")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Evaluating Upadacitinib in the Treatment of Moderate-to-Severe Active Ulcerative Colitis: Design, Development, and Potential Position in Therapy
Authors Napolitano M, D'Amico F, Ragaini E , Peyrin-Biroulet L, Danese S
Received 8 April 2022
Accepted for publication 3 June 2022
Published 17 June 2022 Volume 2022:16 Pages 1897—1913
DOI https://doi.org/10.2147/DDDT.S340459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Maria Napolitano,1,* Ferdinando D’Amico,1,2,* Elisa Ragaini,2,* Laurent Peyrin-Biroulet,3,4 Silvio Danese1
1Gastroenterology and Endoscopy, IRCCS Ospedale San Raffaele and Vita-Salute San Raffaele University, Milan, Italy; 2Department of Biomedical Sciences, Humanitas University, Milan, Italy; 3Department of Gastroenterology, University of Lorraine, CHRU-Nancy, Department of Gastroenterology, Nancy, F-54000, France; 4Inserm, NGERE, University of Lorraine, Nancy, F-54000, France
*These authors contributed equally to this work
Correspondence: Silvio Danese, Gastroenterology and Endoscopy, IRCCS Ospedale San Raffaele and Vita-Salute San Raffaele University, Via Olgettina 60, Milan, Italy, Tel/Fax +39 0226432069, Email [email protected]
Abstract: Upadacitinib is a selective small molecule that inhibits Janus kinase (JAK) type 1. This molecule is administrated orally and is currently approved for the treatment of rheumatoid arthritis, atopic dermatitis, and psoriatic arthritis. Upadacitinib has been approved by the United States Food and Drug Administration for the induction and maintenance therapy of moderate-to-severe ulcerative colitis (UC) and is under investigation by the European Medicines Agency. Data from two induction and two maintenance Phase III randomized controlled trials (RCTs) proved the efficacy of upadacitinib in achieving clinical and endoscopic remission in patients with moderate-to-severe UC, regardless of previous inadequate response to other biologic therapies. The most frequently reported adverse events in the induction trials were acne, creatine phosphokinase increase, nasopharyngitis, headache, and anemia, while in the maintenance studies nasopharyngitis, elevation of creatine phosphokinase, UC exacerbation, upper respiratory tract infection, arthralgia, and anemia were reported. A limited proportion of upadacitinib-treated patients experienced adverse events of special interest, like herpes zoster infections or thromboembolic events, indicating a reliable safety profile. The aim of this review is to summarize the available evidence on upadacitinib in UC providing useful insights about the positioning of this drug in the therapeutic algorithm.
Keywords: upadacitinib, small molecule, JAK1 inhibitor, ulcerative colitis, inflammatory bowel disease
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) characterized by continuous inflammation of the colon that usually requires lifelong therapy due to a remitting and relapsing course.1 To date, several options are available besides the traditional steroid or immunosuppressive therapies including tumor necrosis factor α (TNFα) inhibitors, integrin inhibitor, interleukin (IL) 12–23 inhibitor, and tofacitinib.2 Despite the expansion of therapeutic armamentarium for UC, primary or secondary failures occur in up to 46%, emphasizing the need for new drugs.3 Among the new molecules under investigation for IBD, Janus Kinase inhibitors (JAKi) are of great interest. These molecules belong to the family of small molecule drugs (SMDs) and they are already in use for several autoimmune conditions.4 JAKi are orally administrated and target an entire molecular pathway, the JAK/Signal Transducer and Activator of Transcription (STAT) pathway, differently from the selective blockage of a single molecule mechanism of monoclonal antibodies.4 The activation of these pathways is involved in many cellular functions including hematopoiesis, lymphocytes differentiation, and viral immunity.5
Tofacitinib, a pan-JAKi, was the first small molecule approved in 2018 by United States Food and Drug Administration (FDA) and European Medicines Agency (EMA) for treatment of moderate-to-severe UC.6,7 This drug proved to be rapidly effective for the induction of remission in patients with moderate-to-severe UC.8 However, concerns still remain about its safety profile, since cases of thrombosis, dyslipidemic disorders, and Herpes zoster reactivation were recorded.9 Actually, the most involved pathway in IBD immune response is mediated by JAK1 isoform, justifying the development of selective JAK1 inhibitors in order to have an improved safety profile.10 Upadacitinib (UPA) is a new selective JAK1 inhibitor currently approved for the treatment of rheumatoid arthritis (RA), atopic dermatitis (AD), and psoriatic arthritis, and is under evaluation for the management of UC and Crohn’s disease (CD).11 The aim of this review is to summarize the available literature about UPA and position this new molecule among the therapeutic options for moderate-to-severe UC.
Methods
For this review, we searched in PubMed, Embase, clinicaltrials.gov, and Scopus databases to find all studies about the use of UPA in UC up to March 2022. We used the following search terms: “UC”, “ulcerative, colitis”, “inflammatory bowel disease”, “IBD” in combination with “upadacitinib”, “JAK inhibitors”, “anti-JAK”, “selective drug”, “small molecule”. We also considered abstracts from the main international congresses (United European Gastroenterology week, European Crohn’s and Colitis Organisation, and Digestive Disease Week). Three authors (MN, FD, and ER) independently selected and examined all the suitable articles, including the references for any additional work.
Mechanism of Action
UPA is a selective JAK1 inhibitor.12 The JAK/STAT family includes four types of tyrosine kinases (JAK1, JAK2, JAK3, and tyrosine kinase 2, TYK2), associated with intracellular domains. The cytokine binding with the extracellular receptor of JAKs causes dimerization of the intracellular domain and its subsequent activation.13 Once activated, JAKs phosphorylate themselves and reach the nucleus, where they bind DNA sequences and regulate gene expression.14,15 The activation of the JAK/STAT pathway is mediated by different cytokines and each cytokine receptor is associated with a JAK monomer.13 The main cytokines leading to the activation of JAK/STAT pathway are IL-6, IL-12, IL-23, IL-13, IL-10, and interferon γ (IFNγ). All these cytokines have different roles in the immune response and are involved in the pathogenesis of IBD.16 JAKs are composed of seven homologous domains (JH1–7). The JH5–7 domains are significant for the receptor binding, while the JH1 kinase region is a catalytic domain and is critical for the pathway activation, with a high grade of homology in the different isoforms.17
The selectivity of JAKi decreases at higher doses, because the isoform selectivity depends on the difference between concentration needed to inhibit 50% of activation (IC50) for different JAK isoforms.18 For this reason, UPA is selective for JAK1 but at higher doses it can inhibit JAK2 and, to a minor extent, JAK3 and TYK2.18 Differently from monoclonal antibodies, UPA has a low molecular weight, usually <1 kDa and passes easily through cell membranes to the intracellular space. In addition, in contrast to monoclonal antibodies, it is non-immunogenic and has a more stable structure.19 A Phase 1 trial by Mohamed et al investigated the pharmacokinetic profile of UPA. It has a 4-hour half-life and 80% hepatic metabolism, mediated mostly by cytochrome P450 34A (CYP3A4) and to a lesser extent by CYP2D6.20 According to an open-label, multiple-dose, two-period study on the effect of repeated doses of UPA 45 mg on the pharmacokinetics of CYP enzymes in healthy adults, the impact of daily UPA administration on midazolam (CYP3A) and dextromethorphan (CYP2D6) exposures was limited, while no relevant effects on the sensitive probe substrates for CYP1A2, CYP2C9 and CYP2C19 were recorded.21
UPA is eliminated unchanged for 24% in urines and 38% in feces, while approximately 34% of dose is excreted as metabolites. To date, no UPA active metabolites are known.20 Dose adjustment is not necessary in patients with renal and hepatic impairment, but effects on end stage renal failure have not been investigated, while UPA is not recommended in patients with severe hepatic impairment. No differences in clinical effect were observed in patients depending on body weight and age, even if there was a higher rate of overall adverse events (AEs), like serious infections, in the elderly population (>75 years).22 Limited data are available on the use of UPA in pregnant women and during lactation, but studies in rabbits and rats showed reproductive toxicity and excretion of UPA in milk; therefore, UPA is not recommended during pregnancy and breastfeeding.22 Pharmacokinetics and pharmacodynamics characteristics of UPA are summarized in Table 1.
