")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Endovascular Thrombectomy for Acute Ischemic Stroke in Indonesia: Challenging and Strategic Planning
Authors Rilianto B , Kurniawan RG, Rajab NM, Prasetyo BT
Received 7 December 2023
Accepted for publication 6 March 2024
Published 21 March 2024 Volume 2024:20 Pages 621—630
DOI https://doi.org/10.2147/NDT.S453629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Beny Rilianto, Ricky Gusanto Kurniawan, Nurfadilah M Rajab, Bambang Tri Prasetyo
Neurointervention Division, Mahar Mardjono National Brain Center Hospital, East Jakarta, Indonesia
Correspondence: Beny Rilianto, Neurointervention Division, Mahar Mardjono National Brain Center Hospital, East Jakarta, Indonesia, Tel +62 823-8945-7858, Email [email protected]
Abstract: High rates of morbidity and mortality indicate that stroke is a major health concern. Unfortunately, the management of ischemic stroke is hindered by several obstacles, particularly in developing countries such as Indonesia, where the burden of morbidity and mortality remains high. In this literature review, we intend to conduct a thorough investigation and analysis of the obstacles to stroke thrombectomy in developing countries, with a focus on Indonesia. Even though numerous studies and recent advances in thrombectomy techniques have been developed, many centers around the world continue to struggle to implement them. The majority of these institutions are located in developing nations like Indonesia. It faces numerous obstacles, including a lack of public awareness, infrastructure, human resources, and financial difficulties. The absence of early education and large-scale campaigns contributes to the dearth of public awareness. Inadequate imaging facilities, prehospital and referral systems, as well as disparities in healthcare expenditure and accessibility, contribute to the absence of infrastructure. Inadequate numbers of neurointerventionists, neurologists, and neurosurgeons, as well as a disparate distribution of these professionals, contribute to human resource issues. Inadequate national insurance coverage, high import tariffs on medical devices, and the high cost of healthcare have a negative impact on the financial situation. We provide related strategies regarding the current situation in Indonesia based on the recent evidence and comparison with developed countries. Academic institutions, medical associations, and government agencies must collaborate to overcome these challenges.
Keywords: ischemic stroke, endovascular thrombectomy, large vessel occlusion, Indonesia, challenge
Introduction
Ischemic stroke is a cerebrovascular disorder characterized by acute episode of focal neurological dysfunction that persists for more than 24 hours, decreased blood flow to the brain tissues, which can be caused by atherosclerosis or thromboembolism.1 Cardioembolic stroke and atherothrombotic stroke are the highest in-hospital mortality among the subtypes of ischemic stroke and short-term prognosis compared with other ischemic stroke subtypes. Clinical characteristics detected at the time of stroke start can aid in identifying cardioembolic from atherothrombotic infarctions and critical for the utilization of therapeutics.2 Globally, the incidence of ischemic stroke is rising, affecting both developed and developing countries. In 2019, the Global Burden of Disease study ranked stroke as the second leading cause of death, accounting for 11.6% (10.8–12.2) of total deaths, and the third leading cause of combined death and disability, accounting for 5.7% (5.1–6.2) of total DALYs (Disability-Adjusted Life Years).3 From 1990 to 2019, the absolute number of incident strokes increased by 70.0% (67.0–73.0), prevalent strokes increased by 85.0% (83.0–88.0), stroke-related fatalities increased by 43.0% (31.0–55.0), and DALYs due to stroke increased by 32.0% (22.0–42.0).3 In the Southeast Asian region, the incidence of ischemic stroke per 100,000 individuals in thirteen nations increases every year (Figure 1). In general, it is evident that the incidence of ischemic stroke has shown an exponentially rising trend in the majority of countries since 1990, with the exception of Myanmar, Mauritius, and the Maldives. Indonesia initially ranked third in terms of the highest incidence rate and then saw notable growth, notably from 2017 to 2019, with the number of new cases rising from 121 to 128 per 100,000 individuals. If 30% of that is caused by Large Vessel Occlusion (LVO), it would be estimated that the number of LVO cases every year will be between 326.700 and 345.600 (based on Indonesia’s population of 270 million in 2019). This increasing trajectory is predicted to persist in the foreseeable future.4
