")
Back to Journals » Clinical Interventions in Aging » Volume 19
Evaluation of a Fall Prevention Program to Reduce Fall Risk and Fear of Falling Among Community-Dwelling Older Adults and Adults with Disabilities
Authors Hawkins M , Goldhammer T, McClave R, Jenkins-Smith E
Received 2 December 2023
Accepted for publication 27 February 2024
Published 6 March 2024 Volume 2024:19 Pages 375—383
DOI https://doi.org/10.2147/CIA.S448196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Melissa Hawkins,1 Tori Goldhammer,2 Robin McClave,1 Edwinta Jenkins-Smith3
1Department of Health Studies, American University, Washington, DC, USA; 2Safe at Home Program, Home Care Partners, Washington, DC, USA; 3Department of Aging and Community Living, District of Columbia Department of Health, Washington, DC, USA
Correspondence: Melissa Hawkins, Department of Health Studies, American University, McCabe Hall Room 222, 4400 Massachusetts Avenue NW, Washington, DC, 20016, USA, Tel +1 202-885-6252, Email [email protected]
Purpose: The overarching goal of the program evaluation was to determine the reach and impact of the District-funded Safe At Home (SAH) modification program in reducing falls, fall injuries, and fear of falls among community-dwelling older adults and adults with disabilities. The SAH program has served over 6000 adults since 2016, the majority of whom are women (79%) and over age 60 (92%).
Materials and Methods: Letters were mailed in September 2022 to clients (n=492) who had home modifications completed between October 2021-March 2022 inviting them to participate in a brief phone survey about program satisfaction, falls, fall location, and severity. The validated Fall Efficacy Scale (FES) was administered pre (at first visit), post (at last visit), and during the phone survey (within 6 months to 1 year of program completion) to assess fear of falling. The response rate was 55% (n=241).
Results: Older adults (n=219) and adults with disabilities (n=22) reported high program satisfaction. Most clients, 79%, did not report a fall since the completion of the home modifications. The majority of falls reported, 76%, occurred inside the home. The average evaluation FES score was 32.5 (SD=22.6, range 10– 100), indicating relatively low fear of falling. Higher FES scores were associated with a greater likelihood of reporting a fall (r=0.44, p < 0.001, n=51) and older age (r = 0.17, p < 0.01). FES scores were not related to gender. Evaluation FES scores were significantly lower than the pre-FES scores, indicating a reduction in fear of falling and positive impact of the home modifications (T(107) = 5.14, p < 0.001).
Conclusion: The client-centered SAH program demonstrates significant reductions in falls, fear of falling, and high satisfaction among clients. Recommendations include program expansion to offer other evidence-based components to reduce falls and support safe aging in place.
Keywords: program evaluation, home modification, fall efficacy scale, FES, injury, prevention, independent living
Introduction
Falls impact the health and independence of older adults (aged 60+ years). Older adults are the fastest growing demographic in the United States (US).1 The number of older adults is estimated to double to over 14 million individuals in 2040.2 Older adults are at risk for falls and fall-related injuries. Millions of older adults fall each year in the US and this number is increasing. A 2023 Centers for Disease Control and Prevention (CDC) report determined that on average 100 older adults die from falls every day.3 Unintentional falls are the leading cause of injury and of deaths from injury among older adults.
Most falls occur in the home. Further, individuals who fall are more likely to fall again.4 There are both demographic and geographic variations in the distribution of falls. Women report falls and fall-related injuries more frequently than men; however, men have higher rates of fatal falls compared to women.3 Further, fall injury incidence trends are likely underreported as self-reported survey data significantly undercount fall injuries.5 Falls also have financial implications to individuals, their caregivers/families, and the health-care system. In addition to being the leading cause of death from unintentional injury among older adults, falls are the leading causes for emergency department visits for unintentional injuries. A recent 2023 study among over 900,000 patients across two large northeast metropolitan hospital systems between 2013 and 2019 found that average cost of a fall was $62 521.6
Even falls that are not severe may result in significant health impacts, including fear of falling, social isolation, and declines in mobility.7 Adults who have fallen may have fears about falling again which may be associated with reduced activities, which increases frailty and increased risk for a future fall. Further, there is a need to support older adults, given that loneliness and social isolation also negatively impact physical health.8
Trends in fall incidence and the health ramifications of a fall underscore the importance of investment in prevention and funding for fall prevention programs. Risk of falling does increase with age. However, falls are preventable by decreasing modifiable risk factors, raising awareness about fall prevention, promoting preventive behaviors, and improving screening and referrals for those at fall risk.9 Fall prevention efforts are an important part of older adult education and health. Recent research suggests that many falls can be prevented through a variety of comprehensive evidence-based interventions.10
Over the past two decades, the CDC has maintained a compendium of falls prevention interventions11 that have demonstrated, in randomized controlled trials, to reduce falls and fall risk among older adults. There are currently nine federal programs designed to prevent falls for older adults or adults with disabilities by providing evidence-based falls prevention (eg, exercise classes), home assessments (eg, home safety checklist), or home modifications (eg, railings or ramps). Some interventions address multiple fall risk factors, such as removing or reducing potential fall hazards in the home environment; others address individual fall risk factors, such as exercise programs to improve balance. Both impact and outcome studies of home assessment and home modification program studies suggest significant positive health outcomes for older adult participants. The US Department of Housing and Urban Development (HUD) is currently conducting an evaluation of the Older Adults Home Modification Program to examine program’s impact on emergency room visits and ability to age in place. This study will be completed in 2026.
