")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Evaluating the Utility of a Near-Peer Situation-Based Course to Prepare Medical Students for the UK Foundation Programme: A Pilot Study
Authors Dunin-Borkowska A , Cardoso Pinto AM, Xu J , Bhandari N, Ranasinghe L
Received 7 September 2023
Accepted for publication 8 November 2023
Published 22 November 2023 Volume 2023:14 Pages 1317—1325
DOI https://doi.org/10.2147/AMEP.S434080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Aleksandra Dunin-Borkowska,1 Alexandra M Cardoso Pinto,1 Joshua Xu,1 Nikhil Bhandari,2 Lasith Ranasinghe3
1Department of Medicine, Imperial College London, London, UK; 2Department of Medicine, St George’s Medical School, University of London, London, UK; 3Department of Acute Internal Medicine, Homerton Healthcare NHS Foundation Trust, London, UK
Correspondence: Aleksandra Dunin-Borkowska, Department of Medicine, School of Medicine, Imperial College London, London, UK, Tel +44 7378324178, Email [email protected]
Background: Starting the Foundation Programme can be challenging for many medical graduates, as medical school alone may not adequately prepare them for complex tasks like managing comorbidities or emergencies. Growing evidence supports the role of transition interventions to meet this knowledge gap, however data on the utility of situation-based learning are limited. This pilot study aimed to assess the efficacy of a near-peer case-based course in improving knowledge and preparedness for foundation training in recent medical graduates.
Methods: Recent Imperial College graduates who attended a “Junior Doctor on Call” course were eligible for inclusion. This transition intervention, designed and delivered by a Foundation Year 1 doctor, covered six patient cases that integrated high-yield clinical concepts and practical tips. An online questionnaire was distributed one week before and after the course to assess perceptions of knowledge, confidence, and preparedness for training. Participants were also invited to attend an online semi-structured after the course.
Results: Out of 19 attendees, 17 (89.5% response rate) completed the pre-course questionnaire, 14 (73.7% response rate) completed the post-course questionnaire, and 3 completed the interview. 68.75% (n=11) had not previously attended a preparatory course for foundation training. Results demonstrated that 85.7% of participants felt more knowledgeable than before in the key topics covered. Participants also demonstrated an increase in self-rated confidence in commencing work as a junior doctor following the course, with 92.9% of participants stating that they felt more confident.
Conclusion: This study offers support for short-term situation-based courses in enhancing medical students’ knowledge and confidence for foundation training. These findings add to the growing evidence-base encouraging implementation of short-term courses in preparing for practice. However, further research on the utility of such transition interventions is critical to inform the development of evidence-based recommendations for recent medical graduates, educators, and programme directors.
Keywords: medical education, clinical practice, situation-based learning, near-peer learning, foundation training
Introduction
Embarking on the Foundation Programme is a challenge often met with apprehension, stress, and anxiety amongst medical students.1 Over the last few decades, a rising number of reports consistently demonstrate that recent graduates feel underprepared for clinical practice.2–5 Specific areas in which students feel underprepared include, but are not limited to: safe and legal prescribing, error management, working within a multidisciplinary team, and the management of acute medical emergencies.4,6 This is likely due to multiple factors,6,7 including limited exposure to complex cases during medical school, poor vocational understanding of on-call duties, and more recently, the COVID-19 pandemic.
Several factors which promote preparedness have been identified to date, including those pertaining to medical school programmes (eg early clinical shadowing), the workplace (eg perceived support from fellow and senior staff) and the individual (eg self-confidence, leadership skills, and an accurate awareness of one’s limitations).7 Recent studies have, however, highlighted the efficacy of educational interventions in preparing students for the transition.8 For instance, 97% of junior doctors who attended a “targeted structured induction programme” felt prepared to subsequently practise medicine when asked to complete a questionnaire four months after starting to work as a foundation doctor.9 This is echoed in recent guidance from the General Medical Council (GMC) which highlights the need for transition interventions to support graduates for their first year of training, Foundation Year 1 (FY1), given the detrimental downstream effects a real or perceived lack of preparation may have on anxiety and burnout.10
To date, most UK-based studies which investigate the utility of such interventions are limited to perceptions of junior doctors who have already begun foundation training, or students still at medical school. Furthermore, although recent interest has shifted towards simulation-based learning,11,12 the evidence base for transition interventions is dominated by courses using didactic teaching on discrete topics (eg prescribing). This pilot study therefore sought to investigate the efficacy of a junior doctor-led situation-based course in improving perceptions of preparedness in recent medical graduates. The course focused on concepts which are typically poorly understood, but are routinely encountered by FY1 doctors while on call. The team hypothesised that reviewing high-yield topics in the context of patient cases, with an emphasis on application as opposed to rote recall, would improve perceived confidence and preparedness for training in recent medical graduates.