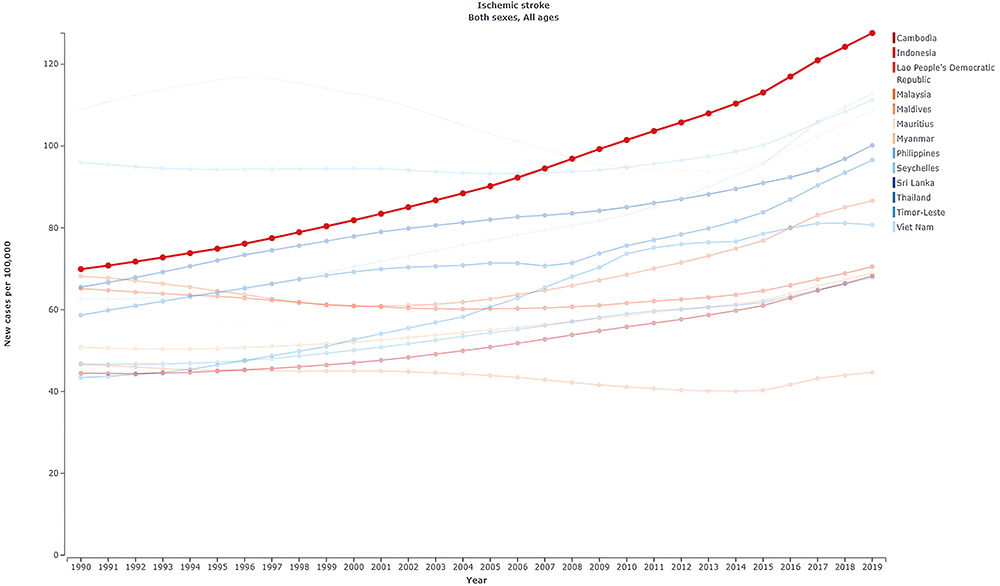 |
Figure 1 Incidence of Ischemic Stroke Among Southeast Asian Countries. Note: Adapted from Institute for Health Metrics and Evaluation. Global Burden Disease 2019 [Internet]. 2019 [cited 2023 Nov 24]. Available from: https://vizhub.healthdata.org/gbd-compare/. Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (https://creativecommons.org/licenses/by-nc-nd/4.0/).4 |
Acute ischemic stroke poses a significant hazard to life, particularly when large blood vessels become occluded large vessel.5 Initial treatment for ischemic stroke consisted of intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT).6,7 However, it was studied that the efficacy and treatment rates of alteplase for LVO were relatively low.7 In 2015, thrombectomy therapy became the standard treatment for patients with LVO with enhanced safety and efficacy.5–7 In 2018, two trials showed that acute ischemic stroke patients with onsets more than golden hour (>6 hours) could benefit from EVT through selected perfusion imaging (DAWN and DEFUSE 3).8,9 Recently, several trials in 2023 showed the benefits of thrombectomy even in large infarct cores (ANGEL-ASPECT and SELECT-2).10,11 Recent evidence of EVT in posterior circulation stroke generated significant benefit for patient over alone medical therapy such.12
Unfortunately, there are many barriers to the management of ischemic stroke, particularly in developing nations like Indonesia which the burden of morbidity and mortality remains high.13,14 To improve healthcare services and reduce the morbidity and mortality associated with stroke, it is crucial to address obstacles in the pre-hospital and in-hospital phases, as well as those related to infrastructure and financial resources.14 In this literature review, we intend to investigate and analyze comprehensively the barriers to stroke thrombectomy in developing countries, with a particular focus on Indonesia. Understanding these obstacles is crucial for devising effective strategies and interventions to surmount the obstacles associated with thrombectomy implementation in resource-limited settings. By identifying and addressing these obstacles, we can improve the quality of stroke care, reduce the burden of stroke-related disability and mortality, and ultimately improve the overall landscape of stroke management in developing nations, such as Indonesia.
Materials and Methods
The method of this study is a scoping literature review using international and national publications through various databases in terms of research articles, reports, and working papers published in the last decade (2015–2023) using keywords “endovascular thrombectomy”, “stroke”, “developing countries” in order to enrich the strategies which developed by the authors related to the current situation in Indonesia. The sources such as The Lancet Neurology, The New England Journal of Medicine, European Heart Journal, Bulletin of World Health Organization, International Journal of Stroke, Quantitative Imaging in Medicine and Surgery, American Journal of Neuroradiology, Journal of Neurointerventional Surgery, BMC Neuroscience, AHA Journal, Journal of Stroke, JAMA Neurology, web page and regulation of Ministry of Health of Republic of Indonesia, Global Burden Diseases 2019, several working papers, and reports.
Results
Recent advancements in treatment for acute ischemic stroke such as IVT and EVT have revolutionized the treatment of acute ischemic stroke, especially in LVO. Significant outcomes of EVT reducing the economic burden due to the globally high-cost effectiveness and time-sensitive. Even though numerous studies and recent advances in thrombectomy techniques have been developed, many centers worldwide still struggle to implement them. The majority of these institutions are located in developing countries, such as Indonesia. Regarding the previous study titled Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization–Lancet Neurology Commission, they used four pillars as a basis of the assessment such as surveillance, prevention, acute care, and rehabilitation.15 Nonetheless, authors in this study provide numerous recommendations and strategies based on the current challenges in Indonesia such as infrastructure, human resources, emergency medical services, financial issues, and a lack of public awareness to generate recent evidence and comparison with developed countries. Findings of the previous study listed in Table 1.
