")
Back to Journals » Clinical Audit » Volume 16
Empowering Catchment Health Center to Deliver Comprehensive and Safe Obstetric Care Near Clients’ Home: An Institutional Experience in Ethiopia
Authors Teferi DA , Dadi DK, Hassen IS, Teklemariam BT , Yesufe AA
Received 29 September 2023
Accepted for publication 15 March 2024
Published 20 March 2024 Volume 2024:16 Pages 29—37
DOI https://doi.org/10.2147/CA.S442144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zoka Milan
Dagmawi Anteneh Teferi,1 Dawit Kebede Dadi,1 Ishmael Shemsedin Hassen,2 Berhanetsehay Teklewold Teklemariam,3 Abdu Adem Yesufe1
1Quality Improvement and Clinical Governance Directorate, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Critical Care Medicine Unit, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Endocrine and Breast Surgery Unit, Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Dagmawi Anteneh Teferi, Quality Improvement and Clinical Governance Directorate, St. Paul’s Hospital Millennium Medical College, P.O. Box 1271, Addis Ababa, Ethiopia, Email [email protected]
Background: Three-quarters of maternal deaths can be prevented by proper emergency referral procedures, early recognition of obstetric complications, and timely and adequate care. Nonetheless, lots of women still experience difficulties getting the life-saving emergency obstetric interventions they need promptly.
Aim: Aim to improve maternal service delivery at the highest referring catchment health center to a tertiary teaching hospital through establishing a comprehensive obstetric care from December 2020 to April 2022.
Methods: A pre and post-intervention follow-up study design was employed to evaluate the impact of a quality improvement project at a health center on the access and quality of maternal service. After identifying a highly referring catchment health center, we established a multidisciplinary team responsible for preparing a readiness plan, facilitating staff training on obstetric care, resource mobilization, and continuous supportive supervision.
Results: Caesarian section delivery, holistic obstetric ultrasound service, and comprehensive abortion care were started at the catchment health center. The total monthly delivery at the health center almost quadrupled from 94 to an average of 334, referral out decreased from 156 mothers to a median of 12, and maternal emergency referral-in to the health center from the surrounding health centers increased from zero to a median of 44 mothers. The total number of deliveries at the tertiary hospital decreased from a monthly average of 902 to 827.
Conclusion: Delivering comprehensive obstetric care near the client’s home by empowering the catchment health center has a significant role in reducing unnecessary referrals and costs, overcrowding of tertiary hospitals, and increasing antenatal and postnatal care attendance and institutional delivery.
Strengths and Limitations: Meticulous application of the science of improvement, data interpretation and analysis, and data driven decision-making are the strengths. Being tested in a single health center might make its generalizability questionable and needs further testing on a larger scale.
Keywords: maternal service, cesarean section, comprehensive obstetric care, referral system, catchment health center, prevention of obstetric complications, LMICs
Introduction
Ethiopia has a three-tier healthcare system that categorizes healthcare facilities based on the services it provide and the healthcare facilities are interlinked with a referral system to maintain efficient, timely, safe, effective, equitable, and person-centered care.1
Delivering primary health care is one of the basic and priority areas of focus by healthcare facilities. In low-income countries, improving primary health care is essential to enhance access and quality of health care service delivery.2 Maternal and neonatal services are one of the primary health care services being delivered in health centers and hospitals.3
Between 2000 and 2017 the global maternal mortality ratio decreased by 38%.4 However, hundreds of thousands of mothers are still dying from easily preventable causes.5 Ethiopia has also reduced maternal death from 871 to 412 between 2000 and 2016.6 The reduction of maternal, neonatal, infant, and under-five mortality rates is by large attributable to the utilization of promotive, preventive, and curative primary health care interventions.7 According to a 2019 Ethiopian demographic health survey, coverage of Antenatal Care (ANC) more than four visits was 43%, and delivery by a skilled birth attendant was 50%.8 One of the key strategies encouraged to reduce maternal mortality in low and middle-income countries (LMIC) is timely access to Comprehensive Emergency Obstetric and Newborn Care (CEmONC).9