Methods
Course Design and Delivery
The course consisted of six cases encountered over a simulated Foundation Year 1 (FY1) night shift. Each case involved a patient with a distinct set of interacting comorbidities (Supplementary Material 1). Attendees were presented with a patient experiencing an acute medical emergency, and subsequently tasked with performing ABCDE assessments, interpreting observation and drug charts, requesting and interpreting key investigations, managing the patient, and re-assessing where relevant. The course was advertised through social media and mailing lists of a medical education charity (Make a Medic), as well as word of mouth. All medical graduates who were registered to attend the course were eligible for inclusion.
Data Collection
Attendees were asked to complete an optional pre- and post-course questionnaire (Supplementary Material 2). Both questionnaires were allotted a one-week period during which participants could submit responses. Questions evaluating factors such as self-rated confidence in distinct clinical concepts and preparedness for foundation training were designed using a modified 6-point Likert scale. Participants could further expand on their learning experiences using free text responses where possible. All participants were invited to an optional semi-structured interview upon completion of the pre-course and post-course questionnaires.
Statistical Analysis
Questionnaire data was exported to Microsoft Excel for data cleaning. The final Likert scale used for analysis and data presentation ranges from 1 (not confident at all), up to 6 (completely confident).
Quantitative pre- and post-course data were tested for normality using the Shapiro–Wilk test, and subsequently analysed for statistically significant differences using the non-parametric Mann–Whitney U-test. Qualitative data were analysed using thematic analysis. Incomplete entries in either questionnaire were excluded. Statistical analysis was conducted using Microsoft Excel. Data is presented as median ± interquartile range (IQR) where possible, or descriptively using percentages. A p-value of <0.05 was considered statistically significant.
Participant Consent
Participants were issued an information sheet about the study protocol including the purpose of the study and the type of data that would be collected. The participants then completed and submitted a consent form agreeing to take part in the study and allowing for the publication of anonymised responses.
Ethical Approval
Ethical approval for this study was granted by the Imperial College Education Ethics Review Board (EERP2122-080a).
Results
Participant Demographics
19 medical graduates attended the course. Overall, 17 attendees completed the pre-course questionnaire (89.5% response rate), and 14 attendees completed the post-course questionnaire (73.7% response rate). Therefore, the matched questionnaire response rate was 82.4%. 3 attendees agreed to participate in the optional interview following the course completion.
The average age was 25 ± 2 years (range: 22–29) and 52.9% (n=9) identified as female. A total of 87.5% (n=14) were undergraduate students and 75% (n=12) held an additional degree. 37.5% (n=6) were undecided about their specialty of interest. Participant data are summarised in Table 1.