 |
Table 1 Pharmacokinetic and Pharmacodynamic of UPA |
Efficacy Data in UC
Firstly, a Phase 2 double blind randomized trial tested the efficacy of UPA in patients with moderate-to-severe UC refractory to conventional therapies, the U-ACHIEVE study.23 In this dose-ranging, placebo-controlled trial, 250 patients were randomized in five arms receiving placebo, UPA 7.5 mg, 15 mg, 30 mg, or 45 mg once a day (QD) for 8 weeks. The primary endpoint was clinical remission at week 8 defined according to the adapted Mayo score as stool frequency subscore of ≤1, rectal bleeding subscore (RBS) of 0, and endoscopic subscore of ≤1. Main secondary endpoints were endoscopic improvement (endoscopic Mayo subscore ≤1 at week 8) and clinical response according to the adapted Mayo score at week 8, defined as decrease from baseline in the adapted Mayo score of ≥2 points and ≥30% and decrease in rectal bleeding subscore (RBS) of ≤1 or RBS ≤1). Other secondary endpoints were clinical response at week 2 (decrease from baseline in the partial Mayo score of ≥2 points and ≥30% from baseline, decrease in RBS of ≥1 or RBS ≤1), endoscopic remission (endoscopic subscore of 0), and histologic improvement (any grade of reduction of Geboes Score from baseline) at week 8.
Concerning the primary endpoint, a general dose-response relationship was observed. In particular, clinical remission was achieved in a greater proportion of patients treated with UPA, respectively, those receiving UPA 45 mg (19.6%, P = 0.002), 30 mg (13.5%; P = 0.011), 15 mg (14.3%; P = 0.013) and 7.5 mg (8.5%; P = 0.052), compared to the placebo group (0% of patients). Among secondary endpoints, endoscopic improvement, clinical response and endoscopic remission and histologic improvement at week 8 were reported in more patients receiving any dose of UPA compared to placebo. [Table 2]
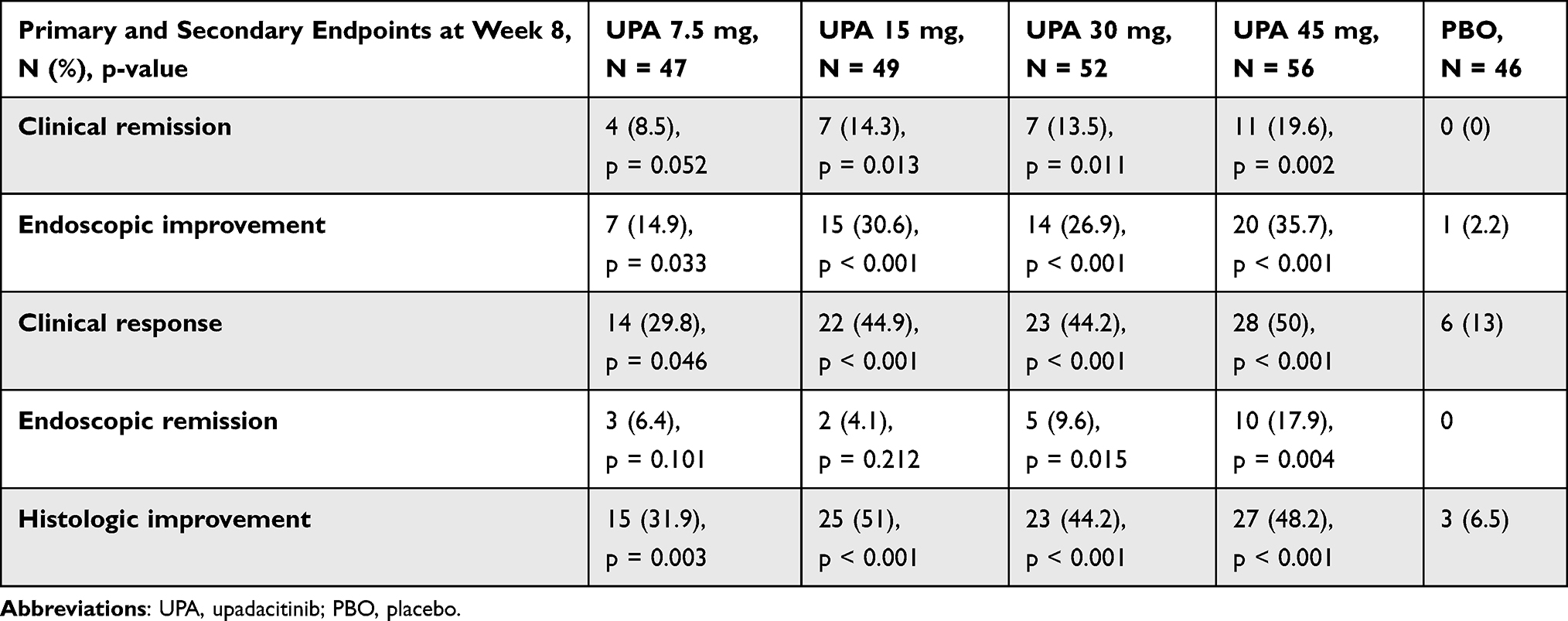 |
Table 2 Efficacy of UPA in U-ACHIEVE Phase 2 Trial |
Changes from baseline in C-reactive protein (CRP) concentrations at week 8 were greater for all UPA treated groups compared with placebo, with median decrease ranging from –0.340 to –4.355. Also, median fecal calprotectin reduction at week 8 was higher for UPA groups, from –338.0 to –720.0.23
Two Phase 3 multicenter, randomized, double-blind, placebo-controlled trial, U-ACHIEVE and U-ACCOMPLISH induction studies, randomized patients 2:1 to UPA 45 mg QD or placebo for 8 weeks.9 Results from these trials confirmed significant greater proportion of patients achieving the primary endpoint of clinical remission at week 8 with UPA 45 mg QD compared to placebo (26.1% vs 4.8% and 33.5% vs 4.1%, respectively, p < 0.001).9
Histologic endoscopic mucosal improvement (HEMI) and mucosal healing (endoscopic score = 0 and Geboes score <2.0) were also achieved at week 8 in a significant greater number of patients treated with UPA in both U-ACHIEVE induction study (respectively, 30% and 10.7% versus 6.6% and 1.3% in placebo group) and U-ACCOMPLISH induction study (36.7% and 13.3% versus 5.8% and 1.7%).24 Rates of clinical response at week 2 and week 8 and endoscopic improvement and endoscopic remission at week 8 were achieved in a significant higher number of subjects receiving UPA 45 mg QD versus placebo (p < 0.001 for all endpoints).9 Concerning mucosal healing (MH), patients who achieved the histology threshold for MH (Geboes score <2.0) at the end of U-ACHIEVE induction study had a significant greater probability to reach clinical remission (OR 1.8, p < 0.03) and endoscopic improvement (OR = 1.8, p < 0.015) at week 52. Similarly, clinically meaningful improvements in Ulcerative Colitis Symptoms Questionnaire (UC-SQ), Inflammatory Bowel Disease Questionnaire (IBDQ), physical component summaries of Short Form 36 (SF-36), and European Quality of Life-5 Dimensions and 5 Levels (EQ-5D-5L) index scores (p < 0.001, p = 0.01, p = 0.018, p = 0.009, respectively) were found, suggesting an association between MH and long-term clinical and patient-reported outcomes.25 Moreover, in a subset of patients from the U-ACHIEVE study, modulation of genes associated with UC disease activity, B-cell responses barrier function, and wound repair were observed in colonic mucosa at week 8 in UPA treated patients versus placebo. These changes were associated with clinical response, clinical remission, histologic and endoscopic improvement.26
For those patients who failed the 8-week induction phase, prolonged exposure to UPA for 16 weeks led to achievement of clinical response in 48.3% of cases. Patients were re-randomized in the U-ACHIEVE maintenance study, receiving 15 mg QD, 30 mg QD or placebo.27 The primary endpoint of clinical remission at week 52 was reported with higher rates in patients receiving UPA 30 mg QD and UPA 15 mg QD versus placebo (52%, 42% and 12%, respectively, p < 0.001), while secondary endpoints are reported in Table 3, showing significant differences between both UPA 15 mg and UPA 30 mg QD arms and placebo.27
 |
Table 3 Efficacy of UPA in U-ACHIEVE Maintenance Study |
Patients who failed to achieve clinical response at week 8 in U-ACHIEVE induction study were treated with UPA 45 mg for further 8 weeks in an open-label extension and responders were randomized 1:1 to UPA 15 mg and UPA 30 mg in the U-ACHIEVE maintenance study.28 Among these patients, rates of clinical remission, maintenance of clinical response, and endoscopic improvement at week 52 were superior to placebo (respectively, 33.3% vs 19.0%, 66.7% vs 35.7%, and 37.5% vs 23.8% of those who received UPA 30 versus UPA 15 mg QD as maintenance treatment).28