In 2012, the Federal Ministry of Health took steps to strengthen Addis Ababa’s healthcare system, not only to meet current needs but also to prepare for future demand. This guideline split the cities and surrounding areas into eight hospital-health center referral networks, each with one comprehensive specialized hospital and 7 to 10 nearby health centers, to ensure optimal use of limited healthcare resources.10 The hospital-health center referral networks were organized with the fact that; the majority of deliveries are low-risk and should take place in health centers, while pregnant women who are high-risk and develop complications should be referred to give birth in tertiary hospitals.11 Bypassing the lower levels of health facilities makes an enormous number of patients spend longer waiting time in the hospitals and it also results in inefficient use of highly trained health professionals and resources.12
Government health officials hoped this organization would create efficient use of health services, unburdening the highly accessed specialized hospitals, and increasing the utilization of health centers. Despite the reorganization, cases that could be managed in primary healthcare facilities are being referred to tertiary care facilities leading to suboptimal care in these facilities due to overcrowding.13
Collaboration between facilities within the referral network in terms of human resources, supply, finance, and capacity building can improve the quality of care, patient and staff satisfaction, overall patient cost reduction, and reduction of preventable morbidity and mortality from unnecessary referrals. In addition, continuous follow-up of maternal service in the hospitals showed the need to design a quality improvement project that can enhance the access and quality of maternal service in highly referring low-level referral network facilities. Enabling health centers to deliver comprehensive obstetric care will improve the quality of maternal service delivery by referring selected high-risk patients to tertiary healthcare facilities as shown in Figure 1. Based on our maternal referral audit, health centers located in Burayu town are the leading referring health facilities.
 |
Figure 1 Conceptual framework showing how an improvement science result in an improvement in maternal service delivery by empowering a health center. |
Aim
This project aims to improve maternal service delivery by establishing and sustaining comprehensive emergency obstetric care at the highest referring catchment health center to SPHMMC from December 2020 to April 2022.
Method
The project was conducted by SPHMMC, a tertiary teaching hospital located in Addis Ababa, Ethiopia. Following the maternal service referral audit at SPHMMC, it was found that four health centers located in Burayu town were found to be the leading referral catchment health centers. The project was implemented at Anne Dimma health center, one of the health centers located in Burayu town in collaboration with the SPHMMC quality improvement and clinical governance directorate, and the department of Obstetrics and Gynecology from 1 December 2020 to 30 April 2022.
A multidisciplinary team from the senior management team, quality improvement and clinical governance directorate, obstetrics and gynecology department, anesthesia, liaison, biomedical engineering units, and Anne Dimma health center management team was established to cascade the establishment of a comprehensive obstetric care at Anne Dimma health center. The team is responsible for the identification of gaps, devising solutions, preparation of documents, and follow-up on the performance of the service delivery.
A pre and post-intervention study design was employed to evaluate the impact of establishing and supporting a health center on the access and quality of maternal service.
Project Strategy and Implementation
This project had four phases; initiation, implementation, monitoring and evaluation, and sustainability.
Phase One
In the initiation phase, the project proposal was first presented to the SPHMMC senior management team followed by a project site visit by the senior management team with subsequent approval. Later, a memorandum of understanding between SPHMMC and Anne Dimma health center was signed and a cascade of decisions was made by a multi-disciplinary team (Table 1).
 |
Table 1 Phase One - Initiation of the Project |
Phase Two
Phase two of the project mainly focuses on capacity building, mobilizing required equipment, and installation of operation theatre for Cesarean Section (C/S). After service area redesign and human resources deployment, the project was inaugurated on May 17, 2021 (Table 2).