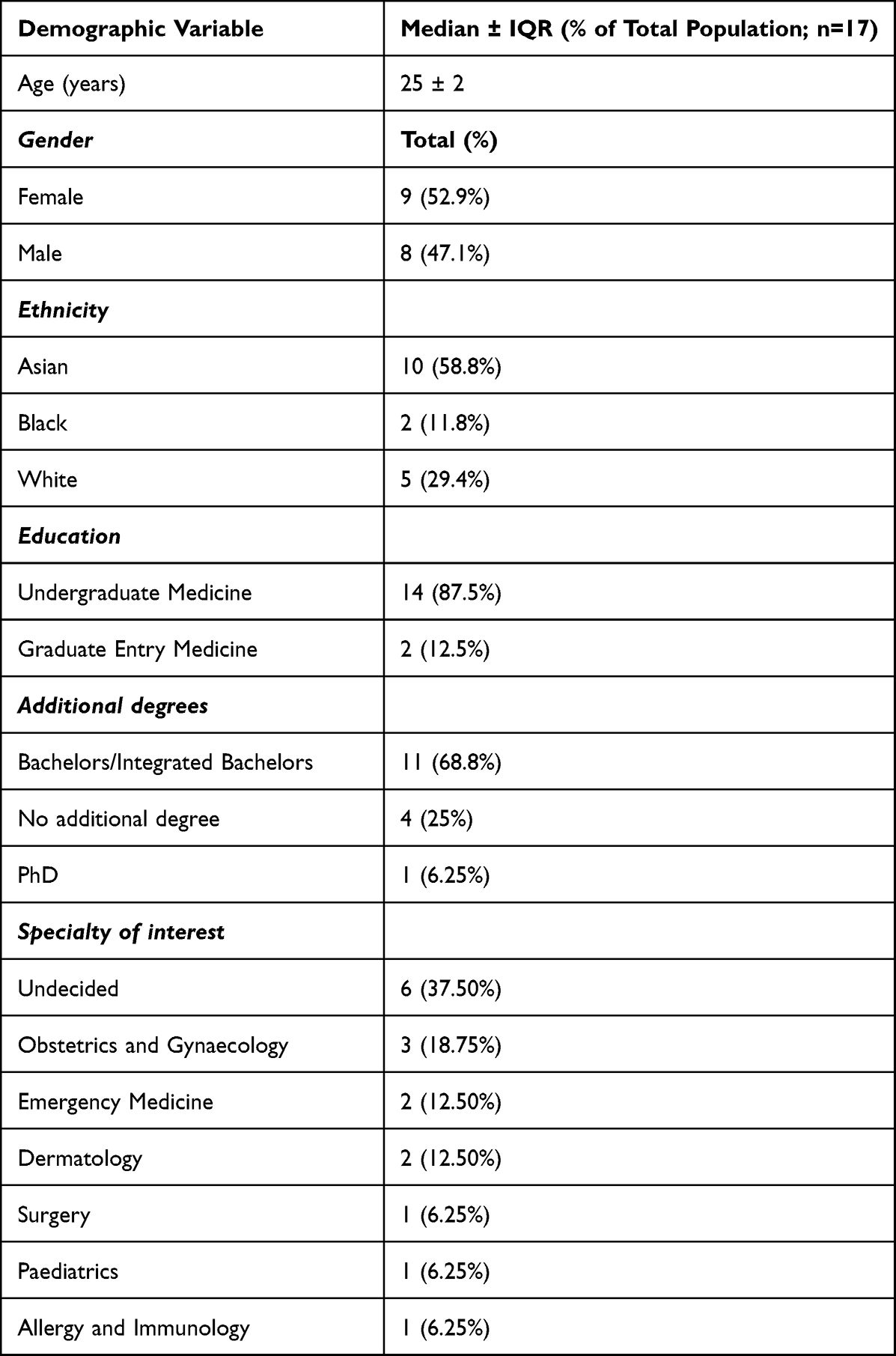 |
Table 1 Summary of Participant Demographics, Including Age, Gender, Ethnicity, Education, Additional Degrees and Specialty of Interest |
Survey results
Of the 17 participants who completed the pre-course questionnaire, 43.8% (n=7) of participants indicated that their knowledge base was inadequate to commence work as a foundation trainee, and 56.3% (n=9) did not feel confident about starting training. Median self-rated confidence in starting the Foundation Year 1 programme prior to the course was 2 (IQR 2–3), indicating that most participants did not feel very confident. The main aspects of foundation training that participants felt most concerned or anxious about included working independently, managing a large workload, prioritising tasks, prescribing medications, being on call, making decisions, managing acutely ill patients and remember knowledge from medical school after several months off.
Most participants (68.8%, n=11) had not previously attended a preparatory course for the Foundation Programme. Resources that participants used to prepare for training included websites (56.3%, n=9), university society events (50%, n=8), university resources (43.8%, n=7) and friends/colleagues (43.8%, n=7). However 68.8% (n=11) of participants found it difficult to locate relevant resources to do so.