The University of Southern California’s Fall Prevention Center of Excellence has facilitated coordination among federal, state, and local stakeholders to advance home modification programs, in homes and community-based programs, as a key policy and program priority for aging in place. Their Home Modification Information Network, developed with support from the Administration for Community Living (ACL), is a searchable database (https://homemods.org/acl/hmin/) that provides an inventory of home modification policies, funding sources, resources for older adults, and home modification programs available by state.
Key evaluation questions included: Who is most likely to complete the SAH program? What was clients’ overall satisfaction with the SAH program? Are home modifications associated with decreased fall risk and/or reduced fear of falling?
Materials and Methods
In 2016, the innovative Safe at Home (SAH) fall prevention program was established with the Department of Aging and Community Living (DACL) and administered by Home Care Partners, to offer comprehensive services to the underrepresented aging population in Washington, DC (DC) and adults with disabilities. SAH promotes aging-in-place by providing in-home accessibility adaptations (eg, grab bars, safety railings, stair lifts, and bathtub cutouts) to reduce the risk of falls and reduce barriers that limit mobility. The program is based on the rationale that environmental factors play a large role in falls and population-targeted risk mitigation is cost effective and beneficial.
SAH incorporates one access point for referrals and screening. Adults are referred to the program by contacting the DACL Intake/Referral and Assistance line and completing a falls risk assessment. Home Care Partners, senior wellness centers, community-based organizations, and/or health-care providers can also refer clients to SAH. SAH is also a close partner of DACL’s Community Transition Program, specifically working with DC residents who are transitioning back to the community from long-term care settings through the Money Follows the Person program. A key component of SAH is the integration of occupational therapy practitioners, with training and certification in home modification practices, who are uniquely qualified to provide comprehensive client evaluations and to develop client-centered home modification recommendations that acknowledge the multifactorial nature of falls.12 SAH has served more than 6000 residents installing safety adaptions since 2016.
Demographic Profile
Several key demographic trends in DC are relevant to priorities for expansion of services and partnerships to prevent falls among older adults and adults with disabilities. DC has a total population of ~685,000 residents, among which 113,644 (16.5% of total population) are older adults.13 Approximately, 1 in every 9 residents is an older adult. Similar to national trends, this is the largest growing segment of the DC population. Most DC older adults are female (59.3%), Black (62.5%), unmarried (58.6%), live alone (74.1%), or are homeowners (65.5%).14 In DC, one in four older adults experience a fall each year. The rate of falls among older adults is 29% and the death rate from falls per 100,000 people is 70, which is comparable to the US national average.15 However, the rate of reported falls and fall-related injuries and deaths varies significantly across underserved demographic segments.
SAH Eligibility Criteria
Adults 60 or older or adults 18 or older with disabilities who have an income of up to 100% of the Area Median Income (maximum of $72,550 annually for an individual or $82,550 for a married couple) are eligible to participate in SAH. Adults with disabilities are required to submit a form signed by their physician affirming their disability impacts mobility in their home or submit proof of state disability insurance (SDI) benefits. SAH provides up to $6000 of preventative modifications for clients to reduce fall risk. Beginning in Fiscal Year 2024, the home modification maximum will be raised to $7000.
SAH eligibility criteria also include assessment of fear of falling and falls risk, determined at intake over the phone using the Vulnerability of Elders Survey (VES-13). SAH uses evidence-based assessments to quantify fall risk and modification recommendations. Given the multifactorial risk of falling, SAH uses a variety of standardized assessments and a minimum of three assessments on each client. The assessments include 1) Safety Assessment of Function and The Environment for Rehabilitation in home version (SAFER HOME) assessment completed pre and post to determine the number of safety hazards; 2) Falls Efficacy Scale (FES) completed pre and post to determines the level of fear of falling; and 3) Falls Risk of Older People in the Community (FROP-Com) is a multifactorial fall risk assessment measures cognition, medication, and history of falls. Demographic information including client age, race/ethnicity, gender, and type of housing is also collected.
