")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 16
Evaluation of Adverse Drug Events in Patients on Anti-Retroviral Therapy Regimen at Omdurman Voluntary Counselling and Testing and Anti-Retroviral Therapy Center in Sudan – A Cross-Sectional Study
Authors Ibrahim EEM, Badi S, Yousef BA , Elsayed LA, Elkheir HK
Received 14 November 2023
Accepted for publication 13 April 2024
Published 20 April 2024 Volume 2024:16 Pages 153—164
DOI https://doi.org/10.2147/HIV.S449900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Eiman Eltayeb M Ibrahim,1 Safaa Badi,1 Bashir A Yousef,2 LutzBashir A Elsayed,3 Habab K Elkheir1,4
1Department of Clinical Pharmacy, Faculty of Pharmacy, Omdurman Islamic University, Khartoum, Sudan; 2Department of Pharmacology, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan; 3Department of Pharmaceutics, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan; 4Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, University of Science and Technology, Khartoum, Sudan
Correspondence: Habab K Elkheir, Department of Clinical Pharmacy, Faculty of Pharmacy, Omdurman Islamic University, Aboseid Street, Khartoum, 14415, Sudan, Tel +249912161326, Fax +249183780696, Email [email protected]
Background: Anti-retroviral therapy-related adverse drug events are accounted as a main cause of anti-retroviral therapy non-adherence. In Sudan, pharmacovigilance studies are relatively rare and obstructed by the problem of under-reporting. It is a well-defined issue worldwide and is highly reported in developing countries. This study aimed to evaluate the prevalence of adverse events associated with anti-retroviral therapy among adult patients with immunodeficiency virus at Omdurman Voluntary Counselling and Testing and Anti-retroviral Therapy Center.
Methods: The study was a descriptive cross-sectional study conducted through direct interviews with 429 patients at the selected center using the Adverse Drug Events (ADEs) reporting form. The collected data were analyzed by The Statistical Package for Social Sciences.
Results: More than half (55.5%) of the participants experienced adverse events, with 48.7% having experienced them at the beginning of treatment. Central nervous system manifestations were the most common adverse events. By using the Naranjo scale, most adverse events showed a “probable” relationship to anti-retroviral medicines. Based on the chi-square test, medication regimen was significantly associated with the presence of ADEs (namely abdominal pain and jaundice) (p values = 0.03 and 0.001), respectively.
Conclusion: This study clearly stated that ART-related ADEs are common among Sudanese PLHIV and with central nervous system being the main adverse events. More pharmacovigilance studies and efforts by healthcare providers should be applied targeting ART-related ADEs under-reporting in Sudanese healthcare facilities.
Keywords: adverse drug event, HIV, AIDS, causality, pharmacovigilance
Background
Human Immunodeficiency Syndrome (HIV) has been ranked among the top health concerns in many parts of the world.1 By the year 2021, the total number of people living with HIV (PLHIV) has averaged 38.4 million, with Africa accounting for more than two-thirds of them.1,2
Sudan is a low-epidemic area with HIV3 despite being boarded by countries with high rates of HIV infections. The first HIV reported case was in 1986.4 Based on The United Nations Programme on HIV/AIDS (UNAIDS) statistics for the year 2022, there are 41,000 [34,000–50,000] adults and children living with HIV in Sudan.5 However, there is a continuous fear that the figures related to HIV infection in Sudan are underestimated. It is associated with high social stigma and discernment.3
The introduction of anti-retroviral therapy (ART) despite having complicated regimens and not a final treatment for HIV has turned it into a controllable chronic disease.6,7
ART is accompanied by a wide range of adverse drug events (ADEs).8 The literature stated that the occurrence of ADEs due to ART is common.9–12
These events are accounted as the main cause of patient non-adherence and affect the patient’s quality of life.10,13 Medication adherence is a cornerstone in HIV management. Without it, the success of treatment could not be warranted.6 Adherence level to HIV therapy should not be lower than “high” equaling 95% to succeed14 which means “achieving and maintaining virological success”.6
ADEs are also considered the main reason for changing or modifying a patient’s initial therapy or even drug discontinuation.15,16 According to the Sudanese study of Elnagar, 2017, the most reported adverse drug reactions were gastro-intestinal and dermatological reactions.11 In Nigeria, nausea was the most common adverse event, followed by abdominal discomfort then insomnia.12 While in Italy, the gastro-intestinal, blood or metabolic, and allergic symptoms were mentioned as the most common adverse events that caused drug discontinuation, with the gastro-intestinal ranked first representing about a quarter of the cases.16
The World Health Organization (WHO) defines pharmacovigilance as the “science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other possible drug-related problems”.17,18
Pharmacovigilance is obstructed by the problem of under-reporting. Two studies stated that close monitoring of patients is the key solution for dealing with the issue of ADEs.7,9 Although adverse drug reactions (ADRs) of ART in developed countries are well known, they cannot be taken as a prediction for ART toxicity profile in developing countries.10,18 The presence of opportunistic infections, malnourishment, and many other conditions and co-morbidities may alter the toxicity of ART.7
The post-marketing pharmacovigilance is crucial for patients’ safety that is evidenced by the number of withdrawn drugs after approval because of safety concerns, as the safety data extracted during the pre-marketing study phase are limited in terms of population and time.19
To the best of our knowledge, no pharmacovigilance study has been conducted targeting ART-related ADEs at Omdurman Voluntary Counselling and Testing (VCT) and Anti-retroviral Centre, which is the largest center of HIV treatment in Sudan. Presence of these ADEs constitutes an inherent risk to the HIV patient’s health. It is a well-defined barrier to drug adherence and subsequently successful treatment. This study aims to shed light on the issue of ADEs of HIV medications including their prevalence. We recognize the importance of this aspect and how the results of such studies can influence HIV programs by raising awareness among patients and healthcare professionals in Sudan. This awareness can educate them on how to deal with these events and reduce their occurrence or avoid them if possible. Additionally, it motivates specialists to strive towards providing regimens with comparable efficacy and fewer adverse effects.