According to the results of U-ACHIEVE maintenance study, UPA 30 mg QD showed higher maintenance remission rate compared to UPA 15 mg QD, especially in patients with severe disease (full Mayo score >9) rather than in those with moderately active disease (31.2–50.4% vs 53.1–54.2% respectively).29 Interestingly, a significantly higher number of patients experienced no abdominal pain in UPA 15 mg group at week 8 (60.8% vs 48.3%, p < 0.05) and in UPA 30 mg group at week 12 (59.7% vs 43.6%, p < 0.01) compared to placebo.30 These differences were maintained at week 52 both in 15 mg QD (45.9%) and 30 mg QD (55.3%) arms versus placebo (20.8%, p < 0.001) and similar results were observed for no bowel urgency reported with UPA 30 mg at week 4 (68.8% vs 54.4%, p < 0.05) and with UPA 15 mg at Week 8 (64.9% vs 49.7%, p < 0.01), maintaining significant difference at week 52 (15 mg: 56.1%; 30 mg: 63.6% vs placebo: 17.4%, p < 0.001).30
Stratifying the results based on baseline corticosteroid (CS) use, no benefits emerged with CS, with significantly higher achievement of CS-free clinical remission at week 52 (CS free for ≥90 days immediately prior to week 52) with UPA 30 and 15 mg than placebo (p < 0.001).31
Additionally, UPA 45 mg QD was effective versus placebo in the induction of clinical remission in patients with moderate-to-severe UC regardless of previous treatment failure of biologic therapies, with higher difference in remission percentage for the non-biologic inadequate response group versus the biologic inadequate response group (26% versus 17.5% in U-ACHIEVE and 31.6% versus 27.1% in U-ACCOMPLISH).32
UPA proved also to be effective for the management of extraintestinal manifestations (EIMs) in a post-hoc analysis from the UPA Phase 3 program. The most common EIMs at baseline were anemia (14%), peripheral (10.7%) and axial (2.1%) arthropathy. The proportion of patients with resolution of any EIM (40% vs 33.3%), arthropathy (54.7% vs 42.1%) or anemia (38.2% vs 32.6%) at week 8 was higher in UPA 45 mg QD group than placebo in the induction studies. The resolution at week 52 of any EIM in patients presenting ≥1 EIM at baseline was significantly higher in UPA 30 mg QD (p < 0.001) versus placebo.33
Safety Data in UC
A recent systematic review and meta-analysis including 43 studies (74.4% randomized clinical trials and 25.6% observational cohort studies) investigated safety of JAK inhibitors in IBD, rheumatoid arthritis (RA), psoriasis (PSO), and ankylosing spondylitis (AS). The overall incidence rate of AEs in JAKi-treated patients was 42.65 per 100 person-years, while serious adverse events (SAEs) were detected in 9.98 cases per 100 person-years. Incidence rates of AEs and SAEs in patients undergoing UPA therapy were, respectively, 133.52 and 12.66 per 100 person-years. Serious infections occurred in 2.16 cases per 100 person-years.34
According to the results from U-ACHIEVE induction study, overall AEs and SAEs throughout 8 weeks were reported more frequently in patients receiving placebo (60% and 5.8%) compared to patients receiving UPA 45 mg QD (56.4% and 2.5%).9 Most common AEs in UPA treated patients were acne (4.7%), creatine phosphokinase increase (4.7%), nasopharyngitis (4.7%), headache (4.1%), and anemia (2.2%). Serious infections occurred in 5 cases (1.6%) in UPA group and in 2 cases in placebo group (1.3%). Of note, one case of herpes zoster infection was observed with UPA (0.3%). In the U-ACCOMPLISH induction study, a higher rate of any AEs was detected in the UPA 45 mg QD arm compared with placebo (52.9% versus 39.5%). The U-ACHIEVE maintenance study confirmed that overall AEs were more frequent in the placebo group compared to both UPA 15 mg and UPA 30 mg arms (505.1 cases per 100 person-years versus 327.8 and 318 cases per 100 person-years respectively). Likewise, onset of SAEs was higher in the placebo group (21.9 cases per person-years) than the UPA 15 mg (12.6 cases per person-years) and UPA 30 mg (10.6 cases per person-years) groups.35 AEs leading to treatment discontinuation were reported in 6 cases per 100 person-years in both UPA 15 mg and UPA 30 mg arms, compared to 20.3 cases per 100 person-years of the placebo group. Most frequently reported AEs were nasopharyngitis, elevation of creatine phosphokinase, UC exacerbation, upper respiratory tract infection, arthralgia, and anemia, as reported in Table 4. Higher rates of herpes zoster (6 cases per 100 person-years vs no cases), creatine phosphokinase increase (7.7–11.1 cases per 100 person-years vs 3.9), hepatic disorder (17.5–9.1 cases per 100 person-years vs 5.5), and venous thromboembolism (VTE) (1.0–1.1 cases per 100 person-years vs no cases) were found in the UPA arms than in placebo arm. Conversely, lower rates of anemia were observed in the UPA groups compared to placebo (6 and 3.5 cases per 100 person-years vs 14.8). Non-melanoma skin cancer (NMSC) was reported with UPA 30 mg (1.0 cases per 100 person-years) but not in the UPA 15 mg arm, while 2 major cardiovascular events (MACEs) were observed (one in the placebo group and one in the UPA 30 mg arm). VTE was reported only with UPA treatment (1.0–1.1 cases per 100 person-years).35 No deaths occurred in the induction and maintenance studies. Safety events were stratified based on plasma exposure to UPA. No new safety events were identified (eg, >2 g/dL decrease in hemoglobin, hemoglobin <8 g/dL, lymphopenia ≥ grade, 3, neutropenia ≥ grade, 3, Herpes Zoster infection, serious infections, and pneumonia).36