Evaluation Data Collection Procedures
All clients who completed the SAH program between October 1, 2021, and March 31, 2022 (n=492) were sent a letter in August 2022 inviting them to participate in a brief phone evaluation survey. Phone surveys were completed in September 2022 between the 9am-8pm Monday-Saturday. Verbal informed consent was provided before the administration of survey items. The research assistants administered the 10-question phone survey in Qualtrics, an online survey software program.
Three research assistants were trained to administer the survey to collect data, clean and recode data, and conduct descriptive data analyses. During the training, the research assistants reviewed the phone survey script, practiced asking questions/probes slowly and clearly, and role-played interviewing techniques. Emphasis was placed on effectively developing rapport and answering clarifying questions regarding the purpose of the survey.
American University Institutional Review Board (IRB) approval was granted (#2023-106) on September 9, 2022. The research team implemented several precautions to ensure the privacy, confidentiality, and protection of information provided by all clients, as well as a high evaluation survey participation rate. This study complies with ethical and scientific standards that protect the rights of participants as detailed in the Declaration of Helsinki. Data were de-identified during data analysis and contain unique client IDs. Verbal informed consent was provided by respondents before the phone survey questions were administered. Data were collected via phone, recorded in Qualtrics using a secure link, and stored on computers encrypted with a password.
Measures and Survey Pre-Testing
Best practices for survey design were followed for the development, pre-testing, and administration of the evaluation phone survey. This included clarity and brevity of questions to reduce respondent burden, specificity in questions and response options, and a mix of open and close-ended questions with “don’t know” options included. The survey was pre-tested with a small representative sample of older adults prior to administration (n=25, mean age=73 years). The survey was revised with minor revisions to improve clarity including information for food or other health services provided by DACL, if requested, and adding a response option for the survey to be completed by a “support person/caretaker”.
The 10-item post-program survey included a brief introduction describing the SAH program and purpose of the phone survey, informed consent to participate, program satisfaction (2 questions), feedback on SAH (2 questions), fall history since SAH modifications completed including location and severity (5 questions), and fear of falling (Fall Efficacy Scale).16 Fall severity was defined as follows: not severe; able to get up easily; somewhat severe; needed assistance from family/friend/neighbor etc; severe, went to doctor/health care provider for medical attention. The respondent also had the opportunity to provide open-ended feedback about the SAH program in closing.
The FES asks respondents to rate how confident they are in doing 10 daily activities without falling on a scale of 1 to 10, with 1 being very confident and 10 not confident at all. The 10 activities include taking a bath or shower, getting in and out of bed, getting dressed and undressed, and walking around the house and stairs. The FES is administered three times: 1) at the first program visit before home modifications, by the occupational therapist; 2) at the last program visit after home modifications, by the occupational therapist, and 3) over the phone by the research evaluation team, within 6–12 months of program completion. Ratings for the items are summed to give an overall score ranging from 10 to 100. Lower scores indicate greater confidence in not falling. Scores of above 70 are indicative of low confidence during everyday activities. The FES has strong psychometric properties with a test–retest reliability of 0.96 in an older adult population and an internal reliability of 0.96.17,18
Analysis
SPSS Version 29 (IBM Corp, Armonk, NY, USA) and R Core Team’s (2021) tidyverse package (R Foundation for Statistical Computing, Vienna, Austria) were utilized for data cleaning, recoding, and statistical analysis. Statistical analyses were performed with the alpha level of significance at p < 0.05 and 95% confidence intervals calculated for all effect estimates.