Methods
Study Design and Setting
A descriptive, cross-sectional study was conducted through direct interviews with PLHIV, at Omdurman Voluntary Counselling and Testing (VCT) and Anti-retroviral Therapy (ART) Centre – Omdurman Dermatology and Venereology Teaching Hospital. The center is the main center in Sudan that provides treatment and counselling for adult and pediatric PLHIV. There are four specialists, one consultant, and two professors working at the center. In addition to five counsellors, two pharmacists, two lab technicians, and one nurse. There are also many trainers, volunteers, and people enrolled in the national service. Upon the time of conduction of the study, there were 3320 adult patients registered in the center and had been enrolled on ART.
Study Population and Sampling Procedure
The target population was all registered adult PLHIV enrolled on ART at VCT-ART center and agreed to be part of the study. Patients unable to communicate owing to their health status were excluded from the study.
Sample Size and Sampling Method
The sample size was calculated using, as calculated by Slovin’s Formula, n = N/1+N(e)2. Where n = sample size, N = total target population attending the center (3320 patients), and e = margin of error (0.05) at 95% confidence level.20 The calculated sample size was 357 patients. Due to missing information in many files, we asked and interviewed 429 patients to join the study. The sample size was adjusted by adding 20% to account for potential PLHIVs with missing information and non-response. The participants were selected using a simple random method during the period of the study.
Data Collection
Data were collected using ADEs reporting form designed based on the WHO forms for pharmacovigilance of antiretroviral medicines.18 Data were collected primarily for the purpose of the study. Each ADE has been studied in terms of outcome, severity, and seriousness. The outcome is divided into recovered, recovering, recovered with sequelae, not recovered, died, and unknown. Severity is divided into mild, moderate, and severe. Regarding seriousness, ADEs are divided into non-serious and serious ADE based on certain criteria determined by WHO. Serious events cause death, initiation or prolongation of hospitalization, permanent disability, congenital anomaly/birth defects, or necessitated intervention to prevent permanent damage. Seriousness is of high importance as it guides the regulatory reporting requirements. The intervention for non-serious events has been divided into pharmacological and non-pharmacological interventions. The pharmacological includes modification in ART such as stop therapy, switch therapy, therapy substitution, and adjusting the dose of the current therapy and includes symptomatic treatment. Non-pharmacological intervention stands mainly for counselling either pre-treatment or post-treatment counselling. The difference between switch therapy and therapy substitution is that switch therapy is the transition from first-line therapy to second-line therapy, while therapy substitution is the replacement of the drug with another drug within the same line. Stop therapy is associated with the practice of de-challenge and rechallenge, a clinical protocol of stopping and re-administering the drug accompanied by close monitoring of the adverse effects.
The patient’s file was used to complete information regarding ART therapy, WHO clinical stage, laboratory investigations and other used medications. Each regimen has been separated into three combined medications. The relationship between each medication and the targeted adverse effect has been studied.
The Naranjo Adverse Drug Reaction Probability Scale has been used to assess causality of the suspected adverse reactions. It consists of 10 questions answered by “yes”, “no”, or “I do not know”. Each answer has its value in each separate question. The causality relationship is divided into four groups: definite, probable, possible, and doubtful.21 The platform vigiAcess was used to access the database VigiBase® for answering the first question in the Naranjo scale that explores the previous conclusive reports about the specific adverse events. VigiBase® is the World Health Organization’s (WHO) global database for ADEs, maintained by the Uppsala Monitoring Center.22
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) for Windows, Version 25.0 software (Armonk, NY, USA: IBM Corp). The descriptive statistics were presented in terms of tables as number and frequency percentages. Chi-square test was performed to test associations between adverse events and the socio-demographics and the used ART regimens. Results were considered significant at P value less than 0.05.