Following the course, 14 participants completed the post-course survey. Overall, 92.9% (n=12) of respondents indicated improved knowledge and confidence in managing acute medical presentations than before the course, with statistically significant improvements in data across all the key topics covered (Figure 1). Median self-rated confidence across all topics following the course was 5 (IQR 4–5), an increase from a median of 3 (IQR 2–3) in the pre-course questionnaire. The topics that showed the largest increase in confidence included oxygen therapy (pre-course median of 2 (IQR 2–4), post-course median of 5 (IQR 4–5)); opioid prescribing (pre-course median of 2.5 (IQR 2–3), post-course median of 5 (IQR 4–5)); and lactate metabolism (pre-course median 1.5 (IQR 1–2), post-course median 4 (IQR 3–5)). The topics that showed least extent of improvement in confidence included acid-base balance (pre-course median of 3 (IQR 2–4), post-course median of 4 (IQR 4–5));, antibiotic prescribing (pre-course median of 3 (IQR 3–3), post-course median of 4 (IQR 4–5)); and anticoagulant prescribing (pre-course median of 3 (IQR 2–3), post-course median of 4 (IQR 4–5)).
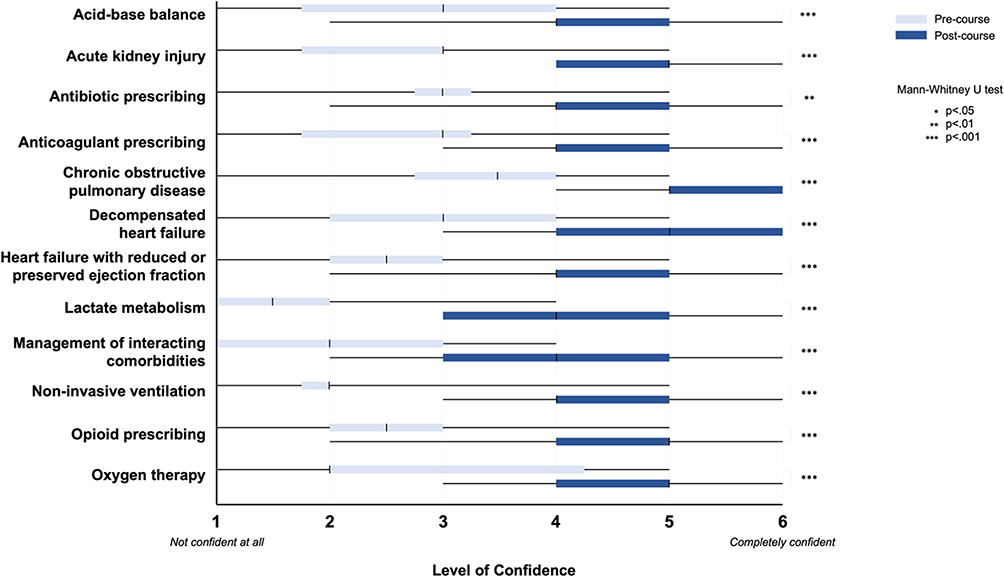 |
Figure 1 Median (±IQR and range) levels of confidence in acute medical presentations shown by participants before and after attending the course. |
Half of respondents of the post course survey (n=7) felt affected by the COVID-19 pandemic, although to varying extents. Participants who felt that their confidence was decreased following the COVID-19 pandemic included limited patient exposure, fewer opportunities to perform clinical skills, cancelled electives and exams with simulated patients precluding identification of “real” signs. On the other hand, half of the course participants cited that the COVID-19 pandemic did not impair their confidence and preparedness to commence work as a foundation trainee. One participant stated that they “don’t think [they] would have felt prepared either way”.
With regards to feedback on the course and its delivery, all (n=14) participants felt that the course enjoyable and 93% (n=13) found it as effective as face-to-face teaching. In particular, participants described the case-based structure and “having to commit to a decision or management plan” particularly useful. Furthermore, participants felt that the “diagrams” and “physiology explanations” were useful to set the clinical scenarios in context.
However, 50% (n=7) of participants found the course difficult to immerse themselves in and 42.9% (n=6) found it difficult to ask questions throughout. Suggested improvements included reducing the pace of the course, integrating additional breaks, including further interactive elements (eg opportunities to document blood test results or to take short histories), and dedicating time to the practicalities of the role (such as when to escalate treatment independently and when to seek senior support).
Thematic Analysis
Five primary themes emerged from the interviews:
- Concerns of final-year medical students before starting FY1: concerns about ward workload, prescribing, independent management, and integration within the medical team
- Reflections of recent graduates after starting FY1: challenges on transitioning from medical school to work, lack of confidence, lack of knowledge and work environment
- Effect of the COVID-19 pandemic on preparedness: impact of COVID-19 on formal teaching, information opportunities for learning, exposure to clinical knowledge and the use of online medical resources
- Lack of adequate resources available for Foundation Doctors: availability and usefulness of available resources
- Value of simulation programmes: benefits of simulation programmes and potential improvements
Theme 1: Concerns Before Starting FY1
Final-year medical students’ described numerous concerns surrounding starting FY1prior to graduation. Specifically, participants feared that medical school did not prepare them for triaging issues, looking for patient information on the hospital system and missing vital or emergency signs.