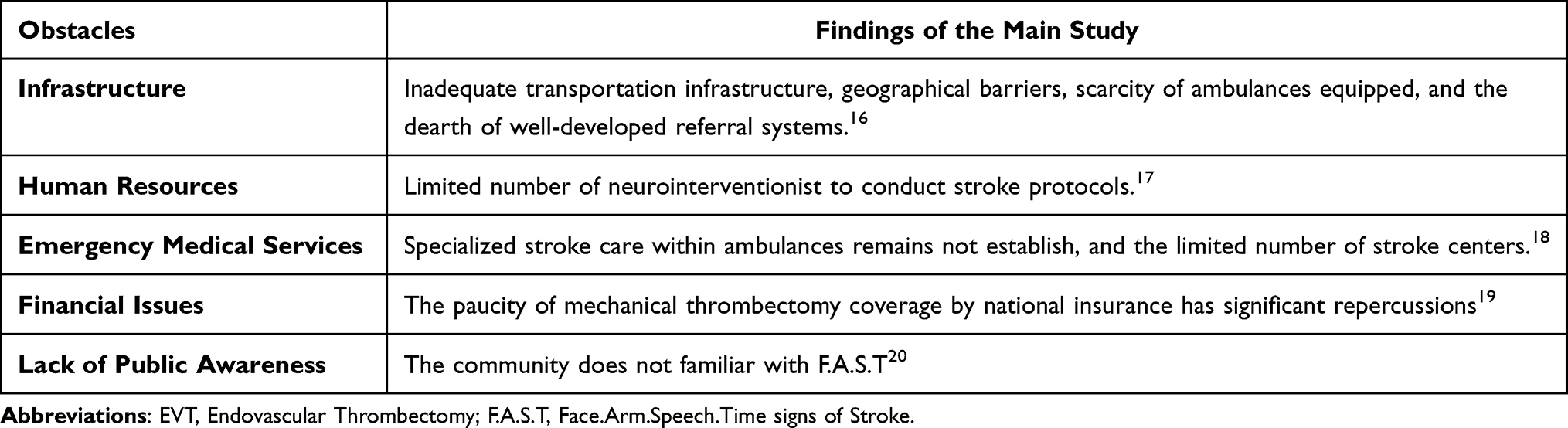 |
Table 1 The Primary Findings of the EVT Barriers |
Discussion
Optimizing Reperfusion Therapy in Early Time Windows
The standard treatment for acute ischemic stroke has been thrombolysis, specifically the symptoms onset of 4.5 hours. With the advent of EVT, however, the role of IVT in the modern era has been called into question. New results from a recent study suggest that using intravenous thrombolysis both alteplase and tenecteplase (TNK) along with EVT lead to better outcomes.21 The study demonstrated that TNK led to a higher rate of angiographic reperfusion and improved clinical outcomes without increasing the risk of bleeding.21 Multiple randomized controlled trials have presented compelling evidence supporting the use of EVT in specific patient populations.8 In addition, recent studies have investigated the efficacy of EVT in patient subgroups previously excluded from randomized trials. Patients with large ischemic core strokes constitute one of these subgroups. Prior trials largely precluded patients with an Alberta Stroke Programme Early CT Score (ASPECTS) of less than 6, leaving the efficacy of EVT in this population uncertain.22–25 The SELECT study, however, was limited to patients with ASPECTS 5 or extensive ischemic foci on CT perfusion.26 At 90 days, the EVT group demonstrated a significant increase in functional independence compared to the medical therapy group even in patients with significant ischemic centers. Significant outcomes of EVT reducing the economic burden due to the globally high cost-effectiveness and time-sensitive (Table 2).27
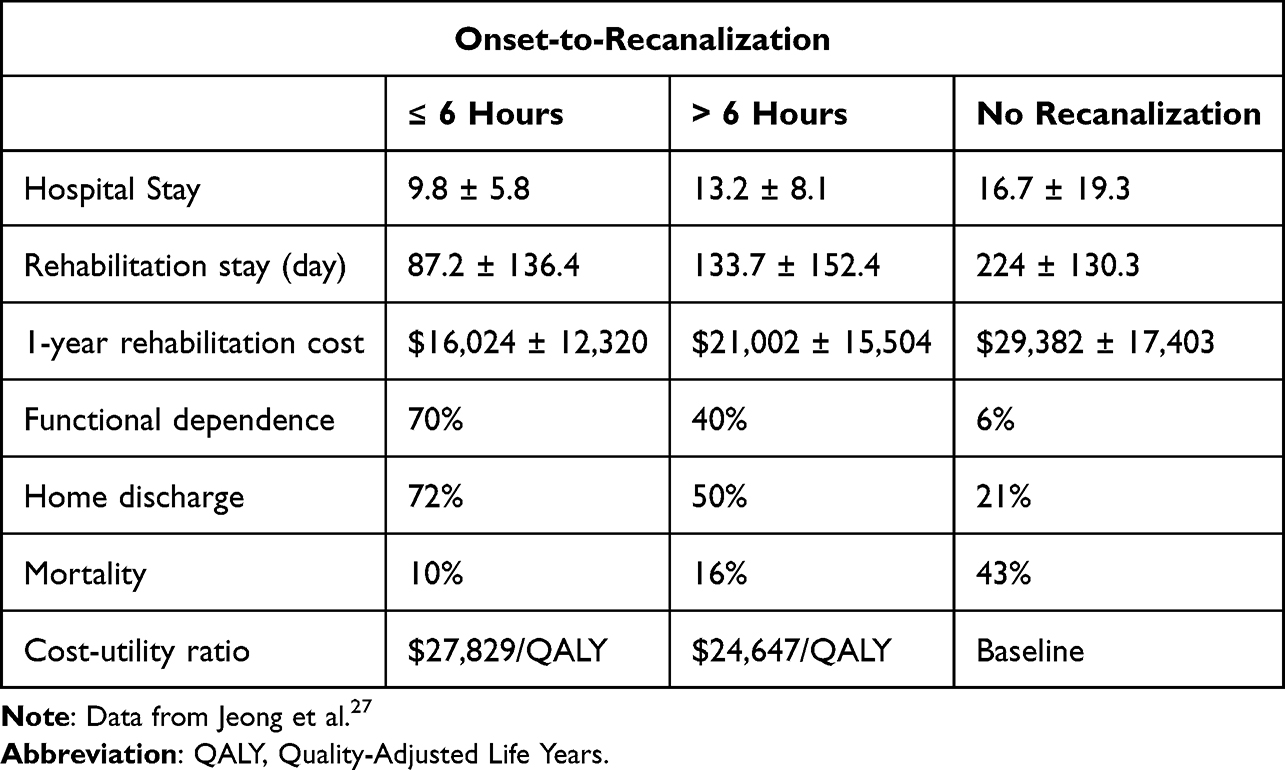 |
Table 2 Global Cost-Effectiveness of Recanalization Using Mechanical Thrombectomy.27 |
The subgroup of patients with moderate strokes, medium vessel occlusion (MeVO) and proximal LVO are also of interest. In general, these patients were excluded from previous trials, making it difficult to determine the benefits of EVT in this population. Regarding the poor natural history of MeVO, EVT trial seemed appropriate due to efficacy and safety evidence in middle cerebral artery segment occlusion. Nevertheless, numerous issues such as adequate devices and techniques for MeVO thrombectomy must be devised and evaluated, establish adequate outcome measurement tools is necessary.28 Nowadays, additional evidence of EVT in MeVO will be generated by ongoing trials such as DISTAL (performed all EVT techniques), DISCOUNT (performed EVT in AIS related to a distal arterial occlusion), ESCAPE-MeVO (performed EVT with Solitaire X (Medtronic, USA)), and DISTALS (performed EVT with Tigertriever 13 (Rapid Medical, Yokneam, Israel)).29–32 A crucial part of EVT is giving thrombolysis before thrombectomy. This is in addition to choosing the right patient and time window.33
Increase the Number, Capability, and Distribution of Neurointerventionists by Fellowship Program
In developing countries like Indonesia, implementation of EVT faces several challanges, including lack resources: there are not enough health care services, including neurointerventionists, and doctors do not aware how to conduct stroke protocols.17 To address these challenges, strategic measures are required, such as increasing the number and distribution of specialized neurointerventionists, enhancing training programs and capacity-building initiatives, and encouraging hospitals to implement stroke protocols.