Ethical Consideration
The study was conducted agreeing with the recommendations of the Declaration of Helsinki and approved by the Ethics Committee of Omdurman Islamic University, Faculty of Pharmacy (OIU-FP-3/2020). Permission was obtained from VCT-ART Center’s administrators to conduct study. Prior to conducting the study, each participant was asked to provide written informed consent to be included in the study. For patients unable to read (eg, illiterate participants), a third person in the research team was used to read the informed consent for him/her, then the patient was asked to sign the form if he/she could sign, otherwise the co-patient has to sign instead after obtaining patient’s permission. The purpose of the research was explained to them. They were also assured that their participation in this research is voluntary and that their refusal will not forfeit their right to any benefits from this research like increasing their awareness regarding the topic or accessing interventions in future. The research did not include any laboratory or clinical trials; however, patients could experience emotional discomfort. The participant had the right to withdraw from the research at any stage and sign the withdrawal request. We affirmed our full commitment to the confidentiality of the patients’ data. The patient's identity was not disclosed to anyone, even the participants in the research and the statisticians. All questionnaires were coded to ensure confidentiality throughout the study.
Results
Socio-Demographic Characteristics of the Participants
The study included 429 participants, 357 of them responded giving a response rate of 83.2%. The average age of the participants was 39 (±14.1) years, and 36% of them were from the age group 35–44 years. About 52% of them were males and about 90% were residents in Khartoum State and 58.8% were married (Table 1). Only 16% of them were illiterate and more than one-third were unemployed. Furthermore, more than two-thirds (67.2%) of the participants were non-smokers, while more than three-quarters (75.9%) did not use Tombak. Almost all of the participants (95.5%) stated that they do not drink alcohol.
 |
Table 1 Socio-Demographics of the Studied Patients (n=357) |
Clinical Characteristics of the Participants
All of the participants (100%) were within the functional status “work”. Clinically, 61.9% (N = 221) of the participants were in the WHO clinical stage III. Almost all (97%) of the participants reported that they had no signs or symptoms of tuberculosis. Most of them (81.2%) had no other comorbidities (Table 2). About one-third (34.2%) of the participants had a past-history of hospital admission.
 |
Table 2 Clinical Characteristics, Used Antiretroviral Therapy (ART) Regimens, Opportunistic Infections, and Other Related Problems Among the Studied Patients (n=357) |
Medications Data
The median duration since the start of ART was 53 (IQR 22–109) months, and 34.7% of them were using ART for a duration of 36 months and less. The most commonly used ART regimen was 1e regimen (Tenofovir + Lamivudine + Efavirenz) in 78.2% of patients (Table 2). The majority of the studied population (74.8%) did not suffer from any type of opportunistic infections or other related problems since the start of the last regimen (Table 2).
Prevalence, Timing, Distribution and Factors Affecting ADEs Among PLHIV
The prevalence of ADEs in this study was 55.5%. Among patients experiencing ADEs, 48.7% of them started experiencing ADEs at the beginning of treatment (First Month). More than half of the participants (56.1%) experienced ADEs suffered from CNS-related adverse events. Fatigue was observed in 31.8% of patients. Nausea and peripheral neuropathy were documented in 26.8% and 19.7%, respectively (Table 3).
 |
Table 3 Distribution of Adverse Drug Events (ADEs) Among the Studied Patients Experienced ADEs (n=198) |
Table 4 demonstrates the distribution of outcome, severity, seriousness, and intervention to ADEs among HIV patients who experienced ADEs. Most of the participants who experienced ADEs stated full recovery from the events. All participants experienced non-serious ADEs. The severity of ADEs varied between different experienced ADEs (Table 4). Most of the patients did not receive any intervention for most experienced ADEs. Pre-treatment counselling was the most common intervention for nausea, fatigue, abdominal pain, peripheral neuropathy, and CNS-related ADEs except for depression. However, post-treatment intervention was mainly applied for jaundice ADE (Table 4).