The data analyses were performed sequentially. Age was examined as both a continuous variable (age in years) and a dichotomous variable (below 60 and 60+ year). FES scores were also examined as a continuous variable (overall score) and a dichotomous variable (below 70 and 70+). Demographic characteristics (age, gender, ward, and race/ethnicity) were summarized. The representativeness of the post-program phone survey sample and the sample of adults with disabilities was compared with the overall number of SAH clients served using chi-square tests of independence for categorical variables. Descriptive statistics (means, standard deviations, counts, and frequencies) and distributions are obtained for all survey items to summarize measures, including fall history, severity, and fear of falling. Bivariate analysis was conducted to examine associations and relationships between pre- and post-program changes in falls and fear of falling, and demographic characteristics. Fall rate and FES scores change over time were calculated to examine baseline-post-evaluation assessment differences. Mean scores for each item, as well as summary scores, were compared using paired t-tests for all assessments. The two groups (adults 60 years and older and adults 18 years and older with disabilities) were analyzed separately, when the sample size was sufficient, given that individuals with disabilities may have characteristics related to falls and fear of falling that are distinct from the older age group. Determination of the impact and reach of the SAH program was determined by examining between-group differences for each outcome (falls and FES) and was evaluated using regression for repeated measures, which are robust to missing data because they allow subjects with differing numbers of repeated measures to remain in the analysis.
Results
Of the 492 clients invited to participate, 241 completed the phone survey (n=219 were older adults and n=22 were adults with disabilities). The response rate was 54.9%. The time to complete the post-program survey averaged 11.6 min (mean)/9.0 min (median) (SD=6.7 min, range 4.9 min to 24.4 min).
Demographic Characteristics
Demographic characteristics of evaluation respondents and SAH clients were similar, indicating that the survey sample is representative of the larger SAH population (Table 1). The majority of SAH clients are women (79%) and over age 60 (92%). The mean age is 75 years. Among the SAH population, 90% live alone, 97% identify as Black/African-American, and 72% are homeowners. In the survey sample, the majority of the adults with disabilities (n=22) are women (64%) and the mean age is 51 (range 29–60). The average time for SAH program completion, from intake to the completion of home modifications, is 5–6 weeks. Overall, standard grab bars (18 inch), custom grab bars such as toilet roll holders or towel racks, and power lift recliners were the most common modifications provided.
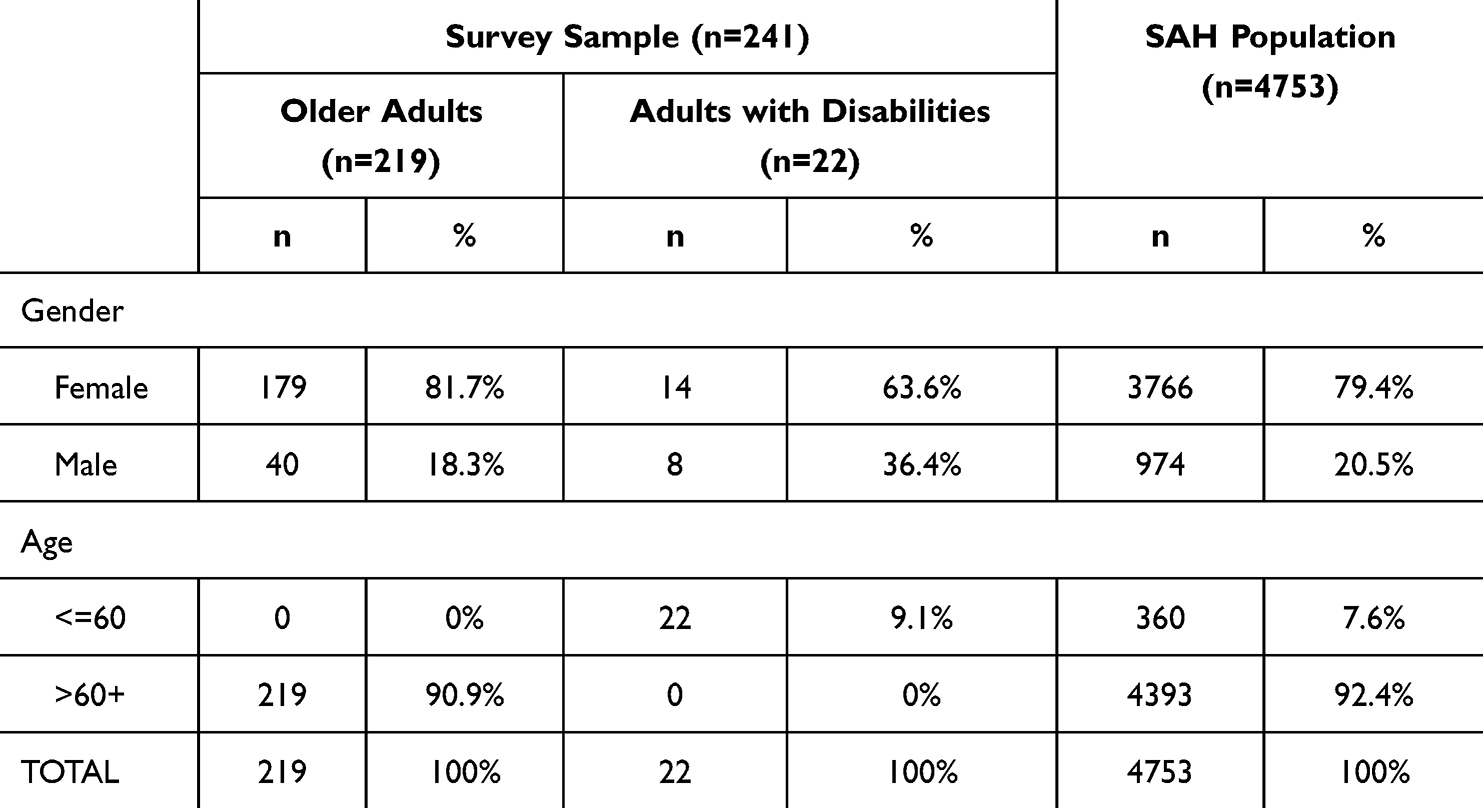 |
Table 1 Demographic Characteristics of Survey Sample and SAH Population |
Cost
In 2022, the average cost per client (occupational therapists and contractors) was $4100. There is a significant, positive correlation between average total cost per client and pre-program FES score (r = 0.15, p < 0.01). Neither residence location nor age is correlated to average amount spent.
