit to clinical contexts.
Conclusion
In conclusion, our study demonstrates a positive impact of a novel EI-Resilience curriculum on preclinical medical students. Teaching EI skills and resilience strategies through a structured “PROGRAM” in the preclinical setting might be an opportune time for this type of educational intervention. We encourage further research to explore the effectiveness of similar interventions across different stages of medical training and diverse student populations. Understanding the long-term effects of EI training on medical students and its influence on their future professional development is essential for fostering emotionally intelligent and resilient physicians.
Ethics Approval and Informed Consent
This study met the criteria for exemption from Institutional Review Board approval; therefore, the requirement for informed consent was waived.
Acknowledgments
The authors wish to thank Gregory Gruener, MD, MBA, MHPE, FANA Vice Dean for Education, Loyola University Chicago Stritch School of Medicine and Claudia Kubnick, Executive Assistant to Gregory Gruener for their support of the Emotional Intelligence-Resilience Elective.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cherry MG, Fletcher I, O’Sullivan H, Shaw N. What impact do structured educational sessions to increase emotional intelligence have on medical students? BEME Guide No 17. Med Teach. 2012;34(1):11–19. doi:10.3109/0142159X.2011.614293
2. Kaplan-Liss E, Lantz-Gefroh V, Bass E, et al. Teaching medical students to communicate with empathy and clarity using improvisation. Academic Med. 2018;93(3):440–443. doi:10.1097/ACM.0000000000002031
3. Boateng A, Aslakson R. Elisabeth Kübler-Ross as Astrophysicist: emotional Intelligence and Resilience Unlock the Black Hole of Physician Burnout, Moral Distress, and Compassion Fatigue. Am J Bioeth. 2019;19(12):54–57. doi:10.1080/15265161.2019.1674423
4. Emanuel EJ, Gudbranson E. Does medicine overemphasize IQ? JAMA. 2018;319(7):651–652. doi:10.1001/jama.2017.20141
5. Mintz LJ, Stoller JK. A systematic review of physician leadership and emotional intelligence. J Grad Med Educ. 2014;6(1):21–31. doi:10.4300/JGME-D-13-00012.1
6. Petrides KV. Trait Emotional Intelligence Questionnaires Manual First Edition Technical Manual for the Trait Emotional Intelligence Questionnaires (TEIQue) First Edition 2 Trait Emotional Intelligence Questionnaire (TEIQue) Technical Manual; 2009. Available from: www.psychometriclab.com.
7. Salovey P, Mayer JD. What is emotional intelligence? In: Emotional Development and Emotional Intelligence. Harper Collins; 1997:3–34.
8. Goleman D. Working with Emotional Intelligence. Bantam Books; 1998.
9. Bar-On R The bar-on model of emotional-social intelligence. Psicothema. 2006; 18 Suppl:13–25.
10. Bradberry T, Greaves J. Emotional Intelligence 2.0. TalentSmart; 2009.
11. Epstein RM, Krasner MS. Physician resilience:: what it means, why it matters, and how to promote it. Acad Med. 2013;88(3):301–303. doi:10.1097/ACM.0b013e318280cff0
12. Hollis RH, Theiss LM, Gullick AA, et al. Emotional intelligence in surgery is associated with resident job satisfaction. J Surg Res. 2017;209:178–183. doi:10.1016/j.jss.2016.10.015
13. Blanchard C, Kravets V, Schenker M, Moore T. Emotional intelligence, burnout, and professional fulfillment in clinical year medical students. Med Teach. 2021;43(9):1063–1069. doi:10.1080/0142159X.2021.1915468
14. Lin DT, Liebert CA, Tran J, Lau JN, Salles A. Emotional intelligence as a predictor of resident well-being. J Am Coll Surg. 2016;223(2):352–358. doi:10.1016/J.JAMCOLLSURG.2016.04.044
15. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45(8):835–842. doi:10.1111/J.1365-2923.2011.03985.X
16. Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N. Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies. Med Educ. 2010;44(8):749–764. doi:10.1111/j.1365-2923.2010.03709.x
17. Kirch DG, Gusic ME, Ast C. Undergraduate medical education and the foundation of physician professionalism. JAMA. 2015;313(18):1797–1798. doi:10.1001/JAMA.2015.4019
18. Satterfield JM, Hughes E. Emotion skills training for medical students: a systematic review. Med Educ. 2007;41(10):935–941. doi:10.1111/j.1365-2923.2007.02835.x
19. Toriello HV, Vande Ridder JMM, Brewer P, et al. Emotional intelligence in undergraduate medical students: a scoping review. Adv Health Sci Educ. 2022;27(1):167–187. doi:10.1007/s10459-021-10079-2
20. Borges NJ, Thompson BM, Roman BJ, et al. Team emotional intelligence, team interactions, and gender in medical students during a psychiatry clerkship. Acad Psychiatry. 2015;39(6):661–663. doi:10.1007/s40596-015-0282-4