The lack of neurointerventionists in Indonesia is a significant barrier to the widespread use of EVT for ischemic stroke patients. Investing in the training and education of healthcare professionals in the field of neurointervention is essential for addressing this issue. Essential steps include the development of specialized fellowship programs and the provision of training opportunities for practitioners to learn neurointervention techniques and stroke protocols. Collaboration with international institutions can also facilitate knowledge exchange and capacity building, thereby bridging the disparity in specialized knowledge. World Federation for Interventional Stroke Treatment (WIST) can provide information, courses, and training guidance to the neurointerventionist. WIST are using their guidelines and establishing clinical knowledge and procedural skills to raise the capability requirements of interventionalist to perform endovascular stroke intervention.34 Likewise, collaborate with ANGELS Academy provide e-learning program for stroke care knowledge and skills is potential to enhance the competency of neurointerventionist.35 Providing a proctoring session to the fellow via telemedicine can increase the rate of IVT in many hospitals. Proctoring is under neurointerventionist responsibilities.
Currently, Indonesia still requires many neurointerventionists until 2024. Therefore, one of the recommendations for optimizing Stroke Service Hospitals in Indonesia is to increase the number of centers of neurointerventional fellowships which are expected to generate an output of 40 neurointerventionists per year. In early 2023, six Centers of Neurointervention Specialist Hospital opened fellowship programs with a training period of one year. If the capacity of fellows per semester above is sufficient, the target to increase the number of neurointerventionists can be achieved.
Creating favorable conditions for neurointerventionists to function in Indonesia is likewise essential. This involves offering competitive compensation, attractive benefits, and opportunities for career advancement to attract and retain qualified employees. Establishing centers of excellence for neurointervention can attract neurointerventionists and nurture a thriving ecosystem. By addressing the lack of neurointerventionists and increasing the availability of mechanical thrombectomy services, more stroke patients in Indonesia will have access to this lifesaving treatment.
In addition, a lack of familiarity with stroke protocols can delay the transfer of patients to specialized stroke centers that offer mechanical thrombectomy. It may result in suboptimal stroke care in the early phases, including delays in brain imaging and thrombolytic therapy administration, if applicable.18 These delays can have a substantial impact on the overall efficacy of EVT and the likelihood of favorable patient outcomes.
Collaboration between medical societies, academic institutions, and government agencies can aid in the development of locally tailored, standardized stroke protocols and guidelines.19 In addition, the establishment of stroke centers of excellence and multidisciplinary stroke teams can facilitate the exchange of knowledge and expertise between healthcare professionals. These institutions can serve as sites for training, research, and collaboration, allowing for continuous professional development and the dissemination of best practices in stroke care, such as the correct use of thrombectomy.
Establish Adequate Stroke Facilities and Infrastructure Nationwide
One of the major concerns is the access to specialized stroke facilities that offer EVT is hampered in rural regions of developing countries due to inadequate transportation infrastructure and geographical barriers.16 The dearth of well-developed referral systems and the scarcity of ambulances equipped to treat stroke patients impede timely access to care.16 Collectively, these factors contribute to delayed treatment and decreased utilization of thrombectomy services in marginalized regions. Thus, policies aimed at increasing financing for healthcare and distributing resources equitably are necessary to close the disparity between urban and rural areas. There are differences between the US system and the Indonesian system in stroke services (Table 3).