Program Satisfaction
The overall satisfaction with the SAH program is high across all demographic characteristics. Approximately, 90% (n=197) of older adults and 86% (n=19) of adults with disabilities reported that they were “completely satisfied.” The specific program components were also rated highly. The majority of respondents, over 80%, indicated they were “completely satisfied” with the specific program components (Table 2). Respondents were asked an open-ended question about the home modifications they found to be most helpful. The five most helpful modifications respondents noted were as follows: handrails, chair lift, grab bars in bathroom, shower chair, and toilet seat.
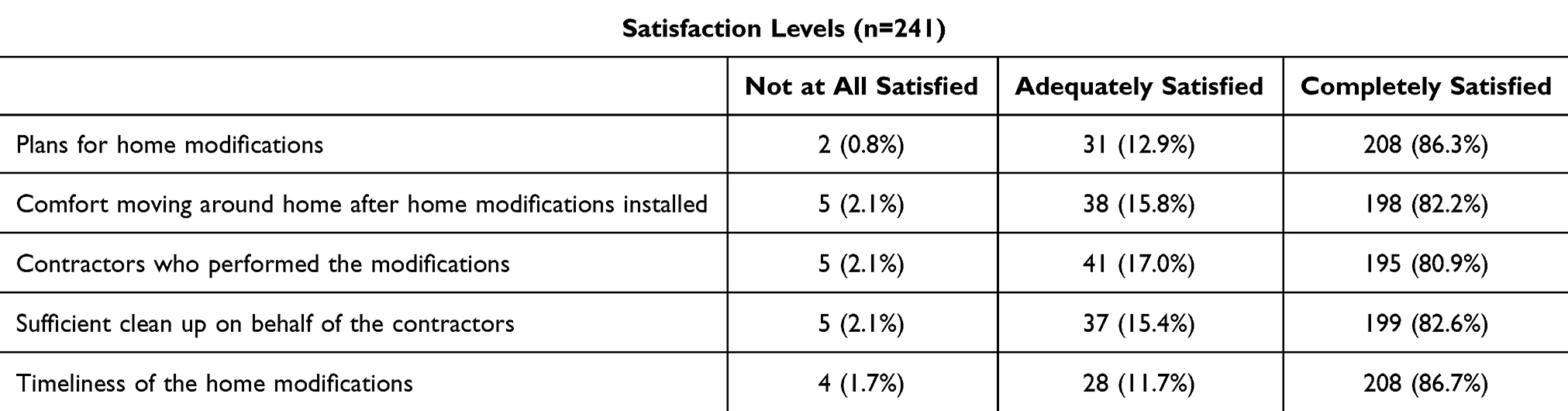 |
Table 2 Satisfaction with the Specific Components of the SAH Program (n=241) |
Falls
The majority of older adults, 80.3% (n=176) stated that they had not fallen since the SAH program home modifications were completed; among adults with disabilities, 63.6% (n=14) did not report a fall. Of the 43 older adults and 8 adults with disabilities who reported a fall, most reported having one fall (54.9%, n=28) since the completion of the program (range 1–6 falls). Seventy-five percent of the falls occurred inside the home; among adults with disabilities who reported a fall, 62.5% (n=5) were inside the home. Falls occurring inside the home averaged 2.53 (SD = 2.5) per person per year in the previous 12 months at intake; at the follow-up evaluation survey, the average rate of falls inside the home per person per year had dropped significantly to 1.5 (SD = 0.74) (z = 5.35, p < 0.01). For falls reported inside the home, the respondent was asked about fall location and severity of each fall. Those who reported an inside fall near a modification are also more likely to report having more than one fall. Approximately 50% of falls were self-reported as somewhat severe, 30% not severe, and 20% of falls were severe. Further, those respondents who experienced a severe fall were two times more likely to also report having more than one fall.