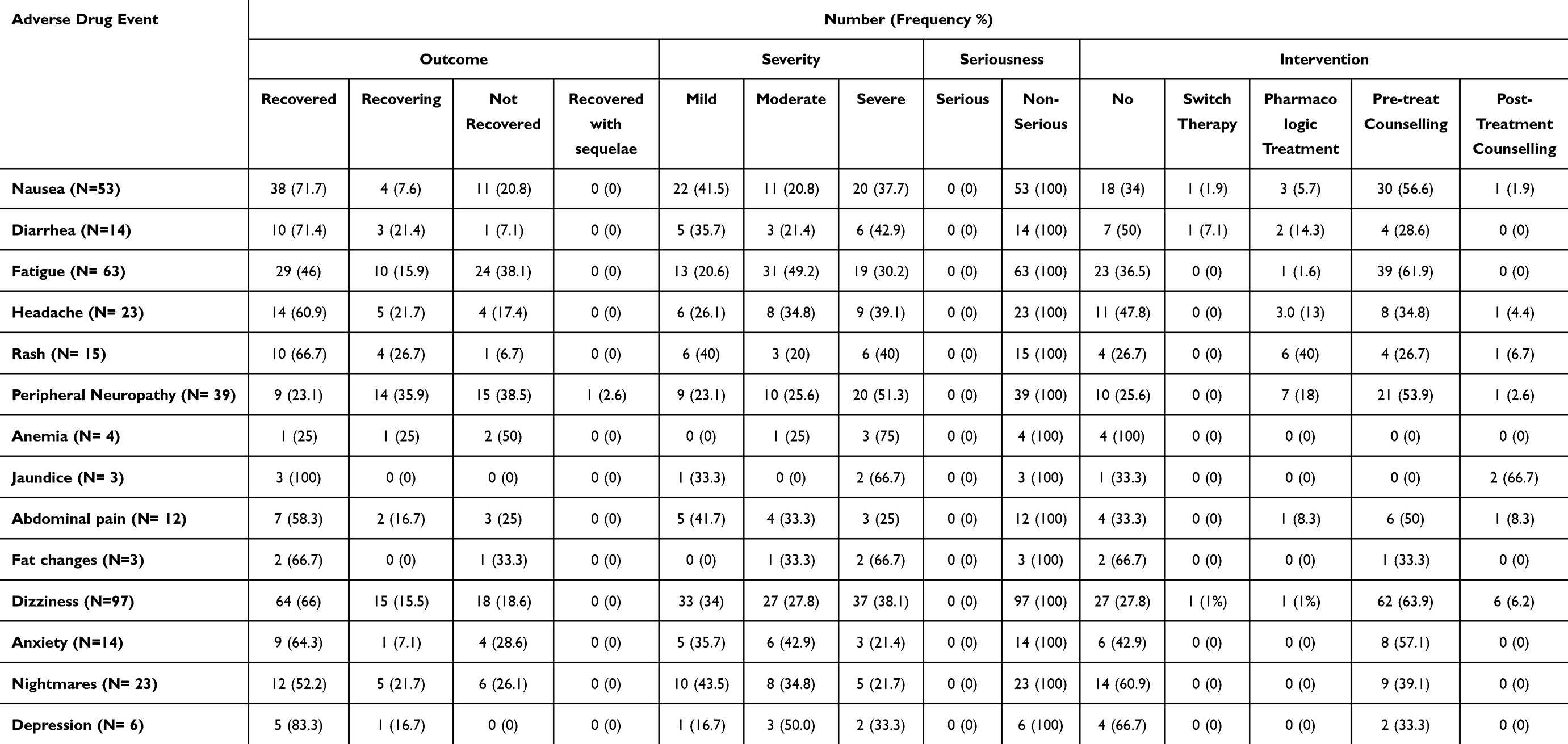 |
Table 4 Distribution of Outcome, Severity, Seriousness and Intervention to Adverse Drug Events (ADEs) Experienced by the Studied Patients (n=198) |
The Naranjo Scale was used to assess the causality of medications to ADEs. As shown in Table 5, almost all experienced ADEs had a probable relationship with the used regimens except for anemia where all the cases had a “possible” relationship. For diarrhea and depression, 50% were classified as possible and 50% as probable.