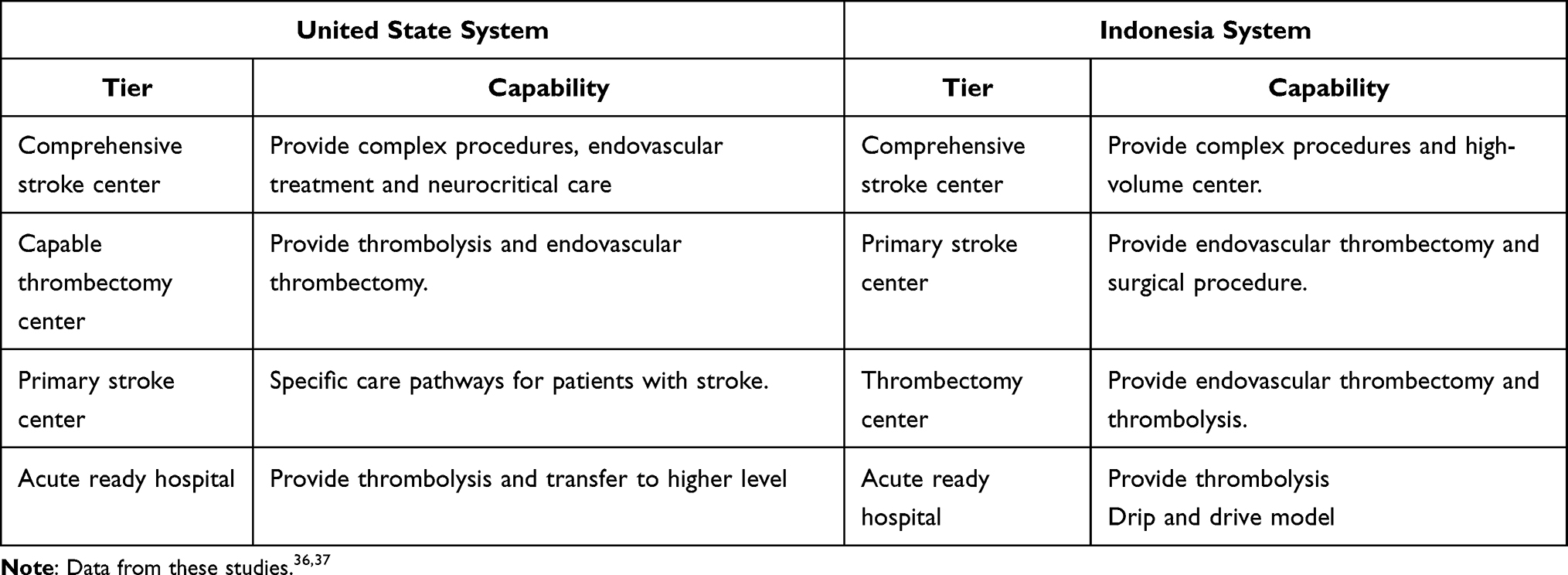 |
Table 3 Comparison Between Stroke Centers by US System and Indonesia System |
Fulfillment of Cath-lab facilities is necessary for addressing lack of access to reach Stroke Service Hospitals. In 2021, there are 346 Cath-lab in public and private hospitals. Nevertheless, this number is still insufficient to meet the needs of Cath-lab in Indonesia. In 2022–2024, an additional 80 cath-labs are needed as the main component for developing a Stroke Service Hospital. By 2027, Indonesia targeted to develop rumah sakit strata utama (primary stroke center) in each Province and rumah sakit strata madya (thrombectomy center) in each regency nationwide. The equitable distribution of stroke center is essential due to the current situation that stroke center especially paripurna and utama is centralized on the Java Island.
Based on the decision of the Indonesian Ministry of Health, one of the strategic plans to improve stroke service in Indonesia is hospital stratification. It divided the hospital into several stratifications with different capabilities, human resources, and facilities for stroke intervention services (Table 2). The least advanced hospital stratification in Indonesia is called rumah sakit dasar (acute stroke ready hospital) with the intervention for stroke therapy limited to IVT. Rumah Sakit Madya is authorized to perform non-surgical neurovascular intervention and IVT. Rumah Sakit Utama is certified to perform EVT and surgical treatment. Then rumah sakit paripurna is standardized to perform cerebrovascular complex procedures.37 Stroke leading scheme and regionalization of stroke leading hospital shown in Figures 2 and 3.
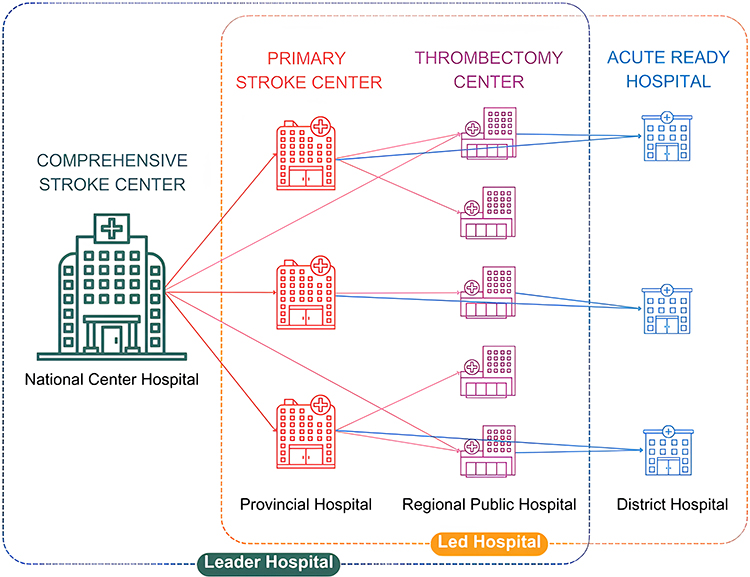 |
Figure 2 Stroke Leading Scheme. Notes: Data from Ministerial Decree of The Minister of Health of Republic of Indonesia No. K.01.07/MENKES/1336/2023 [Internet]. Available from: https://yankes.kemkes.go.id/unduhan/fileunduhan_1684965444_953452.pdf37. |
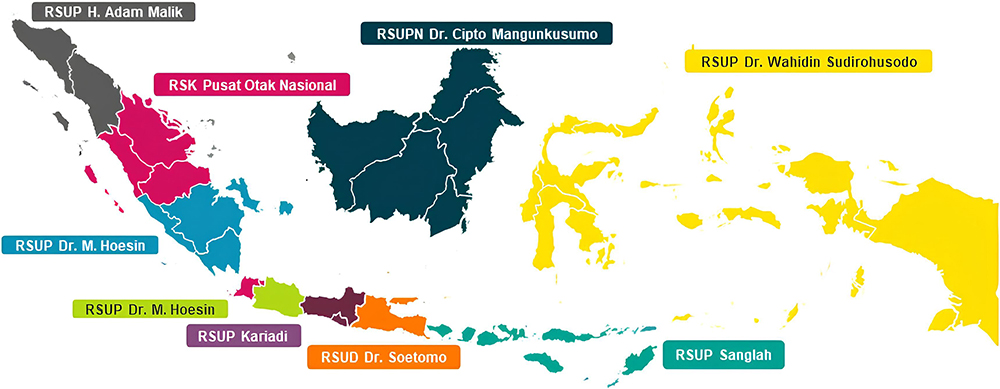 |
Figure 3 Regionalization of stroke leading hospital. Notes: Data from Ministerial Decree of The Minister of Health of Republic of Indonesia No. K.01.07/MENKES/1336/2023 [Internet]. Available from: https://yankes.kemkes.go.id/unduhan/fileunduhan_1684965444_953452.pdf.37 |
Enlarge the Emergency Medical Services by Adequate Prehospital Care
In Indonesia, insufficient availability of ambulances outfitted to treat stroke patients and the geographical obstacles impede the prompt treatment of stroke patients, particularly in remote and underserved areas. Delays in reaching hospitals able to perform EVT are caused by a paucity of specialized stroke care within ambulances, which reduces the efficacy of the treatment.18 Inadequate roads, transportation infrastructure, and emergency medical services impede the transit of stroke patients to stroke centers, making it difficult to establish a well-connected referral system.18
To resolve these obstacles, a multifaceted strategy is required. It is essential to invest in emergency medical services, particularly in underserved areas. This requires a sufficient number of well-equipped ambulances and the training of emergency medical personnel to effectively manage stroke cases. Collaborations between government agencies, healthcare institutions, and non-governmental organizations can assist in enhancing the existing infrastructure and closing stroke care accessibility gaps.