 |
Table 4 Most Frequently Reported AEs with UPA in U-ACHIEVE Maintenance Study |
Efficacy and Safety in Other Immunomediated Inflammatory Diseases
UPA was evaluated as induction and maintenance therapy in mild-to-moderate CD patients in a randomized Phase II trial, the CELEST study, including 180 patients with mild-to-moderate CD.37 Patients were randomized to placebo or UPA 3-mg, 6-mg, 12-mg, or 24-mg twice daily or 24-mg once-daily oral doses.37 The primary endpoint of clinical remission (defined as average daily stool frequency of 1.5 and abdominal pain score of 1.0, with neither worse than the baseline value) at week 16 was achieved more with UPA compared to placebo, with no clear dose response between the different UPA arms, but with numerically higher rate in UPA 6 gm twice a day (BID) (27%, p < 0.10). Moreover, CS-free remission rate was significantly higher in patients receiving UPA 24 mg BID compared to placebo (33% vs 0%, p < 0.05). The co-primary endpoint of endoscopic remission (defined as Simple Endoscopic Score for Crohn’s Disease, SES-CD of ≤4 and a ≥2-point reduction from baseline, with no subscore >1) at week 16 was achieved in 14% of patients receiving UPA 24 mg QD and 22% of patients receiving UPA 24 mg BID (p < 0.05 and p < 0.01, respectively), compared to none of patients receiving placebo. Among patients who achieved clinical response (defined as a ≥30% reduction from baseline in stool frequency and/or abdominal pain score) at week 16, clinical remission and endoscopic remission at week 52 were not significantly different among UPA groups but with highest rate among patients receiving 12 mg BID (63% vs 41% for clinical remission and 38% vs 24% for endoscopic remission, p < 0.1).
Incidence of any AEs in the induction study was higher in the UPA 12 mg BID arm (27.8%) compared to other UPA arms (from 5.4% to 20%) and placebo (5.4%). Serious infections occurred more frequently in patients treated with any dosage of UPA (from 0% to 8.3%) than placebo (no cases) during the induction phase, and only one case of herpes zoster was reported in the 24 mg BID arm (2.8%). No deaths occurred.
UPA, as mentioned before, has been studied in other immunomediated diseases.38 UPA demonstrated to be effective in monotherapy compared to continuing methotrexate in RA patients for the achievement of American College of Rheumatology criteria 20 (ACR20) response, defined as 20% improvement in the ACR criteria (68% with UPA 15 mg and 71% with UPA 30 mg versus 41% in the continued methotrexate group, p < 0.0001) and a score of less than or equal to 3.2 in the 28-joint disease activity score using C-reactive protein (DAS28[CRP]) (45% with UPA 15 mg and 53% with UPA 30 mg vs 19% in the continued methotrexate group, p < 0.0001) at week 14.38,39 Importantly, UPA was compared to adalimumab, while continuing to take a stable dose of methotrexate (MTX), in a Phase III, double-blind, randomized controlled trial in RA patients.40 In this study, the primary endpoints of ACR20 improvement (71% in the UPA group compared to 36% in the placebo group) and a DAS28-CRP score of <2.6 (29% with UPA vs 6% with placebo) were significantly achieved at week 12 (p ≤ 0.001). UPA was also superior to adalimumab to reach the ACR 50% (ACR50) improvement response criteria (45% with UPA, 29% with adalimumab, 15% with placebo, p < 0.001), a DAS28-CRP score of ≤3.2 (29% with UPA, 18% with adalimumab and 6% with placebo, p < 0.001) and obtaining low disease activity or remission at week 26 (p ≤ 0.001).40 Concerning safety data in RA studies, the most reported AEs were nausea, nasopharyngitis, upper respiratory tract infections, headache, urinary tract infections, and worsening of RA. Low incidence of SAEs was reported, but with higher rates in UPA groups versus placebo groups. Few cases of herpes zoster infections, MACEs, and VTE occurred in UPA treated patients.39–42
UPA demonstrated significant efficacy against placebo in the treatment of moderate-to-severe atopic dermatitis (AD) in patients with inadequate control by topical treatment. In a phase II study, higher rates of improvement were found in Eczema Area and Severity Index (EASI) from baseline at week 16 (39% with UPA 7.5 mg, 62% with UPA 15 mg and 74% with UPA 30 mg versus 23% for the placebo group, p < 0.001).43 Most frequently observed AEs were acne, upper respiratory tract infection, nasopharyngitis, headache, elevation in plasma creatine phosphokinase levels, and worsening of AD. Serious infections and herpes zoster infection rates were higher in patients treated with UPA compared to placebo or comparators.44–47
Recently, EMA approved UPA for the treatment of active psoriatic arthritis (PsA) and ankylosing spondylitis (AS) not responsive to conventional therapies.48 Efficacy data from two randomized trials (SELECTPsA 1 and SELECTPsA 2) showed ACR20 response in higher proportion of PsA patients receiving UPA compared to placebo or adalimumab (70.6–78.5% versus 36.2% and 65.0%, respectively, p < 0.001).49,50 In a randomized controlled trial (SELECT-AXIS 1) significantly more AS patients met the primary endpoint (Assessment of SpondyloArthritis international Society 40% improvement [ASAS40] response) at week 14 in the UPA group versus the placebo group (52% vs 26%; p = 0.0003). Safety data in these studies were similar to previously reported data in RA and AD, with no new safety issues in the UPA treated patients.49–51, More detailed safety data from studies testing UPA in RA, AD, PsA and AS are reported in Table 5.