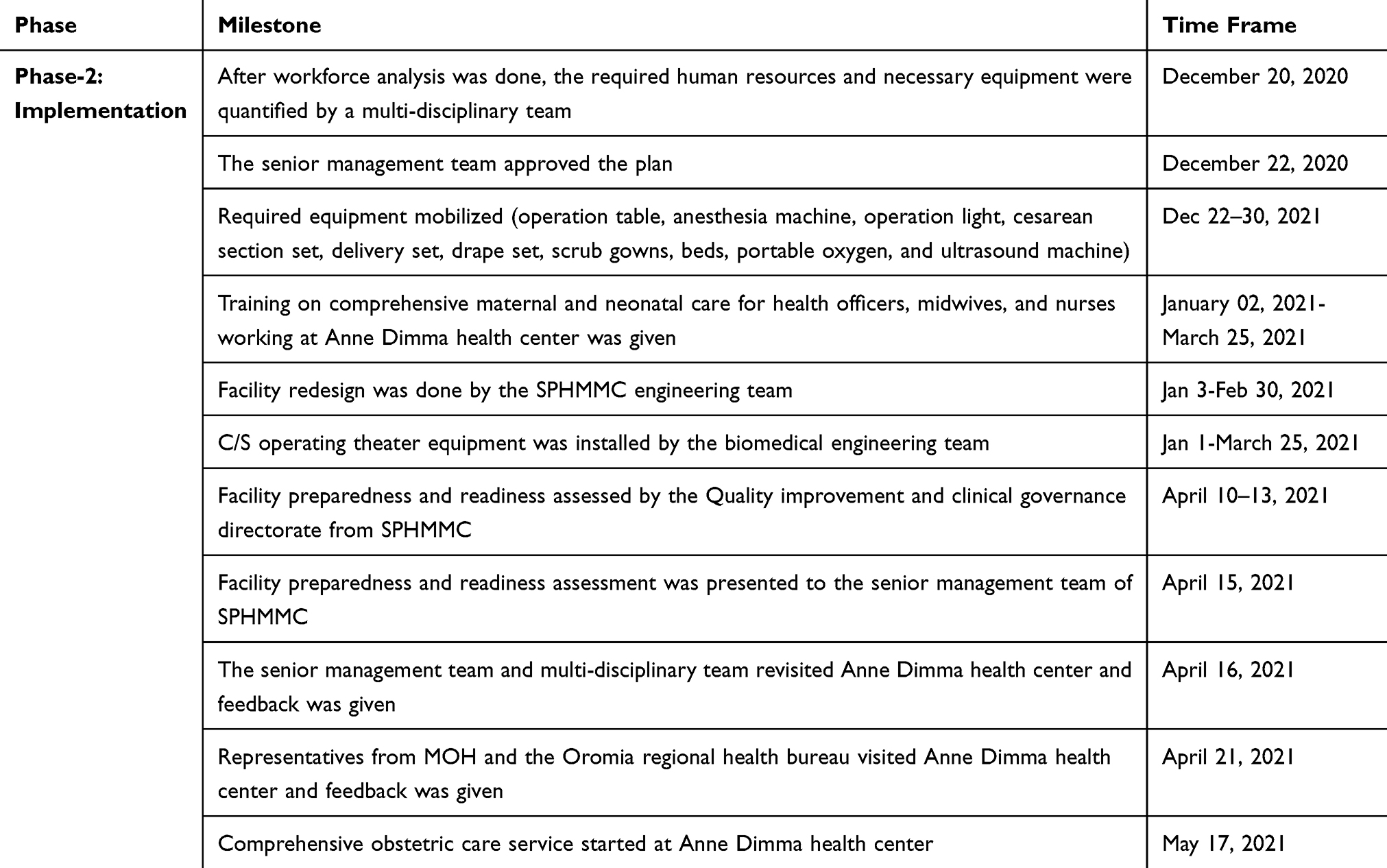 |
Table 2 Phase Two - Implementation Strategy of the Project |
Phase Three and Four
The third phase of the project is monitoring and evaluation of the implementation of the project through continuous supportive supervision and clinical audit. The final phase of the project is to fully make the health center independent of support in terms of supply and human resource exit plan strategy preparation (Table 3).
 |
Table 3 Phase Three and Four – Monitoring & Evaluation and Sustainability Plan |
Result
Anne Dimma health center’s total number of monthly deliveries became 347 from a baseline of 95 while the monthly C/S deliveries became 39 from a baseline of zero after the launching of this project in May 2021 (Figure 2).
 |
Figure 2 Monthly total and cesarean section delivery at Anne Dimma health center from April 2021 to April 2022. Abbreviation: C/S, Cesarean Section. |
SPHMMC’s total number of monthly deliveries and C/S deliveries five months prior to the initiation of this project were 902 and 405 respectively. Following the initiation of the project, the average overall monthly and C/S deliveries became 827 and 374, respectively (Figure 3).
 |
Figure 3 Monthly total and cesarean section deliveries at SPHMMC from December 2020 to April 2022. Abbreviations: C/S, cesarean section; SPHMMC, St. Paul’s Hospital Millennium Medical College. |
Anne Dimma health center’s referral out has decreased to a median of 12 from the baseline of 156 while its emergency maternal referral-in from neighboring health centers has increased to 44 from nil on a monthly basis after the launching of this project in May 2021 (Figure 4).
 |
Figure 4 Total number of monthly maternal referral-out from and referral-in to Anne Dimma health center from April 2021 to April 2022. Abbreviations: R-I, Referral in; R-O, Referral out. |
On average, twenty safe abortions were done at Anne Dimma health center using medical, Manual Vacuum Aspiration, and extraction methods every month after the initiation of this project. The monthly obstetric ultrasound service provided to mothers on antenatal care at Anne Dimma health center became 539 from nil after the launching of this project in May 2021 (Figure 5).