In addition, telemedicine and telestroke programs provide innovative means of overcoming geographical limitations.20,38 These programs facilitate real-time assessment and decision-making regarding EVT by facilitating remote consultation between stroke experts and healthcare providers in underserved areas.20 Telemedicine can resolve the expertise divide, increasing the accessibility of stroke care in regions where specialized stroke centers are scarce or nonexistent.20
The limited number of stroke centers indicates that reperfusion procedures only can be obtained in big cities. For this reason, adequate ambulance facilities are needed in quantity and quality to reach Stroke Service Hospitals over quite long distances with high traffic problems in big cities. Hence, early detection is necessary to prevent late diagnosis and treatment of stroke.
High public awareness in Singapore to promote and practice the F.A.S.T method should be a great model for Indonesia and other countries. Currently, Indonesia is developing the F.A.S.T Rescue mobile app as a platform for providing first aid to stroke patients. Users can find out the location of the nearest stroke-ready hospital. This application also provides a complete list of the locations of all stroke-ready hospitals in Indonesia. It is essential to find the list of stroke-ready hospitals due to the characteristic of stroke that can occur anytime, anywhere, and by anyone.39 Therefore, an additional solution to enhance the access to acute stroke-ready hospitals is increasing the amount of public transportation.
There is less awareness identifying LVO among doctors, even among neurologists. The consequence is that many LVO patients do not receive further treatment until thrombectomy. Providing LVO identification is essential through regular screening such as Visual Aphasia Neglect (VAN) scale in the prehospital setting and emergency unit.
Compared with other ASEAN countries, an adequate prehospital care in Thailand such as Stroke One Stop (SOS) is a solution to enlarge the prehospital care with mobile stroke unit which set up by onboard CT scanner and a medical team consisting of a doctor, nurse, and radiologic technician to begin initial management immediately.40 Therefore, better-organized Emergency Medical Services (EMS) in Thailand are still facing a lack of utilization, specifically only around 5.5–20.5% of patients. This indicates that by EMS, only one-half of stroke patients are transferred to the stroke center.41
Comparing problems of EMS in developed countries such as the United States, EMS providers reported insufficient LVO training and knowledge gaps in LVO, stroke severity scales, and stroke center levels. Systematic efforts are required to improve and standardize the educational content and delivery of LVO education in order to save more lives.42
Enhance the Health Care Affordability and Organize Financial Problems
Reperfusion with thrombectomy is frequently not fully covered by national insurance in developing nations like Indonesia, and high import tariffs on medical supplies are another financial barrier to using mechanical thrombectomy. Expanding insurance coverage to include stroke therapy, lowering import duties on medical devices, and investigating cost-effective techniques for purchasing and maintaining essential equipment are all part of a complete response to these difficulties.