 |  |  |  |
Table 5 Safety of UPA in Other Immunomediated Diseases |
Discussion
Several new drugs have been tested during the last decades for the management of UC. This effort is driven by the increasing necessity of more effective and rapid molecules, a better safety profile, and an easier administration route, in order to provide a better quality of life for patients. Efficacy data from U-ACHIEVE and U-ACCOMPLISH induction and maintenance trials provided promising results about UPA. [Figure 1] UPA was recently approved by the FDA for the treatment of moderate to severe UC and is being evaluated by the EMA.52 UPA has a rapid mechanism of action owing to its pharmacokinetics and fast half-life. Indeed, a significant improvement of symptoms was observed as early as day 1 after UPA therapy and a higher likelihood of achieving clinical remission or clinical response at week 8 were reported in patients treated with UPA.53 Moreover, the oral administration route can improve patients’ quality of life, reducing the number of accesses to the hospital and lost workdays.54,55 In fact, a significantly greater proportion of patients who responded to UPA induction phase maintained improvements in health-related quality of life (HRQOL) compared to placebo after 52 weeks of maintenance treatment.
 |
Figure 1 Pros and cons of upadacitinib in patients with moderate-to-severe ulcerative colitis. Note: The figure shows the benefits and limitations of using upadacitinib in patients with ulcerative colitis. |
UPA is a small molecule with a selective mechanism of action, differently from tofacitinib, a pan-JAK inhibitor. One of the major concerns about JAK inhibitors is the risk of VTE and herpes zoster infections. Most safety data about JAKi come from studies on RA, showing higher rates of MACE (hazard ratio (HR) = 1.33, 95% confidence interval [CI], 0.91 to 1.94) and cancer (HR = 1.48 95% CI, 1.04 to 2.09) in patients treated with tofacitinib compared to anti-TNF inhibitor.56 Also, adjudicated opportunistic infections, nonserious and serious herpes zoster infections, and adjudicated nonmelanoma skin cancer occurred more often with tofacitinib than with a TNF inhibitor.56 However, it should be considered that UPA is a selective drug with a better safety profile than tofacitinib and that long-term data of tofacitinib in UC did not show an increased risk of thromboembolic or cardiovascular events.57 In addition, it is not reliable to extrapolate the data from rheumatological conditions as UC and RA are different diseases as demonstrated by the different etiopathogenesis, the age of onset of disease and the available therapies. According to a meta-analysis evaluating the thrombotic risk with JAKi in immuno-mediate disorders, no increased risk of VTE, pulmonary embolism (PE), and deep vein thrombosis (DVT) events was found in patients receiving JAK inhibitors.58 Interestingly, another meta analysis including patients with immune-mediated disorders showed a higher relative risk (RR) of herpes zoster among patients exposed to tofacitinib or baricitinib (1.50 95% CI 0.76–2.96, and RR 2.05, 95% CI 0.99–4.24) versus filgotinib or upadacitinib (1.28, 95% CI 0.32–5.07, and 1.09 95% CI 0.41–2.86).34 A further meta analysis confirmed that there was no increased risk for herpes zoster infection in patients treated with UPA.59 The occurrence of thromboembolic AEs could be prevented by carefully evaluating risk factors and by preferring the administration of these molecules in patients of young age and at low risk of thromboembolic events. Regarding herpes zoster infection, patients should get vaccination against the virus before starting therapy.60 To date, a recombinant herpes zoster vaccine is available and it is recommended for patients with IBD receiving immunosuppressive therapy.61–63
UPA should not be administrated during pregnancy, because of potential teratogenic risk and should be avoided during breastfeeding due to lack of human studies reporting outcomes of small molecules during lactation.64
Besides UPA, another selective JAK1 inhibitor is under evaluation for the treatment of UC. Filgotinib is a JAK1 inhibitor that proved to be effective and safe for the management of UC patients.65 However, the use of high-dose filgotinib in animal models has been associated with potential testicular toxicity raising doubts about its safety profile. A study is ongoing in UC to evaluate testicular safety and to resolve any concerns (NCT03201445).66 Further studies will be needed to compare UPA and filgotinib and to define whether one drug is superior to the other.
A recent systematic review and network meta-analysis including 29 phase 3 RCTs (4 head to head RCTs) compared the efficacy and safety of biologics and small molecules (infliximab, adalimumab, golimumab, vedolizumab, tofacitinib, ustekinumab, ozanimod, filgotinib, etrolizumab, and upadacitinib) in moderate-to-severe UC.67 UPA was significantly superior to other treatments and ranked highest for the induction of clinical remission (SUCRA 0.996), followed by infliximab. UPA also ranked highest when considering AEs (SUCRA 0.843) but concerning SAEs, ozanimod (SUCRA 0.831) and placebo (0.784) ranked highest, followed by etrolizumab (0.766) and filgotinib.67 Likewise, another network meta-analysis including 28 RCTs compared biologics and small molecules (infliximab, adalimumab, golimumab, vedolizumab, etrolizumab, ustekinumab, tofacitinib, filgotinib, upadacitinib and ozanimod). UPA 45 mg QD ranked first in terms of clinical remission and clinical response at 6–14 weeks in anti-TNF exposed patients and in anti-TNF naïve patients (risk of failure to achieve clinical remission = 0.73; 95% CI 0.68 to 0.80, p value = 0.98).68 Of note, although UPA ranked last for total number of AEs, no significant difference in the rate of serious AEs was detected between UPA and placebo, and UPA was less likely to lead to drug-related withdrawal compared with the other drugs.68
Based on the available data, UPA is a safe and effective drug for the management of moderate to severe UC. However, only a limited proportion of UPA treated patients (19–33%) achieved the efficacy outcome, supporting the need for further and more effective therapeutic options. It remains to define when to choose UPA and how to position it into the therapeutic algorithm. It is plausible to use it both in the first and second line for the treatment of naïve or biologic treated patients, and also in case of further failure. Indirect studies show that UPA is associated with greater efficacy than the remaining available drugs, but this evidence is not sufficient to demonstrate its superiority and head-to-head studies are needed to confirm this hypothesis.
To date, the European Crohn’s and Colitis Organization (ECCO) recommends anti-TNFs, vedolizumab, ustekinumab, and tofacitinib for the induction and maintenance of UC patients who fail conventional therapies.2 Although there is no specific algorithm, anti-TNFs are generally the most commonly used drugs as first-line due to the existence of biosimilars and their low price which makes them cost-effective.69 However, there is a growing trend towards personalized medicine and the therapy is tailored according to the specific patient’s need (eg, need for clinical response in a short time or preference regarding the administration route) and the patient’s medical history (eg, personal cancer or thrombosis history, elderly age, pregnancy, or presence of extraintestinal manifestations).70 The efficacy of UPA in other immunomediated disease makes it a reliable option in patients with rheumatological manifestations.41,43,49,51 Furthermore, given its rapid effect, UPA could be a valid alternative when the disease is clinically active and our target is a rapid improvement.