Fear of Falling (FES)
Average pre-FES scores were 36.9 (SD = 21.3, range 10–100), indicating some fear of falling during daily activities. Pre-FES scores were higher among adults with disabilities, with average scores of 45 (SD = 24.6, range 13–85). FES scores significantly decreased (indicating more confidence in not falling) for both older adults, mean 20.5 (SD = 15.4, range 10–88), and adults with disabilities, mean 21 (SD = 13.5, range 10–37) at post assessment. FES scores remained significantly lower than pre-SAH modifications at the phone evaluation assessment for older adults (M = 27.3, SD = 16.4, T(107) = 5.14, p < 0.001). The median evaluation FES score was 26 and mean was 32.5 (SD = 22.6, range 10–100). Two adults with disabilities did not complete the FES questions because they were not mobile (both were wheelchair bound). Less than 10% of respondents (n=20) had FES scores > 70, indicating high fear of falling.
Evaluation FES scores were significantly associated with age and falls. There was a positive correlation between older age and higher FES scores (r = 0.17, p < 0.01). Higher FES scores were also associated with a greater number of falls reported (r = 0.44, p < 0.001, n=51). The mean FES score among those who reported a fall (n=51) was 42.4 (SD = 22.6) which was significantly higher than the mean FES score of 29.8 (SD = 21.9) among those who did not report a fall (n=188) (p < 0.001, t=3.6, df=237). Among those who reported a fall, those who experienced two or more falls (n=23) also had a higher FES score (M = 54.1, SD = 23.3) compared to those who reported 1 fall (M = 32.8, SD = 17.1) (p < 0.001, t=3.8, df=49). This indicates that those who fell more often also report a greater fear of falling compared to those who fell 1 time. Evaluation FES scores were not related to gender, neighborhood of residence (Wards), number of inside falls experienced, or fall severity (if a fall was reported).
Discussion
Falls pose a significant risk to the health, well-being, and autonomy of older adults. Evidence-based fall prevention programs, including those with a home modification component,19,20 have consistently demonstrated effectiveness in reducing fall risk among older adults.21–23 However, most evaluations of fall prevention programs have been implemented in a clinical setting.24–26 To our knowledge, this evaluation is among the first of a fall prevention program focused on home modifications in a community-dwelling older adult population. The SAH program is a part of a strategic plan to make DC more age friendly. SAH aims to prevent falls and fall injuries and reduce fear of falling to improve health outcomes for older adults and adults with disabilities in a community setting. Its delivery in a structured, time-bound, health professional supported format provides consistently strong outcomes and results for the majority of participants.
Currently, the majority of SAH clients are women (~80%) and older adults (90%). Recent studies have demonstrated gender differences in older adults’ perceptions of falls, fall risk, and fall prevention.27,28 A targeted approach to understand the factors influencing engagement in fall prevention behaviors, and how they may differ by gender, age, and race, is important in implementing equitable programs and interventions that serve priority populations. Research suggests that home modification programs may reduce falls and improve health outcomes for older adults, although research is limited for adults of varying ages, including those with disabilities who may be at higher risk of falling. This is due, in part, to the focus of national falls data analyses on older adults. A recent 2021 VA-sponsored outcome study found veterans with disabilities who received home modifications based on health-care providers’ recommendations reported a significant reduction in hospitalization after 1 year.29 Although veterans of any age were eligible to participate in the program, the average age was 73. Future research is necessary to expand analysis of falls data to better understand populations at risk of falls and to inform fall prevention programs.
The SAH program appears to be cost-effective, with an average investment of $4100 per client to provide home modifications and adaptations to support safe aging in place. A recent analysis determined the average cost of average cost of a hospital visit for a fall was $62,521.6 This return on investment is critical in keeping older adults safe, active, and independent.