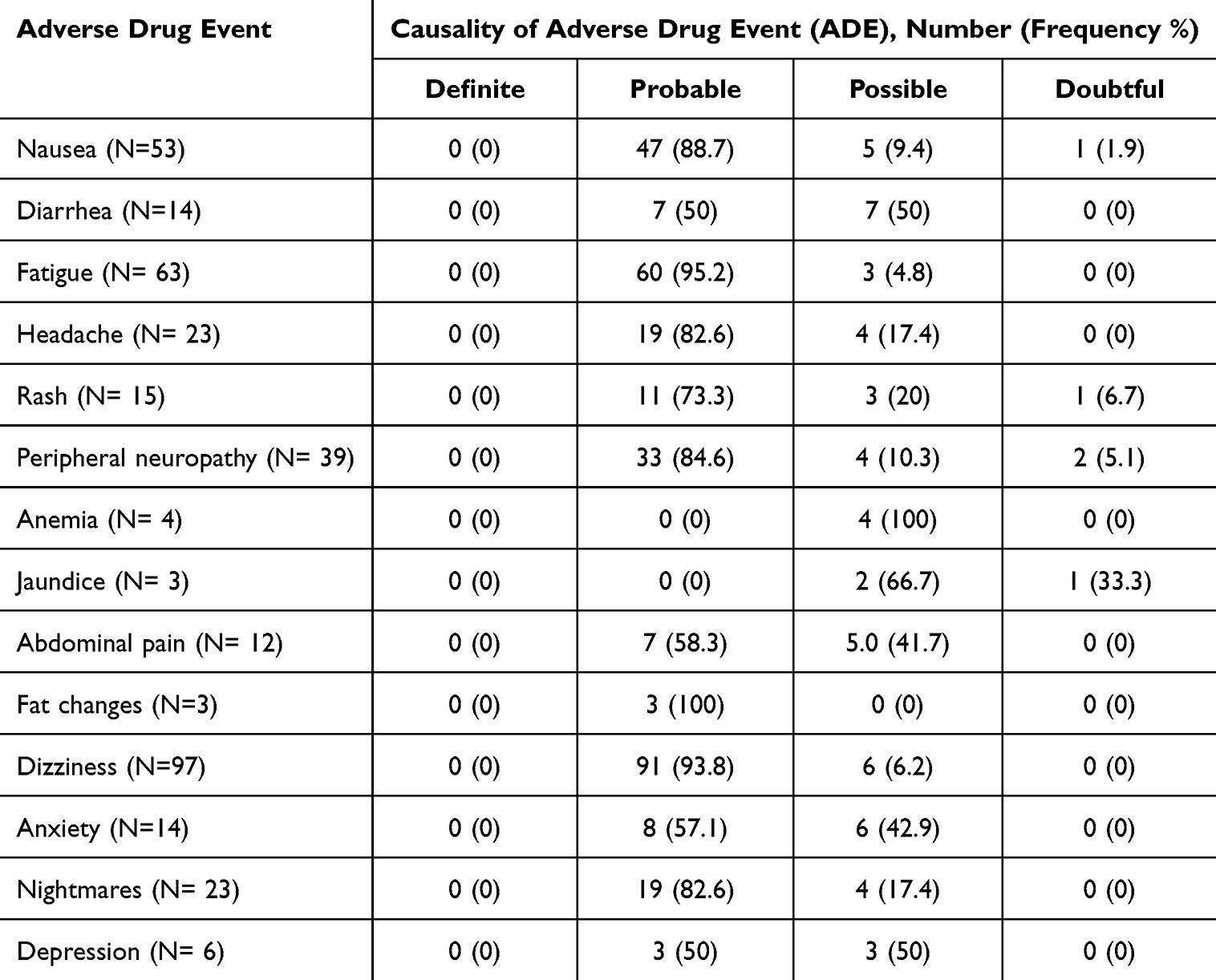 |
Table 5 Causality Assessment of Each Adverse Drug Event (ADE) Using Naranjo Scale Among the Studied Patients Experienced ADEs (N=369) |
The association between the socio-demographic characteristics of the studied population and the presence of ADEs revealed a significant association with the educational status of the patients. Educated patients were more likely to experience ADEs than non-educated people (P value = 0.039) (Table 6). When chi-square test was performed to determine the association between regimen and the presence of ADEs, we found that medication regimen was significantly associated with the presence of ADEs (namely jaundice and abdominal pain) (P values = 0.001 and 0.02), respectively (Table 7).