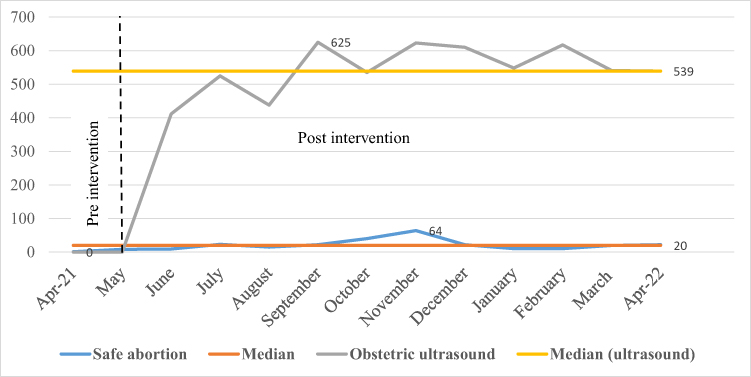 |
Figure 5 Total number of monthly obstetric ultrasounds done for clients who had antenatal follow-up and safe abortion service delivered at Anne Dimma health center from April 2021 to April 2022. |
The average number of pregnant women who received antenatal care at Anne Dimma health center at least once and four times by maternal age became 230 and 198 from a baseline of 56 and 65 respectively from April 2021 to April 2022 (Figure 6).
 |
Figure 6 Total number of pregnant women that received antenatal care at least once and four visits on a monthly basis from April 2021 to April 2022 at Anne Dimma health center. Abbreviation: ANC-Antenatal Care. |
Discussion
Improving access and quality of comprehensive obstetric care based on data-driven evidence at a health center level requires a step-wise approach, coordinated effort, and collaboration to re-innovate the existing structure and sustain service delivery in the long run. There were challenges in each phase of the project: During the initial phase of the project, the major challenges faced were the emergence of the COVID-19 pandemic which hindered resource mobilization, late induction of trained staff to service delivery, and diversion of health facilities’ attention which is similar to challenges paused by COVD-19 pandemic on essential health service in Ethiopia.14 The other challenges were work overload due to the scale-up of services at the health center which was managed by hiring additional staff and financial compensation.
Underperforming autoclave and hematology machines, non-functional chemistry machines, inadequate suturing materials and anesthesia drugs, and low levels of regional and zonal health bureau engagement to support the health center were the other major setbacks that affected the sustainability of the project. It was managed by corrective maintenance of equipment by the biomedical engineering team from SPHMMC, outsourcing sterilization, laundry, and laboratory services freely at SPHMMC to avoid service interruption in the health center.
Following the establishment and initiation of comprehensive obstetric care at Anne Dimma health center, maternal service provision has shown a dramatic increment in the health center while the labor and delivery burden at SPHMMC has shown a reduction. In the later phase of the project, the labor and delivery service at SPHMMC has increased despite the continuation of service delivery at Anne Dimma, which could be due to the assignment of additional catchment health centers to the SPHMMC because of the re-innovation of one of the major referral hospital in Addis Ababa referral network starting from February 2022.
The strength of this project is the presence of strong leadership roles from the senior management team of SPHMMC and Anne Dimma health center, the presence of motivated staff working at Anne Dimma health center to adapt themselves easily to the new environment and the workload, strong and uninterrupted communication between SPHMMC and Anne Dimma health center, and continuous supportive supervision and evaluation system enable the project to be impactful. In addition, meticulous application of the science of improvement, data interpretation and analysis, and decision-making based on the facts are the strengths of this project.
Being tested in a single health center only might make its generalizability questionable and need further testing on a larger scale. However, as far as we follow the improvement science which dictates data-driven change that targets building a system could make this kind of project reproducible locally or universally.