21. Bar-On R. Emotional Quotient Inventory 2.0 User’s Handbook. Multi-Health Systems; 2004.
22. Shahid R, Stirling J, Adams W. Promoting wellness and stress management in residents through emotional intelligence training. Adv Med Educ Pract. 2018;9:681–686. doi:10.2147/AMEP.S175299
23. Dugan JW, Weatherly RA, Girod DA, Barber CE, Tsue TT. A longitudinal study of emotional intelligence training for otolaryngology residents and faculty. JAMA Otolaryngol Head Neck Surg. 2014;140(8):720. doi:10.1001/jamaoto.2014.1169
24. Winkel AF, Tristan SB, Dow M, et al. A national curriculum to address professional fulfillment and burnout in OB-GYN residents. J Grad Med Educ. 2020;12(4):461–468. doi:10.4300/JGME-D-19-00728.1
25. Bird AN, Martinchek M, Pincavage AT. A curriculum to enhance resilience in internal medicine interns. J Grad Med Educ. 2017;9(5):600–604. doi:10.4300/JGME-D-16-00554.1
26. Doherty EM, Cronin PA, Offiah G. Emotional intelligence assessment in a graduate entry medical school curriculum. BMC Med Educ. 2013;13(1):38. doi:10.1186/1472-6920-13-38
27. Raut A, Gupta S. Reflection and peer feedback for augmenting emotional intelligence among undergraduate students: a quasi-experimental study from a rural medical college in central India. Educ for Health. 2019;32(1):3. doi:10.4103/efh.EfH_31_17
28. Guseh SH, Chen XP, Johnson NR. Can enriching emotional intelligence improve medical students’ proactivity and adaptability during OB/GYN clerkships? Int J Med Educ. 2015;6:208–212. doi:10.5116/IJME.5658.0A6B
29. Lolaty HA, Ghahari S, Tirgari A, Fard JH. The effect of life skills training on emotional intelligence of the medical sciences students in Iran. Indian J Psychol Med. 2012;34(4):350–354. doi:10.4103/0253-7176.108217
30. Cheung EO, Kwok I, Ludwig AB, et al. Development of a positive psychology program (LAVENDER) for preserving medical student well-being: a single-arm pilot study. Glob Adv Health Med. 2021;10:216495612098848. doi:10.1177/2164956120988481
31. Fletcher I, Leadbetter P, Curran A, O’Sullivan H. A pilot study assessing emotional intelligence training and communication skills with 3rd year medical students. Patient Educ Couns. 2009;76(3):376–379. doi:10.1016/j.pec.2009.07.019
32. Tucker T, Bouvette M, Daly S, Grassau P. Finding the sweet spot: developing, implementing and evaluating a burn out and compassion fatigue intervention for third year medical trainees. Eval Program Plann. 2017;65:106–112. doi:10.1016/J.EVALPROGPLAN.2017.07.006
33. Houpy JC, Lee WW, Woodruff JN, Pincavage AT. Medical student resilience and stressful clinical events during clinical training. Med Educ. 2017;22(1):1320187. doi:10.1080/10872981.2017.1320187
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.