 |
Table 6 Association Between Socio-Demographic Characteristics and the Occurrence of Adverse Drug Events (ADEs) Among the Studied Patients (n=357) |
 |
Table 7 Association Between Antiretroviral Therapy (ART) Regimens and Adverse Drug Events (ADEs) Among the Studied Patients (N=369) |
Discussion
This study aimed to investigate ADEs related to ART in PLHIV. The study contained 357 adult patients agreed to participate in the study. They were concentrated in the age group of “35 to less than 45 years” (36.1%), the accumulation of the patients in the productive age was shown in many previous studies.3,23–25 The distribution of gender was thought to be equal (52.1% for males and 47.9% for females) coming in line with the UNAIDS global statistics for the year 2021, which showed a percentage of 54 for female PLHIV with 80% of them had access to treatment compared to 70% for males.2 About 83.8% of participants were literate, consistent with other studies with percentages of 86%14 and 66%.26 However, one-third of them (37%) were unemployed. This might be connected to the large proportion of female patients, as in this study, the female group recorded clearly less levels in education and employment compared to the males. Generally, females suffer from narrowed chances of getting higher education and job chances in most African countries, as mentioned in a study that pointed to the socioeconomic implications among PLHIV in Sudan.3 Besides that, they are more subject to family discrimination than males.27 However, in a previous study carried out in Khartoum State, Sudan, the employment rate among PLHIV was 45.5%26 indicating improvement over time as evidenced in our study. An Ethiopian study reported a concerning percentage of 78.9 of total study population for unemployed participants.25
Almost one-third of the participants began therapy within the last three years. This could be a result of increasing awareness of the necessity of HIV testing and enrollment in treatment owing to international and local efforts. In 2014, the UNAIDS stated a target to reduce HIV epidemic, by achieving the following figures by 2020: at least 90% of HIV cases should be diagnosed, 90% of those diagnosed patients have been enrolled on ART, and 90% of those under treatment have a maintained suppressed level of the viral load.28 Most of the participants (78.2%) are in 1e (tenofovir + lamivudine + efavirenz) regimen, which reflects doctors adherence to the national guidelines in Sudan.29
The study revealed that more than half of the participants (55.5%) suffered from ART-related ADEs. A large number of authors in the broader literature stated that the occurrence of ADEs due to ART is common.9,10,30 ADEs targeted in the study were determined by the WHO as the most common ART-related adverse events and are documented in the patient’s monitoring sheet.31 Thus, spontaneous reporting of ADEs is fundamental in ADE surveillance, as it is used to detect ADEs that were not discovered in previous studies.18
In our study, almost half of the patients (48.7%) had ADEs experienced them at the beginning of therapy. Most of the participants (56.1%) who experienced ADEs had CNS manifestations (dizziness, anxiety, nightmares, depression), while one-third (31.8%) of them reported suffering from fatigue, this is expected as most of the patients were on 1e regimen (efavirenz, lamivudine, tenofovir) that contains efavirenz. Comparison with other studies revealed variations in the most occurring ADEs, CNS-related ADEs were the main occurrences, in some studies,7,10 while in others, dermatological events ranked first, then gastro-intestinal problems and neuronal events.11,15 In another study conducted in Nigeria, digestive disorders including nausea and abdominal pain were the most common ADEs followed by insomnia.12 In a South African study targeting patients on second-line ART, anemia, and kidney problems were the most reported adverse events.32
ART-related ADEs have been studied in terms of outcome, severity, seriousness, and the used interventions. The study showed a high rate of recovery among all adverse events except anemia and peripheral neuropathy, where the percentages of “not recovered” exceeded “recovered”, coming in line with the Sudanese report-based study where the outcome of ADRs was mostly “recovered”.11
Most participants who experienced ADEs rated them as severe. In my belief, results regarding severity are not completely reliable due to the difficulty of participants’ understanding of the concept of evaluating severity using daily activities and intervention. This is agreed with the author of the Sudanese report-based study in his belief in the inaccuracy of data regarding severity and patients’ dependence on their perceptions.11 However, in another study, more than 40% of the adverse cases were in WHO grade 1.10 Another study supporting this finding indicated that most ART-related ADEs are mild in general, not serious, and resolved over time.12 In another study, more than 70% of anemia cases and 90% of renal problems detected as ADRs to second-line ART were mild.32 Seriousness has several criteria determined by the WHO depending on the impact of the event on the patient. It is of high importance and guides the regulatory reporting requirements.18 Fortunately, no serious cases were detected in this study.