Conclusions
UPA is a selective JAK1 inhibitor with rapid mechanism of action and oral route of administration. Results from phase 3 studies showed efficacy and safety of UPA in moderate-to-severe UC patients leading to its approval by the FDA. UPA can be used in both biologic-naive patients and patients who have already failed other therapies. Its efficacy in other immune-mediated diseases makes it an attractive option in individuals with extraintestinal manifestations.
Data Sharing Statement
No new data were created or analyzed in this study.
Acknowledgement
We thank FIRMAD for the support to this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
M Napolitano, F D’Amico and E Ragaini declare no conflict of interest. L Peyrin-Biroulet declares personal fees from Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Index Pharmaceuticals, Sandoz, Celgene, Biogen, Samsung Bioepis, Inotrem, Allergan, MSD, Roche, Arena, Gilead, Amgen, BMS, Vifor, Norgine, Mylan, Lilly, Fresenius Kabi, OSE Immunotherapeutics, Enthera, Theravance, Pandion Therapeutics, Gossamer Bio, Viatris, Thermo Fisher. Grants from AbbVie, MSD, Takeda, Fresenius Kabi. Stock options: CTMA. S Danese has served as a speaker, consultant, and advisory board member for Schering-Plough, AbbVie, Actelion, Alphawasserman, AstraZeneca, Cellerix, Cosmo Pharmaceuticals, Ferring, Genentech, Grunenthal, Johnson and Johnson, Millenium Takeda, MSD, Nikkiso Europe GmbH, Novo Nordisk, Nycomed, Pfizer, Pharmacosmos, UCB Pharma and Vifor. The authors report no other conflicts of interest in this work.
References
1. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel J-F. Ulcerative colitis. Lancet Lond Engl. 2017;389:1756–1770. doi:10.1016/S0140-6736(16)32126-2
2. Raine T, Bonovas S, Burisch J, et al. ECCO guidelines on therapeutics in ulcerative colitis: medical treatment. J Crohns Colitis. 2022;16:2–17. doi:10.1093/ecco-jcc/jjab178
3. Misselwitz B, Juillerat P, Sulz MC, et al. Emerging treatment options in inflammatory bowel disease: janus kinases, stem cells, and more. Digestion. 2020;101:69–82. doi:10.1159/000507782
4. Baker KF, Isaacs JD. Novel therapies for immune-mediated inflammatory diseases: what can we learn from their use in rheumatoid arthritis, spondyloarthritis, systemic lupus erythematosus, psoriasis, Crohn’s disease and ulcerative colitis? Ann Rheum Dis. 2018;77:175–187. doi:10.1136/annrheumdis-2017-211555
5. Olivera P, Danese S, Peyrin-Biroulet L. Next generation of small molecules in inflammatory bowel disease. Gut. 2017;66:199–209. doi:10.1136/gutjnl-2016-312912
6. FDA approves XELJANZ® XR (tofacitinib) extended-release tablets for the treatment of ulcerative colitis Pfizer. Available from: https://www.pfizer.com/news/press-release/press-release-detail/fda_approves_xeljanz_xr_tofacitinib_extended_release_tablets_for_the_treatment_of_ulcerative_colitis.
7. Xeljanz EMA. European medicines agency; 2018. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/xeljanz.
8. D’Amico F, Parigi TL, Fiorino G, Peyrin-Biroulet L, Danese S. Tofacitinib in the treatment of ulcerative colitis: efficacy and safety from clinical trials to real-world experience. Ther Adv Gastroenterol. 2019;12:175628481984863. doi:10.1177/1756284819848631
9. Danese S, Vermeire S, Zhou W, et al. OP24 efficacy and safety of upadacitinib induction therapy in patients with moderately to severely active ulcerative colitis: results from the phase 3 U-ACHIEVE study. J Crohns Colitis. 2021;15:S022–S024.
10. Danese S, Argollo M, Le Berre C, Peyrin-Biroulet L. JAK selectivity for inflammatory bowel disease treatment: does it clinically matter? Gut. 2019;68:1893–1899. doi:10.1136/gutjnl-2019-318448
11. Rogler G. Efficacy of JAK inhibitors in Crohn’s Disease. J Crohns Colitis. 2020;14:S746–S754. doi:10.1093/ecco-jcc/jjz186
12. Shukla T, Sands BE. Novel non-biologic targets for inflammatory bowel disease. Curr Gastroenterol Rep. 2019;21:22. doi:10.1007/s11894-019-0689-2
13. Banerjee S, Biehl A, Gadina M, Hasni S, Schwartz DM. JAK–STAT signaling as a target for inflammatory and autoimmune diseases: current and future prospects. Drugs. 2017;77:521–546. doi:10.1007/s40265-017-0701-9
14. Salas A, Hernandez-Rocha C, Duijvestein M, et al. JAK–STAT pathway targeting for the treatment of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2020;17:323–337. doi:10.1038/s41575-020-0273-0
15. Langrish CL, McKenzie BS, Wilson NJ, et al. IL-12 and IL-23: master regulators of innate and adaptive immunity. Immunol Rev. 2004;202:96–105. doi:10.1111/j.0105-2896.2004.00214.x
16. Gilardi D, Gabbiadini R, Allocca M, et al. PK, PD, and interactions: the new scenario with JAK inhibitors and S1P receptor modulators, two classes of small molecule drugs, in IBD. Expert Rev Gastroenterol Hepatol. 2020;14:797–806. doi:10.1080/17474124.2020.1785868
17. Rane SG, Reddy EP. Janus kinases: components of multiple signaling pathways. Oncogene. 2000;19:5662–5679. doi:10.1038/sj.onc.1203925
18. Choy EH. Clinical significance of Janus Kinase inhibitor selectivity. Rheumatology. 2019;58:953–962. doi:10.1093/rheumatology/key339
19. Pérez-Jeldres T, Tyler CJ, Boyer JD, et al. Targeting cytokine signaling and lymphocyte traffic via small molecules in inflammatory bowel disease: JAK inhibitors and S1PR agonists. Front Pharmacol. 2019;10:212. doi:10.3389/fphar.2019.00212
20. Mohamed M-EF, Camp HS, Jiang P, et al. Pharmacokinetics, safety and tolerability of ABT-494, a novel selective JAK 1 inhibitor, in healthy volunteers and subjects with rheumatoid arthritis. Clin Pharmacokinet. 2016;55:1547–1558. doi:10.1007/s40262-016-0419-y
21. Ibrahim M, Pangan A, Feng T, Mohamed ME. P556 The effect of multiple doses of upadacitinib 45 mg on the pharmacokinetics of cytochrome P450 substrates in healthy adult subjects. J Crohns Colitis. 2022;16:i501–i502. doi:10.1093/ecco-jcc/jjab232.682
22. FDA. Rinvoq [package insert]. Chicago, IL: AbbVie; 2019.
23. Sandborn WJ, Ghosh S, Panes J, et al. Efficacy of upadacitinib in a randomized trial of patients with active ulcerative colitis. Gastroenterology. 2020;158:2139–2149.e14. doi:10.1053/j.gastro.2020.02.030
24. Peyrin-Biroulet L, Siegel C, Tanida S, et al. P522 upadacitinib promotes histologic and endoscopic mucosal healing: results from the upadacitinib ulcerative colitis Phase 3 program. J Crohns Colitis. 2022;16:i477–i478. doi:10.1093/ecco-jcc/jjab232.649
25. Parkes G, Ungaro R, Danese S, et al. P521 Correlation of histological assessment of mucosal healing with long-term clinical and patient-reported outcomes in patients with moderately to severely active ulcerative colitis treated with upadacitinib: results from the Phase 3 U-ACHIEVE maintenance trial. J Crohns Colitis. 2022;16:i476–i477.