Conclusion and Recommendation
This project taught us that strengthening catchment health centers can significantly reduce unnecessary and delayed referrals, promote institutional maternal delivery, increase antenatal care attendance, ensure equitability of obstetric service, and cost containment. Starting cesarean delivery in our highly referring catchment health center with a collaborative approach also helps the mothers to get the service in their vicinity without affecting the quality of service.
Tertiary hospital overcrowding can be minimized by supporting and empowering catchment health centers and hospitals. Therefore, similar projects should be planned and implemented by other hospitals to improve access and quality of service delivery. Strong engagement of the Oromia health bureau to ensure the sustainability of service is very crucial, particularly in the annual budget allocation to the Anne Dimma health center. Lastly, a comprehensive neonatal care service should be preplanned and integrated with comprehensive obstetric care to improve the outcome of the newborns as both services are inseparable.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The current manuscript got ethical approval from St. Paul’s Hospital Millennium Medical College institutional review board (IRB).
Further, informed consent for publication was obtained from the two institutions as the data is institution-specific rather than individual information that the data will be published in an international journal. Consent to participate for individual participants was waived by St. Paul’s Hospital Millennium Medical College IRB. The collected data is kept confidential by the primary investigator and co-investigators. All methods were carried out in accordance with the relevant guidelines and regulations.
Acknowledgments
The authors acknowledge SPHMMC- IRB for timely ethical evaluation and approval. The authors also acknowledge the hospital management, staff of the obstetrics and gynecology department of SPHMMC, and staff of Anne Dimma health center for their cooperation during data collection and willingness to provide the necessary information.
Author Information
Dagmawi Anteneh Teferi, Dawit Kebede Dadi, Ishmael Shemsedin Hassen, Berhanetsehay Teklewold, and Abdu Adem Yesufe work at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Funding
There is no source of funding for the current manuscript.
Disclosure
All authors read and approved the final manuscript. The authors declare that they have no competing interests.
References
1. FMOH. Health sector transformation plan (2015/16–2019/20), Ethiopia. Federal Ministry of Health Addis Ababa; 2015.
2. van Weel C, Kidd MR. Why strengthening primary health care is essential to achieving universal health coverage. CMAJ. 2018;190(15):E463–E466. doi:10.1503/cmaj.170784
3. UNICEF. Levels & trends in child mortality: report 2017. UNICEF, WHO, the World Bank, United Nations Population Division New York: UNICEF on behalf of the UN Inter-agency Group for Child Mortality Estimation. UNICEF; 2017.
4. World Health Organization. Trends in maternal mortality: 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2019.
5. World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs Sustainable Development Goals. Geneva: World Health Organization; 2018.
6. CSA. Ethiopia Demographic and Health Survey 2016: key indicators report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
7. Wendimagegn NF, Bezuidenhout MC. Integrating promotive, preventive, and curative health care services at hospitals and health centers in Addis Ababa, Ethiopia. J Multidiscip Healthc. 2019;12:243–255. doi:10.2147/JMDH.S193370
8. EPHI. Ethiopia mini demographic and health survey 2019: key indicators. Central Statistical Agency; 2019.
9. Biadgo A, Legesse A, Estifanos AS. Estifanos A.S. Quality of maternal and newborn health care in Ethiopia: a cross-sectional study. BMC Health Serv Res. 2021;21(1):679. doi:10.1186/s12913-021-06680-1
10. Maternal Health Task Force. Strengthening the Maternal Health Care System in Ethiopia, women and health initiative. Harvard T.H. Chan School of Public Health; 2012.
11. Singh S, Doyle P, Campbell OMR, et al. Management and referral for high-risk conditions and complications during the antenatal period: knowledge, practice and attitude survey of providers in rural public healthcare in two states of India. Reprod Health. 2019;16(1):100. doi:10.1186/s12978-019-0765-y
12. Osibogun A. The role of health center in the rational use of health resources.
13. Millar K. How to create well-coordinated change to save women’s lives. Women and Health Initiative, Harvard T.H. Chan School of Public Health; 2015.
14. Mebratie AD, Nega A, Gage A, Mariam DH, Eshetu MK, Arsenault C. Effect of the COVID-19 pandemic on health service utilization across regions of Ethiopia: an interrupted time series analysis of health information system data from 2019–2020. PLOS Glob Public Health. 2022;2(9):e0000843. doi:10.1371/journal.pgph.0000843
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.