I was really stressed and (.) don’t know how to do anything. A lot of the stuff you learn on the wards and a lot of it jogs your memory. (VP1)
Participants thought that their concerns were further exacerbated by the long break between final-year exams and starting work as an FY1.
I think a big part of it is having a large gap between exams and starting [work]. Having gone on holiday and not doing anything made a big difference. (VP2)
Participants therefore agreed that a short course between final-year and starting FY1 could help ameliorate these concerns by providing a recap and preparation before starting the job.
Theme 2: Reflections After Starting FY1
Participants reported feeling that they were under large amounts of stress once starting work as an FY1 and agreed that having a transition course such as the one delivered in this study would have helped to build this confidence.
I also think the way we are assessed is very different to the knowledge you need on the wards. (.) if I see things written down, I’m good. But, on my feet, I’m not very confident. I think we almost need to get more of that. (VP1)
Participants reported that minimal amounts of the knowledge acquired throughout medical school was useful, and often exam assessments did not reflect or correlate to the knowledge required on the job.
I think that’s what medical school doesn’t teach us – the severity of issues. You know the immediate management of hyperkalaemia (…), but less about the practical stuff of what you need to do or who should be managing that. (VP3)
Most knowledge and confidence was gained through practice and with a supportive work environment. In addition, due to low expectations set by the hospital, FY1 doctors felt that they were provided with a lot of support and were not thrown into the deep end.
My hospital is very supportive, they’re really great. It’s so funny because their expectations are so low – in my head I thought they’d expect me to have consultant-level knowledge. Stuff you know from medical school – you don’t really use that in practicing medicine as much. (VP2)
Theme 3: The Effect of Covid-19 on Preparedness
A variety of responses were given regarding the effect of COVID-19 on their preparedness for work as a junior doctor. Overall, participants reported an increase in the use of healthy actors in their final practical exams, which was not reflective of clinical practice. This meant there was a reduced emphasis on learning pathological signs. This lack of preparedness was exacerbated by changes in the format of final exams and reduced clinical experience.
[The] only thing that may have been affected was that my PACES were on healthy actors rather than patients with signs. That automatically meant that there were a limited number of things I could prepare for – I didn’t go into hospital searching for signs or listening to different sounds, which is probably the best thing you could be doing to prepare. (VP2)
Despite the majority of participants reporting feeling much less prepared, some found that their confidence remained the same. There were no participants reporting increased preparedness.
I wasn’t affected too much by COVID. When the pandemic hit, I was in 4th year and I wasn’t on wards anyways, and by 5th year they had got us back into the wards. (VP1)
Further expanding on this theme, a topic that was explored was the use of online medical resources, which have substantially increased since the start of the pandemic. One participant reported feeling doubtful about undertaking the simulation-based training online and admitted that they would have found it more helpful if the course had been carried out in-person rather than online. However, they agreed that more simulation-based teaching was required and that testing in the format of an FY1 would be the most useful.
Theme 4: Lack of Adequate Resources Available for Foundation Doctors
Participants reported that despite a range of resources being provided to them to aid with the transition from being a medical student to junior doctor, most of the resources are not used and that “reading resources are not helpful till you do it for yourself” (VP1), which would be combated by using a simulation programme like the one provided. Current resources provide a good way to refresh knowledge, but not necessarily to learn new information.
[The course] helped as it helped to refresh my knowledge – I don’t think I learned particularly loads of new information, and I don’t know if in an emergency I would be thinking about about that, but it made me feel much more comfortable about recognising ‘yeah I know that, yeah I know that. (VP3)
Previous lectures were not helpful for improving their confidence. Simulation-based training was reported as being the most helpful as a learning opportunity for life as an FY1.