26. Verstockt B, Blink Polakow S, Mahi N, et al. OP30 Upadacitinib modulates inflammatory pathways in gut tissue in patients with Ulcerative Colitis: transcriptomic profiling from the Phase 2b study, U-ACHIEVE. J Crohns Colitis. 2022;16:i033–i034. doi:10.1093/ecco-jcc/jjab232.029
27. Panaccione R, Hebuterne X, Lindsay J. Efficacy and safety of upadacitinib maintenance therapy in patients with moderately to severely active ulcerative colitis: results from a randomized Phase 3 study. United Eur Gastroenterol Week Virt. 2021;4:54.
28. Vermeire S, Danese S, Zhou W, et al. DOP41 Efficacy and safety of extended induction treatment with upadacitinib 45 mg once daily followed by maintenance upadacitinib 15 or 30 mg once daily in patients with moderately to severely active Ulcerative Colitis. J Crohns Colitis. 2022;16:i090–i091. doi:10.1093/ecco-jcc/jjab232.080
29. Higgins P, Colombel JF, Reguiero M, et al. DOP39 effect of baseline disease characteristics on clinical outcomes in moderate-to-severe Ulcerative Colitis treated with upadacitinib: results from a Phase 3 trials programme. J Crohns Colitis. 2022;16:i088–i089. doi:10.1093/ecco-jcc/jjab232.078
30. Danese S, Tran J, D’Haens G, et al. OP08 The effects of maintenance therapy with upadacitinib on abdominal pain, bowel urgency, and fatigue in patients with moderately to severely active Ulcerative Colitis: phase 3 U-ACHIEVE maintenance results. J Crohns Colitis. 2022;16:i008–i010. doi:10.1093/ecco-jcc/jjab232.007
31. Raine T, Ishiguro Y, Rubin D, et al. DOP40 Impact of corticosteroid usage on efficacy and safety outcomes in patients receiving upadacitinib for Ulcerative Colitis. J Crohns Colitis. 2022;16:i089–i090. doi:10.1093/ecco-jcc/jjab232.079
32. Vermeire S, Tanida S, Hu R, et al. S856 Efficacy of upadacitinib induction therapy in patients with moderately to severely active ulcerative colitis by biologic inadequate responder status: results from two randomized Phase 3 studies. Am J Gastroenterol. 2021;116:S399–S400. doi:10.14309/01.ajg.0000776956.67877.43
33. Colombel JF, Cao Q, Ghosh S, et al. OP33 Effect of upadacitinib (UPA) treatment on extraintestinal manifestations (EIMs) in patients with moderate-to-severe Ulcerative Colitis (UC): results from the UPA Phase 3 programme. J Crohns Colitis. 2022;16:i036–i037. doi:10.1093/ecco-jcc/jjab232.032
34. Olivera PA, Lasa JS, Bonovas S, Danese S, Peyrin-Biroulet L. Safety of janus kinase inhibitors in patients with inflammatory bowel diseases or other immune-mediated diseases: a systematic review and meta-analysis. Gastroenterology. 2020;158:1554–1573.e12. doi:10.1053/j.gastro.2020.01.001
35. Colombel JF, Panaccione R, Nakase H, et al. P573 The safety profile of upadacitinib maintenance therapy in ulcerative colitis in the Phase 3 U-ACHIEVE study is consistent with that in approved indications. J Crohns Colitis. 2022;16:i514–i514. doi:10.1093/ecco-jcc/jjab232.699
36. Ponce-Bobadilla AV, Stodtmann S, Eckert D, et al. P341 Pharmacokinetics and exposure-response analyses of upadacitinib in patients with moderate to severe ulcerative colitis – analyses of induction and maintenance clinical trials. J Crohns Colitis. 2022;16:i355–i357. doi:10.1093/ecco-jcc/jjab232.468
37. Sandborn WJ, Feagan BG, Loftus EV, et al. Efficacy and safety of upadacitinib in a randomized trial of patients with Crohn’s Disease. Gastroenterology. 2020;158:2123–2138.e8. doi:10.1053/j.gastro.2020.01.047
38. Kerschbaumer A, Smolen JS, Nash P, et al. Points to consider for the treatment of immune-mediated inflammatory diseases with Janus kinase inhibitors: a systematic literature research. RMD Open. 2020;6:e001374. doi:10.1136/rmdopen-2020-001374
39. Smolen JS, Pangan AL, Emery P, et al. Upadacitinib as monotherapy in patients with active rheumatoid arthritis and inadequate response to methotrexate (SELECT-MONOTHERAPY): a randomised, placebo-controlled, double-blind phase 3 study. Lancet. 2019;393:2303–2311. doi:10.1016/S0140-6736(19)30419-2
40. Fleischmann R, Pangan AL, Song I-H, et al. Upadacitinib versus placebo or adalimumab in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a Phase III, double-blind, randomized controlled trial. Arthritis Rheumatol Hoboken NJ. 2019;71:1788–1800. doi:10.1002/art.41032
41. Genovese MC, Fleischmann R, Combe B, et al. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): a double-blind, randomised controlled phase 3 trial. Lancet. 2018;391:2513–2524. doi:10.1016/S0140-6736(18)31116-4
42. Burmester GR, Kremer JM, Van den Bosch F, et al. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391:2503–2512. doi:10.1016/S0140-6736(18)31115-2
43. Guttman-Yassky E, Thaçi D, Pangan AL, et al. Upadacitinib in adults with moderate to severe atopic dermatitis: 16-week results from a randomized, placebo-controlled trial. J Allergy Clin Immunol. 2020;145:877–884.
44. Reich K, Teixeira HD, de Bruin-Weller M, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2021;397:2169–2181. doi:10.1016/S0140-6736(21)00589-4
45. Guttman-Yassky E, Teixeira HD, Simpson EL, et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): results from two replicate double-blind, randomised controlled phase 3 trials. Lancet. 2021;397:2151–2168.