We found a low likelihood of falls after home modifications (21%) and low severity among those who reported a fall/s. Twenty-one percent of respondents reported a fall after participating in the SAH program, which is lower than both the US and the DC average reported by the CDC.30 Seventy-five percent of the reported falls occurred inside the home, which is consistent with national and local data. Higher FES scores were associated with a greater likelihood of reporting a fall (either inside the home or outside of the home), which is also consistent with the literature and previous findings.17
Based on these positive preliminary findings, the SAH program is being expanded to offer multiple components that contribute to fall risks as identified by the CDC including medication review, vision screenings, and evidence-based fall prevention classes. Evidence-based activity classes will be offered virtually and in-person at senior wellness centers, accommodating a variety of abilities. Multiple component interventions that include exercise programs are most effective in reducing falls and fall risk compared to programs that do not include an exercise component.20,21
Limitations
There are several limitations to note. Survey data on number of falls, fall location, and fall severity were self-reported by the clients and thus subject to recall bias. Respondents may have provided responses they think are expected, which may contribute to response bias. The study design is observational and does not include a comparison group. The FES items may have caused some confusion as the respondents are asked to give a lower number for higher confidence; the RAs attempted to reduce errors by reading each statement carefully and slowly, repeating as necessary. Program data did not allow for analysis of average cost per client by number of modifications; therefore, it was not possible to examine the relationship between number of modifications and changes in fall risk after program participation. Other important factors that may impact both falls and fall risk were not reported in these data, including Activities of Daily Living (ADL) and the relationship with hours of Personal Care Assistance (PCA) services.
The SAH clients include both older adults (n=219) and adults with disabilities (n=22) who may have characteristics related to falls and fear of falling that are distinct. There were no differences between the groups in demographic characteristics, but number of adults with disabilities was too small to stratify by other factors.
Conclusion
The client-centered SAH program demonstrates significant reductions in falls, fear of falling, and high satisfaction among participants. The SAH program may serve as a model intervention for other communities to support older adults to age in place safely. Further, the high overall satisfaction and significant reductions in fall risk experienced by residents who complete the SAH program offers an opportunity to address other priority health needs of older adults through similar outreach methods.
Acknowledgments
Thanks to the Safe at Home program participants for their time and willingness to complete the phone survey to support this evaluation. We also thank Louise Benning, Lily Duboff, Janvier Richardson, and Samuel Siktar for their many valuable contributions with data collection and analysis support. We express our gratitude to the DACL and Home Care Partners program staff for their support, especially Kathy Gessner, Melanie Johnson, Jessica Smith, Rinaldo Washington, and Elexa Waugh. Thank you to Anastasia Snelling for providing leadership, guidance, and support on all aspects of this project.
Funding
This work was supported by the District of Columbia Department of Aging and Community Living (DACL) (American University, ID 37313).
Disclosure
The authors report no conflicts of interest in this work.
References
1. U.S. Department of Health and Human Services, Administration for Community Living (May 2022); Profile of Older Americans; 2021.
2. U.S. Census Bureau. National Population Projections Tables: Main Series. 2023. https://www.census.gov/data/tables/2023/demo/popproj/2023-summary-tables.html
3. Kakara R, Bergen G, Burns E, Stevens M. Nonfatal and fatal falls among adults aged >65 years- United States, 2020–2021. MMWR. 2023;72:938–943. doi:10.15585/mmwr.mm7235a1
4. Special Committee on Aging, United States Senate. Fall prevention: national, state, and local solutions to better support seniors; 2019. Availabnle from: https://www.aging.senate.gov/imo/media/doc/SCA_Falls_Report_2019.pdf.
5. Hoffman GJ, Ha J, Alexander NB, Langa KM, Tinetti M, Min LC. Underreporting of fall injuries of older adults: implications for wellness visit fall risk screening. J Am Geriatr Soc. 2018;66(6):1195–1200. doi:10.1111/jgs.15360
6. Dykes PC, Curtin-Bowen M, Lipsitz S, et al. Cost of inpatient falls and cost-benefit analysis of implementation of an evidence-based fall prevention program. JAMA Health Forum. 2023;4(1):e225125. doi:10.1001/jamahealthforum.2022.5125
7. Boyd R, Stevens JA. Falls and fear of falling: burden, beliefs and behaviours. Age Ageing. 2009;38(4):423–428. doi:10.1093/ageing/afp053
8. Holt-Lunstad J. The potential public health relevance of social isolation and loneliness: prevalence, epidemiology, and risk factors. Public Policy Aging Rep. 2017;27(4):127–130. doi:10.1093/ppar/prx030
9. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas. 2013;75:51–61. doi:10.1016/j.maturitas.2013.02.009
10. United States Government Accountability Office. Older adults and adults with disabilities: federal programs provide support for preventing falls, but program reach is limited. GAO-22-105276; 2022. Availabnle from: https://www.gao.gov/assets/gao-22-105276.pdf.