Theme 5: Value of Simulation Programmes
Overall, there was a positive outlook on the simulation course delivered. Participants reported that there were excellent explanations and good summaries. The acute clinical cases were particularly helpful, both as a refresher and for consolidation of knowledge. The course delivered in this study helped to identify and highlight gaps in their knowledge, increased their awareness of which topics were most high-yield and increased their confidence. However, participants did not report learning new knowledge. Interestingly, while the course did not teach participants new material, exposure to clinical cases helped to reinforce their existing knowledge base and refreshed their understanding of the management of unwell patients.
One participant cited that they “felt surprised by how much [they] knew and felt confident in” (VP1), a sentiment echoed in other responses. Some participants also reported that their confidence was improved through correctly answering questions integrated throughout the course, as well as through explanations of practical aspects not necessarily covered at medical school. Participants also noted that animated schematics, explanations of relevant physiology, and interactive quizzes were elements of the course they considered most useful.
I think Imperial should do more [simulations]. I think they’re starting to introduce them in third year. (.) I think that’s the most important thing as a junior doctor – being able to perform well in these [simulations] as that is really the thinking of your feet part and making snap decisions and noticing things. (VP1)
When asked about improvements that could be made to our programme and simulation-programmes in general, a common remark was the scheduling of breaks and not receiving physical handouts, although this is an expected limitation of undertaking a simulation-course in an online setting. In addition, participants stated that there was too much physiology and an extensive content amount, which, as mentioned before, they found was not as important for work as an FY1. Participants also felt that there needed to be more case-based scenarios.
[Improvements would be] to make it in person and do a [simulation] session after each section. So [for example] a section on hyperkalemia and lactic acidosis, but do a [simulation] session where you’re being bleeped about that situation – (.) you’re actually using the knowledge that’s been taught to you and implementing it in a way that you’d do as a doctor. (VP2)
Discussion
Our findings support the combination of near-peer and situation-based transition interventions as an effective and efficient means of improving perceptions of preparedness in recent medical graduates. Tailoring this intervention around an on-call shift allowed for targeted clinical reasoning and integrated multiple applied concepts at once, thereby representing a distinct alternative to conventional learning environments at medical school, such as consultant-led bedside teaching, tutorials or lectures. However, importantly, our findings highlight that certain high-yield topics, such as the prescribing for a patient with interacting comorbidities, require deeper interrogation than others, such as COPD alone, owing to their greater challenges in understanding and/or application of cross-curricular knowledge. It follows that such areas should be given more coverage in future transition interventions and/or supplemented with more immersive modes of learning.
In contrast to traditional methods of preparing medical graduates for the transition to foundation training, such as didactic lectures and simulated patient encounters, case-based transition courses offer a unique and potentially more effective approach. However, there are other factors that may contribute to preparedness. A recent systematic review identified that workplace factors (eg lack of support and constructive feedback from seniors), medical school programmes (eg early clinical exposure) and personal factors (eg lack of self-confidence and ability to deal with uncertainty) may play a role.7 Transition interventions address the latter two by immersing medical graduates in authentic clinical cases, allowing them to apply their knowledge and skills in context. Additionally, case-based learning promotes critical thinking in the face of uncertainty, problem-solving, and confidence in decision-making skills, which are crucial for successful clinical practice. However, without addressing the other factors, particularly workplace factors, this may not be adequate alone. Combining transition courses with guidance on seeking support during training, managing a lack of continuity and learning with a lack of valuable feedback, may enhance the impact of these courses on preparedness.
We recognise that this study has several limitations. Most importantly, this is a pilot study, with small sample size from a single university in London, which limits generalisability to the entire UK medical student population. There may also be a strong degree of selection bias; as the course was optional, students who feel less confident in starting training may be more inclined to attend. This study also did not formally assess participants’ knowledge in the clinical domains covered and relied only on self-reported data. Finally, the study also did not follow-up participants long-term; it is possible that later into their foundation training their level of confidence of preparedness would have changed, and their view of the value of the course therefore be different.
Further research in this area is critical in understanding how the transition from medical student to junior doctor, and beyond may be eased. A national collaborative effort is especially warranted to investigate whether situation-based transition interventions represent an effective stand-alone means of alleviating the steep learning curve, or whether alternative or supplementary interventions may be more effective. Randomised trials comparing the efficacy of similar interventions may enable further optimisation of course delivery (eg online, non-online, or hybrid, or delivered by junior doctors, consultants, or other allied health professionals). Longitudinal studies which follow final-year medical students prior to the transition through to the first year of training may also ascertain the combination of qualitative and quantitative factors which may ease this transition from student to doctor and, perhaps more importantly, have wider implications for patient care.