Intervention to ADEs should be considered, ART-related ADE events accounted as a main cause of patients’ non-adherence to their medicines,10 and they also stand beyond changing or modifying patients’ initial therapy,14 besides affecting their quality of life and hindering them achieving the therapeutic goals.10,11 A substantial portion of the studied population who experienced ADEs received no intervention. In our study, only three types of intervention were detected: switch therapy, pharmacologic treatment, and patient counselling, where pre-treatment counselling was the most followed intervention. About 64% of cases of dizziness and 63% of fatigue stated that there was pre-treatment counselling. In the Sudanese report-based study, switch therapy and symptomatic and/or supportive therapy were the only undertaken interventions.10 In the prospective observational study, counselling (noted as advice) was the most followed intervention, as it was provided in 78% of cases, then symptomatic treatment in 25.7%, and modification in ART in 14.7%.12
Causality assessment of ADRs is an essential part of pharmacovigilance studies. The adverse drug reaction probability scale (Naranjo) has been used in this study for its adequateness and ease of use. In most of the participants who suffered from ADEs, probable relationships were found between ADEs and the used medicine. The prospective observational study mentioned above applied the WHO-UMC scale and it was found that 308 out of 369 events of ADR cases had “probable” relationships with suspected drugs.7 Another study with the same design and scale assigned “certain” causality as the most common with a percentage of 29.8%.10
In this study and based on chi-square analysis, ART medications were significantly associated with the presence of ADEs, namely abdominal pain and jaundice. While in another Sudanese study, the ART regimens 1a, 1b, and 1c were significantly associated with anemia, peripheral neuropathy, redness of the eye and optical neuritis, and neurological ADRs.11 This difference could be explained to some extent by the difference in used drug regimens, selection criteria, and sampling technique between the two studies. Patients’ educational level has also shown a significant effect on reporting the presence of ADEs. This could be attributed to the increased awareness regarding the HIV symptoms and distinguishing them from the adverse events of the used medications, as well as the higher skills of communication in expressing symptoms to healthcare workers. However, in Nigeria, the educational level has no significant effect on patients’ experience of adverse events, but their awareness regarding the disease and the related adverse events specifically has shown a significant effect with the educational level.33
Despite the importance of these types of studies that highlight the importance of pharmacovigilance, many obstacles stemming from the problem of under-reporting were detected. The scarcity of pharmacovigilance research in Sudan has limited the input data used for comparing and interpreting results to draw firm conclusions or even to generalize findings to the whole population. Owing to the inability to access the desired information from the patients’ documents, the study was conducted through direct interview method, which holds the drawbacks of interviewer bias and social desirability bias. Furthermore, laboratory investigations play a significant role in the detection, evaluation, and treatment of adverse events, but there was a clear shortage of these resources.
Conclusion
This study clearly stated the prevalence of ART-related ADEs among Sudanese PLHIV and identified the most common ADEs. ART-related ADEs were found to appear in almost half of the population with central nervous system being the most frequent. Although most are transient, they appear at the beginning of therapy in almost half of patients. All these findings warrant more pharmacovigilance studies and efforts to improve adverse events reporting process in Sudanese healthcare facilities, along with subsequent responses by healthcare practitioners and stakeholders.
Acknowledgments
We do appreciate all participants for their voluntary participation in this study.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. 2007;69(18):1789–1799. doi:10.1212/01.WNL.0000287431.88658.8b
2. Jeudason T. Global progress reported for AIDS. Lancet Infect Dis. 2023;23(9).
3. Ismail SM, Kari F, Kamarulzaman A. The socioeconomic implications among people living with HIV/AIDS in Sudan: challenges and coping strategies. J Int Assoc Provid AIDS Care. 2017;16(5):446–454. doi:10.1177/2325957415622449
4. Sudan National AIDS Council. Sudan National Plan and Sectoral Plans on HIV/AIDS. 2009. 1–49 p.
5. UNAIDS. UNAIDS 2023 Reference; 2023:1–463.
6. Iacob SA, Iacob DG, Jugulete G. Improving the adherence to antiretroviral therapy, a difficult but essential task for a successful HIV TREATMENT-CLINICAL POINTS OF VIEW AND PRACTICAL CONSIDERATIOns. Front Pharmacol. 2017;8(831). doi:10.3389/fphar.2017.00831
7. Reddy TM, Ts DP, Reddy SG, et al. A pharmacovigilance study of antiretroviral therapy in HIV positive out patients at a tertiary care teaching hospital. Int J Basic Clin Pharmacol. 2018;7(12):2419–2422. doi:10.18203/2319-2003.ijbcp20184858
8. Al-Dakkak I, Patel S, McCann E, Gadkari A, Prajapati G, Maiese EM. The impact of specific HIV treatment-related adverse events on adherence to antiretroviral therapy: a systematic review and meta-analysis. AIDS Care. 2013;25(4):400–414. doi:10.1080/09540121.2012.712667
9. Rukmangathen R, Brahmanapalli VD, Thammisetty DP, Pemmasani D, Gali SP, Atmakuru RB. Study of adverse drug reactions to antiretroviral therapy in a tertiary care hospital, Tirupati. Perspect Clin Res. 2020;11(4):158–163. doi:10.4103/picr.PICR_133_18
10. Oumar AA, Abdoulaye A, Maiga M, et al. Adverse drug reactions to antiretroviral therapy (ART): prospective study in HIV infected adults in sikasso (Mali). J Pharmacovigil. 2017;5(2):1–7. doi:10.4172/2329-6887.1000228
11. Elnagar BMI. Prevalence and Extent of Adverse Drug Reactions in Sudanese Patients in Highly Active Anti-retroviral Therapy Regimens. Int J Pharmacovigil. 2017;2(2):1–12. doi:10.15226/2476-2431/2/2/00118
12. Popoola TD, Awodele O, Oshikoya KA. A prospective study of adverse events to antiretroviral therapy in HIV- infected adults in Ekiti State, Nigeria. Afr J med Sci. 2016;45:179–187.