11. Stevens JA, Burns E. A CDC Compendium of Effective Fall Interventions: What Works for Community-Dwelling Older Adults.
12. American Occupational Therapy Association. Occupational therapy practice framework: domain and process (4th ed.). American. J Occup Ther. 2020;74(Suppl. 2). doi:10.5014/ajot.2020
13. DC Office on Aging (DACL). 2019–2022 District of Columbia state plan on aging. Availabnle from: https://dacl.dc.gov/sites/default/files/dc/sites/dacl/page_content/attachments/DACL%20State%20Plan%20on%20Aging_0.pdf.
14. DC Policy Center. A portrait of DC’s older adults; 2018. Availabnle from: https://www.dcpolicycenter.org/publications/a-portrait-of-d-c-s-older-adults/.
15. Office of the Budget Director, Council of the District of Columbia. The state of older adults in the District of Columbia; 2020. Availabnle from: https://static1.squarespace.com/static/5bbd09f3d74562c7f0e4bb10/t/5f91dbfcf4433c22bbc35756/1603394563391/The+State+of+Older+Adults+in+the+District+of+Columbia.pdf.
16. Tinetti M, Richman D, Powell L. Falls efficacy as a measure of fear of falling. J Gerontol. 1990;45(6):239. doi:10.1093/geronj/45.6.P239
17. Greenberg M, Jacoby J, Barraco RD, et al. Analysis of falls efficacy scale and vulnerable elders survey as predictors of falls. Cureus. 2021;13(4):e14471. doi:10.7759/cureus.14471
18. Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing. 2005;34(6):614–619. doi:10.1093/ageing/afi196
19. Chase CA, Mann K, Wasek S, Arbesman M. Systematic review of the effect of home modification and fall prevention programs on falls and the performance of community-dwelling older adults. Am J Occup Ther. 2012;66(3):284–291. doi:10.5014/ajot.2012.005017
20. Müller C, Lautenschläger S, Dörge C, Voigt-Radloff S. A feasibility study of a home-based lifestyle-integrated physical exercise training and home modification for community-living older people (Part 2): the FIT-at-Home fall prevention program. Disability Rehabil. 2021;43(10):1380–1390. doi:10.1080/09638288.2019.1700564
21. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7. doi:10.1002/14651858.CD012221.pub2
22. Stubbs B, Brefka S, Denkinger M. What works to prevent falls in community-dwelling older adults? An umbrella review of meta-analyses of randomized controlled trials. J Am Phys Ther Assoc. 2105;95:1095–1110. doi:10.2522/ptj.20140461
23. Tricco AC, Thomas SM, Veroniki AA, et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA. 2017;318:1687–1699. doi:10.1001/jama.2017.15006
24. Casey CM, Parker EM, Winkler G, Liu X, Lambert GH, Eckstrom E. Lessons learned from implementing CDC’s STEADI falls prevention algorithm in primary care. Gerontologist. 2017;57(4):787–796. doi:10.1093/geront/gnw074
25. Peel NM, Travers C, Bell RA, Smith K. Evaluation of a health service delivery intervention to promote falls prevention in older people across the care continuum. J Eval Clin Pract. 2010;16:1254–1261. doi:10.1111/j.1365-2753.2009.01307.x
26. Roigk P, Becker C, Schulz C, Konig HH, Rapp K. Long-term evaluation of the implementation of a large fall and fracture prevention program in long-term care facilities. BMC Geriatr. 2018;18:233. doi:10.1186/s12877-018-0924-y
27. Patton S, Vincenzo J, Lefler L. Gender differences in older adults’ perceptions of falls and fall prevention. Health Promot Pract. 2022;23(5):785–792. doi:10.1177/15248399211009783
28. Sandlund M, Skelton DA, Pohl P, Ahlgren C, Melander-Wikman A, Lundin-Olsson L. Gender perspectives on views and preferences of older people on exercise to prevent falls: a systematic mixed studies review. BMC Geriatr. 2017;17:58. doi:10.1186/s12877-017-0451-2
29. Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Hous Policy Debate. 2021;31(6):862–874. doi:10.1080/10511482.2020.1858923
30. Malani P, Kullgren J, Solway E, Hoffman G, Singer D, Kirch M. National poll on healthy aging physical functioning and falls during the COVID 19 pandemic; 2021. Available from: https://deepblue.lib.umich.edu/bitstream/handle/2027.42/168424/0239_NPHA-Falls-report-FINAL-08022021.pdf.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.