Compared to highly diverse health coverage in the Southeast Asia Region (SEAR) which mixes private and public health insurance, Thailand and Singapore are being role models for stroke financing around SEAR which is predominantly under national health coverage. Unfortunately, thrombolysis use is still limited with a rate of only 0.18–8.04%.41
In Indonesia, the Minister of Health Regulation 2023 determines the claim value for thrombolysis agents such as alteplase as a standard treatment for health facilities to bill claims to National Health Coverage.43 In addition, the paucity of mechanical thrombectomy coverage by national insurance has significant repercussions. First, it imposes a significant financial burden on stroke patients and their families, as the procedure and associated expenses can be quite expensive. Without insurance, patients may experience delays in treatment or be unable to finance it at all. Second, the lack of coverage exacerbates healthcare disparities, as access to mechanical thrombectomy is restricted to those who can afford out-of-pocket costs or have private insurance. Individuals from lower socioeconomic backgrounds who rely on national insurance are disproportionately affected.19 In addition, the lack of coverage discourages healthcare providers from providing the treatment, thereby limiting its availability even in facilities with the necessary resources. By addressing the dearth of insurance coverage, a greater number of stroke patients will have access to this innovative treatment option.
The limitation of this study is a lack of literature from Indonesia, thus the proportion of the discussion section is greater than the results in order to provide an understanding of actual circumstances in Indonesia. Findings of this study will be utilized to improve the regulations and increasing stroke services quality in Indonesia, as well as to initiate the development of further studies on strategies for addressing EVT problems in acute ischemic stroke.
Conclusion
Even though numerous studies and recent advances in thrombectomy techniques have been devised, many centers around the world continue to struggle to implement them. The vast majority of these institutions are located in developing nations like Indonesia. Lack of public awareness, lack of infrastructure, human resources, and financial problems are among those that hinder it. Academic institutions, medical associations, and government agencies need to work together to surmount these obstacles.
Acknowledgments
We thank to Mahar Mardjono National Brain Center Hospital for supporting this publication.
Disclosure
The authors declare that the study was carried out without any commercial or financial affiliations that may be interpreted as a possible conflict of interest.
References
1. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
2. Arboix A, Oliveres M, Massons J, Pujades R, García-Eroles L. Early differentiation of cardioembolic from atherothrombotic cerebral infarction: a multivariate analysis. Eur J Neurol. 1999;6(6):677–683. doi:10.1046/j.1468-1331.1999.660677.x
3. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
4. Institute for Health Metrics and Evaluation. Global burden disease 2019 [Internet]; 2019. Available from: https://vizhub.healthdata.org/gbd-compare/#.
5. Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–1731. doi:10.1016/S0140-6736(16)00163-X
6. Ospel JM, McTaggart R, Kashani N, Psychogios M, Almekhlafi M, Goyal M. Evolution of Stroke thrombectomy techniques to optimize first-pass complete reperfusion. Semin Intervent Radiol. 2020;37(02):119–131. doi:10.1055/s-0040-1709153
7. von Gadow N, Nikoubashman O, Freiherr J, et al. Endovascular stroke treatment now and then-procedural and clinical effectiveness and safety of different mechanical thrombectomy techniques over time. Quant Imaging Med Surg. 2017;7(1):1–7. doi:10.21037/qims.2017.02.06
8. Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378(8):708–718. doi:10.1056/NEJMoa1713973
9. Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378(1):11–21. doi:10.1056/NEJMoa1706442
10. Huo X, Ma G, Tong X, et al. Trial of endovascular therapy for acute ischemic stroke with large infarct. N Engl J Med. 2023;388(14):1272–1283. doi:10.1056/NEJMoa2213379
11. Sarraj A, Hassan AE, Abraham MG, et al. Trial of endovascular thrombectomy for large ischemic strokes. N Engl J Med. 2023;388(14):1259–1271. doi:10.1056/NEJMoa2214403
12. Adusumilli G, Kobeissi H, Ghozy S, et al. Endovascular thrombectomy after acute ischemic stroke of the basilar artery: a meta-analysis of four randomized controlled trials. J Neurointerv Surg. 2023;15:e3.
13. Setyopranoto I, Bayuangga HF, Panggabean AS, et al. Prevalence of stroke and associated risk factors in sleman district of Yogyakarta Special Region, Indonesia. Stroke Res Treat. 2019;2019:2642458. doi:10.1155/2019/2642458
14. Adeoye O, Nyström KV, Yavagal DR, et al. Recommendations for the establishment of stroke systems of care: a 2019 update. Stroke. 2019;50(7). doi:10.1161/STR.0000000000000173
15. Feigin VL, Owolabi MO, Owolabi MO, et al. Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization–Lancet Neurology Commission. Lancet Neurol. 2023;22(12):1160–1206. doi:10.1016/S1474-4422(23)00277-6
16. Tsang ACO, Yang IH, Orru E, et al. Overview of endovascular thrombectomy accessibility gap for acute ischemic stroke in Asia: a multi-national survey. Int J Stroke. 2020;15(5):516–520. doi:10.1177/1747493019881345