13. Sarfo FS, Sarfo MA, Chadwick D. Incidence and risk factors for neuropsychiatric events among Ghanaian HIV patients on long-term non-nucleoside reverse transcriptase inhibitor-based therapy. eNeurologicalSci. 2016;3:21–25. doi:10.1016/j.ensci.2015.12.002
14. Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S, Mahalingam S. Adherence to antiretroviral therapy among people living with HIV. N Am J Med Sci. 2013;5(3):220–223. doi:10.4103/1947-2714.109196
15. Azevedo LN, Ximenes RA DA, Monteiro P, Montarroyos UR, Miranda-Filho D DB. Factors associated to modification of first-line antiretroviral therapy due to adverse events in people living with HIV/AIDS. Brazilian J Infect Dis. 2020;24(1):65–72. doi:10.1016/j.bjid.2019.11.002
16. Prosperi MC, Fabbiani M, Fanti I, et al. Predictors of first-line antiretroviral therapy discontinuation due to drug-related adverse events in HIV-infected patients: a retrospective cohort study. BMC Infect Dis. 2012;12:1–11. doi:10.1186/1471-2334-12-296
17. World Health Organization. Pharmacovigilance: ensuring the safe use of medicines. World Health; 2004. Available from: http://pvtoolkit.org/toolkit/readers/pv_ensuring_safe_medicine_use.pdf.
18. WHO. A practical handbook on the pharmacovigilance of antiretroviral medicines. WHO press, World Health Organization; 2009. Available from: http://apps.who.int/medicinedocs/documents/s16882e/s16882e.pdf.
19. Fina PM, Cunningham FE, Zhao X, et al. Reporting of adverse drug events in the veterans health administration for patients whose treatment with empagliflozin or apixaban was discontinued. Am J Heal Pharm. 2020;77(1):22–32. doi:10.1093/ajhp/zxz261
20. Slovin E Slovin’s formula for sampling technique; 1960.
21. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
22. Star K, Sandberg L, Bergvall T, Choonara I, Caduff-Janosa P, Edwards IR. Paediatric safety signals identified in VigiBase: Methods and results from Uppsala monitoring centre. Pharmacoepidemiol Drug Saf. 2019;28(5):680–689. doi:10.1002/pds.4734
23. de Los Rios P, Okoli C, Punekar Y, et al. Prevalence, determinants, and impact of suboptimal adherence to HIV medication in 25 countries. Prev Med. 2020;139(106182):25. doi:10.1016/j.ypmed.2020.106182
24. Sendaula E, Buwembo M, Opio D. Clinical profile of HIV-infected adults receiving a holistic approach of care model in Nakawa. Kampala Dis PLoS One. 2022;17(7):1–8. doi:10.1371/journal.pone.0272039
25. Solomon FB, Angore BN, Koyra HC, Tufa EG, Berheto TM, Admasu M. Spectrum of opportunistic infections and associated factors among people living with HIV/AIDS in the era of highly active anti-retroviral treatment in Dawro Zone hospital: a retrospective study. BMC Res Notes. 2018;11(1):1–7. doi:10.1186/s13104-018-3707-9
26. Hassan RHA, Abdelaal AA, Mohammed HA, Elbashir MA, Khalid KB. Survival and mortality analysis for HIV patients in Khartoum State, Sudan 2017. World J Public Heal. 2018;3(4):118–124.
27. UNDP. HIV-related stigma and discrimination In Asia: a review of human development consequences; 2007.
28. UNAIDS. 90-90-90 An ambitious treatment target to help end the AIDS epidemic. UNAIDS; 2014.
29. Saag MS, Gandhi RT, Hoy JF, et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2020 recommendations of the international antiviral society-USA Panel. JAMA. 2020;324(16):1651–1669. doi:10.1001/jama.2020.17025
30. Koochak HE, Babaii A, Pourdast A, et al. Prevalence of adverse drug reactions to highly active antiretroviral therapy (HAART) among HIV Positive patients in imam Khomeini hospital of Tehran, Iran. Infect Disord Drug Targ. 2017;17(2):116–119. doi:10.2174/1871526517666170117111350
31. Sudan National AIDS Control Programme. Global AIDS response progress reporting 2012-2013; 2014.
32. Onoya D, Hirasen K, van den Berg L, Miot J, Long LC, Fox MP. Adverse drug reactions among patients initiating second-line antiretroviral therapy in South Africa. Adis. 2018;41:1343–1353. doi:10.1007/s40264-018-0698-3
33. Agu K, Oparah A, Ochei U. Knowledge and attitudes of HIV-infected patients on antiretroviral therapy regarding adverse drug reactions (ADRs) in selected hospitals in Nigeria. Perspect Clin Res. 2012;3(3):95. doi:10.4103/2229-3485.100657
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.