46. Blauvelt A, Teixeira HD, Simpson EL, et al. Efficacy and safety of upadacitinib vs dupilumab in adults with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2021;157:1047. doi:10.1001/jamadermatol.2021.3023
47. Katoh N, Ohya Y, Murota H, et al. A phase 3 randomized, multicenter, double-blind study to evaluate the safety of upadacitinib in combination with topical corticosteroids in adolescent and adult patients with moderate-to-severe atopic dermatitis in Japan (Rising Up): an interim 24-week analysis. JAAD Int. 2022;6:27–36. doi:10.1016/j.jdin.2021.11.001
48. European commission approves AbbVie’s RINVOQTM (Upadacitinib) for the treatment of psoriatic arthritis and ankylosing spondylitis. AbbVie News Center. Available from: https://news.abbvie.com/alert-topics/immunology/european-commission-approves-abbvies-rinvoq-upadacitinib-for-treatment-psoriatic-arthritis-and-ankylosing-spondylitis.htm.
49. Mease PJ, Lertratanakul A, Anderson JK, et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis. 2021;80:312–320. doi:10.1136/annrheumdis-2020-218870
50. McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384:1227–1239.
51. van der Heijde D, Song I-H, Pangan AL, et al. Efficacy and safety of upadacitinib in patients with active ankylosing spondylitis (SELECT-AXIS 1): a multicentre, randomised, double-blind, placebo-controlled, phase 2/3 trial. Lancet. 2019;394:2108–2117. doi:10.1016/S0140-6736(19)32534-6
52. RINVOQ® (upadacitinib) receives FDA approval for the treatment of adults with moderately to severely active ulcerative colitis. AbbVie News Center. Available from: https://news.abbvie.com/news/press-releases/rinvoq-upadacitinib-receives-fda-approval-for-treatment-adults-with-moderately-to-severely-active-ulcerative-colitis.htm.
53. Vermeire S, Colombel JF, Takeuchi K, et al. DOP38 upadacitinib therapy reduces ulcerative colitis symptoms as early as day 1. J Crohns Colitis. 2022;16:i087–i088. doi:10.1093/ecco-jcc/jjab232.077
54. Panés J, Loftus EVJ, Higgins P, et al. P370 Maintenance of health-related quality of life improvements with upadacitinib treatment among patients with moderately to severely active ulcerative colitis: results from, 52-week phase, 3 study U ACHIEVE maintenance. J Crohns Colitis. 2022;16:i373–i374. doi:10.1093/ecco-jcc/jjab232.497
55. Ghosh S, Sanchez Gonzalez Y, Zhou W, et al. Upadacitinib treatment improves symptoms of bowel urgency and abdominal pain, and correlates with quality of life improvements in patients with moderate to severe ulcerative colitis. J Crohns Colitis. 2021;15:2022–2030. doi:10.1093/ecco-jcc/jjab099
56. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386:316–326. doi:10.1056/NEJMoa2109927
57. Sandborn WJ, Lawendy N, Danese S, et al. Safety and efficacy of tofacitinib for treatment of ulcerative colitis: final analysis of OCTAVE open, an open‐label, long‐term extension study with up to 7.0 years of treatment. Aliment Pharmacol Ther. 2022;55:464–478. doi:10.1111/apt.16712
58. Yates M, Mootoo A, Adas M, et al. Venous thromboembolism risk with JAK inhibitors: a meta‐analysis. Arthritis Rheumatol. 2021;73:779–788. doi:10.1002/art.41580
59. Wang F, Sun L, Wang S, et al. Efficacy and safety of tofacitinib, baricitinib, and upadacitinib for rheumatoid arthritis: a systematic review and meta-analysis. Mayo Clin Proc. 2020;95:1404–1419. doi:10.1016/j.mayocp.2020.01.039
60. Guillo L, Rabaud C, Choy EH, et al. Herpes zoster and vaccination strategies in inflammatory bowel diseases: a practical guide. Clin Gastroenterol Hepatol. 2022;20:481–490. doi:10.1016/j.cgh.2020.10.027
61. Merck & Co., Inc. Zostavax [package insert]. U.S. Food and Drug Administration; 2019. Available from: https://www.fda.gov/media/119879/download.
62. GlaxoSmithKline. SHINGRIX. [package insert]. U.S. Food and Drug Administration; 2021. Available from: https://www.fda.gov/media/108597/download.
63. Kucharzik T, Ellul P, Greuter T, et al. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis. 2021;15:879–913. doi:10.1093/ecco-jcc/jjab052
64. Gisbert JP, Chaparro M. Safety of new biologics (Vedolizumab and Ustekinumab) and small molecules (Tofacitinib) during pregnancy: a review. Drugs. 2020;80:1085–1100. doi:10.1007/s40265-020-01346-4
65. Feagan BG, Danese S, Loftus EV, et al. Filgotinib as induction and maintenance therapy for ulcerative colitis (SELECTION): a phase 2b/3 double-blind, randomised, placebo-controlled trial. Lancet. 2021;397:2372–2384. doi:10.1016/S0140-6736(21)00666-8
66. D’Amico F, Magro F, Peyrin-Biroulet L, Danese S. Positioning filgotinib in the treatment algorithm of moderate to severe ulcerative colitis. J Crohns Colitis. 2021;jjab206. doi:10.1093/ecco-jcc/jjab206
67. Lasa JS, Olivera PA, Danese S, Peyrin-Biroulet L. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2022;7:161–170. doi:10.1016/S2468-1253(21)00377-0
68. Burr NE, Gracie DJ, Black CJ, Ford AC. Efficacy of biological therapies and small molecules in moderate to severe ulcerative colitis: systematic review and network meta-analysis. Gut. 2021;
69. Danese S, Gomollon F. ECCO position statement: the use of biosimilar medicines in the treatment of inflammatory bowel disease (IBD). J Crohns Colitis. 2013;7:586–589. doi:10.1016/j.crohns.2013.03.011
70. D’Amico F, Fiorino G, Furfaro F, et al. Patient’s profiling for therapeutic management of inflammatory bowel disease: a tailored approach. Expert Rev Gastroenterol Hepatol. 2020;14:765–773. doi:10.1080/17474124.2020.1772057
71. Genovese MC, Smolen JS, Weinblatt ME, et al. Efficacy and safety of ABT-494, a selective JAK-1 inhibitor, in a Phase IIb study in patients with rheumatoid arthritis and an inadequate response to methotrexate: ABT-494 In patients with rheumatoid arthritis and inadequate response to methotrexate. Arthritis Rheumatol. 2016;68:2857–2866. doi:10.1002/art.39808
72. Kremer JM, Emery P, Camp HS, et al. A Phase IIb study of ABT-494, a selective JAK-1 inhibitor, in patients with rheumatoid arthritis and an inadequate response to anti-tumor necrosis factor therapy: ABT-494 In patients with ra and inadequate response to anti-tnf therapy. Arthritis Rheumatol. 2016;68:2867–2877. doi:10.1002/art.39801
73. Fleischmann RM, Genovese MC, Enejosa JV, et al. Safety and effectiveness of upadacitinib or Adalimumab plus methotrexate in patients with rheumatoid arthritis over 48 weeks with switch to alternate therapy in patients with insufficient response. Ann Rheum Dis. 2019;78:1454–1462. doi:10.1136/annrheumdis-2019-215764
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.