17. Mesiano T, Kurniawan M, Saputri KM, et al. Endovascular treatment in acute ischemic stroke adoption and practice: a Single-Center Indonesian Experience. Cerebrovasc Dis Extra. 2021;11(2):72. doi:10.1159/000517183
18. Sablot D, Gaillard N, Smadja P, Bonnec JM, Bonafe A. Thrombectomy accessibility after transfer from a primary stroke center: analysis of a three-year prospective registry. Int J Stroke. 2017;12(5):519–523. doi:10.1177/1747493017701151
19. Aroor SR, Asif KS, Potter-Vig J, et al. Mechanical thrombectomy access for all? Challenges in increasing endovascular treatment for acute ischemic stroke in the United States. J Stroke. 2022;24(1):41–48. doi:10.5853/jos.2021.03909
20. Busti C, Gamboni A, Calabrò G, et al. Telestroke: barriers to the transition. Front Neurol. 2021;12:689191. doi:10.3389/fneur.2021.689191
21. Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N Engl J Med. 2019;380(19):1795–1803. doi:10.1056/NEJMoa1813046
22. Nogueira RG, Haussen DC, Liebeskind DS, et al. Clinical effectiveness of endovascular stroke treatment in the early and extended time windows. Int J Stroke. 2022;17(4):389–399. doi:10.1177/17474930211005740
23. Campbell BCV, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11):1009–1018. doi:10.1056/NEJMoa1414792
24. Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019–1030. doi:10.1056/NEJMoa1414905
25. Jovin TG, Chamorro A, Cobo E, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372(24):2296–2306. doi:10.1056/NEJMoa1503780
26. Sarraj A, Hassan AE, Savitz S, et al. Outcomes of endovascular thrombectomy vs medical management alone in patients with large ischemic cores: a secondary analysis of the optimizing patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) Study. JAMA Neurol. 2019;76(10):1147–1156. doi:10.1001/jamaneurol.2019.2109
27. Jeong HS, Shin JW, Kwon HJ, et al. Cost benefits of rapid recanalization using intraarterial thrombectomy. Brain Behav. 2017;7(10):e00830. doi:10.1002/brb3.830
28. Goyal M, Ospel JM, Menon BK, Hill MD. MeVO: the next frontier? J Neurointerv Surg. 2020;12(6):545–547. doi:10.1136/neurintsurg-2020-015807
29. Study Details | enDovascular Therapy Plus Best Medical Treatment (BMT) Versus BMT Alone for MedIum VeSsel Occlusion sTroke | clinicalTrials.gov; 2024. Available from: https://clinicaltrials.gov/study/NCT05029414.
30. Study Details | distal Ischemic Stroke Treatment With Adjustable Low-profile Stentriever | clinicalTrials.gov; 2024. Available from: https://clinicaltrials.gov/study/NCT05152524.
31. Study Details | endovaSCular TreAtment to imProve outcomEs for Medium Vessel Occlusions (ESCAPE-MeVO Trial) | clinicalTrials.gov; 2024. Available from: https://clinicaltrials.gov/study/NCT05151172.
32. Study Details | evaluation of Mechanical Thrombectomy in Acute Ischemic Stroke Related to a Distal Arterial Occlusion | clinicalTrials.gov; 2024. Available from: https://clinicaltrials.gov/study/NCT05030142.
33. Widimsky P, Snyder K, Sulzenko J, Hopkins LN, Stetkarova I. Acute ischaemic stroke: recent advances in reperfusion treatment. Eur Heart J. 2023;44(14):1205–1215. doi:10.1093/eurheartj/ehac684
34. Grunwald IQ, Mathias K, Bertog S, et al. World Federation for Interventional Stroke Treatment (WIST) multispecialty training guidelines for endovascular stroke intervention. Postepy Kardiol Interwencyjnej. 2023;19(1):6. doi:10.5114/aic.2023.124742
35. Angels Initiative [Internet]; 2024. Available from: https://www.angels-initiative.com/angels-community/meet-The-experts.
36. The Joint Commission. Stroke Certification [Internet]; 2023. Available from: https://www.jointcommission.org/what-we-offer/certification/certifications-by-setting/hospital-certifications/stroke-certification/.
37. Ministerial decree of the minister of health of republic of Indonesia No. K.01.07/MENKES/1336/2023 [Internet]. Available from: https://yankes.kemkes.go.id/unduhan/fileunduhan_1684965444_953452.pdf.
38. Gao J, Fan C, Chen B, et al. Telemedicine is becoming an increasingly popular way to resolve the unequal distribution of healthcare resources: evidence from China. Front Public Health. 2022;10:916303. doi:10.3389/fpubh.2022.916303
39. Indonesian Stroke Society. Aplikasi F.A.S.T Rescue, Sekali Klik, Menyelamatkan Nyawa Anda dan Keluarga dari Serangan Stroke yang Tiba-tiba; 2021. Available from: https://strokesociety.id/aplikasi-f-a-s-t-rescue-sekali-klik-menyelamatkan-nyawa-anda-dan-keluarga-dari-serangan-stroke-yang-tiba-tiba/.
40. Siriraj Hospital. Stroke one stop – the mobile stroke unit for emergency cases; 2022. Available from: https://www2.si.mahidol.ac.th/en/news-events/stroke-one-stop-The-mobile-stroke-unit-for-emergency-cases/.
41. Sebastian IA, Gandhi DBC, Sylaja PN, et al. Stroke systems of care in South-East Asia Region (SEAR): commonalities and diversities. Lancet Reg Health Southeast Asia. 2023;17:100289. doi:10.1016/j.lansea.2023.100289
42. Asif KS, Novakovic R, Nguyen TN, et al. Large‐vessel occlusion stroke knowledge and training for stroke severity assessment among emergency medical services personnel in the United States. Stroke. 2023. doi:10.1161/str.54.suppl_1.TMP46
43. Ministerial Decree of The Minister of Health of Republic of Indonesia No. HK.01.07-MENKES-1276-2023 [Internet]. 2023. Available from: https://farmalkes.kemkes.go.id/unduh/kmk-no-hk-01-07-menkes-1276-2023-ttg-nilai-klaim-harga-obat-program-rujuk-balik-obat-penyakit-kronis-obat-kemoterapi-dan-obat-alteplase/.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.