Following the outcomes of these studies, recommendations for the implementation of situation-based transition interventions into medical school curricula could be made. This addresses the important argument surrounding the cost of such courses. Although the medical school curriculum is theoretically designed to prepare students for working life as a doctor, the growing interest in transition courses indicates that this may not be the case. This may be due to learning fatigue and lack of retention following completion of exams. Currently, medical students and junior doctors hoping to refresh their knowledge are expected to fund these courses themselves. Implementing short-term situation-based transition courses into the medical school curricula or providing medical students with financial support could be a solution. Another consideration is making the price of these courses accessible to all, as has been done in this study.
In summary, this study provides evidence in support of near-peer and short-term situation-based courses with the aim of enhancing medical students’ knowledge and confidence for foundation training. These findings add to the growing evidence-base encouraging implementation of short-term courses in preparing for practice. However, further research on the utility of such transition interventions and how to best teach content that requires cross-curricular knowledge will be vital to inform the development of evidence-based recommendations for recent medical graduates, educators and programme directors. Furthermore, funding of these courses is an important consideration.
Abbreviations
FY1, Foundation Year 1; GMC, General Medical Council; ICSM, Imperial College School of Medicine.
Data Sharing Statement
Data from pre- and post-course questionnaires have been made available on an Microsoft Excel spreadsheet. This data is anonymous.
Disclosure
ADB, AMCP and LR are executive members, and JX and NB are non-executive members of the charity, Make a Medic, that delivered this course. They are all volunteers and the success of the organisation bears no monetary benefit to them.
References
1. Michaelides A, Mahr M, Pydisetty G, Loyala JV. Assessing the preparedness of foundation year 1 (FY1) doctors during the transition from medical school to the foundation training programme. BMC Med Educ. 2020;20(1):106. doi:10.1186/s12909-020-01999-5
2. Goldacre MJ, Lambert T, Evans J, Turner G. Preregistration house officers’ views on whether their experience at medical school prepared them well for their jobs: national questionnaire survey. BMJ. 2003;326(7397):1011–1012. doi:10.1136/bmj.326.7397.1011
3. Monrouxe LV, Grundy L, Mann M, et al. How prepared are UK medical graduates for practice? A rapid review of the literature 2009–2014. BMJ Open. 2017;7(1):e013656. doi:10.1136/bmjopen-2016-013656
4. Monrouxe L, Bullock A, Cole J, et al. How prepared are UK medical graduates for practice? Final Report from a Programme of Research Commissioned by the General Medical Council; 2014.
5. Monrouxe LV, Bullock A, Gormley G, et al. New graduate doctors’ preparedness for practice: a multistakeholder, multicentre narrative study. BMJ Open. 2018;8(8):e023146. doi:10.1136/bmjopen-2018-023146
6. Illing J, Morrow G, Kergon C, et al. How prepared are medical graduates to begin practice? A comparison of three diverse UK Medical Schools. Final Report to GMC April 2008; 2008.
7. Cameron A, Millar J, Szmidt N, Hanlon K, Cleland J. Can new doctors be prepared for practice? A review. Clin Teach. 2014;11(3):188–192. doi:10.1111/tct.12127
8. Teagle AR, George M, Gainsborough N, Haq I, Okorie M. Preparing medical students for clinical practice: easing the transition. Perspect Med Educ. 2017;6(4):277–280. doi:10.1007/S40037-017-0352-2
9. Blencowe NS, Van Hamel C, Bethune R, Aspinall R. “From scared to prepared”: targeted structured induction training during the transition from medical school to foundation doctor. Perspect Med Educ. 2015;4(2):90–92. doi:10.1007/S40037-015-0168-X
10. General Medical Council. Tomorrow’s doctors: outcomes and standards for undergraduate medical education; 2009.
11. Laack TA, Lones EA, Schumacher DR, Todd FM, Cook DA. Sharing simulation-based training courses between institutions: opportunities and challenges. Adv Simulat. 2017;2(1):1. doi:10.1186/s41077-016-0034-x
12. Kerr B, Lee-Ann Hawkins T, Herman R, et al. Feasibility of scenario-based simulation training versus traditional workshops in continuing medical education: a randomized controlled trial. Med Educ Online. 2013;18(1):21312. doi:10.3402/meo.v18i0.21312
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.